
Abstract
Background:
Patients with advanced brain tumors often experience dysphagia and excessive drooling, leading to respiratory complications and a reduced quality of life. We evaluated the clinical utility of transdermal scopolamine (TS) in pediatric patients with brain tumors.
Methods:
A 5.0% scopolamine ointment was prepared in-house and applied once daily to the mastoid regions behind the ears.
Results:
Five patients (four children and one adolescent) with brain tumors received TS treatment. All patients had low Lansky/Karnofsky performance status scores, ranging from 20 to 40. Within two weeks of treatment, four patients showed objective improvements, including reduced suctioning and oxygen requirements and alleviation of respiratory symptoms. No severe or unexpected adverse events related to TS were observed. Four patients were able to transition to home-based care.
Conclusions:
The findings of this study suggest that TS may be a safe and effective option for managing salivation in this population.
Introduction
Dysphagia is a common symptom of advanced brain tumors and impairs the ability to swallow saliva, leading to recurrent respiratory complications. In addition, frequent airway suctioning may cause trauma, hypoxemia, and considerable discomfort, further compromising the patient’s quality of life (QOL), complicating home care, and prolonging hospitalization.
To manage dysphagia, excessive drooling, and the associated respiratory problems, various interventions, including pharmacological therapy and botulinum toxin injections, can be considered in clinical practice.1,2 Among the pharmacological options, oral and intravenous anticholinergic agents, such as atropine sulfate, glycopyrrolate, scopolamine (hyoscine) hydrobromide, scopolamine butylbromide, and the newly available propantheline bromide, are used to reduce salivation.3,4 However, these agents often cause non-negligible systemic adverse effects, which raise concerns about their use, particularly in pediatric patients with serious underlying conditions and poor performance status (PS). Moreover, their availability is limited or subject to periodic shortages in Japan. Topical formulations and transdermal therapeutic systems (TTS) of scopolamine reportedly provide targeted effects with fewer systemic adverse reactions.5,6 While these agents have demonstrated utility in patients with neurodegenerative disorders, stroke, or severe motor and intellectual disabilities, their safety and efficacy in pediatric patients with brain tumors remain largely unknown.7–12
Caring for patients with advanced brain tumors is particularly challenging due to the rapid progression of symptoms. At the same time, transitioning to home-based care is often a crucial goal shared by patients and their families. Given these needs, we evaluated the safety and efficacy of transdermal scopolamine (TS) ointment applied to the mastoid region, in combination with other supportive interventions, in pediatric and adolescent patients with advanced brain tumors and poor PS.
Methods
A 5.0% scopolamine ointment was prepared in-house by mixing scopolamine hydrobromide with a hydrophilic ointment base. As the standard initial dosing regimen, a small amount (approximately 0.1 g per site) was applied once daily to the bilateral mastoid regions behind the ears and then covered with a small adhesive patch, irrespective of age or body weight, as previously described. 9 Dose adjustments were made as needed, based on treatment response and observed adverse effects. Efficacy was evaluated within two weeks based on reductions in suctioning frequency and oxygen requirements, as documented in medical records, as well as clinical assessments of patient distress conducted by health care providers. Outpatient follow-up after discharge was principally scheduled at intervals of several weeks, tailored to each patient’s clinical status. The treatment and this study were approved by the Institutional Review Board of Tokyo Metropolitan Children’s Medical Center. Written informed consent was obtained from the patients’ guardians.
Results
Between April 2022 and December 2024, five patients (two males and three females), including four children and one adolescent, with brain tumors received TS at the study center (Table 1). The median age at TS initiation was 9 years (range: 1–17). The cohort included two patients with recurrent, progressive medulloblastoma, two with intractable pontine diffuse midline glioma, and one with newly diagnosed metastatic brainstem ependymoma complicated by intratumoral hemorrhage. All patients had low Lansky/Karnofsky PS scores ranging from 20 to 40. Four patients were being managed as outpatients before experiencing neurological deterioration. All five developed excessive drooling related to their primary disease, which led to dyspnea and complicated clinical management.
Baseline Characteristics and Subsequent Clinical Courses of Patients Treated with Transdermal Scopolamine

“†” indicates that the verbal response could not be assessed due to tracheostomy.
aGlasgow Coma Scale components: Eye (E), Verbal (V), and Motor (M).
DMG, diffuse midline glioma; PD, progressive disease.
The median interval between diagnosis and initiation of TS was 25 months (range: 1–37). Two patients received TS in combination with low-pressure continuous oral suctioning. Three were supported with high-flow nasal cannula (HFNC) therapy, and one had a tracheostomy without mechanical ventilation. None received additional pharmacologic treatments targeting salivation. Within two weeks of TS initiation, improvements in respiratory symptoms were observed in four patients, including desaturation episodes, oxygen dependence, and suctioning frequency (Figs. 1A–D). In the remaining patient (patient 5), the effects of TS could not be assessed due to rapid clinical deterioration and early death. Relief of distress, as evaluated by health care providers, appeared to have been achieved in the same four cases. The clinical courses of three patients (patients 1, 3, and 4) are shown in Figures 1B–D. Although TS was considered effective, detailed data were not available for patient 2 due to early transition to home-based care following treatment initiation.
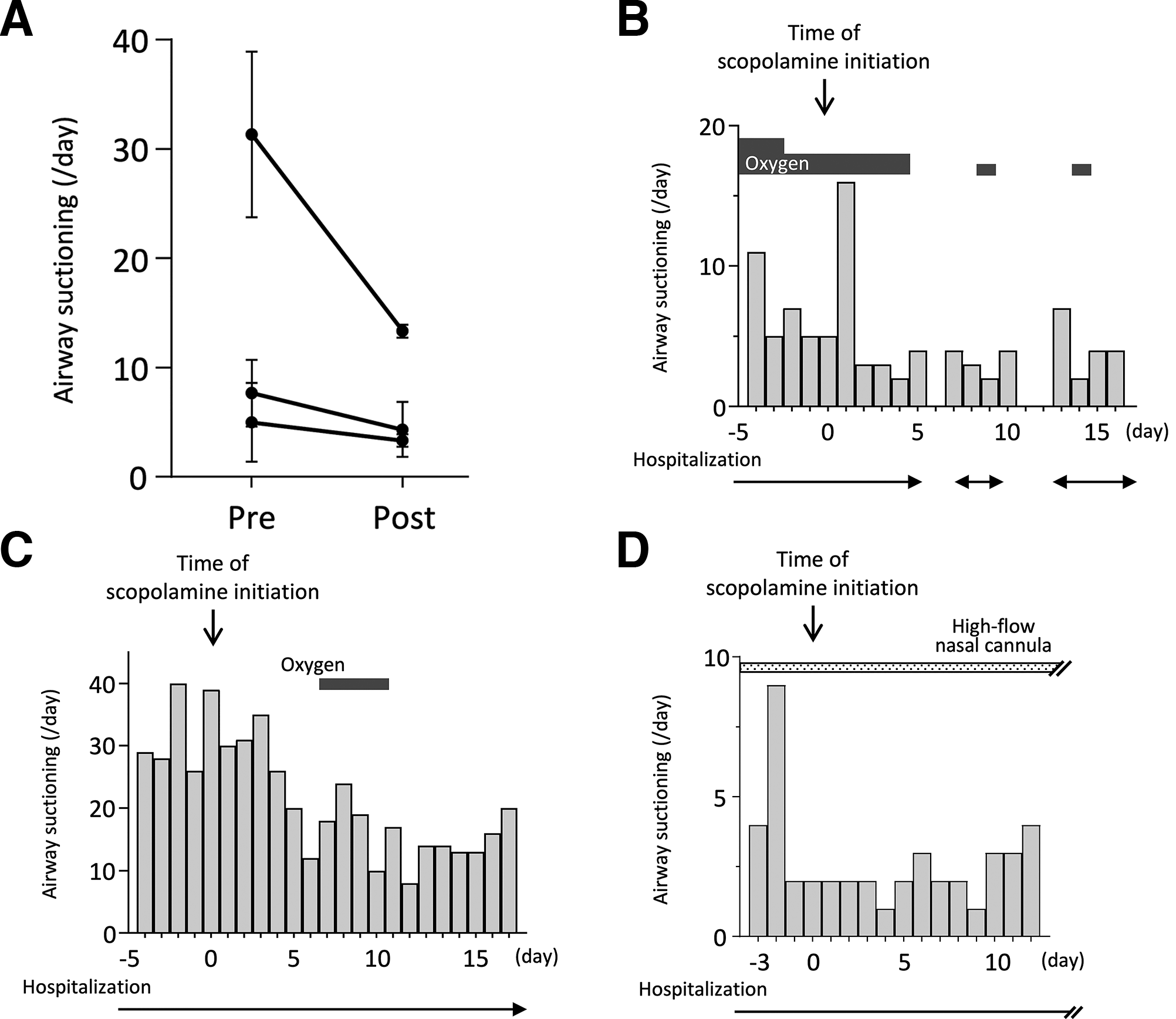
Clinical courses of three representative patients.
From a safety perspective, no severe or unexpected adverse events related to TS occurred in any of the patients during the treatment period. No dose adjustments were required. Four patients were able to transition to home-based care within 1–40 days. Ultimately, four patients died from their primary disease, while one remained on first-line chemotherapy at the time of the final follow-up.
Discussion
The TTS of scopolamine has been used as a long-acting prophylactic antiemetic, initially developed for motion sickness and subsequently applied for the prevention of postoperative nausea and vomiting. Its efficacy and general safety have been supported by randomized controlled trials and systematic reviews.13–15 Early studies have also demonstrated its potential to reduce salivary flow and manage drooling.10,11,16,17 However, as of this report, commercial TTS formulations containing scopolamine remain unavailable in Japan, necessitating the use of an in-house prepared ointment, as previously described. 9
Commercial TTS patches, each containing 1.5 mg of scopolamine, reportedly deliver 1 mg of the drug over 3 days. 18 In contrast, our ointment contained approximately 5 mg per site (0.1 g of a 5.0% preparation), potentially resulting in a higher overall dosage. However, direct comparisons of dosage are difficult without considering differences in transdermal absorption. A recent study in rats demonstrated that the efficacy and systemic absorption of TS varied depending on the application site, such as the skin above or behind the salivary glands. 19 These findings highlight the need for further research to determine the optimal application site, dosage, and drug concentration.
Adverse effects of TS may include dry mouth, decreased sweating, urinary retention, constipation, mydriasis, and other ophthalmological complications. 3 In addition, a recent U.S. Food and Drug Administration safety warning cited the risk of hyperthermia. 20 Central nervous system effects, such as drowsiness, agitation, disorientation, hallucination, and confusion, may also occur. Although no clinically significant adverse effects were observed in our cohort, the findings should be interpreted with caution. Several reports have described such events as frequent.3,12 However, in this study, the small number of patients and the presence of severe neurological impairment and poor PS made it inherently difficult to assess adverse effects systematically. Moreover, central nervous system-related symptoms may overlap with those of tumor progression, making it challenging to distinguish drug-related toxicity from the underlying disease. Therefore, the absence of observed toxicity in our cohort does not exclude the possibility of clinically relevant adverse events.
In our patients with advanced brain tumors and dysphagia, the application of TS appeared to reduce salivation and alleviate respiratory distress, thereby improving patient comfort. Following TS administration, four patients who had previously required frequent suctioning and hospitalization were able to transition to home-based care. The use of TS helped control salivation and reduced caregiver burden, contributing to smoother home care management. Notably, our experience suggests that TS can be safely administered in an out-of-hospital setting.
Alternative approaches to managing excessive salivations, such as intraparotid botulinum toxin injections or surgical salivary gland removal, are invasive and irreversible, making them less suitable for children with brain tumors, especially in palliative care settings. Moreover, these interventions are not standard practice in Japan. HFNC therapy has reportedly improved swallowing in adult patients; however, its efficacy in pediatric patients with severe neurological impairment remains uncertain, although a few of our patients may have benefited from this approach. 21 Other supportive strategies, such as low-pressure continuous oral suctioning and fluid restriction, were also employed alongside TS in several of our cases. These noninvasive and generally well-tolerated interventions are particularly appropriate for end-of-life care. Ultimately, TS administration and adjunctive measures should be tailored to each patient’s clinical condition, the availability of home care resources, and, most importantly, the preferences of the patient and their family.
Our study has several limitations. The limited number of patients precluded statistical analysis to assess the efficacy of TS. The retrospective design and, in two cases, early events (such as death or transition to home-based care) hindered the collection of comprehensive data on clinical responses and detailed QOL measures. Although the use of a validated survey to assess distress relief and QOL would have been desirable, this was scarcely feasible in the context of the present study. Nevertheless, one of the primary goals was to alleviate intractable symptoms and honor the wishes of terminally ill patients and their families, which we believe was achieved through TS treatment.
In conclusion, we presented a case series of five pediatric and adolescent patients with advanced brain tumors complicated by dysphagia and respiratory problems who were treated with TS. This is the first report to describe its clinical utility in pediatric oncology. In our experience, TS was a safe and effective intervention when used in combination with other conventional supportive care measures. Notably, TS administration has the potential to facilitate the transition to home-based care, thereby improving patients’ QOL. Further studies are warranted to optimize TS therapy and to confirm its clinical utility in larger pediatric populations.
Authors’ Contributions
K.S. treated the patients, conducted the research, collected and interpreted the data, and wrote the article. M.M. and M.S. treated the patients and collected the data. N.M. treated the patients, collected and interpreted the data, and supervised the research. All the authors critically reviewed and approved the final version of the article.
Footnotes
Acknowledgments
The authors would like to thank the patients and their families who made this research possible. They would also like to thank Ms. Tomoko Kagawa and Ms. Rie Ayuta for their valuable contributions and Mr. James Robert Valera for his assistance with editing this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
None.