
Abstract
Purpose:
Although racial and ethnic cancer pain disparities are well-documented, there is insufficient Asian American representation in extant literature, leading to inadequate knowledge about pain outcomes in this population. In addition, the prevalence of depression and its relationship with cancer pain in Asian American patients are poorly characterized. This study evaluated pain differences between Asian American and white patients with cancer and the role of depressive symptoms.
Methods:
Data from two randomized clinical trials investigating integrative therapies for chronic musculoskeletal cancer pain were analyzed to examine the association between race and pain interference using bivariate analyses and linear regression models. We pooled participants from both trials, which enrolled cancer patients with pain and used identical pain and depression assessments, to increase the sample size of Asian American cancer patients, a historically underrepresented population in pain and depression research.
Results:
Compared to White counterparts, Asian American patients reported greater pain interference (5.5 vs. 4.7, p = 0.016) and depressive symptoms (7.1 vs. 5.9, p = 0.047). The Asian race was associated with pain interference (coef. = 0.83, 95% CI: 0.1 to 1.5, p = 0.016) in bivariate analysis. When depressive symptoms were added to regression models, Asian race was no longer associated with pain interference (coef. = 0.51, 95% CI: −0.09 to 1.1, p = 0.097).
Conclusions:
Higher pain interference levels among Asian Americans were partly driven by greater depression severity. These findings highlight the mental health burden among the Asian American cancer population and suggest that treatment for depressive symptoms may need to be incorporated in oncology care and pain management for this population. Importantly, results suggest Asian Americans affected by cancer may be at increased risk for poorly managed pain and depressive symptoms.
Background
Pain is prevalent and debilitating among patients with cancer1,2 and is associated with poor cancer-related clinical outcomes, including decreased survival and increased resource utilization.3–5 Yet about 40% of cancer patients are inadequately treated for pain.1,6 Despite being the fastest-growing racial and ethnic group in the United States, 7 Asian Americans are the only racial group in the country for which cancer is the leading cause of death. 8 Although racial and ethnic cancer pain disparities are well-documented,9–12 there is insufficient Asian American representation in extant studies, leading to inadequate knowledge about pain outcomes in this population. Many studies to date lack estimates for Asian Americans, 11 included less than 1% of Asian Americans in study samples,9,10 or grouped Asian patients with other races or ethnicities. 12 The “model minority” stereotype perpetuates the exclusion of Asian Americans from health disparities research, resulting in unidentified and unmet needs.13–15 Provider-held stereotypes—such as assumptions about higher pain tolerance—can also influence pain management decisions in this population.15,16
Depression is prevalent among patients with cancer and is an important factor impacting pain outcomes.17–20 In a systematic review of 14 studies, 9 reported a positive association between pain and depression. 21 However, the prevalence of depression and its relationship with cancer pain in Asian American patients are poorly characterized. To address this gap, this study evaluated pain differences between Asian American and White patients with cancer and the role of depressive symptoms.
Methods
Study design, setting, and participants
This is a secondary analysis of baseline data from two randomized clinical trials (RCTs): (1) the Personalized Electroacupuncture versus Auricular Acupuncture Comparativeness Effectiveness trial—a three-arm, parallel-group RCT that compared electro-acupuncture versus auricular acupuncture to usual care for chronic musculoskeletal pain among English-speaking adult survivors of various cancer types; and (2) the Integrative Medicine for Pain in Patients with Advanced Cancer Trial—a two-arm, parallel-group RCT that evaluated the comparative effectiveness of electroacupuncture versus massage therapy for pain in English- or Spanish-speaking adult patients living with advanced cancer. We pooled participants from both trials to increase the sample size of Asian American cancer patients, a historically underrepresented population in pain and depression research. Both trials enrolled cancer patients with pain and used identical pain and depression assessments, making it appropriate to combine the baseline data from these two trials. Details of the study protocols have been published previously.22,23 The Memorial Sloan Kettering Cancer Center institutional review board reviewed and approved the study protocols (#16-1579; #19-341).
Measures
Pain interference
The Brief Pain Inventory (BPI) was administered at baseline of both trials to evaluate pain interference (i.e., impact of pain on daily activities) and severity. The BPI is a widely used, validated instrument and has demonstrated reliability in cancer populations with a Cronbach’s α ranging from 0.77 to 0.91. 24 The BPI has two subscales both scored on a 0–10 scale, a 4-item pain severity measure (“no pain” to “pain as bad as you can imagine”) and a 7-item pain-related functional interference score (“no interference” to “worst possible interference”). Given that research suggests Asian patients may under-report pain severity, 25 we opted to use pain interference as the dependent variable, as this may better capture the burden of pain in this population. As described below, pain severity was included in the analysis as a covariate.
Asian race
Race (independent variable) was self-reported by participants. The term Asian defines a population that has origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent, according to the United States Census. 26 Although other sources may further distinguish between different Asian populations, the broader term Asian was used in this study because this was the term used in the demographics survey completed at baseline by participants in both RCTs.
Depressive symptoms
The depression subscale of the Hospital Anxiety and Depression Scale (HADs) was administered at baseline to assess depressive symptoms (primary covariate). The HADS depression subscale is a 7 item, self-administered rating scale. 27 Participants were asked to complete the questionnaire and were scored on a scale of 0–21. 27 Scores of ≥11 indicated clinically abnormal depressive symptoms; scores of 8–10 indicated borderline depressive symptoms; and scores of 0–7 indicated no depressive symptoms.
Additional covariates
Besides race, we also assessed gender, education, and cancer type at baseline by participant self-report.
Statistical analyses
Descriptive statistics were presented as means and percentages. Baseline characteristics were compared between Asian and White participants by two-sample t-test and Pearson’s chi-squared test. To examine pain disparities between Asian and White participants, we conducted bivariate analyses to examine whether Asian race was associated with greater pain interference, using White race as the reference. We then used multivariable linear regression to examine whether depressive symptoms or other covariates could explain the association between Asian race and pain interference. Model 1 included Asian race and depressive symptoms. Model 2 added pain severity to the variables in Model 1. Model 3 added gender and education to the variables in Model 2.
Results
Table 1 shows baseline demographic and clinical characteristics of study participants. Compared to the White participants, a higher proportion of Asian participants were female, received a college education or higher, and had a history of breast cancer (all p < 0.05).
Study Participant Characteristics

HADS, Hospital Anxiety and Depression Scale; the bold data indicate statistical significance (p < 0.05).
Among White patients, 328 (67.1%) reported moderate to severe pain interference, and 168 (34.4%) reported depressive symptoms (Table 2). Among Asian patients, 38 (86.4%) reported moderate to severe pain interference, and 20 (45.5%) reported depressive symptoms (Table 2).
Association Between Depression and Pain Interference Among White and Asian Patients
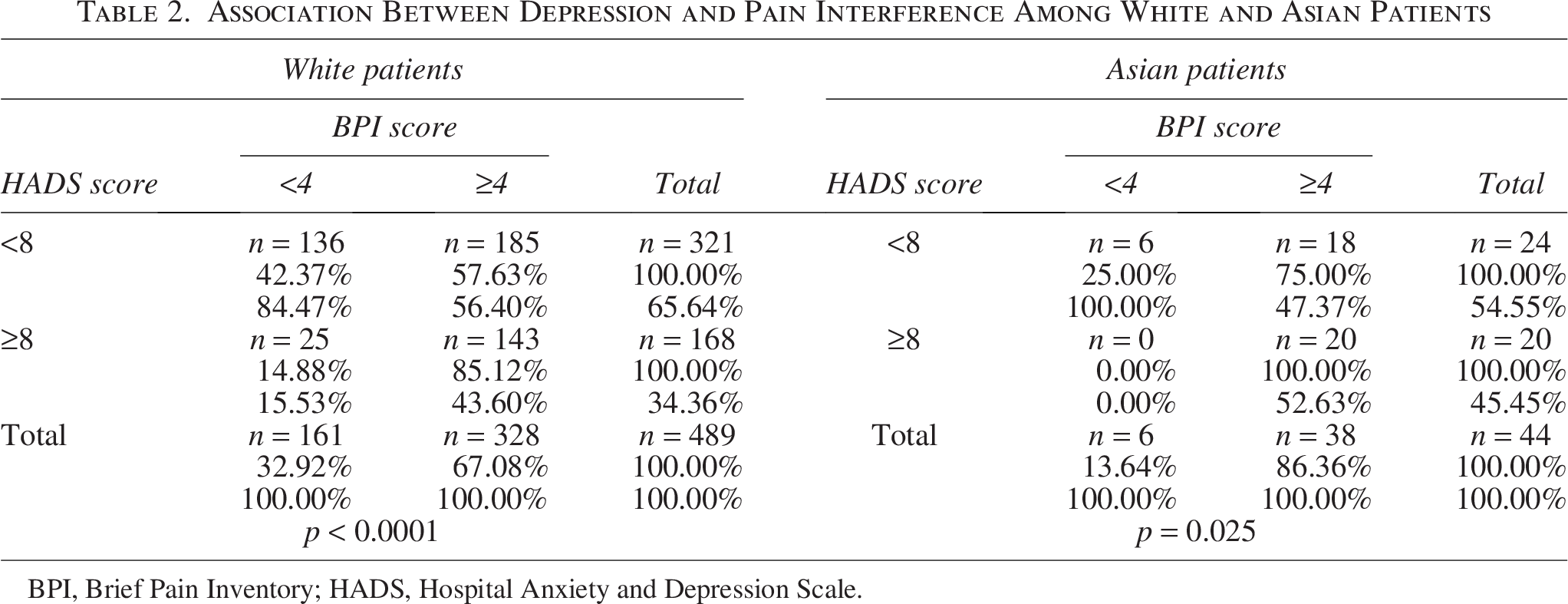
BPI, Brief Pain Inventory; HADS, Hospital Anxiety and Depression Scale.
Asian participants reported greater severity of pain interference (5.5 vs. 4.7, p = 0.016) and depressive symptoms (7.1 vs. 5.9, p = 0.047), relative to their White counterparts (Figs. 1 and 2).
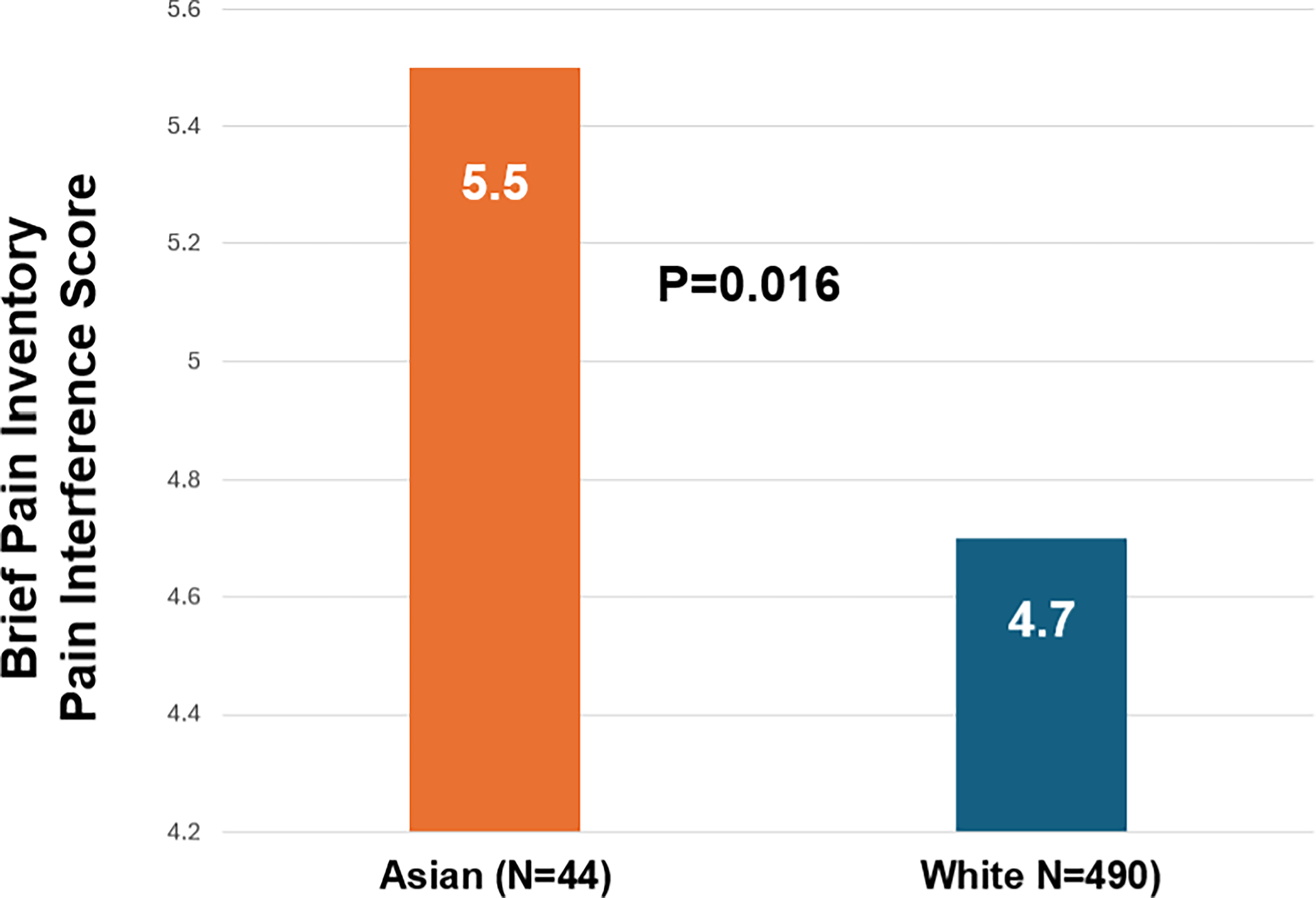
Racial differences in pain interference. The difference in pain interference between Asian patients (n = 44) and White patients (n = 490) in the pooled sample per the Brief Pain Inventory Pain Interference score is statistically significant (5.5 vs. 4.7, p = 0.016).
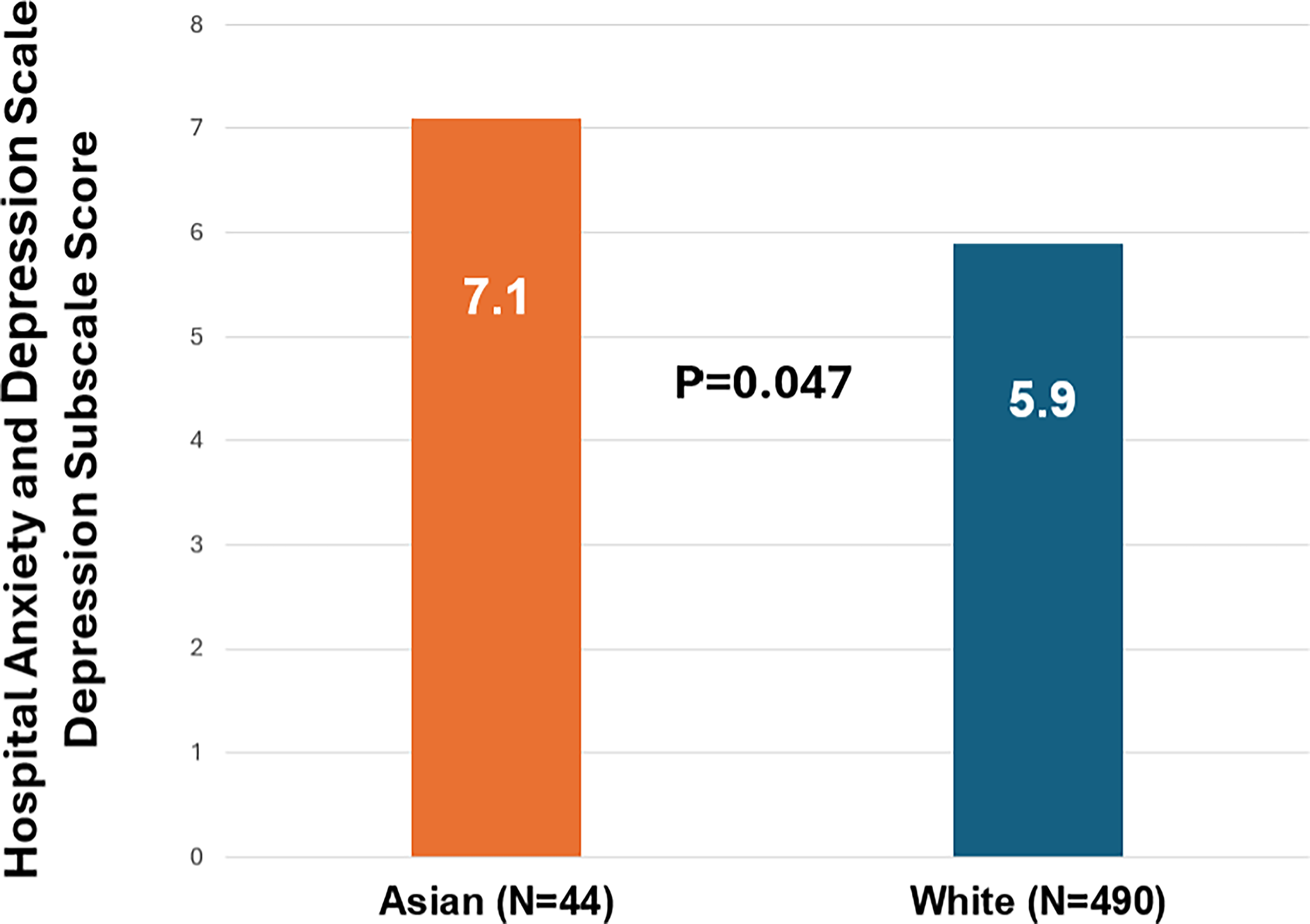
Racial differences in depressive symptoms. The difference in depressive symptoms between Asian patients (n = 44) and White patients (n = 490) in the pooled sample per the Hospital Anxiety and Depression Scale Depression Subscale score is statistically significant (7.1 vs. 5.9, p = 0.047).
In bivariate analyses, Asian race was significantly associated with greater pain interference (coef. = 0.83, 95% CI: 0.1–1.5, p = 0.016). However, this association was no longer significant when depression was added to the multivariable linear regression model. In the regression model that included race, pain severity, and depression, only pain severity and depression remained significantly associated with pain interference (Table 3). The same findings held true when gender and education were added to the analysis.
Factors Associated with Pain Interference Among Study Participants
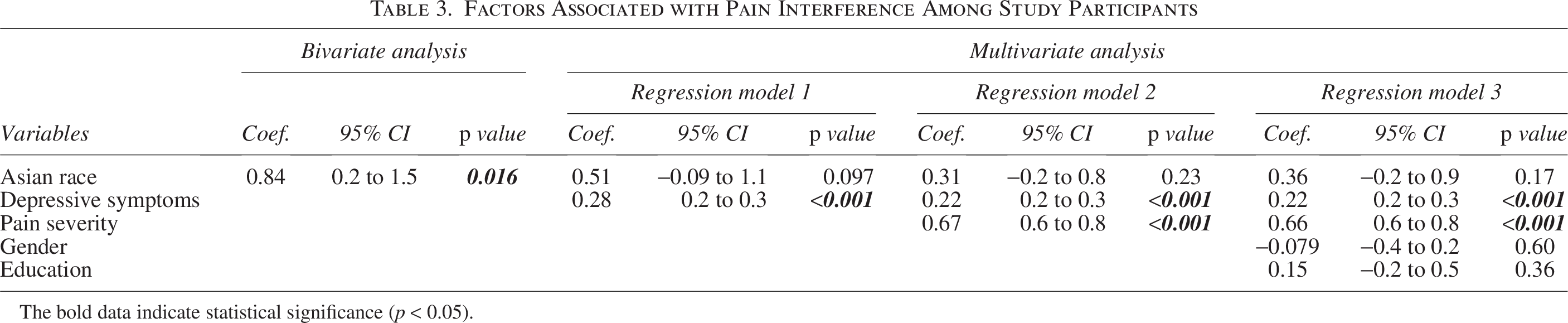
The bold data indicate statistical significance (p < 0.05).
Discussion
In this study of Asian American and White patients with chronic musculoskeletal pain among diverse cancer diagnoses, Asian Americans reported higher interference, which was driven in part by higher levels of depressive symptoms. These findings highlight the mental health burden among the Asian American cancer population and suggest that treatment for depressive symptoms may need to be incorporated in oncology care and pain management for this population. Importantly, results suggest Asian Americans affected by cancer may be at increased risk for poorly managed pain and depressive symptoms.
Our findings align with prior research of Asian populations without cancer, 28 as well as a pilot study of Chinese Americans 29 (n = 50) that found most patients with cancer reported moderate to severe pain and moderate levels of anxiety and depression. Our results point to the crucial need to ensure guideline-concordant pain management strategies for minoritized populations while improving the identification and treatment of comorbid depressive symptoms to bolster clinical outcomes. 30 Documented stoicism of Asian American patients with cancer toward pain contributes to underreporting of pain severity and inadequate pain management. 25 These patients also have concerns related to pain medication use, including tolerance and addiction, posing additional pain treatment barriers. 31 Considering these challenges, improved mental health assessment and treatment, particularly for comorbid depressive symptoms, may provide a novel angle for addressing pain in this population. Such assessments should be informed by culturally relevant evidence regarding somatization of depressive symptoms in some Asian populations.32–34 Our findings on the role of mental health in pain experiences of Asian Americans are especially timely in the post-pandemic era. In 2021, there was a reported sevenfold increase in rates of depression among Asian Americans during the COVID-19 pandemic in comparison to 2019. 35 Although this increase could be partly explained factors such as social isolation, there was a notable increase in xenophobia, racism, and hate incidents directed toward Asian Americans. 36 A study conducted in June 2020 found that Asian Americans who experienced discrimination reported more depression compared to those who did not. Furthermore, Asian Americans are the racial group least likely to seek mental health services, with only 8.6% of Asian Americans seeking mental health treatment compared to 17.9% of the general United States population. 37 This gap in mental health care may be due to negative perceptions and cultural stigmas associated with mental health conditions and treatment within Asian American communities, as well as inadequate cultural and linguistic responsiveness in mental health care. 38 Thus, research aiming to address the barriers to mental health treatment among Asian Americans is imperative and could play a key role in reducing cancer pain disparities in this population.
Several study limitations exist. First, our study focused on depressive symptoms and did not include clinical diagnoses of major depressive disorder or other psychiatric conditions. Future studies should consider including more comprehensive clinical evaluations of other mental health conditions. Second, our sample included patients who were predominantly female, had breast cancer, and possessed a college-level education, potentially limiting the generalizability of findings. Third, given that an estimated 32% of Asian Americans have limited English proficiency and 20% of Asian households in the United States are linguistically isolated (i.e., no household member older than 14 years of age can speak English exclusively or “very well”), 39 the parent trials’ English- and Spanish-language-only inclusion criteria may have limited more diverse experiences from being captured and accounted for in this secondary analysis. Fourth, we did not stratify different ethnic or national subgroups among Asian American participants due to data availability limitations. Since divergent levels of acculturation among Asian Americans may impact pain and depression,29,40 future trials should provide more detailed racial data, rather than presenting Asian Americans as a homogeneous population. Fifth, this study included patients across the cancer care spectrum; thus, depending on their cancer treatment status, it is possible that patients may have had different drivers of their pain symptoms. Finally, due to the relatively small sample of Asian American participants, we do not have adequate power to examine all relevant covariates in the regression models; thus, the possibility of residual confounding between the variables of interest should be considered.
Conclusion
We found a higher pain interference and depressive symptom burden among Asian American patients when compared to White patients. Our findings suggested that addressing unmet mental health needs among Asian American patients with cancer should be a key component of strategies to reduce pain disparities in oncology care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Cancer Institute (K08CA266927); the Department of Defense office of the Congressionally Directed Medical Research Programs (W81XWH-15–1-0245), the Patient-Centered Outcomes Research Institute (SMPAI-2018C2-12883), the National Cancer Institute’s Cancer Research Education Grants Program (5R25CA020449), and the National Institutes of Health’s Cancer Center Support Grant (P30-CA008748). The content is solely the responsibility of the authors and does not represent the official views of the funders. The authors declare no conflicts of interest. WER is partially supported by the Robert Wood Johnson Foundation Harold Amos Medical Faculty Development Program. J-CH and YB are supported by National Cancer Institute (R01CA267996) and American Cancer Society (RSGI-22–130-01-HOPS).