
Abstract
Background:
Hospice care has expanded significantly in recent decades; however, few studies have systematically examined how research themes in this field have evolved over time.
Objectives:
This study aimed to explore the temporal dynamics of hospice care research using topic modeling, identifying emerging and declining areas of focus.
Methods:
A total of 14,862 hospice-related articles published up to April 2025 were retrieved from PubMed. Topic modeling analysis was conducted using Latent Dirichlet Allocation to extract thematic structures across the corpus. The optimal number of topics was determined using perplexity, the elbow method, and coherence scores. Temporal trends were assessed across four stages defined by major World Health Organization milestones: the (1) Foundation (≤2001), (2) Expansion (2002–2013), (3) Institutionalization (2014–2019), and (4) Post-pandemic Transition (2020–2025) periods.
Results:
Ten major research topics were identified, including caregiver support, advance care planning, access to hospice care, and mortality trends. Topic prevalence shifted over time, with increased attention to caregiver support and advance care planning during the Expansion and Institutionalization periods and heightened focus on access to care and mortality trends during the Post-pandemic Transition period.
Conclusion:
Hospice research has shifted from foundational and conceptual inquiries to more applied and policy-oriented themes. The findings reflect the field’s growing institutionalization and underscore the need for sustained research targeting underserved areas to promote equity and responsiveness in end-of-life care.
Keywords
Key Message
This study highlights how hospice research has shifted in response to evolving societal needs. The findings offer researchers, clinicians, and policymakers valuable insight into how scholarly focus aligns with changing care priorities, while also identifying underexplored areas to guide future research.
Introduction
Hospice care has become a vital element of global health systems, especially amid efforts to uphold dignity and quality of life at the end of life. It refers to a specialized care model that prioritizes comfort over cure for individuals with terminal illnesses. 1 Although closely related to palliative care, hospice represents a more time-bound approach, focused on the terminal stage. 1 As discourse and policy around palliative care have advanced, hospice has grown increasingly institutionalized and integrated into national health systems.2,3 Hospice care is delivered through a multidisciplinary team that provides coordinated services such as pain management, psychosocial support, spiritual care, and bereavement services for both patients and their families.1,4,5 This comprehensive approach has been linked to improved quality of life and lower levels of anxiety and depression among patients at the end of life.6,7
The institutional development of hospice has evolved alongside shifts in research priorities. The modern hospice movement began in 1967 with the founding of St. Christopher’s Hospice in London by Dame Cicely Saunders, who introduced the concept of “total pain”—a holistic model addressing physical, emotional, social, and spiritual suffering. 8 The movement expanded to the United States with the establishment of Connecticut Hospice in 1974 9 and gained further momentum with the creation of the Medicare hospice benefit in 1982, which enabled public funding for services. 10 In 2002, the World Health Organization (WHO) redefined palliative care to include all life-threatening illnesses, extending its scope beyond cancer.11,12 This shift allowed hospice services to reach more diverse patient populations.13,14 A major development followed in 2014 with the Global Atlas of Palliative Care at the End of Life, which reframed hospice and palliative care as global public health and human rights priorities, emphasizing the need for national strategies and legal frameworks for service integration.2,15 Around this time, Advance Care Planning (ACP) gained broader policy and legal recognition as reimbursement systems evolved to protect patients’ rights to express preferences for end-of-life care. 16 These milestones signaled a period of policy-driven institutionalization. More recently, the COVID-19 pandemic, declared by WHO in 2020, 17 exposed disparities in hospice access and accelerated the adoption of telehealth and decentralized, community-based care models.18,19 This post-pandemic era marks a transformative phase in hospice delivery and accessibility.
Understanding these historical transitions is critical for grasping hospice care’s evolving role and identifying future directions. Its trajectory has not been uniform; instead, it has been shaped by cultural, clinical, and policy dynamics that differ across regions and time. To enable meaningful global comparisons, consistent temporal markers reflecting institutional change are needed. In this context, the publication of key WHO reports in 2002, 2014, and 2020 serves as globally relevant turning points that delineate distinct phases in the evolution of hospice care.2,11,17 These milestones offer a coherent framework for temporal segmentation, allowing researchers to analyze how hospice research has responded to shifting global priorities.
Despite these major developments, few studies have systematically examined how hospice-related research themes have evolved in response to broader transitions. As global health agendas increasingly prioritize aging populations, equity, and innovation, there is a growing need to contextualize the evolution of hospice discourse over time. Although numerous systematic reviews and empirical studies have addressed specific aspects of hospice care,20,21 data-driven analyses tracing how research themes have shifted in response to historical and institutional change remain limited. Given the growing emphasis on high-quality end-of-life care in achieving a “good death,” hospice must continue adapting to the complex needs of patients and families. To support this evolution, a comprehensive understanding of the thematic trends shaping the field is essential.
To address this gap, this study applied Latent Dirichlet Allocation (LDA) topic modeling to abstracts of hospice research published over the past several decades. Text mining effectively synthesizes large bodies of literature and identifies latent themes. In particular, LDA enables the detection of research patterns and trajectories 22 often overlooked in conventional reviews, making it well suited for mapping scholarly trends and identifying gaps.23,24 Therefore, this method is well suited for systematically organizing and analyzing the extensive body of research that has accumulated on hospice care. The present analysis is descriptive and exploratory, aiming to illuminate patterns and trajectories without inferring direct causal effects.
This study aims to trace the evolution of scholarly discourse on hospice care by examining how institutional and societal changes have influenced thematic shifts in hospice research, using LDA topic modeling. The primary research question asks how hospice research topics changed across these stages in ways that reveal distinct shifts aligned with institutional milestones.
Methods
This study employed LDA topic modeling to identify latent themes and topic structures in hospice-related research. Data collection, preprocessing, and modeling were conducted using the Konstanz Information Miner (KNIME) Analytics Platform (version 5.4.3). Python 3.13.3 was integrated to perform functions not natively supported by KNIME.
Temporal stage framework in hospice research
To establish a globally consistent timeline for examining hospice development, the study delineated four temporal stages based on milestone reports published by the WHO. These periods included (1) the Foundation period (≤2001), characterized by cancer-centered care and limited institutional integration; (2) the Expansion period (2002–2013), following WHO’s broadened palliative care definition; (3) the Institutionalization period (2014–2019), when hospice was designated a public health and human rights priority; and (4) the Post-pandemic Transition period (≥2020), reflecting the impact of COVID-19 on access and care delivery models.
Data collection
A comprehensive literature search was performed using Medical Subject Headings (MeSH) terms “‘Hospices” and “Hospice Care” alongside the keyword “hospice*” to maximize sensitivity (Supplementary Data S1). The search was conducted in PubMed and limited to English-language articles with available abstracts, without restrictions on publication type or country. The search included all entries up to April 27, 2025. The research team developed the search strategy, and a professional medical librarian reviewed it. After excluding articles without abstracts (n = 1) and removing duplicates (n = 253), the final dataset consisted of 14,862 articles. Among publication types, approximately 87% were research articles, 12% were reviews, and less than 1% were letters or editorials. Of these, 318 records lacked publication year information. We retained these for topic modeling but excluded from temporal analyses, as we could not assign periods reliably.
Data analysis
Preprocessing
All abstracts were converted to lowercase, and non-English texts were excluded. Punctuation, numbers, and markup tags were removed. Tokenization was followed by elimination of stop words and terms with fewer than three characters. The built-in English stop word list provided in the KNIME platform was applied, which uses predefined language-specific stop word files maintained within the software package. Lemmatization and part-of-speech tagging were applied to normalize word forms. The corpus was then represented as a bag-of-words (unigram) model for topic modeling. Rare terms (those appearing in fewer than 20 documents) were removed to minimize sparsity. To identify and reduce noise from frequently occurring but analytically uninformative terms (e.g., “hospice,” “study,” and “patient”), term frequency-inverse document frequency (TF-IDF) was computed. Terms with TF-IDF scores below 0.054 were removed after review by the research team to retain conceptually meaningful terms and improve topic separability (interclass distinction). This threshold was refined through an iterative process to ensure stable topic structures and interpretability. 26
LDA topic modeling
LDA is an unsupervised Bayesian generative algorithm that uses Dirichlet priors to identify K latent topics within a text corpus. 27 Each document is modeled as a probabilistic mixture of topics, and each topic is defined by a distribution of words. Dirichlet priors (α and β) govern the document—topic and topic—word distributions, enabling the model to infer thematic structures based on word co-occurrence. 28 Both the number of topics (K) and the number of representative words per topic (N) are user-defined. This approach does not require labeled data and is widely used in health and social science research to uncover trends and inform future inquiry.24,29,30 LDA was implemented in KNIME using the Machine Learning for Language Toolkit (MALLET) library, which applies parallel Gibbs sampling with the SparseLDA scheme. The model was fitted with Dirichlet priors of α = 0.01 and β = 0.01, consistent with previous studies, 31 and 1000 iterations were performed.
Validation of optimal K for LDA topic modeling
Three strategies were used to determine the optimal number of topics (K): perplexity, the elbow method, and semantic coherence. First, perplexity—a measure of statistical uncertainty—was used to evaluate model fit, with lower values indicating better generalization. 27 Perplexity was calculated across a broad range of K values (2–80) and refined to a narrower interval (K = 3–13) for focused evaluation (Supplementary Data S2). Perplexity was calculated across a broad range (K = 2–80). The perplexity curve showed a steady decline from the high-50s at K = 2 to the mid-20s by K = 80. Within the narrower range (K = 3–13), the curve displayed noticeable bends near K = 8, 10, and 12, after which further reductions were marginal, indicating diminishing gains in model fit. Second, the elbow method was applied using k-means clustering to estimate the trade-off between model complexity and interpretability. For this analysis, separate LDA models were trained for each number of topics (K = 2–20), and their topic-document probability matrices were clustered using k-means. The within-cluster sum of squared errors (SSE), computed as the total squared distance between each data point and its cluster centroid, was plotted against K to identify the “elbow point.” This point marks where additional clusters yield only minimal improvements in SSE, indicating an optimal balance between model complexity and explanatory strength (Supplementary Data S3). 32 The SSE curve decreased rapidly up to approximately K ≈ 9 to 10 and then flattened. Third, semantic coherence (intraclass consistency) was calculated using the Gensim library in Python to evaluate the relevance and similarity among words within each topic (Supplementary Data S4). Higher scores indicate more internally consistent and interpretable topics. 33 Coherence increased with K and reached a local plateau around K ≈ 10–12, indicating that further topic splits did not meaningfully improve interpretability. Based on these quantitative metrics and a qualitative review of interpretability, K = 10 was selected as the optimal number of topics. The full analytic workflow is provided in Supplementary Data S5, and reporting follows the LDA Preferred Reporting Checklist 34 (see Supplementary Data S7).
Results
Publication trends in hospice care research
Of the 14,862 studies used for topic modeling, 14,544 included publication year data and were published through April 2025, while 318 lacked year information. As illustrated in Figure 1, the annual number of publications increased steadily from the mid-1970s, with a sharper rise beginning in the 2010s and peaking in 2022 at 1000 articles. Across the four defined periods, 2064 articles were published during the Foundation Period (1972–2001), 3812 during the Expansion Period (2002–2013), 3606 during the Institutionalization Period (2014–2019), and 5062 during the Post-pandemic Transition Period (2020–2025) (Fig. 1).
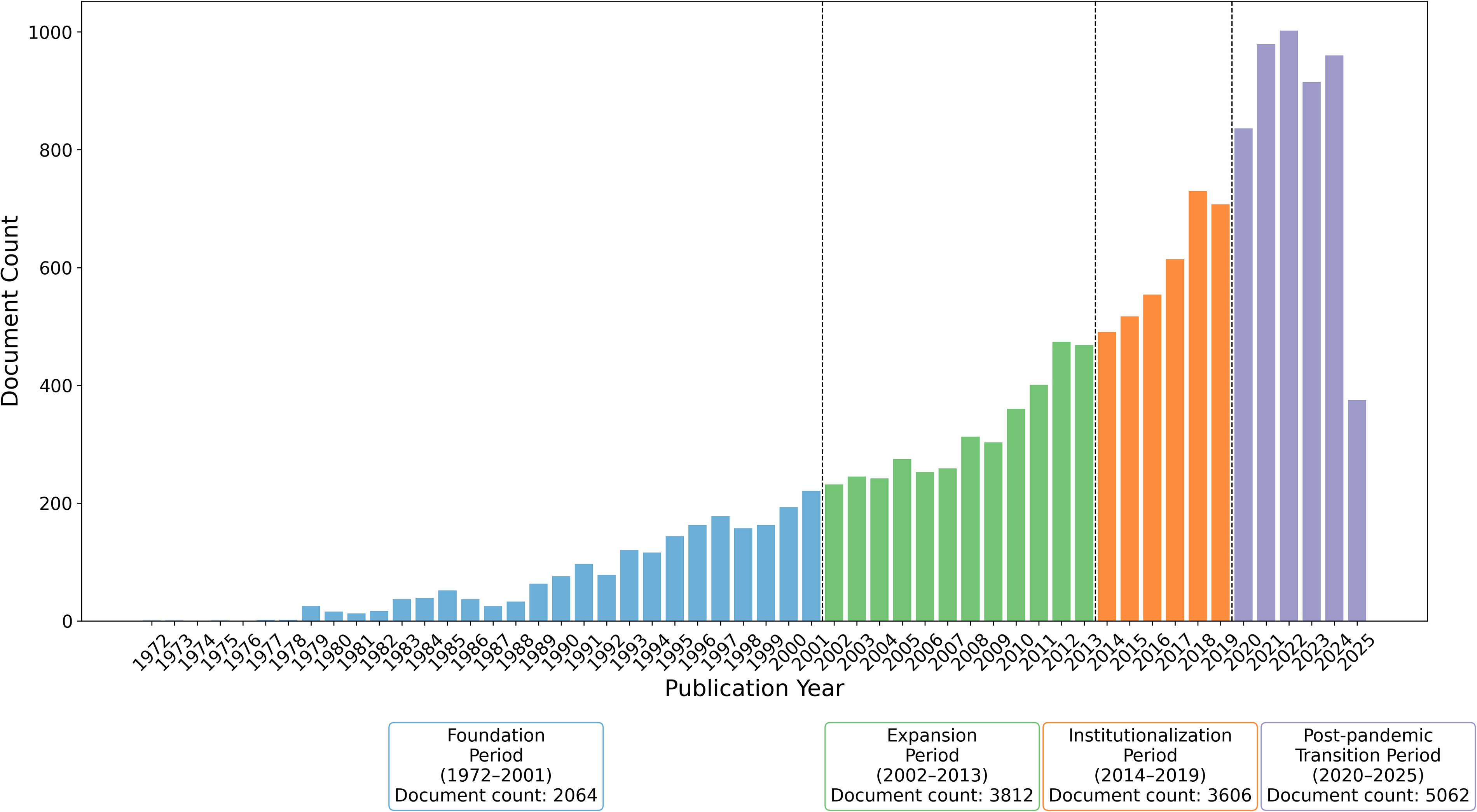
Number of documents per year.
Thematic topics identified through LDA
Application of LDA revealed 10 distinct topics, each representing a major thematic area within hospice-related research. Table 1 presents these topics with their assigned labels, representative keywords, and the proportional distribution of documents. Topic labels were determined through an iterative review by five researchers (M.K., M.B., H.L., M.M., A.K.) and a hospice expert (K.W.) to ensure semantic consistency.
Topic Extracted from Hospice Care Research with Keywords and Distribution (%)
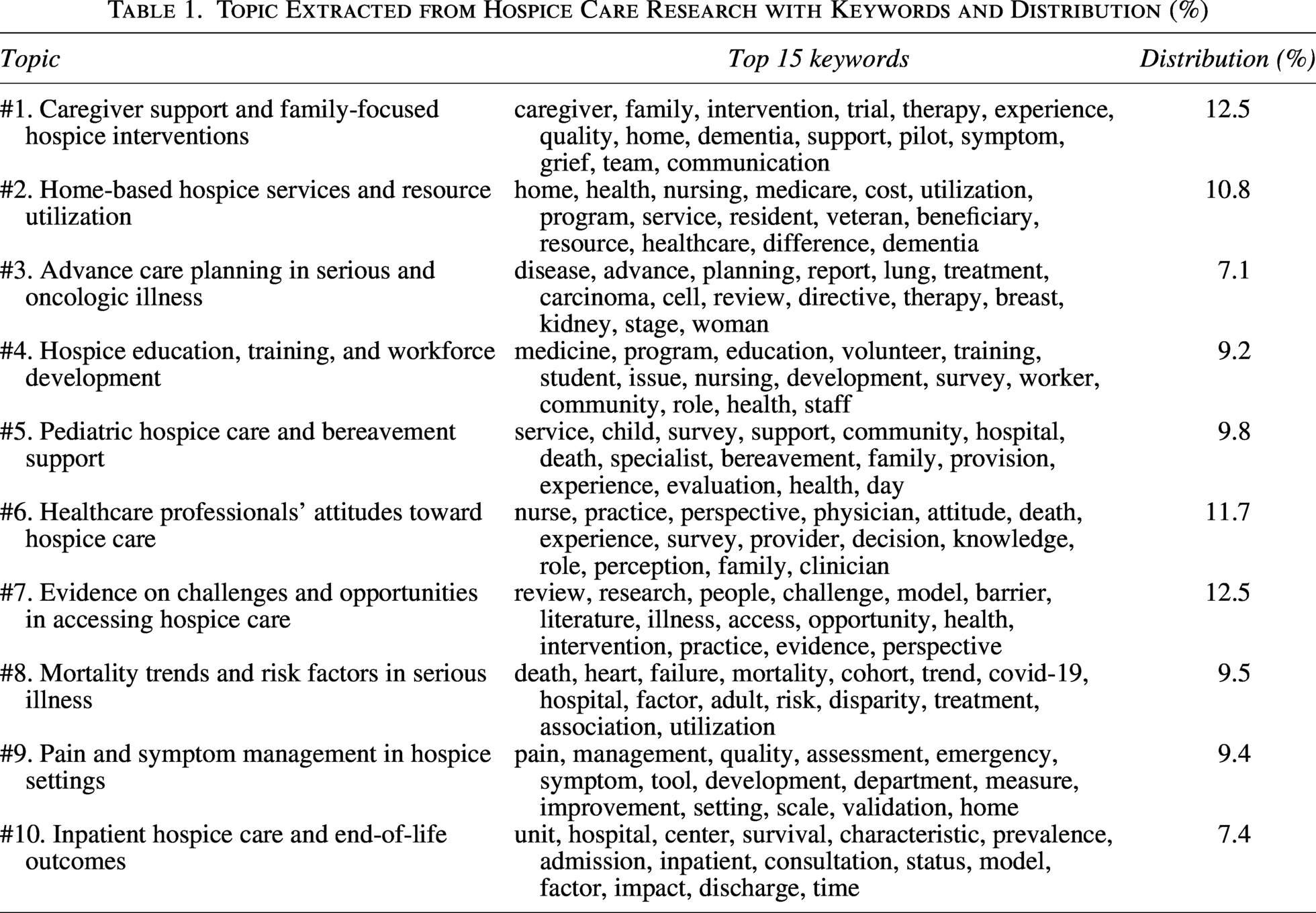
Topic 1 includes studies focused on the needs and experiences of family caregivers, especially through structured interventions and communication strategies in home-based or dementia-related care. Topic 2 pertains to the structure and delivery of hospice services in home and community settings, often associated with public insurance systems. Topic 3 addresses end-of-life decision-making and advance directives in serious illnesses, with a strong focus on oncology settings. Topic 4 covers educational and training efforts to strengthen hospice workforce competencies, including both clinical staff and community-based care providers. Topic 5 explores hospice services for children and their families, with emphasis on psychosocial support, grief counseling, and quality assessment. Topic 6 investigates clinicians’ perceptions, knowledge, and decision-making regarding hospice care, emphasizing professional roles and experiences. Topic 7 examines barriers to hospice access and perspectives on service delivery, drawing primarily on analytical and review studies. Topic 8 focuses on prognostic indicators and clinical trajectories among populations with life-limiting conditions. Topic 9 is concerned with assessing and managing physical distress, including measurement tools and clinical strategies. Topic 10 emphasizes institutional hospice services, particularly admission and discharge processes, patient characteristics, and clinical outcomes at the end of life. Additional examples of high-probability documents are provided in Supplementary Data S8 to support topic interpretation.
Temporal dynamics of topic prevalence across four historical periods
Figures 2–4 illustrate how topic prevalence in hospice research evolved across the four historical periods. Figure 2 displays yearly topic frequency trends, while Figure 3 shows average topic proportions for each period, based on mean topic probability scores from documents published during that time. Figure 4 displays the absolute change (ΔP) in mean per-document topic probability between historical periods, with statistical significance assessed using Bonferroni-corrected t-tests. Each ΔP value reflects the difference in average topic probability.
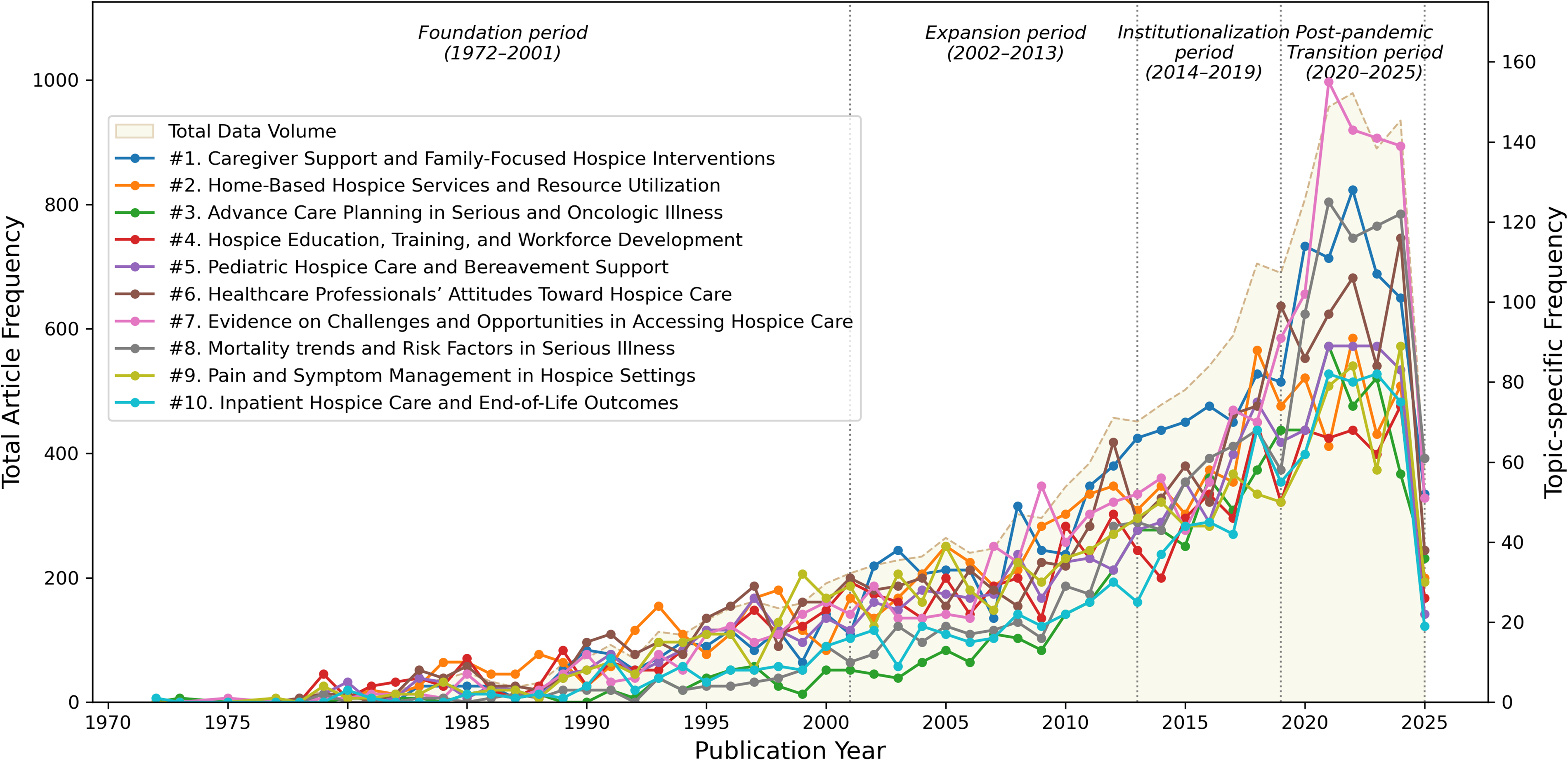
Temporal trends of topics in hospice research.
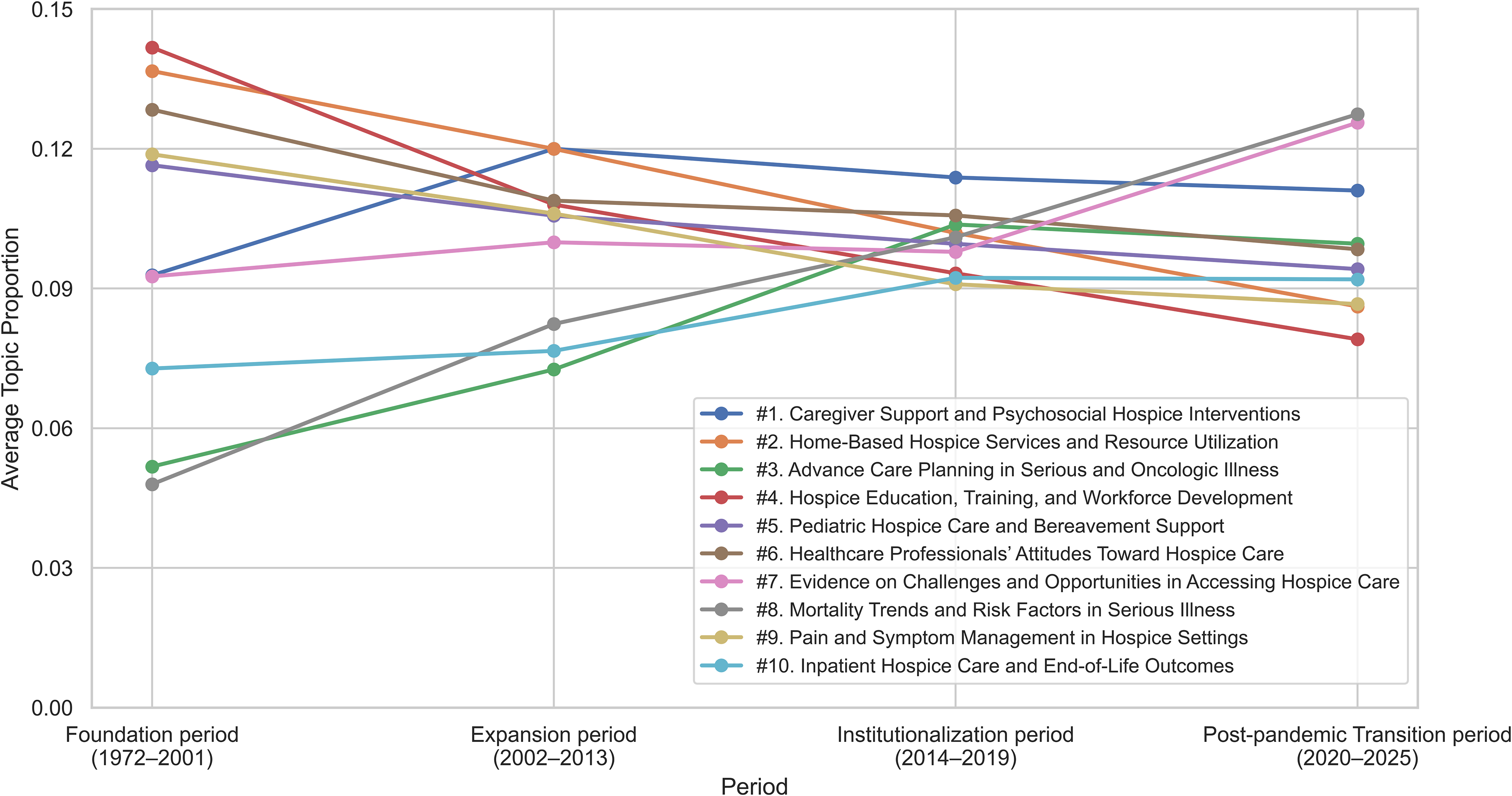
Trends in topic proportions over historical periods. Note: Values represent mean topic probabilities across documents, not document counts.
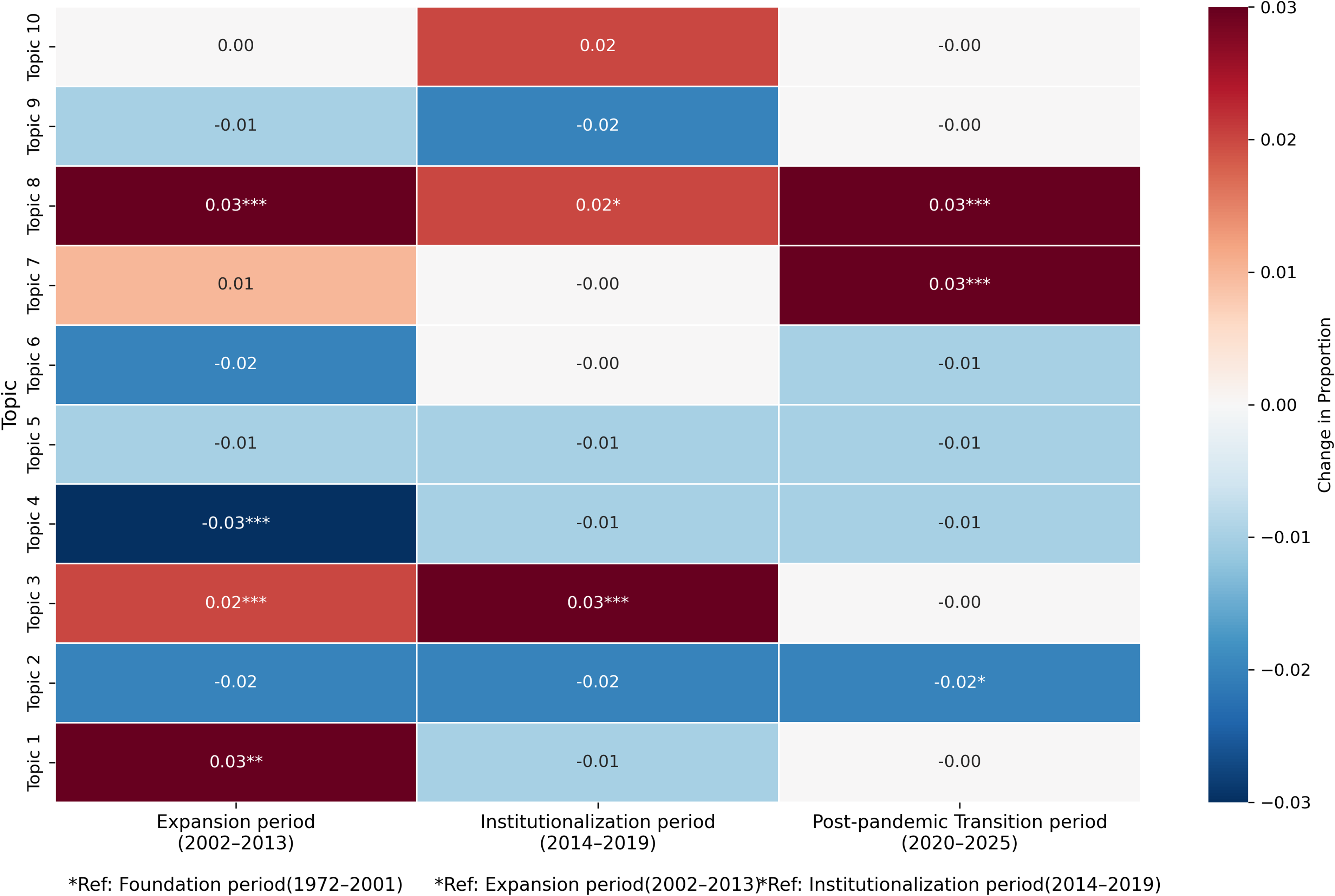
Change in topic proportions compared with prior period. Note: Each cell shows the absolute change (ΔP) in mean per-document topic probability compared with the preceding historical period.
During the Foundation period, topic activity was generally limited (Fig. 2), though Topics 2 and 4 showed relatively greater prevalence (Fig. 3). In the Expansion period, overall topic frequency rose (Fig. 2), with notable increases in Topic 8 and emerging interest in Topics 1 and 3 (Fig. 3). As shown in Figure 4, Topic 1 (ΔP = +0.03; p < 0.01), Topic 3 (ΔP = +0.02; p < 0.001), and Topic 8 (ΔP = +0.03; p < 0.001) experienced statistically significant increases compared with the Foundation period. During the Institutionalization period, Topics 3 (ΔP = +0.03; p < 0.001) and 8 (ΔP = +0.02; p < 0.01) showed significant growth, while Topic 1 accounted for the largest overall proportion (Fig. 3). The Post-pandemic Transition period was characterized by a marked increase in overall topic frequency (Fig. 2) and a pronounced rise in Topics 7 and 8 (Fig. 3). As indicated in Figure 4, Topic 7 (ΔP = +0.03; p < 0.001) experienced a statistically significant increase only during this period, while Topic 8 continued its upward trend, with significant growth during both the Institutionalization (ΔP = +0.02; p < 0.01) and Post-pandemic Transition periods (ΔP = +0.03; p < 0.001). To address potential within-period variation, we examined decade-level topic proportions (Supplementary Data S6), which aligned with four historical periods.
Discussion
Hospice-related research has demonstrated a consistent upward trajectory, reflecting sustained scholarly interest. Topics including caregiver support, pediatric hospice care, and health care professionals’ attitudes toward hospice have maintained stable proportions throughout the study period. These topics align with hospice care’s foundational philosophy, emphasizing holistic approach extending beyond the patient to include families, informal caregivers, and health care providers.1,4,5 Their recurrence should not be regarded as mere repetition but rather as ongoing reassessment and refinement of hospice values. This continued attention has practical implications, underscoring that hospice services must prioritize not only clinical management but also quality of life and relational care dimensions. 35 Accordingly, hospice practitioners and researchers should continue to support caregivers through multidisciplinary interventions, expand pediatric hospice services, and enhance health care professionals’ competencies through sustained education and institutional backing.
Temporal patterns in hospice-related research further illuminate shifts in focus. The Foundation period (1972–2001) introduced hospice philosophy into the medical field, emphasizing ethical and practical care foundations. 4 During this period, research concentrated on home-based hospice models, workforce development, and professional attitudes toward hospice. Home-based care—indicated by keywords including home, Medicare, and resident—emerged as a dominant theme, likely reflecting the U.S. context, where hospice evolved primarily as a home-based model under Medicare.10,36 Simultaneously, increased attention to workforce development reflected the growing demand for formal training to support hospice expansion. 37 At the time, research centered on the necessity and implementation of hospice care, 8 framed within a philosophical context. This aligns with the emergence of contemporary hospice philosophy grounded in an interdisciplinary, holistic approach to end-of-life care. 8
During the Expansion period (2002–2013), following the broadened WHO definition of palliative care, 11 research extended beyond cancer to include a wider range of patients, conditions, and care contexts. This period saw increased focus on mortality trends, caregiver support, and ACP. Increased focus on mortality trends and risk factors in serious illness reflected a shift in hospice discourse to include other life-threatening illnesses,13,14 as more patients with chronic, noncancer conditions such as dementia or frailty began entering hospice in the early 2000s. 3 Scholarly interest in the experiences and needs of families and informal caregivers also expanded, 38 reflecting a more comprehensive view of hospice care. Simultaneously, discussions around ACP began to emerge, signaling heightened recognition of patient autonomy and the need for formal decision-making processes at end-of-life. 39
Between 2014 and 2019—the Institutionalization period—hospice-related research shifted toward policy and structural consolidation. The 2014 WHO Global Atlas of Palliative Care at the End of Life marked a pivotal moment, identifying palliative care as both a public health and human rights issue and calling for its integration into national health systems. 2 During this phase, research on ACP gained considerable momentum, moving from conceptual discourse to policy-backed practice. ACP became reimbursable under Medicare in the United States in 2016, 40 and under Korea’s national health insurance in 2018, 41 signaling its policy-level adoption. ACP research was particularly active in oncology populations during this period, reflecting growing clinical implementation beyond policy adoption. 42 Concurrently, interest in mortality trends and risk factors in serious illness intensified, likely influenced by the rise of predictive research and big data methodologies, particularly in population-level risk analyses.43,44 This development reflects the growing emphasis on early risk identification and timely intervention.
The Post-pandemic Transition period (2020–2025) reflects the COVID-19 pandemic’s impact on hospice care systems and research. During this time, research interest intensified around access barriers and disparities in hospice delivery, alongside sustained focus on mortality patterns. Our topic modeling revealed a significant rise in probability of themes related to access challenges and inequity, indicating that unequal access to hospice care became a more prominent concern. These patterns reflect pandemic-related disruptions to service access, heightened concerns about health equity, and increased attention to remote care and structural adaptation.18,25 The continued emphasis on mortality and risk factors further illustrates growing concern with these issues in the context of COVID-19. The recurring presence of the keyword “disparity” aligns with global public health agendas, including WHO and National Institutes of Health (NIH) efforts to promote health equity and support research on social determinants of mortality. 45 This interpretation is consistent with recent evidence showing that social determinants—such as geographic isolation, restricted carer visitation, and socioeconomic disadvantage—exacerbated inequities in hospice access during the pandemic, while telehealth innovations helped mitigate some barriers but did not eliminate them. 18
Overall, the thematic development across the four periods reveals a progression in hospice research. The field has moved from an early emphasis on theoretical and conceptual foundations—including the philosophical underpinnings and system-level introduction—toward broader engagement with empirical, practice-based, and policy-relevant concerns. Simultaneously, the scope has widened beyond patients with terminal cancer to include individuals with life-threatening noncancer illnesses. This shift signifies more than a change in topics; it marks hospice care’s institutionalization and normalization across global health systems and reflects a conceptual redefinition of hospice as a service grounded in human dignity and individual rights.
Based on these empirical findings, we propose several directions for future research and clinical action. Although early hospice research emphasized home-based care, this has remained relatively stable despite increased policy and clinical interest in models including Aging in Place and Dying in Place. 46 Given the rising preference for home-based end-of-life care, 47 future studies should develop strategies to strengthen home-based hospice care, addressing challenges to better meet patient needs. In addition, despite heightened academic attention to hospice access, it remains limited for socially marginalized and underserved groups. 45 The pandemic has further exposed these disparities, emphasizing the need for targeted strategies to improve equity in hospice delivery. Future research should address structural and systemic barriers—including geographic limitations and socioeconomic disadvantage—that hinder access for these populations. Telehospice represents a promising approach, particularly in rural settings,18,25 and should be further developed through evidence-based research and policy to support effective and equitable implementation.
Limitation
This study has several limitations. First, we retrieved literature solely from PubMed, which may limit source coverage. In addition, because we intentionally restricted the search strategy to hospice-related terms, some relevant studies that discussed hospice but lacked explicit “hospice” keywords or MeSH indexing may not have been captured. However, the dataset—comprising 14,862 articles, significantly more than those in comparable topic modeling studies (typically 2800–7500 documents),30,48—is sufficiently robust for thematic analysis. Second, because we analyzed the abstracts rather than full-text articles, there may be some loss of nuance and contextual detail compared with full-text modeling. Although preprocessing was conducted to enhance topic interpretability, abstracts emphasize study aims and may under-represent specific domains such as spiritual care, end-of-life decision-making, or team collaboration. Third, the topic labeling process carries a degree of subjectivity. To mitigate this, six researchers independently reviewed and discussed labels until reaching consensus, with final confirmation by a hospice research expert to reduce bias. Fourth, the study is subject to language bias because only English-language publications were analyzed. Future research should include additional databases and non-English sources to better capture cross-cultural and international trends.
Conclusion
This study investigated the longitudinal evolution of hospice-related research using topic modeling, identifying 10 core themes and their temporal dynamics across four historical periods. The findings illustrate a clear shift from foundational and philosophical concerns to more applied, inclusive, and policy-oriented topics. By mapping these trends, the study enhances understanding of how hospice care has responded to evolving societal needs. Future research should focus on underexplored areas to ensure hospice services remain inclusive, equitable, and responsive to changing end-of-life needs.
Authors’ Contributions
M.K.: Conceptualization, study design, formal analysis, investigation, methodology, software, visualization, writing—original draft, and writing—reviewing and editing. M.B.: Investigation, methodology, data curation, and writing—reviewing and editing. H.L.: Methodology, writing—original draft, and writing—reviewing and editing. M.M.: Methodology, writing—original draft, and writing—reviewing and editing. K.W.: Funding acquisition, supervision, validation, and writing—reviewing and editing. A.K.: Supervision, data curation, software, validation, and writing—reviewing and editing.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MIST) (No.RS-2024-00334672). Hana Lee received a scholarship from the BK21 education program (Center for World-leading Human-care Nurse Leaders for the Future).
Availability of Data,Code,and Other Materials
Datasets used and analyzed in this study are available from the corresponding author upon reasonable request.
Ethical Approval
As this research did not involve any primary data collection involving human participants, there was no need for ethical approval.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.