
Abstract
Introduction:
Dyspnea is a common and distressing symptom in patients with cancer, particularly in advanced stages and lung cancer. It is associated with poor quality of life and is often challenging to manage. The Respiratory Distress Observation Scale (RDOS) is a validated tool for assessing dyspnea in noncommunicative patients.
Objectives:
To assess the validity of the RDOS by comparing it with patient-reported dyspnea using the revised Edmonton Symptom Assessment System (ESAS-r) in patients with cancer receiving palliative care (PC), and to explore associations with functional status.
Design:
Observational, cross-sectional study.
Setting/Subjects:
The study was conducted at the National Cancer Institute (INCan) in Mexico City from October 2022 to February 2023. A total of 194 adult cancer patients with dyspnea receiving PC were included.
Measurements:
RDOS, ESAS-r, and Karnofsky Performance Status (KPS) scores were assessed. Analyses included Spearman’s correlation and comparisons across KPS groups.
Results:
Median RDOS score was 5 (interquartile range 3–9), with 36.1% experiencing severe dyspnea. Higher RDOS scores were observed in patients with KPS ≤40. RDOS scores correlated significantly with ESAS-r dyspnea, insomnia, and drowsiness. Agreement between RDOS and ESAS-r was higher in moderate/severe cases (79.08%) than in none/mild (63.41%). Notably, 36.59% of patients rated as mild by ESAS-r were classified as moderate/severe by RDOS.
Conclusion:
RDOS is a valuable tool for detecting respiratory distress in cancer patients unable to self-report. Early identification and comprehensive management of dyspnea are crucial, particularly in patients with compromised functional status, or advanced disease, and those vulnerable to undetection because of inability to self-report distress.
Key Message
The RDOS is a practical and reliable tool for identifying respiratory distress in cancer patients unable to self-report. Its correlation with symptom burden and functional decline supports its integration into PC to improve early detection and management of dyspnea in vulnerable patient populations.
Introduction
Dyspnea, defined as a subjective experience of breathing discomfort with varying intensities that patients can describe, 1 is a common symptom in patients with advanced cancer, with a prevalence ranging from 10% to 70%. This symptom not only causes significant suffering but also tends to worsen over the course of the disease, becoming more challenging to manage compared with other symptoms. 2 Dyspnea is particularly prevalent in patients with lung cancer and those in advanced stages of the disease.3–5 It is often refractory to available palliative treatments, which may necessitate measures such as palliative sedation. 6 Its negative impact extends to both patients and their caregivers, reducing quality of life and limiting daily activities.7,8 Furthermore, dyspnea is a strong predictor of mortality and can be useful in predicting the clinical course of patients.9,10
The causes of dyspnea can be directly or indirectly related to cancer, as well as to antineoplastic treatments and other comorbidities. It may result from conditions such as lung neoplasms, end-stage lung disease, renal, hepatic, and cardiac disorders, or pneumonia. 11 Although self-reported dyspnea remains the standard for its assessment, in patients who are unable to communicate or who have cognitive impairment, alternative evaluation tools are necessary. In patients nearing the end of life, decreased consciousness and cognitive function can complicate the assessment of dyspnea.12,13
Respiratory distress not only affects the physical well-being of patients but is also correlated with a decline in their functional status. This decline may manifest as a reduced ability to perform daily activities, which, in turn, can exacerbate other symptoms such as fatigue, depression, and anxiety. These interactions can create a cycle in which increased respiratory distress contributes to further functional decline and heightened intensity of other symptoms. 5 Identifying these correlations is essential for a comprehensive approach to managing dyspnea and its secondary effects.
The Respiratory Distress Observation Scale (RDOS) (Table 1), developed by Campbell et al., is a recognized tool for assessing dyspnea in noncommunicative patients at the end of life.12,14 Cutoff points have been established to classify respiratory distress as mild, moderate, or severe, enhancing its clinical utility. 15
The Respiratory Distress Observation Scale
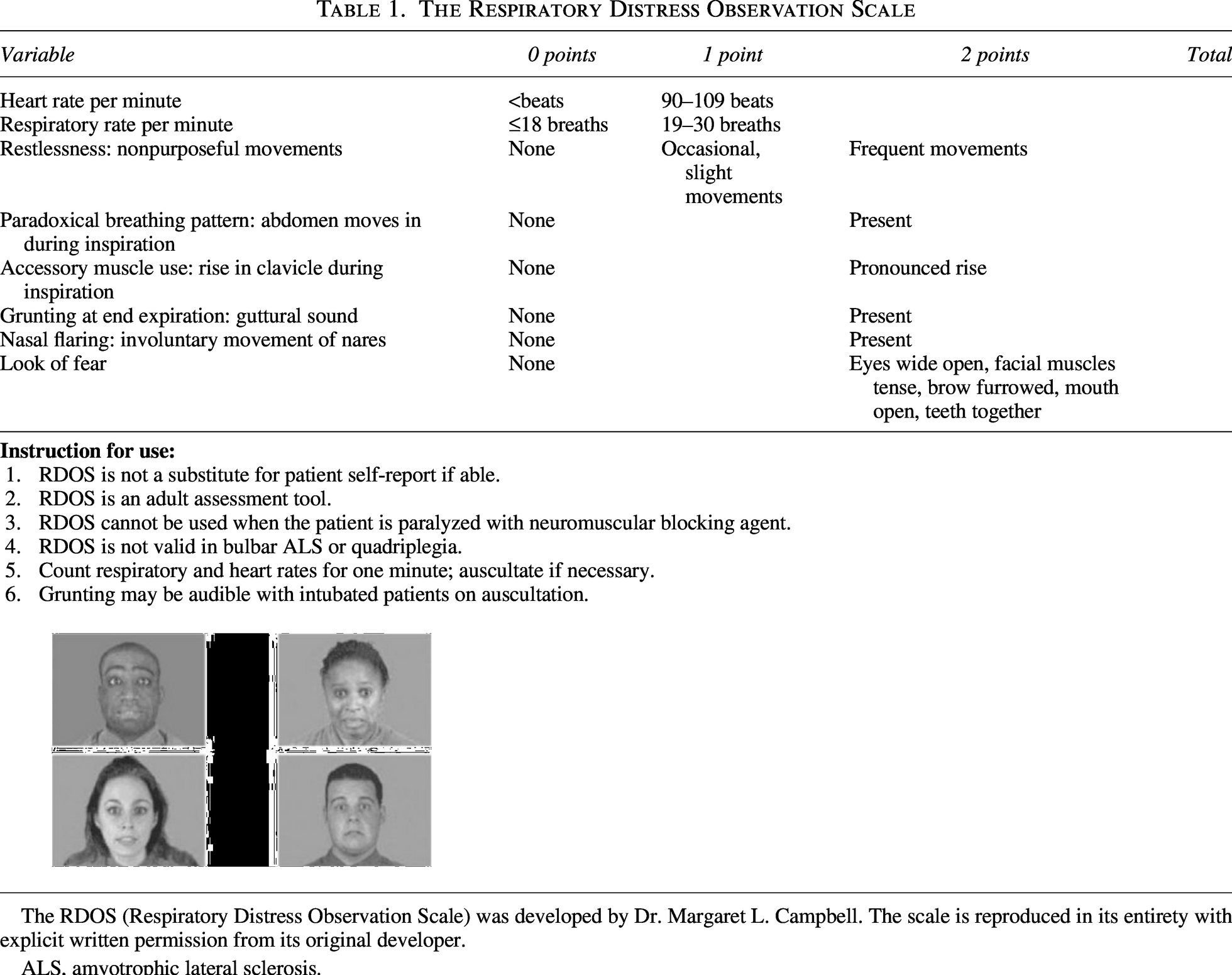
The RDOS (Respiratory Distress Observation Scale) was developed by Dr. Margaret L. Campbell. The scale is reproduced in its entirety with explicit written permission from its original developer.
ALS, amyotrophic lateral sclerosis.
This study aims to replicate the validity between RDOS scores and symptoms assessed using the revised Edmonton Symptom Assessment System (ESAS-r) in patients with cancer admitted to palliative care (PC) services. Additionally, it seeks to determine differences in RDOS scores based on varying levels of functional status.
Materials and Methods
Study design and settings
This was a single-center, cross-sectional, observational study conducted in the PC service of a tertiary care hospital—the National Cancer Institute (INCan) in Mexico City—between October 2022 and February 2023. INCan is a national referral center with 188 beds dedicated to cancer care and provides services to approximately 7300 patients annually. Patients were eligible to participate if they met all the following criteria: (1) age 18 years or older; (2) a cancer diagnosis; (3) reported any degree of dyspnea according to the ESAS-r; and (4) were receiving care in the outpatient clinic, emergency room, or were hospitalized. Patients were identified through three clinical settings: hospitalization wards, the emergency room, and the outpatient clinic. They were recruited through (a) PC consultations specifically requested for dyspnea management; (b) routine outpatient follow-up visits where dyspnea was identified via ESAS-r; and (c) daily rounds in hospitalization areas where any level of dyspnea was reported. Patients were recruited consecutively during the study period, based on eligibility criteria, without a predefined sample size calculation, given the observational and exploratory nature of the study. Patients diagnosed with bulbar amyotrophic lateral sclerosis or quadriplegia, those receiving neuromuscular blocking agents, and those admitted to the intensive care unit were excluded as RDOS is not valid in these conditions, or under invasive mechanical ventilation because the ESAS-r is difficult to obtain from the study.
Revised Edmonton Symptom Assessment System
The ESAS-r is a validated, patient-reported tool used to assess both the presence and severity of 10 cancer-related symptoms: pain, fatigue, drowsiness, nausea, loss of appetite, shortness of breath (dyspnea), depression, anxiety, insomnia, and overall well-being. 16 Each symptom is rated on an 11-point scale, ranging from 0 (no symptoms) to 10 (the most severe symptoms). The ESAS-r was routinely administered to all patients included in the study as part of the standard clinical assessment. In cases where patients presented with severe dyspnea, the symptom was first stabilized by providing supplemental oxygen. Once the patient was clinically stable, they were asked to rate the intensity of their dyspnea, showing them a chart as indicated in Figure 1.
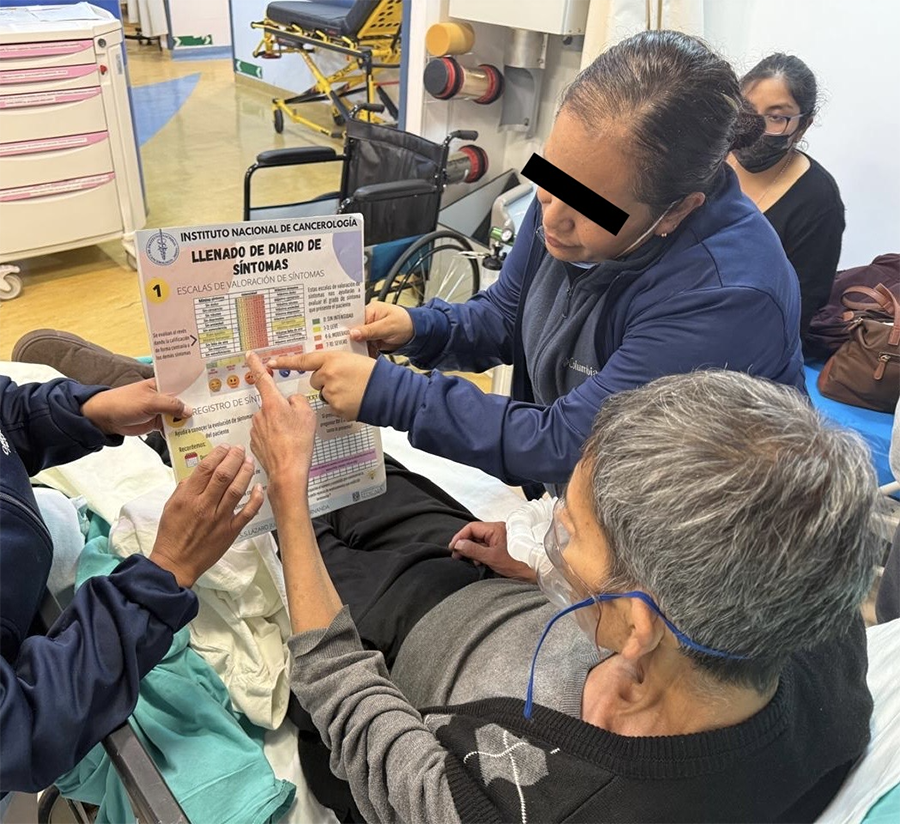
Patient assessment of dyspnea severity using the revised Edmonton Symptom Assessment System (ESAS-r) with nursing staff support. A patient indicates the severity of dyspnea on the ESAS-r scale, assisted by nursing staff, highlighting the collaborative evaluation process.
Respiratory distress assessment
The RDOS, developed by Campbell et al., is an eight-item ordinal scale designed to assess the presence and severity of respiratory distress in nonverbal patients, a common condition near the end of life. 12 Each item is scored from 0 to 2 points, with the total score ranging from 0 to 16. The established cutoff points are as follows: 0–2 points indicate no distress; 3 points indicate mild distress; 4–6 points indicate moderate distress; and 7 or more points indicate severe distress. 15 The RDOS has been validated in PC patients with cancer. 17 The RDOS score was administered to all patients by a trained physician.
Ethical considerations
This study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki. The research protocol was approved by the Ethics and Research Committee of INCan (approval numbers: CEI/049/22 and 022/038/CPI, respectively). All patients were provided with detailed information about the study and gave their written informed consent.
Statistical analysis
Data are reported as absolute and relative frequencies for all categorical variables, and as mean (standard deviation) or median (interquartile range [IQR]) for continuous variables. Normality was assessed using graphical methods and the Kolmogorov–Smirnov test. Continuous variables were analyzed using the T test and Kruskal–Wallis test, and categorical variables were compared using the chi-square test or Fisher’s exact test. Spearman’s correlation test was employed to evaluate the relationship between RDOS and ESAS-r scores. The strength of the correlation was categorized as follows based on the correlation coefficient: <0.3 indicating a weak relationship, 0.30–0.50 a moderate relationship, and >0.50 a strong relationship. 18 No data imputation was performed. Statistical significance was defined as a p value <0.05. Analyses were conducted using R version 4.2.2 (R for Statistical Computing, Vienna, Austria).
Results
A total of 194 patients were included in the final analysis. The characteristics of the participants are summarized in Table 2. The mean age of the participants was 54.9 ± 16.2 years, with 63.4% being women. The most prevalent cancer type was breast cancer (25.8%), followed by genitourinary/gynecological cancer (19.1%) and lung cancer (17.0%). Among the total sample, 67.5% had stage IV cancer, while 21.6% had stage III cancer. Lung metastases were present in 56.2% of the patients, and 21.1% had bone metastases. Regarding marital status, 39.7% of patients were married, 22.2% were single, 11.3% were cohabiting, and 26.8% were widowed or divorced. In terms of educational attainment, 7.7% of participants were illiterate, 30.9% had completed elementary school, 26.3% had a middle school education, 18.6% had completed high school or technical education, and 16.5% had a university or postgraduate degree. The median and IQR of the ESAS-r symptom scores for all participants are presented in Table 3.
Sociodemographic Characteristics of the Sample According to Dyspnea Severity
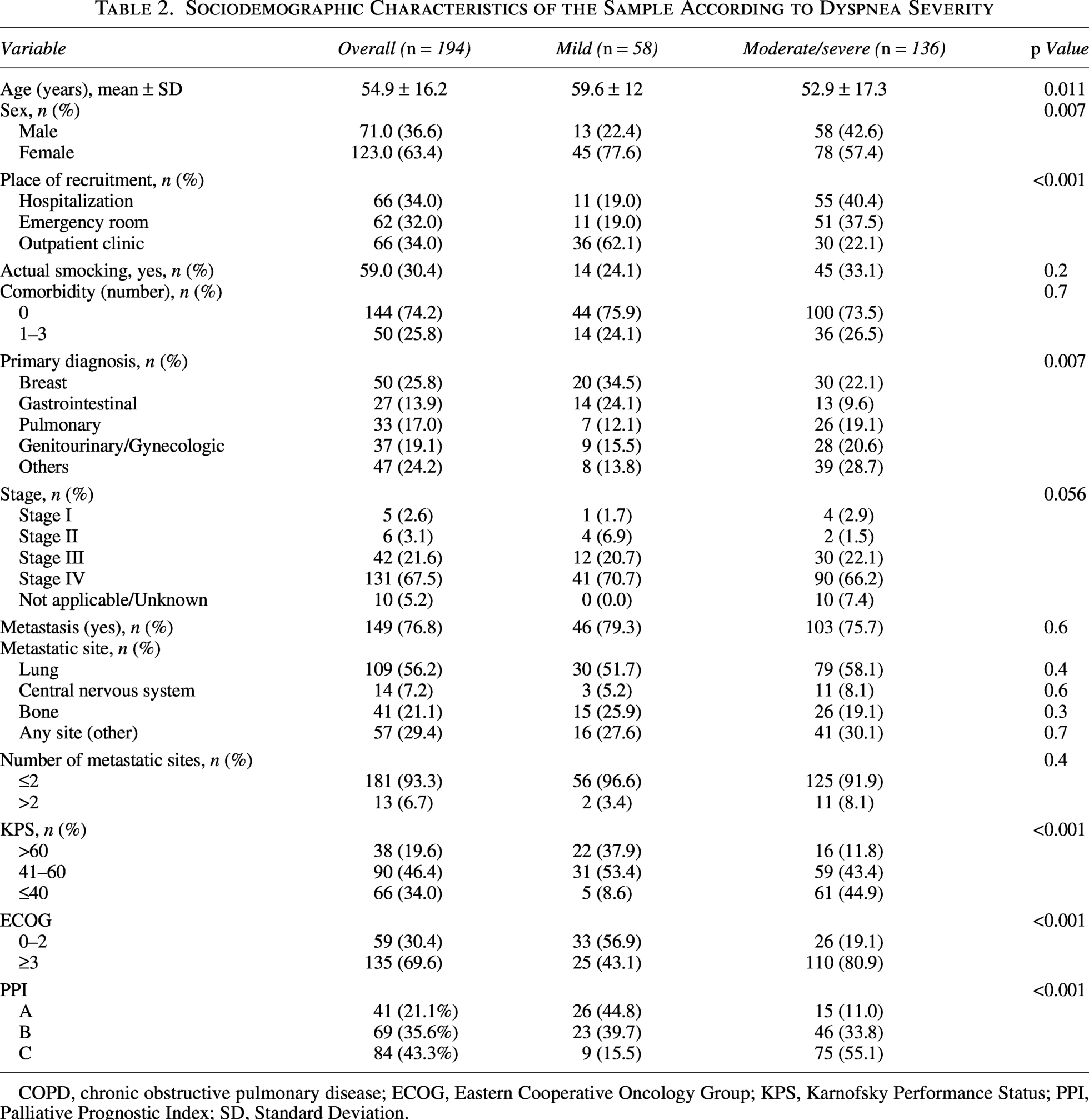
COPD, chronic obstructive pulmonary disease; ECOG, Eastern Cooperative Oncology Group; KPS, Karnofsky Performance Status; PPI, Palliative Prognostic Index; SD, Standard Deviation.
Median and Interquartile Range of Revised Edmonton Symptom Assessment System Symptoms
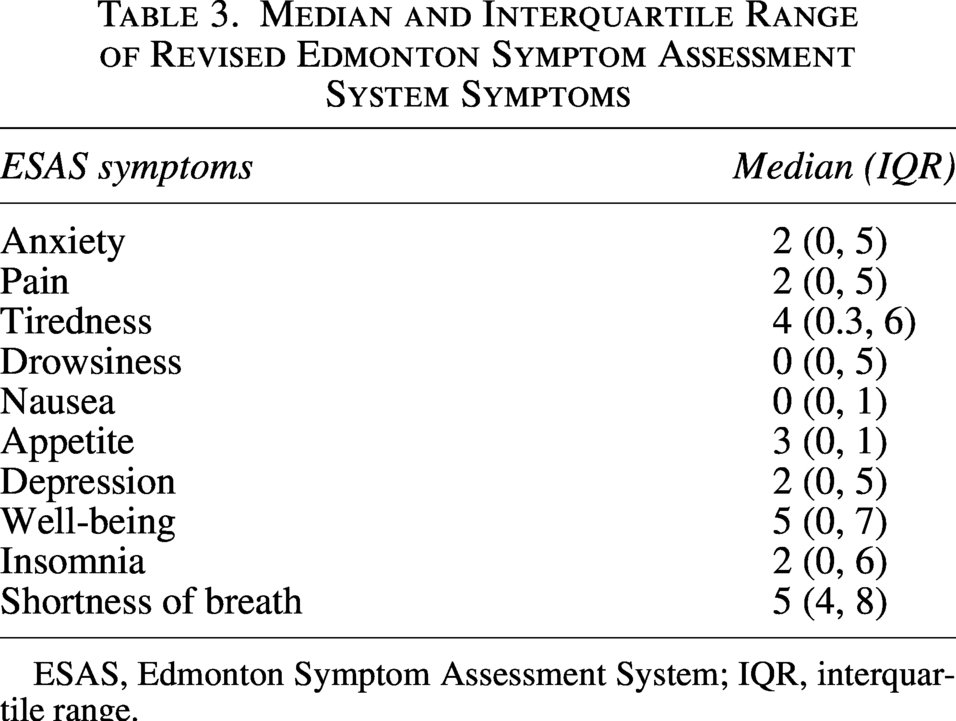
ESAS, Edmonton Symptom Assessment System; IQR, interquartile range.
Severity of dyspnea
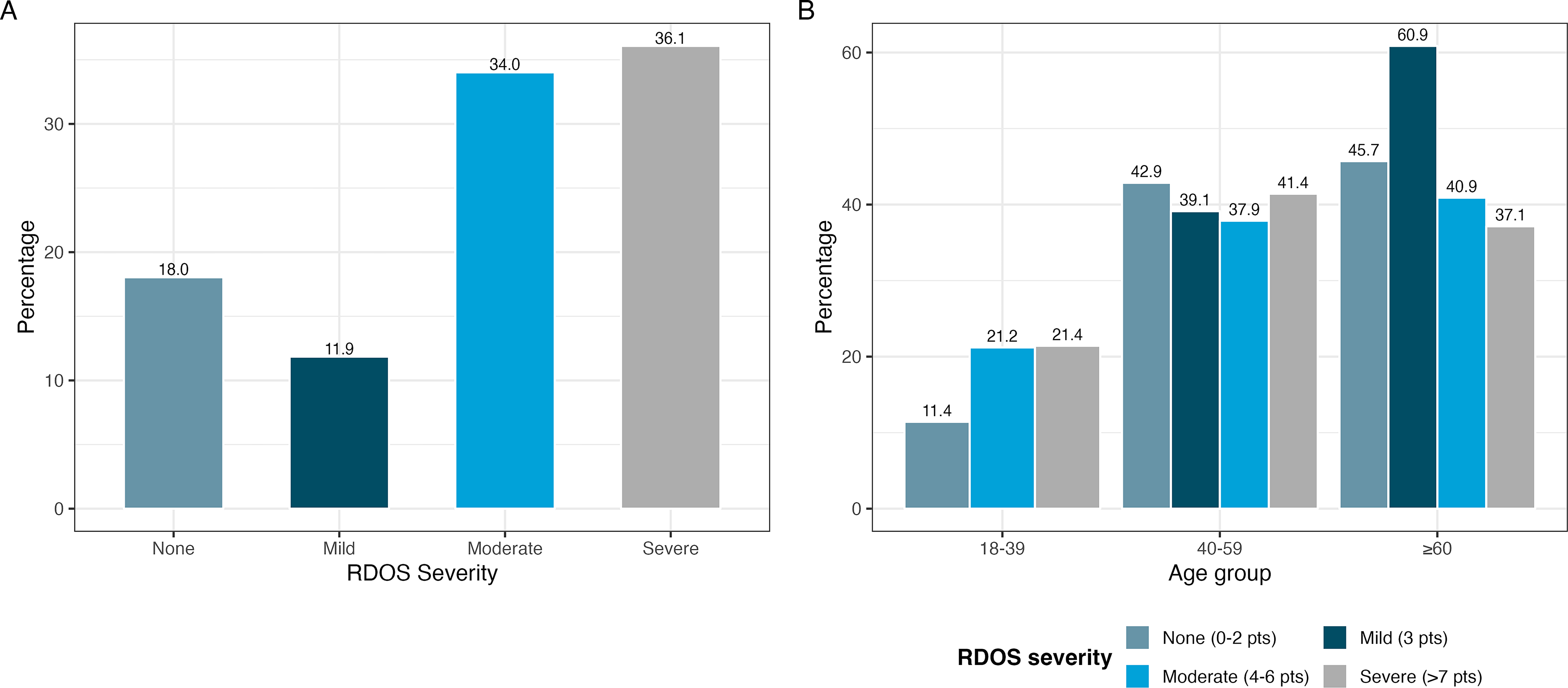
The median RDOS score was 5 (IQR 3–9). According to the RDOS score, 18.0% (n = 35) of patients did not experience dyspnea, 11.9% (n = 23) had mild dyspnea, 34.0% (n = 66) had moderate dyspnea, and 36.1% (n = 70) had severe dyspnea (Fig. 2A). We found that among patients with lung cancer, 19.1% experienced moderate/severe dyspnea, while 66.2% of patients with moderate/severe dyspnea had stage IV cancer (Table 1). In patients aged 40–59 years, the prevalence of severe dyspnea was 41.4%, compared with 37.1% in patients aged 60 years or older (Fig. 2B).
RDOS scores according to performance status
We assessed the difference between RDOS scores and Karnofsky Performance Status (KPS). The median RDOS scores showed significant variation across the three KPS groups (≤40, 41–60, and >60), with the highest scores observed in patients with a KPS ≤40 (Fig. 3).
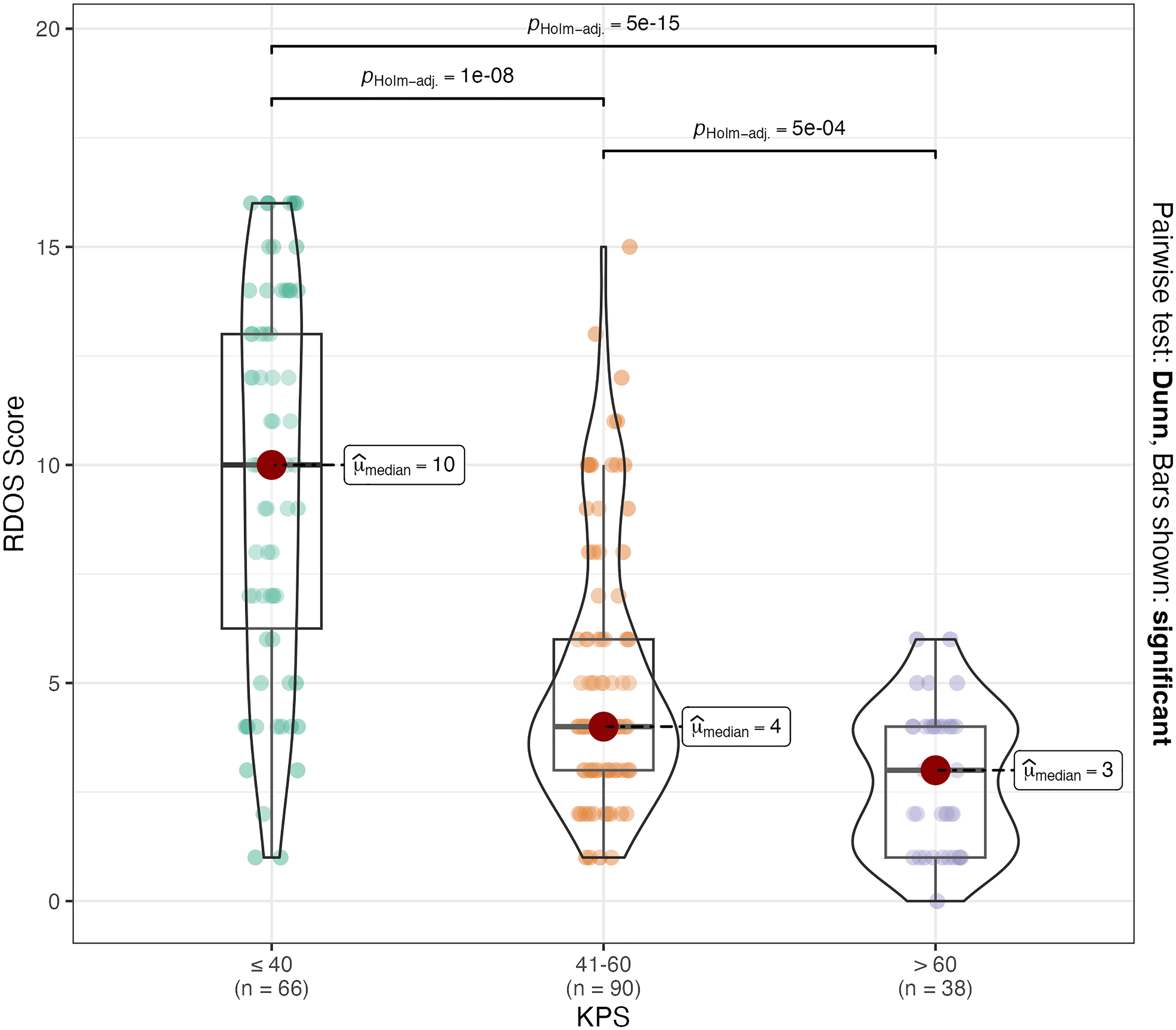
Median RDOS scores across KPS groups. KPS, Karnofsky Performance Status.
Correlation between RDOS score and ESAS-r symptoms
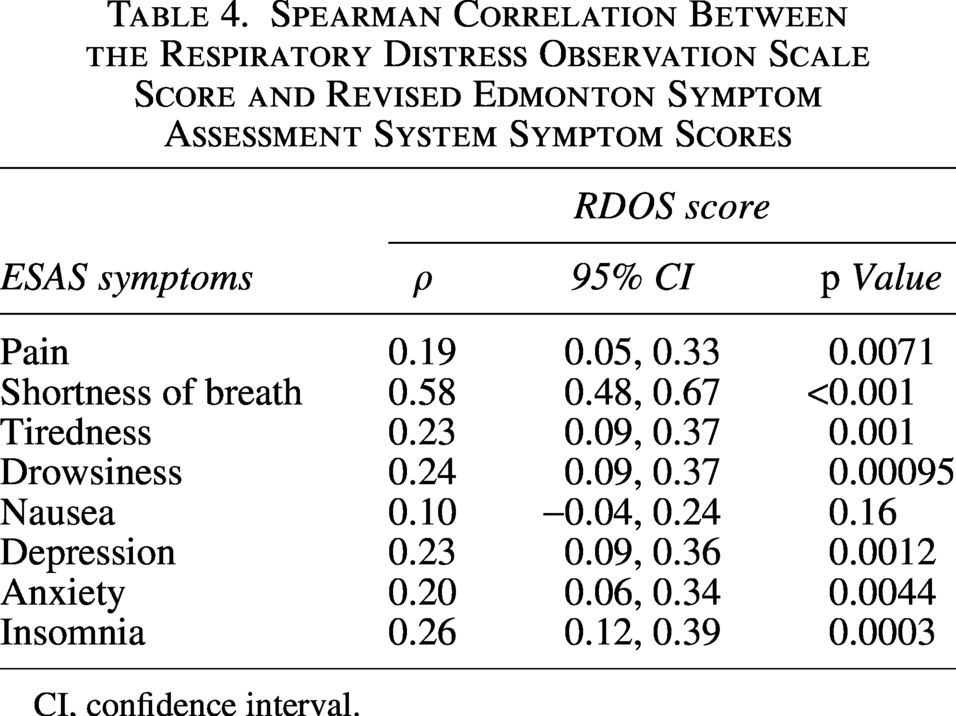
We observed a positive correlation between the RDOS score and ESAS symptoms, with the strongest association found with the ESAS-dyspnea (rho = 0.58, 95% confidence interval [CI]: 0.48, 0.67, p < 0.001). This was followed by insomnia (rho = 0.26, 95% CI: 0.12, 0.39, p = 0.0003) and drowsiness (rho = 0.24, 95% CI: 0.09, 0.37, p = 0.00095). No significant correlation was found with nausea (rho = 0.24, 95% CI: −0.04, 0.24, p = 0.16) (Table 4). Additionally, we classified dyspnea assessed by ESAS-r into two categories: mild (0–3 points) and moderate/severe (4–10 points), to evaluate its agreement with the RDOS classification. As no patient achieved a score of 0, the mild category effectively represents the 1–3 point range. The agreement between ESAS-r and RDOS classifications was higher in patients with moderate/severe symptoms (79.08%) than in those with mild (63.41%). However, significant discrepancies were observed: 36.59% of patients classified as mild by ESAS-r were categorized as moderate/severe by RDOS, while 20.92% of patients with moderate/severe symptoms according to ESAS-r were classified as none/mild by RDOS.
Spearman Correlation Between the Respiratory Distress Observation Scale Score and Revised Edmonton Symptom Assessment System Symptom Scores
CI, confidence interval.
Discussion
To our knowledge, this is the first study in Mexico to assess respiratory distress using the RDOS score in patients with cancer receiving PC. In this observational study, we examined the correlation between RDOS scores and symptoms measured by the ESAS-r scale in oncology patients admitted to the PC service. We found positive correlations between RDOS scores and symptoms, except for nausea. Additionally, we observed that patients with a KPS score of 40 or lower had higher RDOS scores.
In our study, we found that the prevalence of severe respiratory distress reached 36.1%, with breast cancer patients being the most affected by moderate-to-severe dyspnea, at 22.1%. However, patients with primary lung metastases showed a higher prevalence of moderate-to-severe respiratory distress, at 58.1%. Dyspnea is a common symptom in patients with advanced cancer. 19 Multiple factors can contribute to the development of dyspnea in breast cancer patients, including anemia, acidosis, bronchospasm, pneumonia, atrial fibrillation, congestive heart failure, and pleural effusions, among others. 20 Additionally, several antineoplastic agents used in breast cancer treatment can induce pulmonary toxicity. For example, dyspnea has been reported in up to 16% of patients treated with Eribulin and up to 25% of those receiving Gemcitabine. 21
In our analysis, we found that severe dyspnea was slightly more prevalent in patients aged 40–59 years compared with those aged 60 years or older (41.4% vs. 37.1%, respectively). Younger patients with terminal cancer tend to experience greater psychosocial distress, which may lead to elevated levels of anxiety, depression, and sleep disturbances, further contributing to respiratory distress. 22
We also identified that patients with a KPS of 40 or lower had higher RDOS scores. This finding is consistent with multicenter studies conducted in Japan, Taiwan, and Korea, which used observational tools to assess dyspnea in terminally ill patients. 23 In these studies, dyspnea was evaluated through structured interviews asking patients directly about the presence or absence of symptoms, including dyspnea. When verbal communication was not possible, physicians assessed symptoms by proxy based on clinical observation. Similarly, Ekström et al. reported a comparable trend using the ESAS scale in multicenter cohorts across Europe, Australia, and Canada. 4 Research such as that by Pilegaard et al. has shown that dyspnea negatively impacts the ability to perform daily activities and is associated with other symptoms such as pain and fatigue. 24 Dyspnea can also trigger anxiety and fear of movement, known as kinesiophobia, which in turn can impair physical performance and quality of life. In our study, a positive correlation was also observed between RDOS scores and anxiety. Therefore, it is suggested that patients with compromised functional status undergo a comprehensive evaluation to identify risk factors associated with the development of dyspnea. 25
Additionally, we identified significant positive correlations between RDOS scores and several symptoms assessed using the ESAS-r, including pain, shortness of breath, drowsiness, depression, anxiety, and insomnia. However, no such correlation was observed with nausea, a finding consistent with other studies conducted on patients with advanced cancer.8,26 We observed that 36.59% of patients classified as mild by the ESAS-r were categorized as moderate/severe by the RDOS. This discrepancy highlights a critical clinical concern: the potential underestimation of symptom severity when relying solely on self-report tools like the ESAS-r, especially in patients who may be less able to accurately articulate their experience. The finding suggests that a significant subset of patients experiencing clinically relevant distress, as indicated by RDOS, may be perceived as having only mild symptoms if the evaluation depends solely on the ESAS-r. Hui et al. reported higher median ESAS-r scores than RDOS scores (medians of 5 vs. 3, respectively) in advanced cancer patients; however, it is important to consider that the scales differ in magnitude. 26 Crucially, the scales also differ in the timing and context of the dyspnea assessment: the ESAS-r evaluates dyspnea both at rest and during exertion (over the past 24 hours), whereas the RDOS measures dyspnea exclusively when patients are at rest at the time of evaluation. 26
The higher RDOS score in patients with “mild” ESAS-r scores could therefore be attributed to the RDOS’s ability to capture objective physiological distress (e.g., changes in vital signs or nonverbal variables) that the patients may not consciously perceive or articulate effectively, particularly when not exerting themselves. This underscores the complexity of evaluating dyspnea, reinforcing the American Thoracic Society’s definition of dyspnea as a “subjective experience” resulting from multiple complex interactions among physiological, psychological, social, and environmental factors. 1 Furthermore, our results reinforce the conclusion that both self-reported tools like the ESAS-r and observational tools such as the RDOS are essential for a comprehensive evaluation of dyspnea. They are not interchangeable but rather complement each other in capturing the multifaceted nature of this complex symptom, offering a more complete picture of the patient’s discomfort for informed clinical decision making.1,12,17
Most cancer patients experience symptoms, the prevalence and severity of which depend on the type of cancer, disease stage, antineoplastic treatments, and preexisting comorbidities. 27 Among patients with advanced cancer, pain is present in 35–96%, fatigue in 32%, and dyspnea in 10–70%. 27 It is common for patients to experience multiple symptoms simultaneously; those with metastatic cancer and respiratory difficulty, a symptom indicative of advanced disease, have been documented to present an average of 14 symptoms. 27 Dyspnea tends to intensify alongside other symptoms, such as anxiety, depression, fatigue, appetite changes, well-being, and pain. It also worsens in the presence of lung metastases or in patients with impaired functional status, as observed in our study. 28 Since many of these symptoms can be induced by antineoplastic therapies, optimal management requires a thorough evaluation that includes the patient’s premorbid status, early identification of dyspnea through the ESAS-r, current treatment, and a deep understanding of the disease course. 20
Limitations and strengths
This study has several limitations that must be considered when interpreting the results. First, it is a cross-sectional observational study, which prevents the establishment of causal relationships. Additionally, the lack of data on patients’ lifestyle factors, such as alcohol consumption, physical activity, and nutritional and hydration status, limits the understanding of how these factors may influence the course of dyspnea. It is also important to note that certain clinical conditions, such as pulmonary infections, anemia, pleural effusions, pulmonary embolism, prior chest radiotherapy, and the use of specific chemotherapeutic agents like bleomycin, among others, may affect the experience of dyspnea. Furthermore, as a single-center study, the results may not be generalizable to other populations or clinical contexts.
Despite these limitations, the study also has several strengths. First, the inclusion of a significant sample of cancer patients allows for better representation of the affected population. Additionally, the use of the RDOS tool provides a standardized assessment of respiratory distress, facilitating comparisons with other studies. The collection of data on multiple symptoms and their relationship with dyspnea offers a comprehensive view of the patients’ clinical situation. Moreover, the findings can contribute to identifying critical areas for future interventions, thereby improving care and quality of life for cancer patients.
Conclusions
Our results show that the prevalence of severe respiratory distress was 36.1%, with breast cancer patients and those with lung metastases being the most affected. Additionally, we found a positive correlation between RDOS scores and symptoms such as pain, anxiety, depression, and drowsiness, as measured by the ESAS-r scale, highlighting the multifactorial nature of dyspnea and its interaction with other symptoms in cancer patients. These findings underscore the importance of evaluating factors such as age, cancer type, the presence of metastases, and functional status in the management of dyspnea.
Despite the study’s design limitations and the lack of data on lifestyle factors and specific clinical conditions, this study demonstrates the utility of the RDOS for assessing respiratory distress in the context of oncological PC. The results emphasize the need for early detection and comprehensive management of dyspnea, particularly in patients with compromised functional status or identified risk factors. Future research should adopt a longitudinal and multicenter approach to further explore the factors influencing dyspnea, with the aim of improving care and quality of life for patients with advanced cancer.
Authors’ Contributions
S.A.-P.: Conceptualization, methodology, supervision, and writing—review and editing. M.C.: Validation and writing—review and editing. A.L.S.R.: Supervision and writing—review and editing. J.J.C.-S.: Data curation, formal analysis, methodology, and writing—review and editing. O.M.T.T.: Investigation, methodology, and writing—review and editing. E.A.M.C.: Supervision and writing—review and editing. P.C.-G.: Resources, supervision, and project administration.
Footnotes
Acknowledgment
The authors thank Neolpharma S.A. de C.V. for providing a research grant in support of PC research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.