
Abstract
Introduction:
Using time-limited trials of low-dose, sustained-release morphine to reduce chronic breathlessness to evaluate net effects may generate opioid withdrawal symptoms if medication is ceased. This sub-study of a larger randomized, placebo-controlled, double-blind trial aimed to evaluate if this occurred.
Methods:
People with modified Medical Research Council breathlessness scores of 3 or 4 and chronic obstructive pulmonary disease were eligible for a dose-increment titration phase (≤3weeks) and blinded extension (<26 weeks). Participants filled out the Subjective Opioid Withdrawal Scale (SOWS) daily for three days after ceasing/completing study medication (score 0–60; scores >20/60 severe opioid withdrawal). Active therapy was compared with placebo, and then, for people on morphine, comparisons between higher doses (24 mg, 32 mg), and lower doses (8 mg, 16 mg) and duration were undertaken.
Results:
Data were available for 126/156 participants (47% female, median age 73). Placebo or active therapy (Days 1–3) showed no statistically significant differences in SOWS scores (p > 0.05 for all days; Day 1 median 3/60 [IQR 1, 5] compared with 2/60 [IQR 1, 6], respectively; p = 0.475). Neither morphine duration nor dose were significantly different. Two people in the lower dose group in the extension phase had scores >20 for all three days. Individual symptoms that may draw clinical attention to morphine withdrawal include anxiety, a runny nose, perspiration, shaking, hot flushes, or nausea.
Discussion:
This preplanned substudy quantified risks of people experiencing self-reported symptoms of opioid withdrawal using a validated tool to inform discussions between clinicians and people with chronic breathlessness.
Key message
A small percentage of people who take regular, low-dose, sustained-release morphine for the symptomatic reduction of chronic breathlessness may experience transient opioid withdrawal symptoms if the therapy is ceased. People on therapy for longer were at higher risk of more severe withdrawal symptoms.
Introduction
Chronic breathlessness is a symptom for many people late in life, creating disability and suffering, despite optimal treatment of the underlying cause(s). 1 Such breathlessness often worsens at the end of life and is more prevalent in people with underlying respiratory causes as the dominant reason that they are experiencing this symptom. 2
People with advanced life-limiting illnesses who experience moderate to severe chronic breathlessness late in life may be offered a time-limited trial of regular, low-dose, sustained-release morphine to try to reduce their respiratory symptoms.3,4 However, this practice may also expose people to the risk of opioid withdrawal symptoms—limiting the net clinical benefit of the therapy. This raises the key question of whether people may experience clinically important opioid withdrawal symptoms if their therapeutic trial showed no net benefit. 5
Much of our knowledge about opioid withdrawal symptoms does not come from people with advanced life-limiting illnesses but from other clinical populations such as people withdrawing from the nonclinical use of opioids, who often withdraw from markedly higher opioid doses having taken them for much longer periods of time. Understanding any risks of opioid withdrawal symptoms in people with serious illness—with lower doses and generally shorter duration of therapy—is critical to optimize clinical management of people with severe chronic breathlessness.
This preplanned sub-study of a randomized clinical trial (RCT) 6 aimed to evaluate whether there were subjective symptoms of opioid withdrawal in people as they completed a study of regular, low-dose, sustained-release morphine.
Methods
This was a sub-study of the Breathing, Exertion And Morphine Sulfate multisite, placebo-controlled, dose increment, double-blind study evaluating sustained-release morphine for the symptomatic reduction of chronic breathlessness. 6
In brief, the trial enrolled 156 people with chronic obstructive pulmonary disease (COPD) and a modified Medical Research Council breathlessness scale rating 7 of 3 or 4, where underlying cause(s) of their breathlessness had been optimally treated. People who had been on ≥8 mg oral morphine equivalent in the previous seven days, those with a history of experiencing problems with opioids and people with severe renal impairment (cCR ≤15) were excluded (Complete eligibility criteria-Supplementary Table S1).
Participants were randomized at commencement to an arm comprising of three randomizations: week 1—one of three possible doses (0 mg, 8 mg, 16 mg) of sustained-release morphine, and then week 2 and week 3 to an additional 0 mg or 8 mg of the medication giving a final range of sustained-release morphine sulfate of 0–32 mg daily. The primary outcome was worst breathlessness in the previous 24 hours using the validated 0–10 numerical rating scale anchored at zero (no breathlessness) and 10 (worst possible breathlessness). After the initial three-week dose increment phases, there was an optional blinded extension study for up to six months. In this current sub-study, given the pharmacokinetics of the sustained release formulation, people needed to have been on a morphine dose for 72 hours to be included at that dose level; otherwise, the previous dose level was used in the analysis. 8
Assessments
Baseline clinicodemographic data are reported, including age, sex, smoking history, oxygen use, and breathlessness evaluations.
The Subjective Opioid Withdrawal Scale (SOWS) tool was developed originally for the evaluation of opioid withdrawal in people using opioids for nonclinical purposes and had 16 questions each scored on a 0–4 ordinal scale giving a possible score range of 0–64 with higher scores reflecting worse subjective symptoms of withdrawal. 9 It is measured daily for three consecutive days at the time each participant ceased study medication. The last question (“I feel like shooting up”) was not included in the current study, reducing the maximum score to 60. People with scores ≤10 were considered not to have clinically important opioid withdrawal. 10 All responses were participant-reported.
All participants were asked to fill out the SOWS tool at the conclusion of their involvement in the study, whenever that occurred for three consecutive days while still blinded to the arm to which they had been randomized. Conclusion of involvement was at the time anyone ceased medication: early withdrawal, electing not to enter the extension phase, or at study conclusion. No tapering of dose was included in the protocol.
Statistical analyses
The population was described, and Mann–Whitney U tests were used when comparing groups because the data were non-normally distributed, as indicated by the standard deviation being larger than the mean, and the small sample sizes.
Three comparisons on each of the three days of data collection for the total SOWS scores were then analyzed: Whole study population by final treatment group: Participants were assigned to either the placebo or opioid group;
Within the active (morphine) arms, two further comparisons were undertaken using independent sample t-tests:
Duration of sustained-release morphine use: duration was dichotomized between participants who completed their involvement during the titration phase (up to the end of week 3) or entered the double-blind extension phase (weeks 3–26). Dosage of sustained release morphine: participants receiving opioids were dichotomized by dose: lower dose (8 mg or 16 mg) and higher dose (24 mg or 32 mg).
Ethics and reporting
The study was approved by an appropriately constituted Hunter New England Human Research Ethics Committee (Reference No. 15/12/16/3.06) and registered before the first participant was enrolled (ClinicalTrials.gov Identifier: NCT02720822). The study was reported in accordance with the CONSORT criteria for randomized trials.
No data were imputed.
Results
In total, 156 people were randomized, of whom 48% were female, median age 72; 45% were on long-term oxygen therapy (LTOT), and the median age-adjusted Charlson Co-morbidity Index score was 5 (range 1–11). For this sub-study, data were available for 126 participants (47% female; median age 73; 40% on LTOT; and a median Charlson Co-morbidity Index score 5.0; Table 1). People withdrew from or completed the study at different stages (Supplementary Table S2). Final study doses at each individual’s completion of the study were placebo n = 15 (10%); 8 mg n = 42 (28%); 16 mg n = 53 (35%); 24 mg n = 33 (22%); and 32 mg n = 9 (6%), reflecting the expected distribution of doses.
Characteristics of Particpants in a Double-Blind, Placebo-Controlled Randomized Study Who Provided Data at the End of Therapy in a Trial of Regular, Low-Dose, Sustained Release Morphine for the Reduction of Breathlessness in People with Chronic Obstructive Pulmonary Disease (n = 126 of 156 participants)
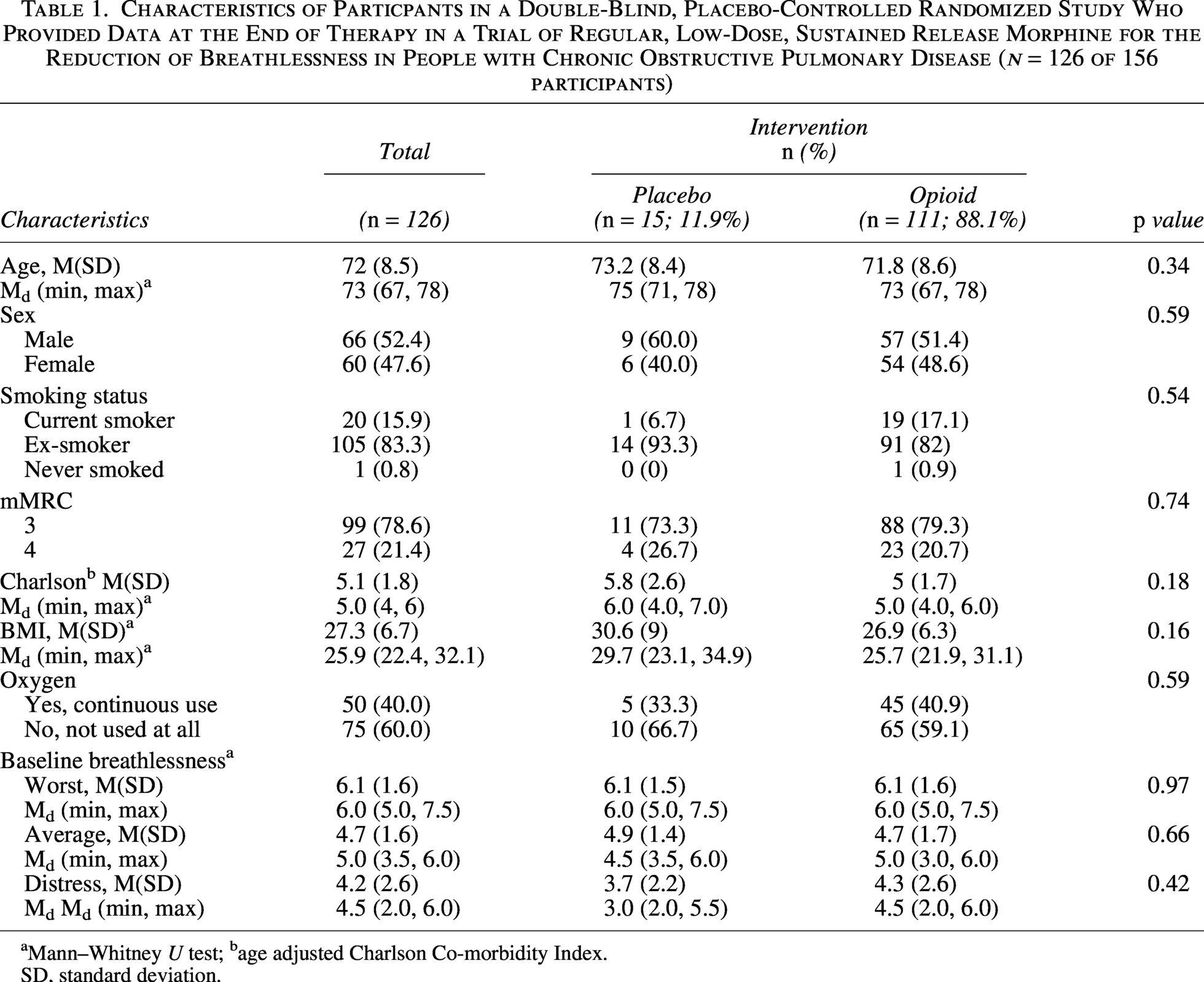
aMann–Whitney U test; bage adjusted Charlson Co-morbidity Index.
SD, standard deviation.
In the analysis of people on active therapy or placebo (Analysis 1), across Days 1–3, no statistically significant differences in SOWS scores were observed between the placebo and opioid groups (p > 0.05 for all days; Day 1 median 3./60 (IQR 1, 5) compared with 2/60 (IQR 1, 6) respectively; p = 0.475; Table 2).
Subjective Opioid Withdrawal Scale (SOWS) Total Scores in the Three Consecutive Days After Finishing Therapy in a Double-Blind, Placebo-Controlled Trial of Regular, Low-Dose, Sustained-Release Morphine for the Symptomatic Reduction of Chronic Breathlessness by Arm (Placebo/Active Arm), Duration of Therapy, and Dosage
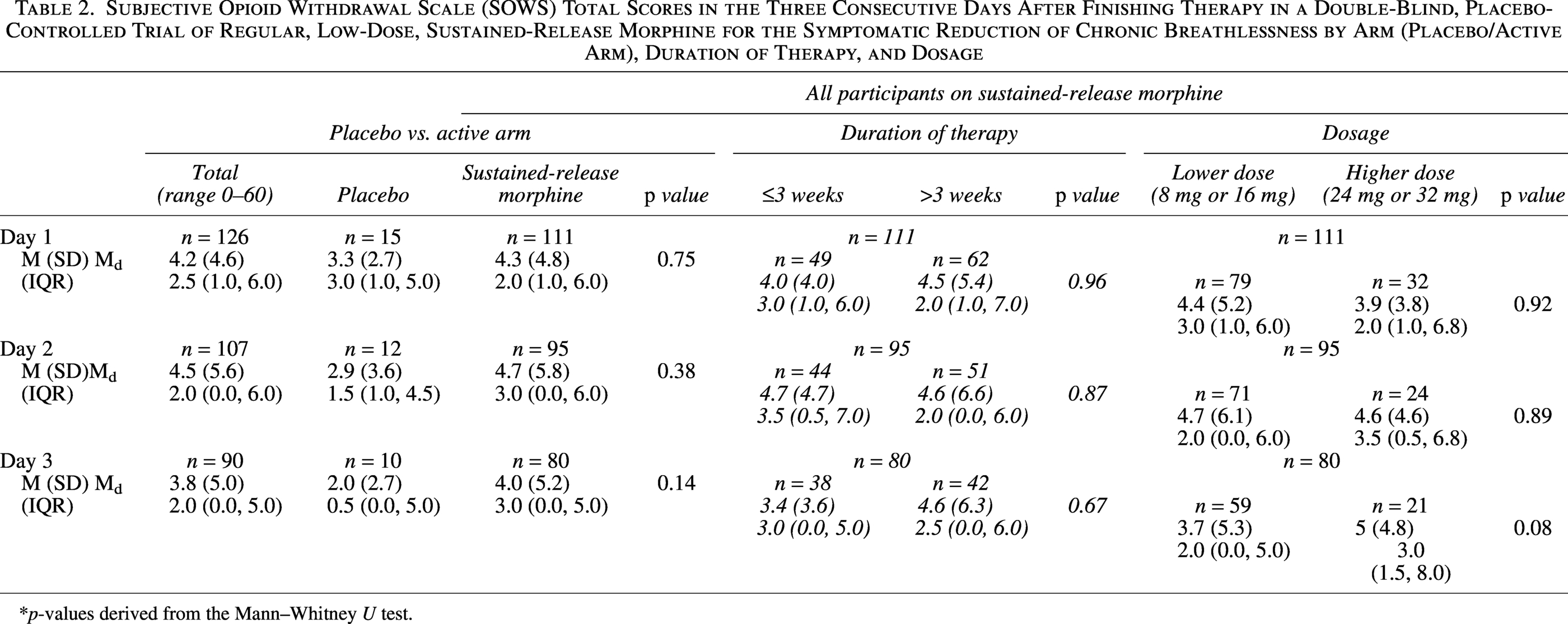
p-values derived from the Mann–Whitney U test.
In people on sustained-release morphine, duration of therapy (Analysis 2a; ≤3 or >3 weeks) revealed no significant differences in SOWS scores (p < 0.05 for all three days after morphine cessation; Day 1 median scores 3/.60 (IQR 1, 6) compared with 2./60 (IQR 1, 7), respectively; p = 0.96; Table 2). In people on lower (8 mg, 16 mg) or higher doses (24 mg, 32 mg) of sustained-release morphine comparing dose intensity (Analysis 2b), there were no significant differences in SOWS scores between the two arms across any of the three days after morphine cessation (p > 0.05 for all three days; Day 1 median scores 3./60 (IQR 1, 6) compared with 2/60 (IQR 1, 6), respectively; p = 0.92; Table 2).
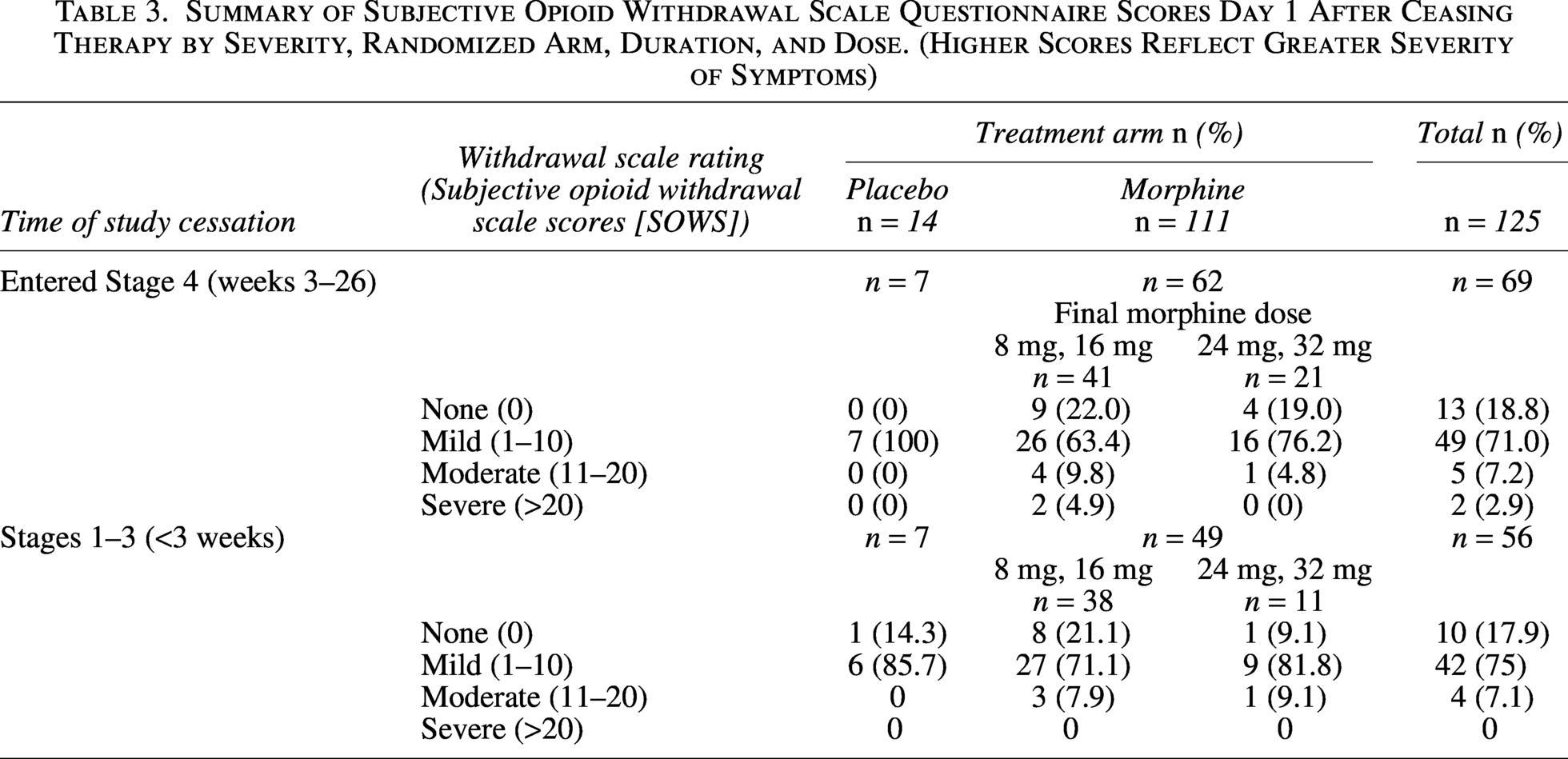
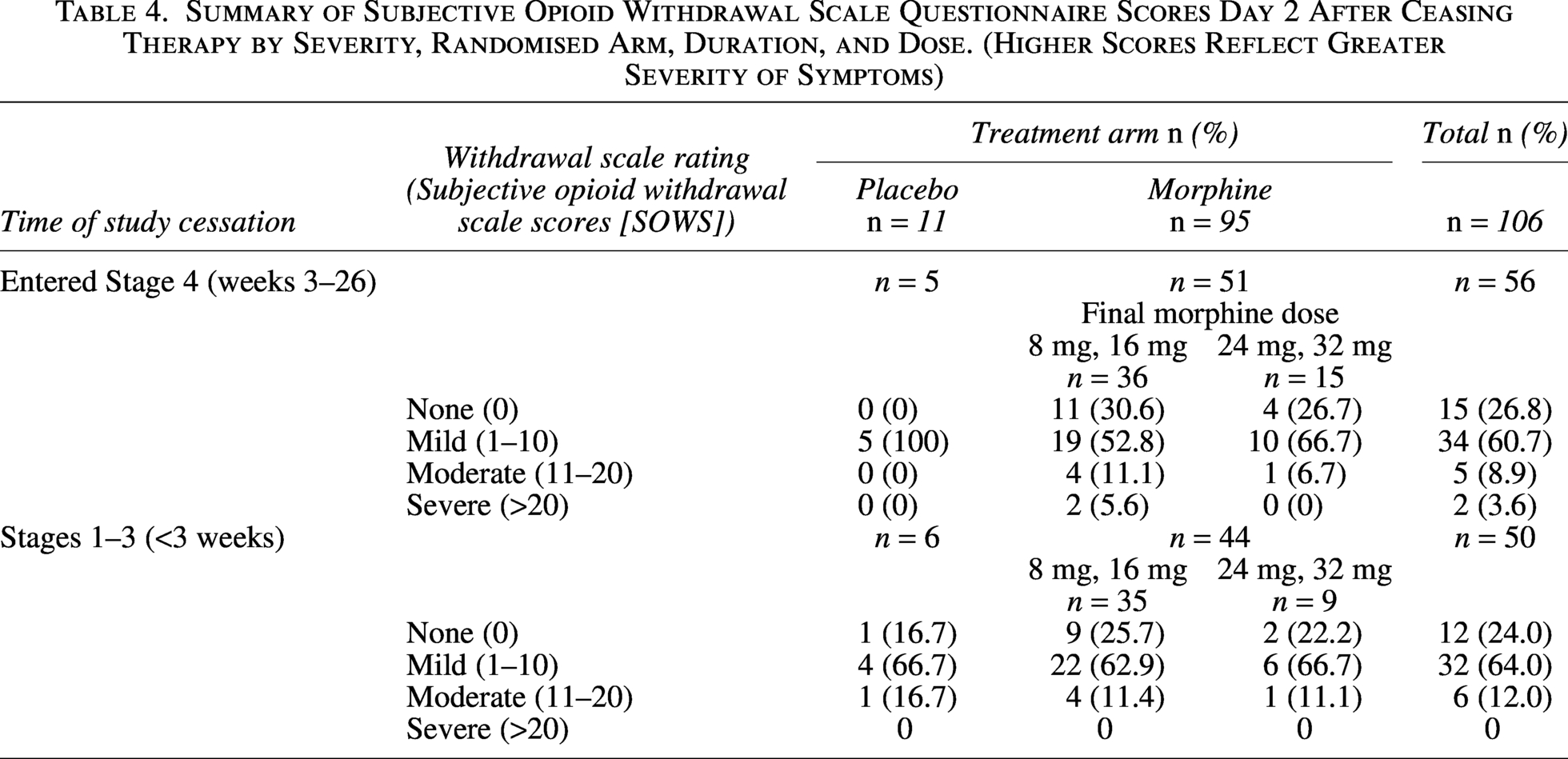
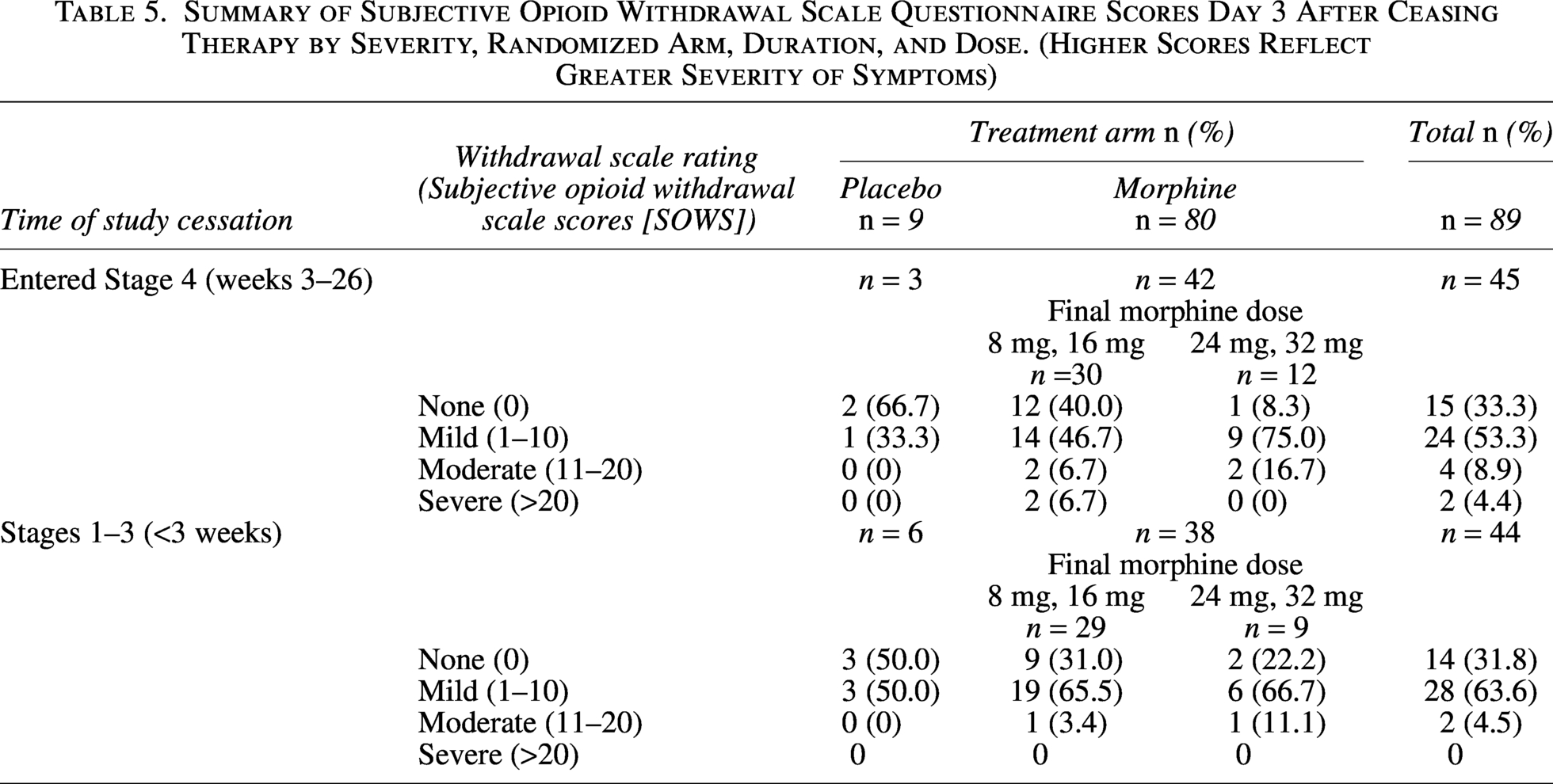
Two people on the active arm in the extension phase at lower doses had total scores that were above the “severe” threshold for SOWS (>20) for all three days (Tables 3–5). SOWS scores of moderate withdrawal (11–20) occurred in fewer than 10% of people on any of the three days after ceasing therapy.
Summary of Subjective Opioid Withdrawal Scale Questionnaire Scores Day 1 After Ceasing Therapy by Severity, Randomized Arm, Duration, and Dose. (Higher Scores Reflect Greater Severity of Symptoms)
Summary of Subjective Opioid Withdrawal Scale Questionnaire Scores Day 2 After Ceasing Therapy by Severity, Randomised Arm, Duration, and Dose. (Higher Scores Reflect Greater Severity of Symptoms)
Summary of Subjective Opioid Withdrawal Scale Questionnaire Scores Day 3 After Ceasing Therapy by Severity, Randomized Arm, Duration, and Dose. (Higher Scores Reflect Greater Severity of Symptoms)
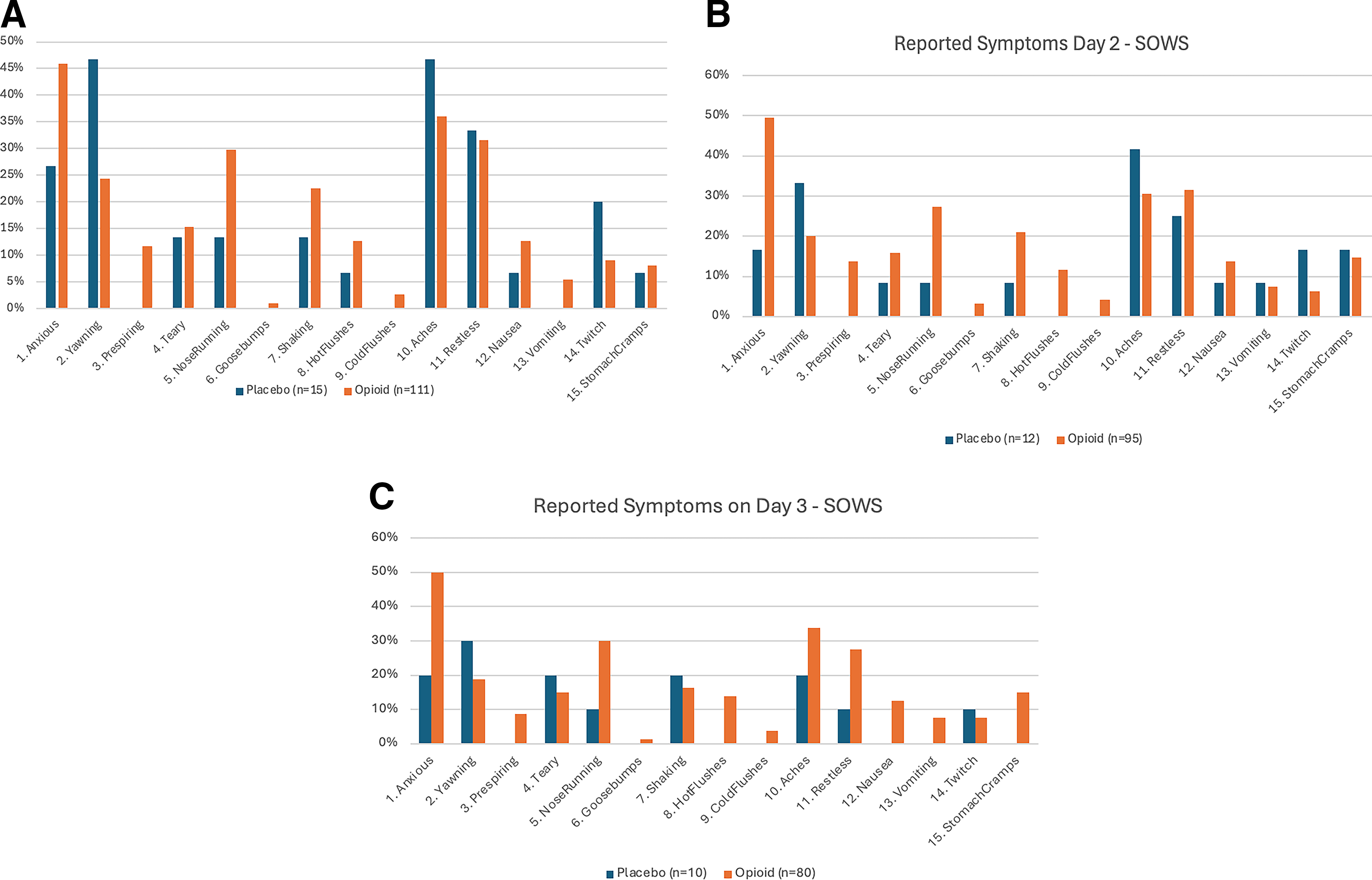
Individual symptoms that may draw clinical attention to opioid cessation on Day 1 include anxiety, a runny nose, perspiration, shaking, hot flushes, or nausea (Figure 1a–1c). By day 3, this may also include stomach cramps (Figure 1c). Each of these symptoms was reported more frequently in people on the active arm of the study.
Discussion
This planned sub-study of a double-blind, placebo-controlled RCT shows that only 3% of people on morphine reported severe withdrawal symptoms when ceasing regular, low-dose, sustained-release morphine of between 8 mg and 32 mg per 24 hours at steady state for the symptomatic reduction of chronic breathlessness. Two people on lower doses from more than three weeks each scored >20/60 (the reported threshold for “severe withdrawal”) for all three days after ceasing therapy. 10
These findings build on previous work that explored harms while on regular low-dose opioids for the symptomatic reduction of chronic breathlessness. 11 That systematic review and meta-analysis focused on people currently taking opioids. By looking at the three days immediately after ceasing opioids, we are in a better position to consider time-limited trials of regular, low-dose, sustained-release morphine for the symptomatic reduction of chronic breathlessness.
These data are consistent with the only other published placebo-controlled data on morphine for chronic breathlessness in a similar population. Johnson et al. reported SOWS data only on day 3 following cessation of 56 days of modified-release morphine or placebo (10 mg or 20 mg daily; morphine n = 73, placebo n = 67) as a secondary outcome. 12 They found no difference in those experiencing mild withdrawal symptoms, but a small excess of moderate/severe symptoms in those allocated to morphine (6/73 [8.2%] compared with 2/73 [2.7%]).
There is ongoing justifiable caution about the role of any opioids for breathlessness. 13 When regular, low-dose morphine forms part of individualized treatment plans for people with late-stage, life limiting illnesses (having properly explored nonpharmacological therapies), the carefully evaluated net effects of pharmacological therapy is the central consideration. Such net effects in people with moderate or severe breathlessness include both potential harms and potential benefits.5,14 In the light of this current study, a judicious trial of regular, sustained release morphine, starting at the lowest possible dose, can be done with quantified risks of symptoms of opioid withdrawal if the medication is ceased. Given that a three-week trial would see people at the maximum dose currently recommended for the reduction of chronic breathlessness, 15 no one in the group who ceased therapy in three weeks or less had severe symptoms of opioid withdrawal.
Strengths and limitations
Strengths include there was a blinded placebo arm to reflect the symptom burden in people who were not taking sustained-release morphine. Using a validated tool whose design required data recording on each of the first three days after ceasing morphine also makes this a unique study.
Limitations of this study include that the tool used was developed for people who were generally on much higher doses of opioids for much longer periods of time. As such, SOWS may not be nuanced sufficiently to pick up signals that are still important to patients. 16 SOWS was originally conceived with a companion assessment tool—the Objective Opioid Withdrawal Scale—which was not measured in the current study. 9 Although data were not available for 30 participants, the sub-population are similar in key characteristics to the whole study population, as was the distribution of the final doses of study medication. This study was not powered to assess individual symptoms, which would require a very large study given the prevalence and severity found in this study. SOWS was not filled out at study baseline, so some symptoms reported may have been there long-term.
Implications for research
There is a need for an international pharmacovigilance program to evaluate outcomes for people who are given a time-limited trial of regular, low-dose morphine for chronic breathlessness in advanced disease and choose to discontinue the therapy. This would provide the power to understand specific symptoms that may be more frequent or severe.
There are only a small number of tools that evaluate opioid withdrawal symptoms. One of these needs to be evaluated in detail and thresholds established for this hospice/palliative care population rather than for people ceasing longer-term, higher-dose opioids that have been used for other purposes.
Implications for clinical care
Implications for clinical care include that this study gives confidence that there are now data reflecting limited, transient harms in the days after ceasing <3 weeks of regular, low-dose, sustained-release morphine for chronic breathlessness. Most people had no clinically significant withdrawal symptoms. However, some people, irrespective of dose, experienced moderate or severe symptoms, with an indication that this is more likely in those taking morphine for longer than 3 weeks. Patients stopping morphine for chronic breathlessness should be warned about this risk and monitored accordingly.
In people who have exhausted nonpharmacological therapies, this study provides information that can inform clinicians’ and their patients’ shared decision-making as they consider a therapeutic trial of judiciously dosed and titrated morphine, knowing that they may need to cease the medication in the absence of net benefit.15,17
Use of artificial intelligence
The authors attest that no artificial intelligence was used to produce this article.
Footnotes
Author Disclosure Statement
D.C. declares intellectual property payments and advisory roles with Mayne Pharma International. All other authors declare no conflicting interests.
Funding Information
This study was funded by grant APP1065571from the National Health and Medical Research Council of Australia.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.