
Abstract
Background:
The Latino community is at high risk for developing dementia. Palliative care can support family caregivers of people living with dementia (PLWD).
Objectives:
To explore the experiences of New York City (NYC) Latino family caregivers of PLWD and identify implications for palliative care.
Design:
We conducted qualitative interviews from June to November 2024 with Latino family caregivers of PLWD. Caregivers were recruited from a single NYC health system. We asked open-ended questions exploring caregivers’ experiences with dementia, palliative care, and culture. Interviews were recorded, transcribed, and analyzed using thematic analysis with deductive and inductive coding.
Results:
Nineteen Latino family caregivers participated. Four interviews were conducted in Spanish and caregivers represented five countries of origin. We identified four themes related to palliative care for Latino family caregivers of PLWD. Caregivers Have a Limited Awareness of Palliative Care (Theme 1) was the backdrop of all other themes. Caregiving Is a Labor of Love (Theme 2) describes caregiving challenges, and Caregiving Is an Act of Strength and Resilience (Theme 3) describes how caregivers summarized their sources of support and needs. Integrating Cultural Values into Caregiving (Theme 4) provided a lens to better understand Latino caregivers’ unique experiences.
Conclusions:
Despite describing unmet needs, caregivers were not familiar with palliative care. In the presence of Latino cultural values, caregivers may underestimate all they do and not seek additional support. Palliative care should be introduced as a supportive service to equip families in taking care of their loved ones as they would want.
Key Message
This study described the Latino dementia family caregiver experience in New York City. Caregivers often underestimate their caregiving responsibilities and do not seek additional support. Our findings suggest potential solutions and implications for providing culture-centered palliative care, such as reframing palliative care for Latino communities.
Introduction
Dementia is a progressive, terminal illness that affects memory and the ability to perform activities of daily living; it causes significant challenges for people living with dementia (PLWD) and their caregivers.1,2 The integration of palliative care and dementia care for PLWD has been shown to improve symptom management3,4 and caregiver satisfaction. 3 Despite known benefits, most PLWD do not receive palliative care. 5
The prevalence of Latino PLWD in the United States is expected to increase by 175% by 2040 from 2018. 6 Latino family dementia caregivers often lack support in managing behavioral dementia symptoms 7 and are less likely to use formal care services.8,9 This has been attributed to a combination of cultural and structural factors, such as out-of-pocket costs 10 and availability of culturally concordant services. 11 To note, we use the term Latino throughout, as the traditional plural term for people with Latin American origins who reside in the United States. 12
The Latino community encompasses over 20 countries, with different lived experiences and phenotypic expression, which impact health outcomes. 13 Cultural, social, and structural factors should be considered when understanding the Latino experience with health care.14–16 For example, in a cross-cultural Latino study, Mexican caregivers were less knowledgeable about Alzheimer’s disease and would associate it with normal aging compared with Puerto Rican caregivers. 17 Latino cultural values also influence ongoing care decisions (e.g., nursing home placement). 18
Disparities in the use of palliative care have been documented in Latino nondementia populations,19,20 and Latino caregivers are underrepresented in dementia research. 21 In New York City (NYC), the population of Latino older adults doubled since 2000. 22 Latinos make up over half of the population of the Bronx, 23 a NYC borough which also has the highest prevalence of Alzheimer’s disease in the United States. 24 Therefore, we aimed to explore the experiences of Latino family caregivers of PLWD in NYC and implications for palliative care.
Methods
Study design and caregivers
Caregivers were recruited from the Mount Sinai Health System sites that provide outpatient dementia care in NYC. This study was approved by the Icahn School of Medicine at Mount Sinai Institutional Review Board.
Physicians (n = 37) in home-based primary care and geriatrics practices were approached to assist in identifying community-dwelling Latino patients with moderate to advanced dementia and to obtain permission to contact their family caregivers about study participation. Caregivers were eligible if they (1) were a family member of a PLWD; (2) were the primary person responsible for the care of the PLWD; (3) self-identified as Hispanic or Latino; and (4) were fluent in English or Spanish. Study recruitment began May 3, 2024, and was completed October 31, 2024.
Sampling and data collection
A chart review was conducted to confirm moderate to advanced dementia diagnosis, country of origin, preferred language, and caregiver contact information. We used purposeful sampling to approach potential caregivers, with the intention of balancing by country of origin. After two letters were sent describing the study and an opportunity to opt out, a bilingual research coordinator followed up by phone to invite caregivers to participate, answer questions, and schedule interviews. Of the 77 caregivers who were sent letters describing the study (65 referred from geriatrics practice, 12 referred from home-based primary care), 38 were reached by phone and 19 participated. Supplementary Table S1 provides detailed recruitment information. Verbal informed consent was obtained, and caregivers were compensated $30.00.
The interview guide was designed by L.V.E. and J.M.R. and guided by a modified culture-centered palliative care (CCPC) model.12,25 The modified CCPC12,25 characterizes cultural values (familismo, personalismo, respeto, confianza, and dignidad) that are meaningful in Latino populations and how they impact the delivery of palliative care.12,25 The interview guide included open-ended questions on experiences (see Interview Guide as Supplementary Table S2) related to dementia, palliative care, culture, and health care. It was pilot tested with two caregivers. Semi-structured interviews (lasting 30–45 minutes) were conducted either in-person, by telephone, or via video conference. L.V.E., a bilingual, Latina, PhD-trained registered nurse, conducted all interviews. Interviews were conducted in either English or Spanish, based on caregiver preference. Data collection continued until thematic saturation was reached. Analytic memos were completed following each interview to reflect on the data collected.
Data analysis
Interviews were digitally recorded, professionally transcribed and translated (for applicable Spanish interviews), and de-identified. Each transcript was verified for accuracy to the audio file by L.V.E. Interview data were analyzed using thematic analysis with a deductive and inductive approach. 26 First, a preliminary codebook was developed, informed by a review of transcripts, analytic memos, and domains assessed in the interview guide. L.V.E., J.M.R., and S.P. applied the preliminary codebook to two interviews and, after discussing each transcript and related codes, revised the codebook for content and clarity. L.V.E. and S.P. then independently coded the remaining transcripts and met weekly to review, refine existing codes, and define emergent codes as needed. The full research team met to discuss and interpret coded data, considering our own cultural biases during the analytic process. In addition, a community advisory board provided insights into data interpretation, which was incorporated into the final results. Qualitative coding and analysis were conducted using Dedoose. 27
Results
Table 1 describes caregiver (n = 19) and care recipient characteristics. The care recipients were mostly female (n = 15), on average 88 years old, born outside of the continental United States (n = 18), and immigrated to the United States before the age of 50 (n = 16). According to caregivers, Spanish was the preferred language among 89% of care recipients. Time since dementia diagnosis ranged from 1 to 18 years, although one caregiver was unsure if the participant had received a formal diagnosis.
Patient and Caregiver Characteristics (N = 19)

Is intended to provide more information on the notes. For “years of caregiving (in years)”, the range was 2-20 years but 2 people indicated “all my life”. For “Age emigrated to the continental United States”, 1 of the 3 was born in US but had grown up in the Dominican Republic.
N/A, not available.
Caregivers were mostly female (n = 15), daughters caring for a parent (n = 14), and were an average age of 65 years old. Caregivers’ country of origin included Bolivia (n = 1), Dominican Republic (n = 5), Ecuador (n = 1), Nicaragua (n = 1), and Puerto Rico (n = 12), reflective of the Latino older adult composition served by our NYC health system. Years of caregiving ranged from 2 to 20 years; however, two caregivers reported caring “all my life.” Most caregivers were born in the continental United States (n = 13) and preferred speaking English (n = 13). Most caregivers reported that they spoke Spanish with the patients (n = 12), and five caregivers reported speaking Spanglish, a mix of Spanish and English, with care recipients. Four interviews were conducted in Spanish.
We identified four themes. Caregivers Have a Limited Awareness of Palliative Care (Theme 1) was the backdrop of all other themes. Caregiving Is a Labor of Love (Theme 2) describes the dementia care challenges of the caregiver. Caregiving Is an Act of Strength and Resilience (Theme 3) describes how caregivers summarized their sources of support and needs. Integrating Latino Cultural Values into Caregiving (Theme 4) shaped the relationship between Themes 2 and 3 and included subthemes describing specific cultural values. Figure 1 illustratively demonstrates the relationship between themes.
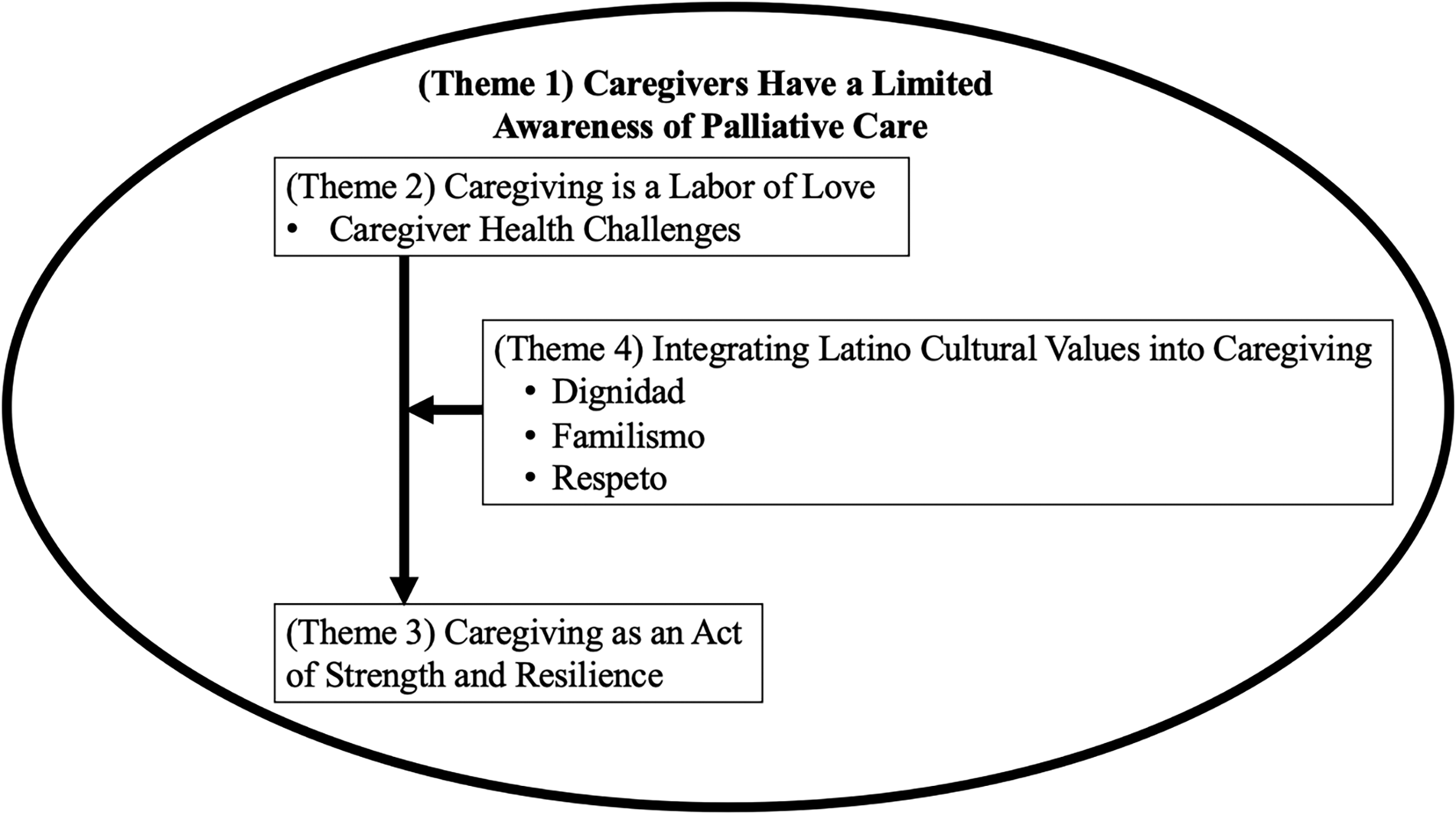
An illustrative description of the four identified themes with respective subthemes: (1) Caregivers Have a Limited Awareness of Palliative Care, (2) Caregiving Is a Labor of Love, (3) Caregiving Is an Act of Strength and Resilience, and (4) Integrating Latino Cultural Values into Caregiving, which helped explain Themes 2 and 3.
Theme 1: Caregivers Have a Limited Awareness of Palliative Care
While we aimed to explore caregivers’ palliative care needs, none of the caregivers interviewed knew what palliative care was, and some caregivers confused it with hospice (see Table 2). Caregivers spoke of their loved ones from a person-centered perspective, not defining them by their dementia diagnosis and were often hesitant to use the word dementia. Notably, after providing more information on palliative care as an additional supportive service, caregivers did not express interest in receiving palliative care.
Theme 1: Caregivers Have a Limited Awareness of Palliative Care

Theme 2: Caregiving Is a Labor of Love
Caregivers often expressed the toll caregiving took on them and the intensity of providing care (see Table 3). They performed many tasks ranging from, but not limited to, managing activities of daily living, ensuring safety at home, managing medical care and households, and advocacy. In addition, regardless of whether the participant had other family members assisting with the care, they expressed that caregiving responsibilities primarily fell on them. The average age of the caregivers interviewed was 65, and many expressed their own health challenges (subtheme 2a). Caregivers interviewed were cancer survivors, had scheduled surgeries or were recovering from surgeries, or history of heart attacks. One family caregiver described the physical toll of providing overnight care without support, saying that, regardless, it had to be done.
Theme 2: Caregiving Is a Labor of Love
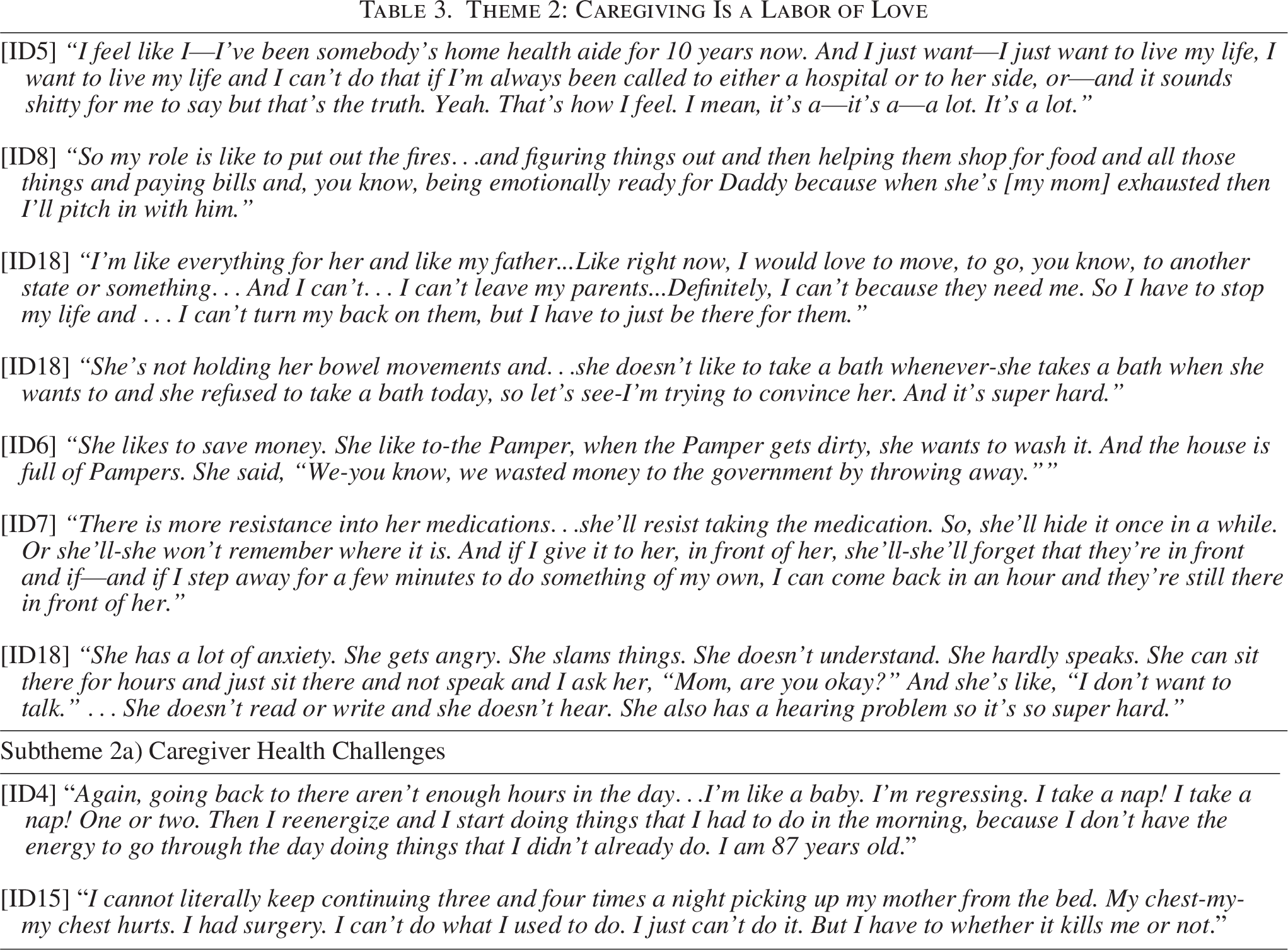
Yet even as caregivers described challenges of providing care and how it impacted them, they were hesitant to describe their role as burdensome. Caregivers described caregiving as a nonnegotiable responsibility. This led to a constant balance or negotiation between their own lives and caregiving expectations, whether real or perceived, of their loved one.
Subthemes were identified that provided further characterization of aspects of providing dementia care that shaped the caregiving experience. These were (2a) Caregiver Health Challenges and (2b) Dementia Symptoms.
Caregiver Health Challenges (subtheme 2a)
Caregivers shared challenges managing behavioral symptoms of dementia such as repetitive questioning, safety concerns (e.g., wandering, falls, and kitchen dangers), verbal aggression, and disrupted sleep due to nighttime agitation (subtheme 2b). They also struggled with patients’ delusions, difficulty recognizing loved ones, resistance to care such as bathing or taking medications, and behaviors such as discarding money, which added emotional and logistical burdens.
Caregivers were less likely to frame functional limitations or disabilities related to dementia from a medical or disease framework. For example, when asked if the patient needed help walking, the caregiver would not mention any issues walking but then later that they would use a walker or be nearly bedbound. One participant did not mention bathroom issues at first but later revealed that the care recipient uses incontinence garments.
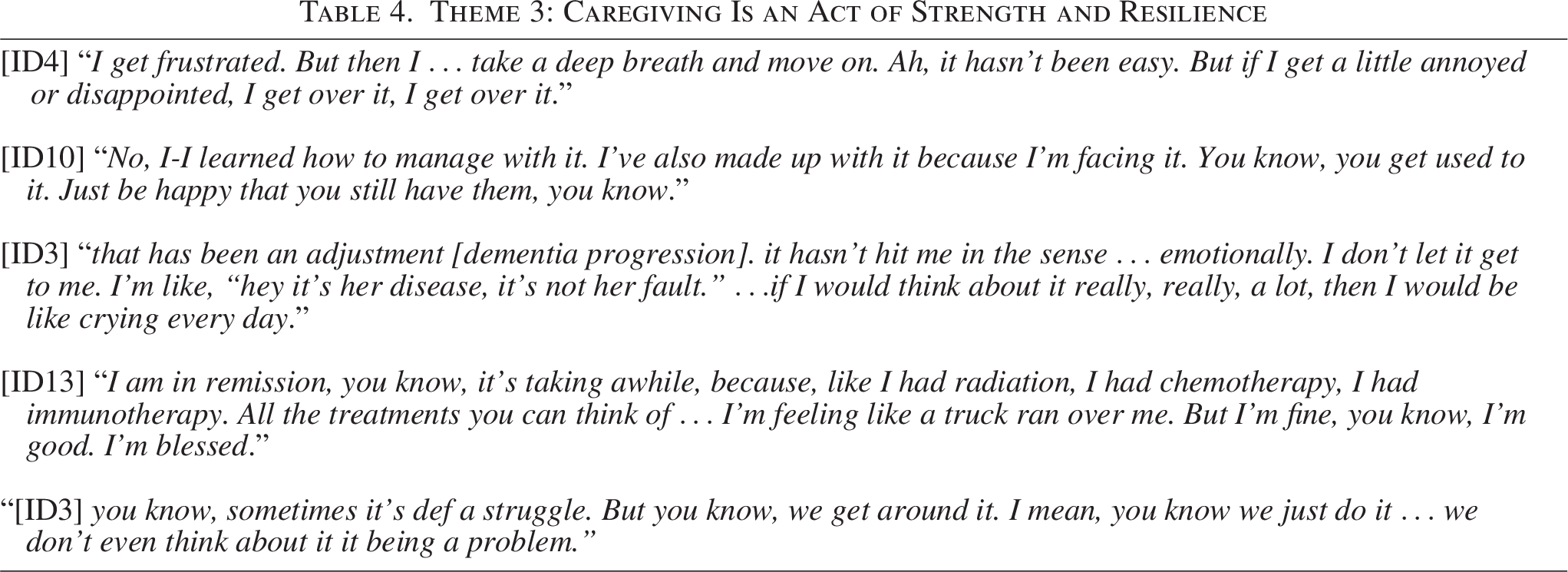
Theme 3: Caregiving Is an Act of Strength and Resilience
While caregivers shared daily caregiving stressors, they demonstrated a high threshold of what they were able to handle. Many caregivers expressed a sense of optimism and an emphasis on patience, taking things “one day at a time.” Coping and support systems were mentioned that helped them in caring for their loved ones and managing their own lives. They shared how, despite their daily life challenges, they were thankful to have their loved ones with them. Indeed, caregivers shared positive outlooks and response to adversity both personally and with their care recipient, which exhibited strength and resilience (see Table 4).
Theme 3: Caregiving Is an Act of Strength and Resilience
Theme 4: Integrating Latino Cultural Values into Caregiving
Latino cultural values (Theme 4) helped explain why caregivers demonstrated a high threshold of what they could handle (Theme 3), despite the toll of caregiving (Theme 2). Latino cultural values also helped explain their attitudes about seeking additional help in caregiving (e.g., nursing home and home health aides). Indeed, caregivers exercised their agency to ensure their loved ones received the best care, which they consistently believed could be best provided by them.
Although the CCPC12,25 includes five Latino cultural values, in our interviews, we identified three and include them as subthemes: (4a) dignidad, (4b) familismo, and (4c) respeto (see Table 5). We aimed to get a diverse Latino sample of family caregivers to learn about the subcultural differences; however, these themes were similar regardless of country of origin.
Theme 4: Integrating Latino Cultural Values into Caregiving: “We don’t give up people. We don’t put [our loved ones] in nursing home …[We were not] brought up like that.” (ID 11)
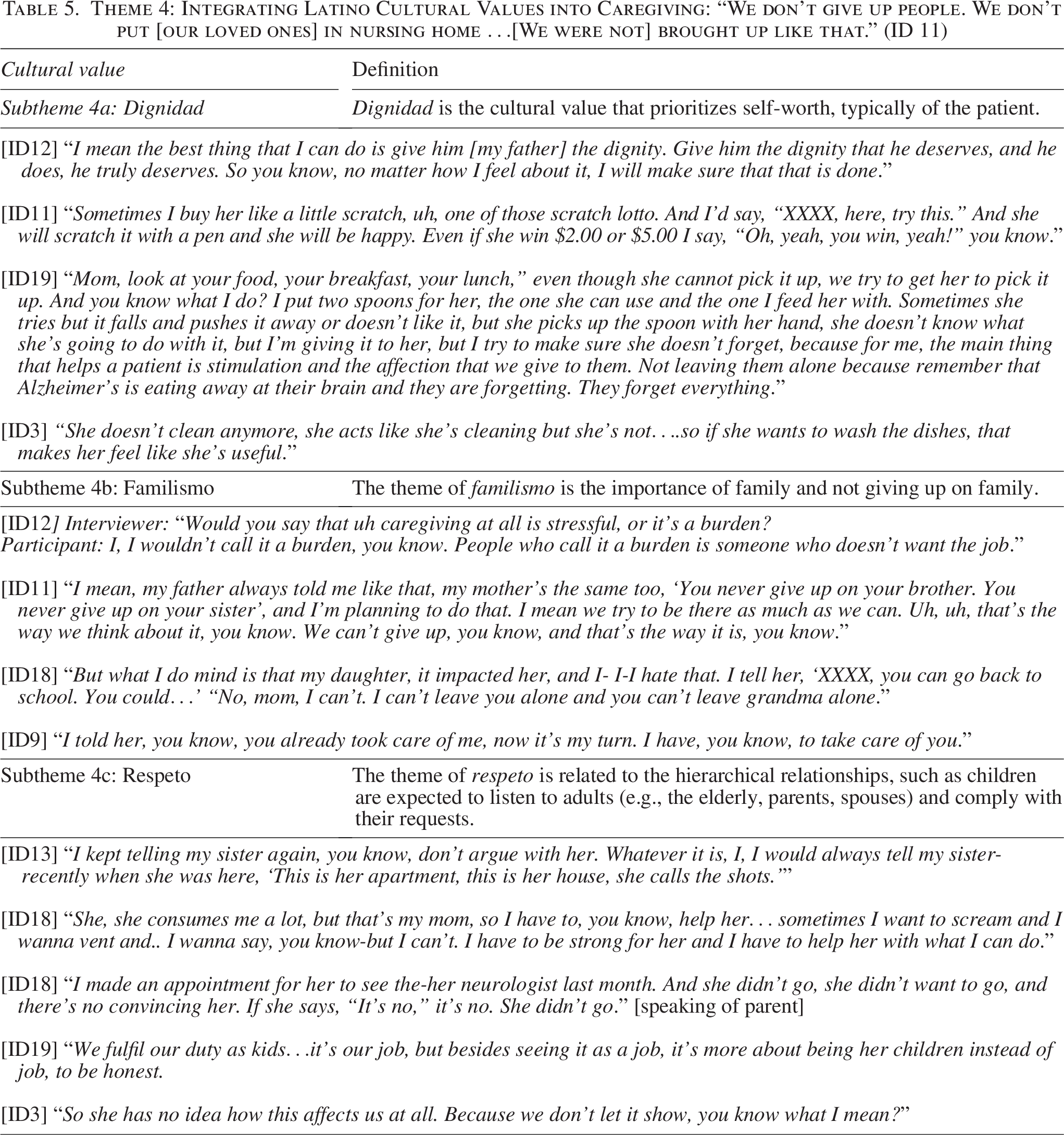
Dignidad (subtheme 4a)
Caregivers emphasized the importance of dignidad in daily caregiving, often maintaining a high standard of personhood despite the challenges of dementia (subtheme 4a). This included supporting the care recipient’s physical appearance—such as daily shaving, dressing up, or visits to the nail and hair salon. Dignidad was also reflected in allowing their loved ones to continue doing tasks like washing dishes, making coffee, or feeding themselves—whether they were fully capable or not—in order to support their sense of worth and independence.
Familismo (subtheme 4b)
Familismo was expressed as spending time together and preference for care provided by family members themselves before seeking other help (subtheme 4b). Caregivers were very involved in every aspect of care from supervising and training home health aides to ensuring small details like new Christmas decorations every year were in place for their loved one. Caring for their loved one was expected and a way to give back. Caregivers honored the family ties that united them and often shared how sometimes the most important thing they did was to be present and keep their family member engaged. This was sometimes difficult, and one caregiver spoke of the guilt they felt after their child moved back home from college to help the caregiver and the care recipient. Despite this tension, most expressed how their loved one would deteriorate faster if it was not for them keeping them from going to a nursing home. Indeed, there was nothing they would not do and no sacrifice large enough for their loved one.
Respeto (subtheme 4c)
Caregivers alluded to respeto in having a high tolerance for dementia symptoms and respecting the hierarchal nature of child and parent relationships (subtheme 4c). Even in the presence of severe dementia, deference to parents was still present. For example, more than one family mentioned how they did not have home health aides because the care recipient did not want aides. Another mentioned how their parent needed hearing aids but refused to wear them, and there was no way to get them to put them on. Many shared how they would not argue with their parent with dementia and tried to respect their desires no matter what. Caregivers were sympathetic with what their loved ones were going through and made efforts to not upset them, including avoiding arguments.
Discussion
In this study exploring the palliative and dementia care needs of Latino family caregivers in NYC, we found that caregivers were not familiar with palliative care. Despite describing aspects of caregiving that would be amenable to palliative care, caregivers did not express interest and often prioritized their loved one’s well-being over their own. Latino cultural values (dignidad, familismo, and respeto) helped explain the perspective of our Latino family caregiver participants. Our findings suggest implications to provide palliative care for Latino communities.
The Latino cultural values of dignidad, familismo, and respeto shaped our caregivers’ experiences and expectations. Previous studies have found that familismo has led to the underuse of health care services. 28 For example, Latino older adults are less likely to reside in long-term care facilities,16,29 similar to our findings where caregivers believed the best care was provided by them at home. Latino older adults have higher rates of disability, 30 which may increase caregiver responsibilities and speaks to our high threshold for what constitutes too much caregiving. Familismo may vary based on acculturation and has been referred to as a negotiation of cultural values and expectations among different generations.31,32 However, we found that the collective culture of familismo and ties to the family were present when discussing caregiving among all caregivers. While dignidad, familismo, and respeto are universally valued in caregiving, given the diversity of the Latino community, caregivers interpret and apply these values uniquely.
Similar to the general public, the Latino caregivers we interviewed were not familiar with palliative care. Only 12.6% of respondents from a 2018 nationally representative survey knew what palliative care was. 33 Educational efforts are needed to make sure Latino family caregivers and PLWD know that palliative care can be consistent with their cultural values and support the family in taking care of their loved ones as they would want. In other words, palliative care supports the concepts of dignidad, familismo, and respeto. Palliative care educational materials should emphasize Latino cultural norms, remaining cognizant about structural issues that may impact palliative care delivery (e.g., availability of palliative care and previous experiences with health care).
Classical clinical language in medical appointments may not be relatable for Latino family caregivers and PLWD. In our interviews, caregivers were hesitant to describe caregiving as challenging or burdensome, language typically used in palliative care,34,35 which may not appropriately assess their needs. Although Latino caregivers are more likely to report that their role gives them a sense of purpose, it often exists with feelings of tension of stress. 36 In a survey of dementia caregivers nationwide, they reported wanting greater support from health care professionals, yet less than half (44%) are asked what they need to provide care or much less about their own self-care needs (24%). 37 Previous research has also found that Latino family caregivers want information on dementia risk factors and progression. 38 Palliative care outreach should consider these factors, acknowledging language, family dynamics, and caregiving purpose.
At the policy level, structural barriers to palliative care services should be addressed. The National Strategy to Support Family Caregivers 39 has brought attention to supporting family caregivers to address these barriers. The introduction of the Caregiver Training Services (CTS) Codes in the 2024 Medicare Physician Fee Schedule 40 is one example of efforts to acknowledge this. The CTS Codes are training strategies and techniques for caregivers of persons with chronic health conditions, disability or functional limitation. Additionally, the Center for Medicare and Medicaid Innovation’s Guiding an Improved Dementia Experience (GUIDE) Model is a new alternative payment method for dementia care management to support PLWD and their caregivers. 41 GUIDE could potentially increase palliative care access for those who need it. Time will tell how effective these policy initiatives are at improving accessibility to caregivers.
This study has limitations. First, our sample was limited to Latino family caregivers in NYC. Given the diversity of the Latino community, we do not intend to overgeneralize our findings from NYC to all Latino dementia family caregivers. Second, although we aimed to get a subcultural diverse Latino sample, none of our caregivers were recent immigrants. Third, we recruited caregivers of care recipients who had moderate to advanced dementia; therefore, we do not know if those with mild dementia may be more receptive to palliative care. Last, although four authors identify as Latino, cultural biases may always influence interpretations in qualitative work.
In conclusion, we sought to explore the palliative care needs for Latino family caregivers of PLWD in NYC. Family caregivers were not familiar with palliative care, although their experiences appeared amenable to palliative care. While certain elements of caregiving are universal among all dementia caregivers, it was particularly embedded in our sample because of the values of dignidad, familismo, and respeto. Framing palliative care as a supportive service to equip families in taking care of their loved ones as they would want may help make it more likely for Latino family caregivers of PLWD to accept and benefit from palliative care services at home.
Authors’ Contributions
L.V.E. and J.M.R. conceived the idea and design for this article. L.V.E. collected the data for the article. L.V.E., J.M.R., and S.P.-G. analyzed the data. L.V.E., S.P.-G., A.L.S., N.E.G., Y.M., and J.M.R. interpreted the data, drafted the article, performed revisions, and contributed their expertise in the area.
Footnotes
Acknowledgments
All authors meet the criteria for authorship stated in the Uniform Requirements for Manuscripts Submitted to Biomedical Journals. The authors would like to thank the study participants for sharing their experiences and Jessy Mera and Alexander O’Donnell for their assistance with recruitment and data collection.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
L.V.E. was supported by a grant from the Robert Wood Johnson Foundation, Harold Amos Medical Faculty Development Program. J.M.R. was supported by the National Institute of Health/National Institute on Aging (K23AG066930). The funders had no role in the design, methods, subject recruitment, data collection, analysis, or preparation of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.