
Abstract

Hospice and palliative medicine (HPM) has built a powerful and robust foundation in serious illness communication (SIC), pioneering an expansive repertoire of skills for sharing difficult information, eliciting values, responding to emotion, and supporting complex decision-making. The codification and widespread dissemination of SIC through established training initiatives have profoundly reshaped serious illness care in medicine.1–3 This foundation now positions our field for its next phase of maturation: refining how we tailor our skill set to meet the psychological complexity and heterogeneity of patient and family coping needs.
A central premise of this evolution is the recognition that SIC, like other domains of medicine, benefits from an explicit assessment step that precedes and informs intervention. Throughout clinical practice, we routinely consider underlying etiologies, such as drivers of pain, dyspnea, or delirium, before selecting a treatment plan. In the same way, even as SIC has advanced substantially, comparatively less emphasis has been given to how clinicians assess which communication tools are most therapeutically aligned with a patient’s coping needs in a given moment.
In considering how to integrate this crucial step into our approach to SIC, the field of psychotherapy offers a useful and relevant scaffolding, not as a replacement for our current skill set, but as an expansion of it. Psychotherapy and SIC share several foundational similarities. Both fields recognize that communication is not merely a vehicle for information exchange, but a core therapeutic intervention; the clinician’s use of self-as-instrument, reflected in how we relate and respond to patients, can itself enhance adaptive coping and support patients and families as they navigate emotional complexities.4,5
At the core of psychotherapeutic practice is the concept of formulation: an ongoing, iterative assessment that seeks to understand why a person is coping in a particular way at a particular time. 6 A formulation is not a diagnosis; instead, it is a working hypothesis about the psychological functions of a patient’s thoughts, emotions, and behaviors. It invites clinicians to ask questions such as: “Why might this patient or family be responding this way right now?” “What underlying fear, need, or struggle might this coping pattern be serving?” Importantly, formulation is not synonymous with intuition; rather, it is an explicit, intentional process that evolves as new information emerges. 7 When adapted and applied to SIC, formulation acts as a compass, allowing assessment to more directly guide communication strategies and therapeutic presence. Rather than responding solely to surface behaviors, it allows clinicians to tailor their words, stance, and timing to the patient’s or family’s unique psychological needs.7,8
Consider, for example, a common scenario in serious illness care: a family delaying a critical care decision, often labeled as “indecision.” A formulation-guided assessment allows clinicians to contemplate the potential psychological functions of this behavior, which may point toward different communication strategies. If our working formulation is that beneath the indecision resides an overwhelming fear of making “the wrong choice” for their loved one, a clear, values-aligned recommendation may therapeutically reduce the family’s burden: “It’s clear how much you care for your father. Given everything we know about him, his values, and his medical situation, would it be okay for us to make a recommendation?” Alternatively, if our working formulation is that the hesitation reflects mistrust of the medical system (perhaps shaped by prior experiences of feeling dismissed or wronged), a directive recommendation may feel coercive or pressuring. In this context, communication tools that center the patient’s voice may restore a sense of agency and trust: “If he could speak for himself right now, what do you imagine your father would say is most important to him?” or “What would it look like for this decision to feel as true to his wishes as possible?” Although the family’s observable behavior is identical in both cases, the underlying psychological needs differ substantially, as do the communication approaches most likely to be therapeutic. 7
To lay the groundwork for this critical bridge between generalized communication skills and targeted psychological intervention in SIC, an interprofessional author team with training in both psychotherapy and palliative care developed a nine-article special series that collectively translates and adapts concepts from psychotherapy into relevant, actionable guidance for general HPM practice.
This series has two closely linked objectives. First, we aim to integrate assessment-informed communication into routine HPM practice by demonstrating how psychological formulation—a working hypothesis of a patient’s core coping challenges—can guide therapeutic communication. Second, we seek to equip clinicians with a repertoire of high-yield psychotherapeutic “micro-skills” that are concrete, teachable, and readily applicable to everyday serious illness care, without requiring formal psychotherapy training. Rather than replacing prior advances in SIC, the series extends them by sharpening the use of existing communication tools through assessment-informed choices and a broadened communicative repertoire. Importantly, it does not propose that HPM clinicians function as psychotherapists; instead, it aims to expand our therapeutic skill set within everyday clinical practice.
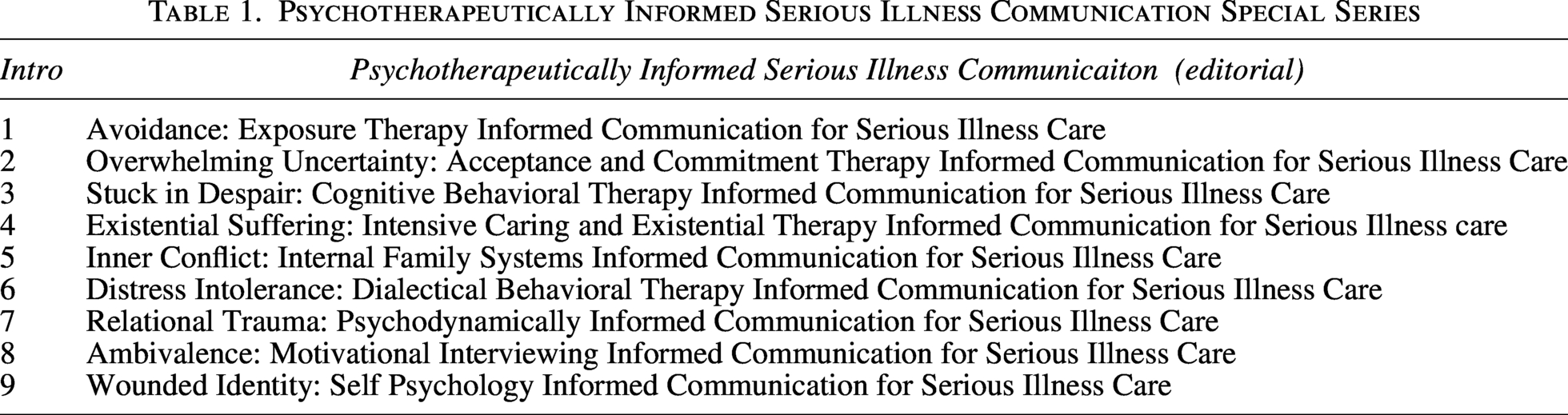
Each article will focus on a common coping pattern encountered in serious illness care, such as avoidance, ambivalence, distress intolerance, or existential overwhelm. Articles will follow a standardized structure: a clinical case illustrating a coping challenge, a working psychological formulation that explores potential underlying drivers, and a set of assessment-aligned, high-yield communication strategies drawn from evidence-based psychotherapeutic traditions (see Table 1). These strategies are translated into practical bedside language, emphasizing applicability within time-limited clinical encounters. Rather than advocating for the universal application of any single psychotherapeutic tool, the series aims to highlight how different approaches may be optimally suited to distinct psychological needs.
Psychotherapeutically Informed Serious Illness Communication Special Series
Our field is particularly well positioned for this next step in SIC, given the depth of psychosocial, mental health, and spiritual expertise within our interprofessional teams. This perspective invites clinicians to expand our inquiry beyond identifying the clinical problem to understanding why a patient or family may be coping in a particular way, what they may need most in a given moment, and how therapeutic presence can be intentionally aligned to meet that need. Such an approach acknowledges that an intervention may be therapeutic in one context and countertherapeutic in another, advancing our field beyond uniform communication strategies toward an assessment-informed approach that is attuned to the psychological context of coping.
When therapeutic presence is intentionally matched to underlying psychological needs, communication becomes not only a learned skill but a deeply personalized form of care. This therapeutic posture positions HPM at the forefront of both the art and the science of SIC, honoring a foundational truth of serious illness care: that each patient has a unique narrative, coping style, and constellation of needs.