
Abstract
Background:
Hospitalized patients with serious illness often face delayed or limited access to palliative care. Embedded hospital primary palliative care (HPPC), led by social workers and nurse practitioners, may deliver more timely, needs-based support compared with referral-based specialty palliative care (SPC).
Objective:
To compare demographics, clinical characteristics, acute care utilization, and sustainability of an embedded HPPC model versus SPC in hospital medicine.
Methods:
We conducted a retrospective cohort study of adults receiving palliative care consults at a New York City academic medical center during two periods: March 2019–February 2020 (HPPC1 vs. SPC) and June 2021–May 2022 (HPPC2 vs. SPC). Variables included demographics, Karnofsky Performance Status (KPS), comorbidities, mortality index, goals-of-care documentation, ICU admission, length of stay, discharge disposition, and 30-day readmissions. Outcomes were compared across groups and periods.
Results:
HPPC patients were older (mean 69.6 vs. 65.2 years; 71.7 vs. 65.0 years), had higher KPS, lower predicted mortality, and more often pursued life-prolonging goals than SPC patients. ICU admissions and hospital stays were consistently lower in HPPC cohorts. Demographic diversity was similar, with ∼27% Black, 23% Latinx, and 30% Medicaid-insured patients in HPPC groups. Volume, patient mix, and utilization outcomes were consistent across HPPC1 and HPPC2, demonstrating sustainability.
Conclusions:
An embedded SW/NP-led palliative care model in hospital medicine improves access, reduces acute care use, and is sustainable over time. This approach supports timely, culturally sensitive, needs-based palliative care and may be scalable for hospital-based delivery.
Key Message
An embedded, social worker—and nurse practitioner—led palliative care model within hospital medicine provided earlier, needs-based support. Their patients had lower ICU use and shorter stays, comparable demographic diversity, and consistent outcomes over time, demonstrating improved access, reduced acute utilization, cultural responsiveness, and sustainability in inpatient settings.
Introduction
Hospitalized patients with serious illness often face delays in receiving timely palliative care. 1 Traditional referral-based specialty palliative care (SPC) models can be constrained by limited coverage, delayed consults, and variability in addressing patient needs.2–4 To mitigate these challenges, our institution implemented an embedded hospital primary palliative care (HPPC) Program within the Hospital Medicine service. More specifically, HPPC is the palliative care team embedded in hospital medicine, which is comprised of a social worker and advanced practice nurse, with no other professionals on that team to provide rapid, culturally sensitive, and needs-based palliative care, with a focus on diverse and underserved patient populations. SPC refers to the inpatient specialty-trained palliative care teams, which are comprised of attending physicians, advanced practice nurses, social workers, chaplains, expressive arts therapists, and massage therapists.
The HPPC model aims to:
Improve access to timely palliative care Support early goals-of-care discussions Address functional and socio-demographic needs
Our initial pilot of an SW-only team embedded into hospital medicine was successful 5 yet could not see patients with symptom management needs given the SW scope of practice. In addition, we determined the hospital medicine team already had established workflows with SWs and APNs, facilitating integration into their service structure.
The majority of consultation requests for the HPPC team go directly to the HPPC team from hospital medicine clinicians. The SPC triage nurse may triage a SPC consultation request to HPPC if the patient is (1) known to the HPPC team, (2) admitted to the hospital medicine service, and (3) the HPPC team is able to see an additional patient.
The onboarding of the HPPC team was multifaceted. The current APN, who had already completed a palliative care fellowship, had a four-week onboarding with the SPC APNs, followed by one week with the Hospital Medicine APNs. The previous APN who did not complete fellowship training had a two-month onboarding with the SPC APNs with an emphasis on cases with Hospital Medicine as the primary service. The HPPC SW was trained with the prior HPPC SW for one week, and the SPC SW for one week. They both completed CAPC modules, read Mastering Communication with Seriously Ill Patients, and completed Geritalk, a serious illness communication skills training adopted from Oncotalk. 5
Annual education includes completion of our departmental grand rounds, CAPC modules, and published articles from the Social Work Palliative Care and Hospice Network (SWMPHN). We also held monthly meetings with two vice chairs from the Department of Geriatrics and Palliative Medicine (e.g., the Vice Chair for inpatient services and the Vice Chair for Quality), the HPPC APN, HPPC SW, and the Hospital Medicine physician liaison. During these monthly meetings, we review challenging cases including patients with refractory symptoms, complex treatment decisions, or discharge planning. In addition, we review operational and quality data on a quarterly basis.
Prior studies indicate that early palliative interventions improve symptom management, hospital utilization, and discharge planning,6–10 but comparative data between embedded HPPC models and traditional SPC in hospitals remain limited. This study aims to compare sociodemographic and clinical characteristics of patients receiving embedded HPPC versus referral-based SPC, and to evaluate acute care utilization and discharge outcomes between HPPC and SPC. Finally, we assessed the sustainability of the outcomes associated with the embedded HPPC model across two one-year periods.
Methods
We conducted a retrospective cohort study of adult patients receiving palliative care consults at a New York City quaternary academic medical center. Two periods were analyzed: March 2019–February 2020 (HPPC team 1 vs. SPC) and June 2021–May 2022 (HPPC team 2 vs. SPC). Patients were included if they received either an embedded HPPC consult or a referral-based SPC consult. Statistical analyses compared groups across both periods and evaluated sustainability over time.
Using electronic health record and claims data, we created a dataset with variables in each of the following categories.
Results
Demographics
HPPC patients were slightly older than SPC patients in both periods, with mean ages of 69.6 years (HPPC1) vs. 65.2 years (SPC1) and 71.7 years (HPPC2) vs. 65.0 years (SPC2). (Table 1) Gender distribution was similar, with approximately half of the patients in each group were female. Racial and socio-economic diversity was comparable across groups: roughly 27% Black, 23% Latinx, and 30% Medicaid-insured in the HPPC cohorts. Marital status showed similar proportions of married, single, and widowed patients.
Demographic Comparison of HPPC and SPC Patients Across Two Periods (2019–2020 and 2021–2022)
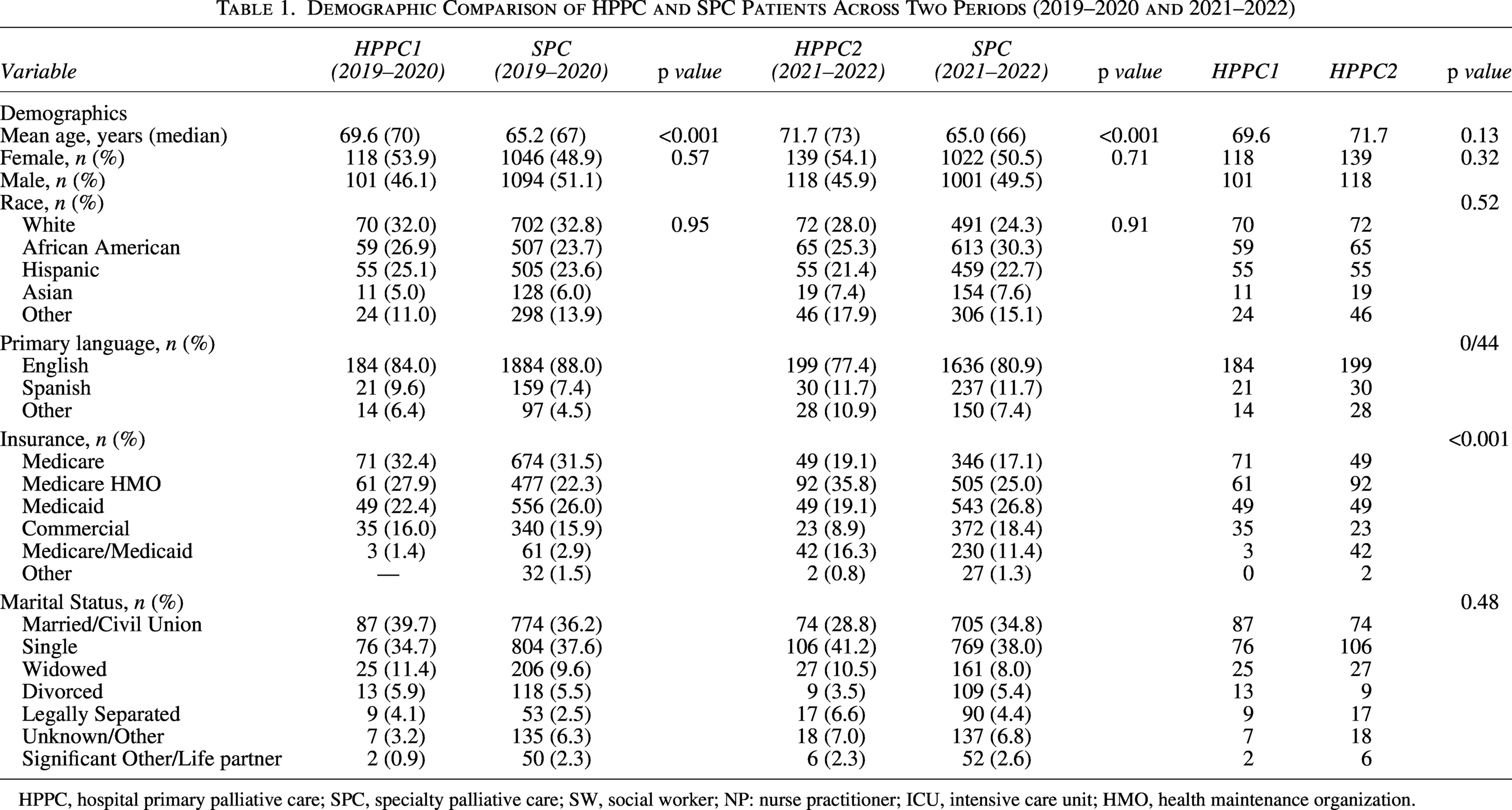
HPPC, hospital primary palliative care; SPC, specialty palliative care; SW, social worker; NP: nurse practitioner; ICU, intensive care unit; HMO, health maintenance organization.
Clinical/serious illness metrics
HPPC patients demonstrated higher functional status as measured by KPS (median 40–40) compared to SPC (40–30). Predicted in-hospital mortality, as indicated by the Premier mortality index, was lower in HPPC patients (14.9%–16.4%) vs. SPC (17.9%–23.7%). Elixhauser comorbidity indices were similar between groups, suggesting comparable baseline illness burden (Table 2).
Clinical Characteristics Comparison of HPPC and SPC Patients Across Two Periods (2019—2020 and 2021—2022)
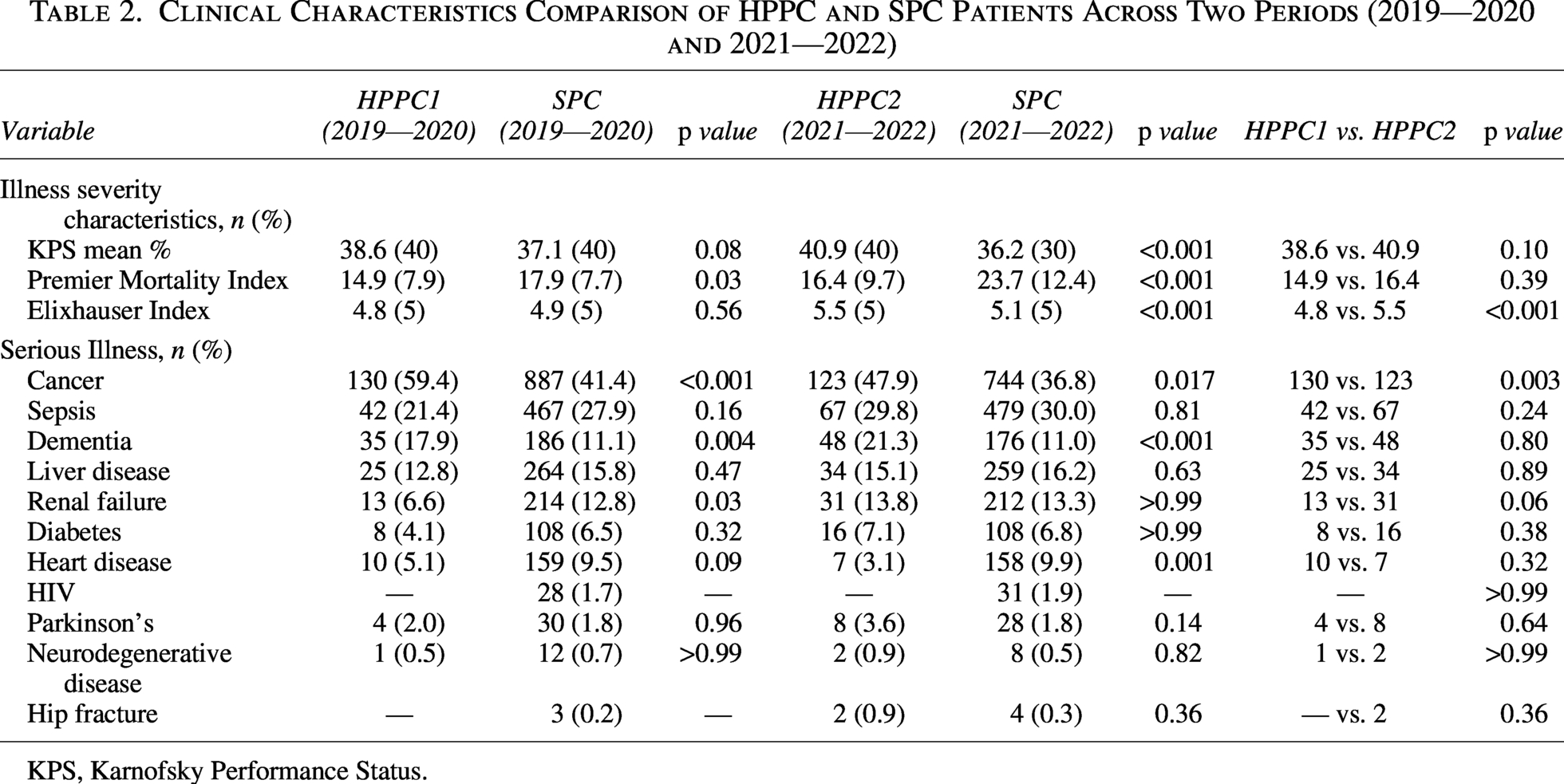
KPS, Karnofsky Performance Status.
Cancer was the most prevalent diagnosis among HPPC patients (48%–59%), followed by sepsis (21%–30%), dementia (11%–21%), liver disease (12%–16%), and renal failure (6%–14%). HPPC saw a significantly greater proportion of patients with cancer and dementia, as compared to SPC during both time periods (cancer: HPPC1 130 (59.4%) vs. 887 (41.4%), p < 0.001; HPPC2 123 (47.9%) vs. 744 (36.8%, p = 0.017) and dementia: HPPC1 35 (17.9%) vs. SPC 186 (11.1%), p = 0.004; HPPC2 48 (21.3%) vs. 176 (11.0%), p < 0.001). Other comorbidities, including diabetes, heart disease, Parkinson’s disease, HIV, neurodegenerative disease, and hip fracture, were distributed across groups with small variations. These findings demonstrate that HPPC and SPC reached patients with significant and diverse clinical needs.
Acute care utilization and discharge outcomes
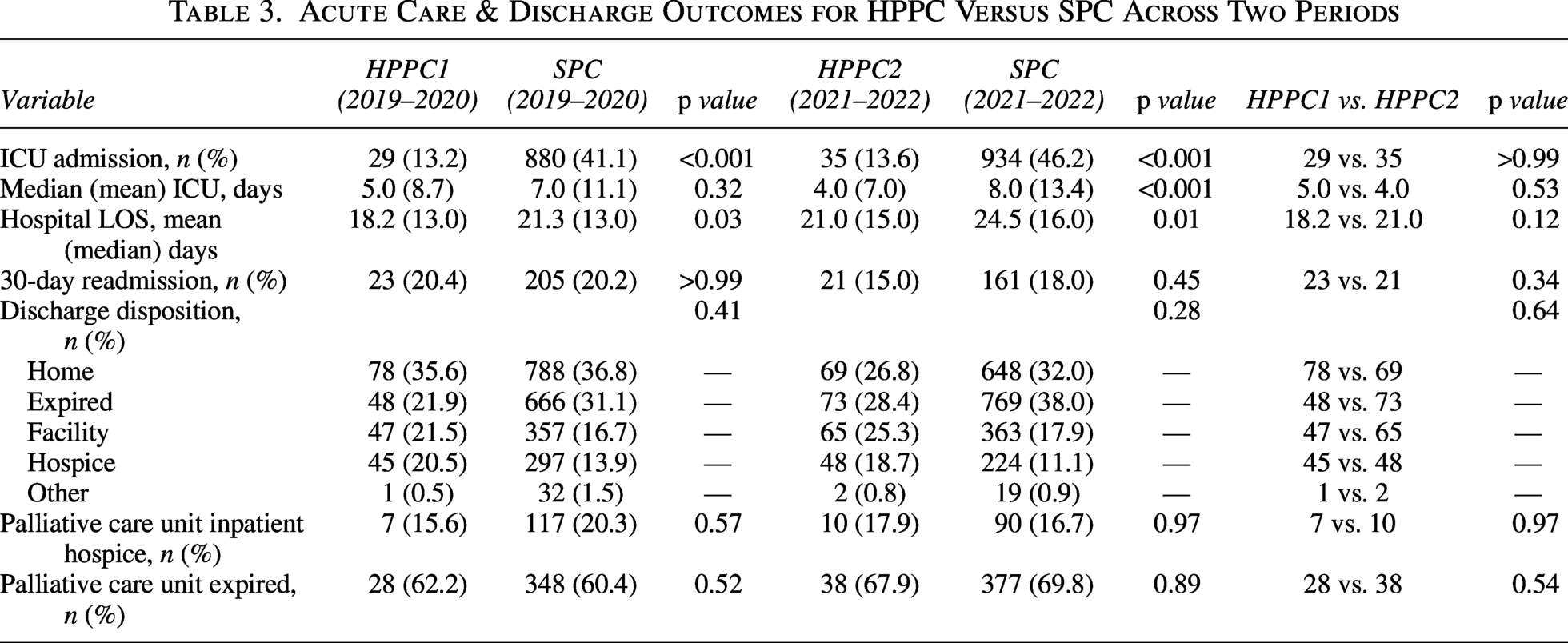
ICU admission rates were significantly lower in HPPC patients (13%–14%) compared to SPC (41%–46%), p < 0.001, with median ICU stay of 4–5 days for HPPC versus 7–8 days for SPC, p < 0.001. Hospital length of stay was shorter for HPPC patients (mean 18–21 days vs. 21–24 days, p = 0.003). Thirty-day readmission rates were comparable between groups.
Discharge disposition favored HPPC patients being discharged home or to a facility, with slightly lower inpatient mortality compared to SPC patients. Hospice enrollment and mortality outcomes were similar between HPPC and SPC, indicating equivalent end-of-life care delivery (Table 3).
Acute Care & Discharge Outcomes for HPPC Versus SPC Across Two Periods
Patterns of palliative care use
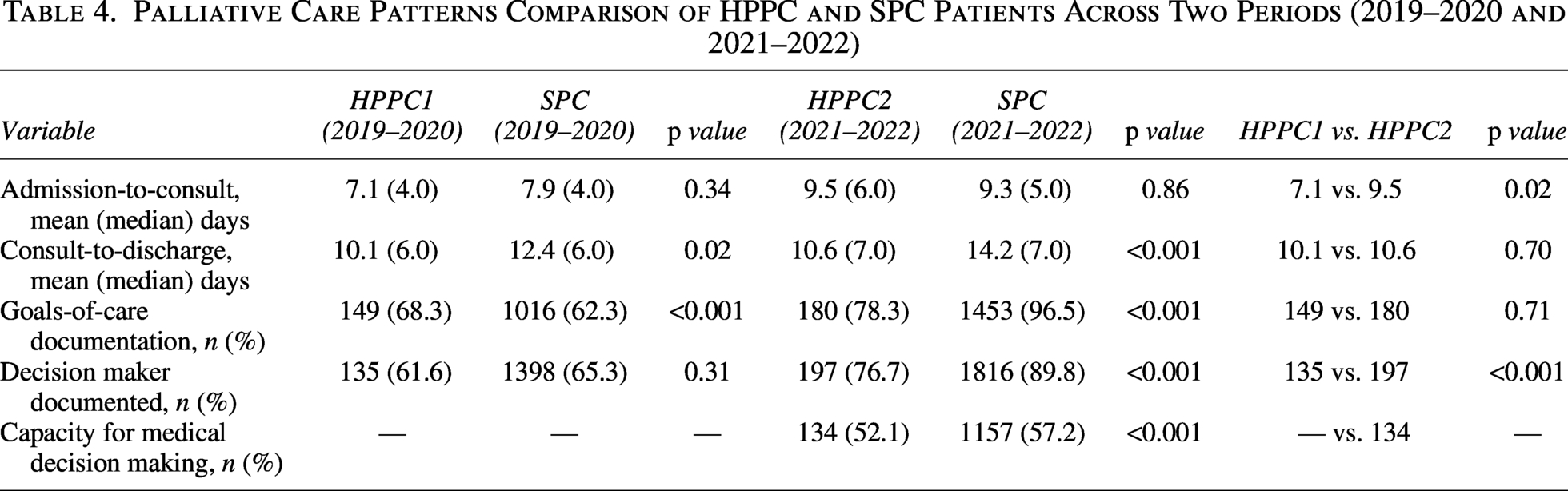
HPPC and SPC patients had a similar number of days between hospital admission and receipt of palliative care consult, as well as days between palliative care consultation and hospital discharge. HPPC and SPC had similar rates of documentation of the medical decision maker. HPPC patients were more likely to have documented life-prolonging goals of care (57% across periods) compared to SPC patients (32%–35%) (Table 4).
Palliative Care Patterns Comparison of HPPC and SPC Patients Across Two Periods (2019–2020 and 2021–2022)
Sustainability
Across both study periods, HPPC maintained consistent patient volumes, demographic diversity, clinical profiles, and acute care outcomes. This demonstrates the sustainability of the embedded model in providing high-quality palliative care over time, despite complete turnover of personnel for both the advanced practice nurse and social work roles.
Discussion
This study provides evidence that an embedded primary palliative care model led by social workers and nurse practitioners (HPPC) can deliver timely, effective, and sustainable care to hospitalized patients with serious illness. Compared to referral-based SPC, HPPC patients were slightly older, had higher functional status, and were more likely to have life-prolonging goals of care. Importantly, the embedded model was associated with shorter hospital stays and lower ICU admission rates, suggesting that early and integrated palliative care interventions may reduce acute care intensity without compromising patient-centered goals. Yet the patients who received HPPC may have been overall less sick as compared with the SPC population, and this may reflect the level of care intensity.
Our findings align with prior research demonstrating that primary palliative care delivered within hospital teams can improve access, particularly for populations that might experience delays or barriers to specialty consultation.14–16 HPPC maintained demographic diversity comparable to SPC, including substantial representation of Black, Latinx, and Medicaid-insured patients, highlighting its potential for equity in palliative care delivery. The model’s sustainability over multiple years, with consistent patient volumes and outcomes, further supports its scalability and operational feasibility in hospital medicine.
Clinical implications of these results are substantial. Embedding palliative care within hospital teams may enhance early identification of patients with serious illness, allow for more rapid goals-of-care discussions, and support care planning aligned with patient preferences. Documented goals of care were used as a proxy for engagement in care planning discussions, recognizing that explicit recording of life-prolonging goals in HPPC may reflect earlier-stage conversations that integrate patient preferences into ongoing treatment decisions. Reduced ICU admissions and shorter length of stay could also translate into resource efficiencies and decreased health care costs. Additionally, the HPPC model provides a framework for workforce development, emphasizing interprofessional collaboration and efficient utilization of social workers and nurse practitioners in palliative care roles.
Because the HPPC team routinely rounds with the hospital medicine service, continuity of patient care is enhanced. The HPPC model creates ongoing opportunities to check in on cases, even after formal consultation has ended. While the team may initially provide a comprehensive assessment and recommendations for a specific point in time, they continue to follow patients informally through natural rounding alongside hospital medicine. This approach ensures the team is readily available if a patient’s condition changes and additional palliative care intervention is needed. In addition, the HPPC team actively monitors readmissions and re-consults for patients previously known to the service. This serves as a powerful benefit in a system of care that is increasingly fragmented with rapidly rotating clinicians across specialty services.17,18
Limitations include the retrospective design and potential unmeasured confounding. The study was conducted at a single academic center, which may limit generalizability. Nonetheless, this model was developed in response to challenges in building another full palliative care interdisciplinary team, due to a limited specialty-trained palliative care workforce and hiring restrictions of new clinicians. By focusing on APN and SW roles, we were able to contain costs, develop a close collaboration with the Hospital Medicine physicians who were more than capable of bridging the gap of medical information, and ensure continuity for the patients who have multiple readmissions with the HPPC team. Therefore, with the appropriate support from and close collaboration with specialty palliative care and hospital medicine, this model is scalable. Future research should evaluate patient-reported outcomes, cost-effectiveness, and the integration of HPPC models in diverse hospital settings.
Conclusions
Embedded HPPC consults reach a slightly older, functionally higher population while maintaining racial, ethnic, and socio-economic diversity. The model is associated with shorter hospital stays and fewer ICU admissions, as this program is designed to reach a population of patients earlier in their illness trajectory. Furthermore, the model was able to maintain consistent outcomes over time, despite staffing changes.
In conclusion, embedded SW/NP-led palliative care represents a sustainable, effective approach to improve access, enhance patient-centered outcomes, and optimize acute care utilization for hospitalized patients with serious illness. These findings support broader adoption of embedded primary palliative care models within hospital medicine.
Footnotes
Author Disclosure Statement
The authors declare that they have nothing to disclose.
Funding Information
L.P.G. received support from the Claude D. Pepper Older Americans Independence Center at the Icahn School of Medicine at Mount Sinai (5P30AG028741) and the Sojourns Scholars Leadership Award from the Cambia Health Foundation.