
Abstract
Medicine finds itself on the brink of an artificial intelligence (AI) revolution, promising to transform what it means to be human and thus what it means to encounter humans with serious illness. The character of such transformation in pain management remains yet to be determined, leaving open to what extent AI might exacerbate or resolve challenges confronting pain management. In this article, I aim to clarify what might be expected from AI in pain management on a conceptual level and proceed by problematizing the tension between, on the one hand, partial data representing the range of incipient AI applications relevant to pain and, on the other hand, total pain representing the core principles and concepts of pain management in palliative medicine. This helps to elucidate those aspects of pain most amenable to automation, generating a call to action within pain research and presenting an opportunity for palliative clinicians to steer AI implementation.
Key Message
The conceptual friction between partial data and total pain raises important clinical and ethical problems. Reflecting on this friction clarifies what can be expected from AI in a general sense and underlines the role palliative clinicians can play in implementation.
Like society writ large, medicine finds itself on the brink of an artificial intelligence (AI) revolution. We expect from AI what historian David Noble prophesied: a mixture of “doom and deliverance,” promising either to make medicine more human or to destroy it, in either case to utterly transform what it means to be human and thus what it means to encounter humans with serious illness.1–3 The transformational potency of AI seems clear; however, the character of such transformations in palliative care, and pain management more specifically, is yet to be determined.4–9
Pain today remains oversimplified and undertreated due to factors ranging from a shortage of palliative providers, implicit and explicit bias, the ongoing opioid use epidemic, and not to mention the fact that pain assessment and management are intrinsically challenging.10–14 Recent literature has highlighted the opportunity for AI to play a role in patient-facing areas relevant to pain management, including patient education, pain self-management, and bedside automatic pain assessment, as well as non-patient-facing areas such as pain prediction and decision support.15–24 To what extent might AI resolve or exacerbate challenges in pain management?
Upon encountering GPT-4, Peter Lee of Microsoft put into words a common experience:
Honestly, I lost a lot of sleep because of it…My computer science background helped me understand the technical underpinnings, but I still felt like a science fiction explorer encountering an alien intelligence, gradually coming to understand its qualities. This isn’t just about feats of amazing technology. I think you will find, as I did, that the experience of GPT-4 is life-changing. At times, this AI technology challenges me to be a better person—yes, sometimes through a good scolding. GPT-4 can make me laugh with its (often dry) wit. And…GPT-4 expresses concern for my well-being. 25
Lee subsequently identifies the focal question AI presents in the coming transformation of medicine: What does it mean to be human? And thus, what does it mean to be in pain and to relieve pain? Are we parrots who babble in probabilities—stochastic parrots processing partial data? Or are we meaning-making creatures in need of compassion for our total pain, for whom pain is the start of poetry? This is the tension between partial data and total pain that I will be problematizing. Reflecting on this tension will shed light upon what we can reasonably expect from AI and how we might best guide AI implementation. This approach will help open a middle ground of thoughtful discernment between the extremes of a priori rejection and uncritical embrace, while expanding the range of issues addressed by AI ethics.3,26–28 This can be a modest first step toward outlining what aspects of pain management may be reasonably automated, generating a call to action within pain research, and presenting an opportunity for palliative clinicians to steer AI implementation.
Two Thought Experiments
In order to adequately take stock of AI for pain management, it will be helpful to take a brief tour through two thought experiments borrowed from philosophy of mind and computer science commonly referenced in arguments about AI. These are the Turing Test and the Stochastic Parrot critique.
Alan Turing was a computer scientist who laid the groundwork for CPUs that run most computers and put forward theoretical reflections on how computers function as minds. Building upon theories from philosophers such as Rene Descartes, Turing understood intelligence very pragmatically: it is the ability to solve problems.29–30 His 1950 article famously demonstrated this in what is known as “The Turing Test.” 31 In Figure 1, imagine a computer A and a human B are in separate rooms. Both are tasked with holding a text conversation with another human C, who is in a third room and does not know which author is human or robot. The test, here, is whether human C can judge which text was authored by a computer. If they cannot reliably tell the difference, the computer passes the test.
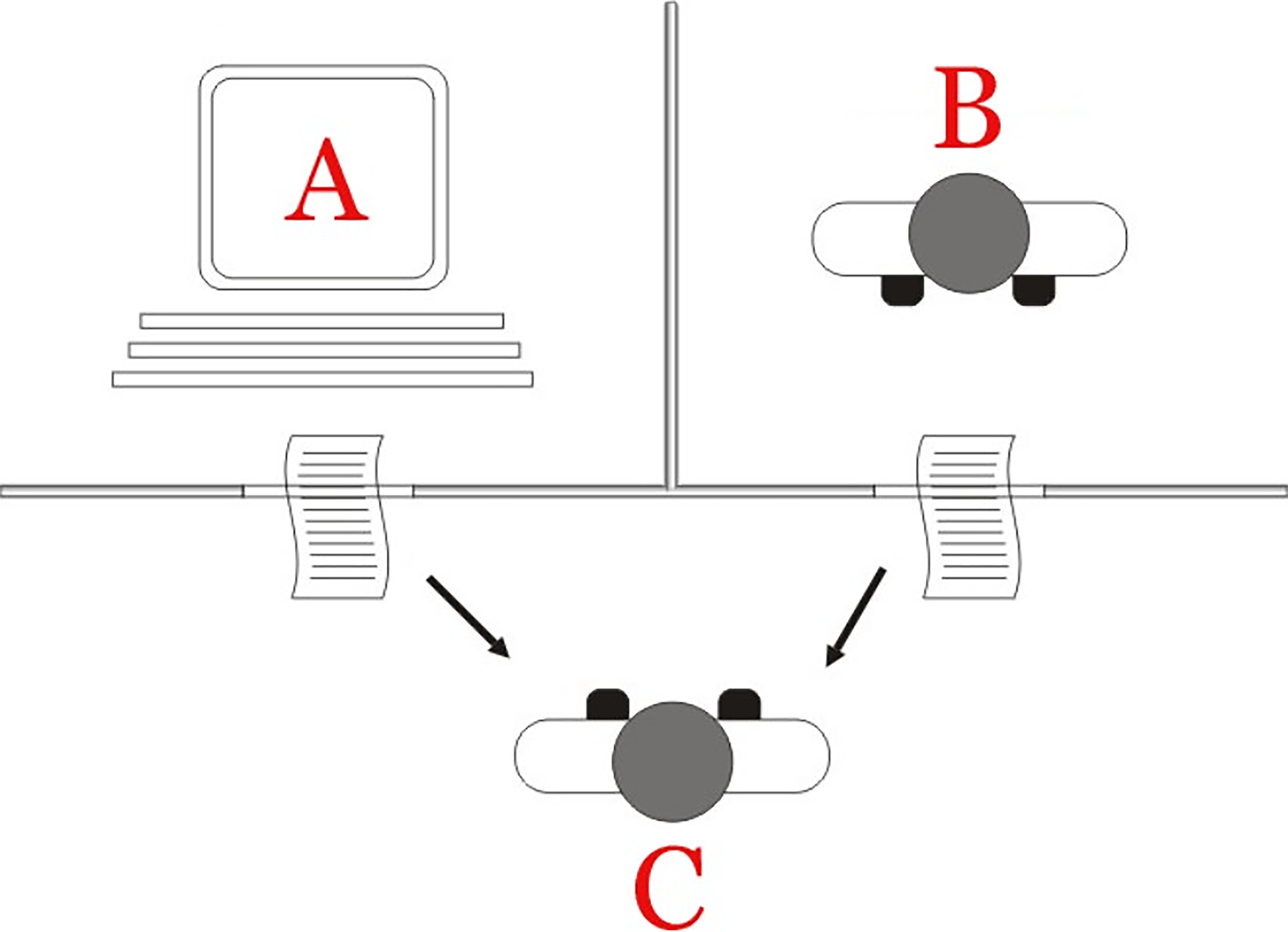
The Turing Test. Human C, blinded to the identities of computer A and human B, is tasked with judging which of the two texts was written by the computer based upon the output text alone. By Juan Alberto Sánchez Margallo-File:Test_de_Turing.jpg, CC BY 2.5, https://commons.wikimedia.org/w/index.php?curid=57298943.
Turing developed this test to sidestep the question of whether machines can think, presenting instead this imitation game as a trick playing upon deeper philosophical commitments. For Turing, what really counts is the algorithm or human’s outputs, not the process or structure of thought giving birth to it. 32 While algorithms that pass this test are certainly impressive, what the Turing test highlights even more than the quality of AI outputs is the reduction of the human B to a computer in the first place. We can easily extend this test so the text output could be pain management recommendations, which straightaway underscores the artificial nature of the test itself. Nowhere does the test allow for contact of either agent with an actual embodied, conscious patient for its inputs. It assumes that the only relevant data inputs can be translated into computer code and that the intelligence ingesting that data work by manipulating it and producing an output that similarly can be delivered in computer code. The text output provides the form of language, though without meaning or understanding. This is similar in some ways to John Searle’s famous “Chinese Room” rebuttal of Turing. 33
The next thought experiment worth exploring briefly is the ‘Stochastic Parrot’ critique of large language models put forward in 2021. 34 Bender and colleagues discuss how large language models principally work through probability, which is curated through immense training data and processed through massive neural networks located at proportionately large data centers. So, given an input piece of data (a token), the algorithm predicts what is the most likely next piece of data—imagine text where the algorithm is providing the most likely next word—based on the data it was trained on. This focus on probability implies that the work accomplished by the algorithm is stochastic manipulation of datasets—rearranging data according to probabilities. Critically, this mimics (or “parrots”) human capacities without reproducing them. Parrots do not understand what they are saying, only that they have been trained to repeat what they have heard, although large language models do this at an enormous scale. In other words, outputs provide the form of language deprived of understanding and meaning, both of which rely upon a real human social-linguistic relational context for communication. Thus, many algorithms are simply very fast stochastic parrots that are only as reliable as their training data as well as the input data.
Algorithms, by definition, cannot have direct experience of real-world patients in pain; their access is derivative from human experience translated into data, meaning they have no real-world corrective to prevent biases in the data from becoming biases in their outputs. Additionally, they have no way to discern the coherence or accuracy of their outputs, meaning they cannot understand whether their outputs are correct or incorrect, or whether those outputs actually correspond, in fact, to the real world. Algorithms might be very effective at generating the form of pain management without the meaning.
The Stochastic Parrot critique brought to light two important dangers inherent in large language models. First, algorithms are vulnerable to biased training data, an effect compounded with size. Second, there is more to being human than being a stochastic parrot. 35
Three Hazards
We strive in palliative medicine to approach seriously ill patients in pain holistically, acknowledging that the suffering patients experience cannot be reduced to nociception. Cicely Saunders’s seminal concept of total pain expresses this nicely: ultimately pain and suffering are about the story, the narrative, and thus the meaning of a patient and family’s life, nested within concentric, overlapping communal, cultural, historical, spiritual, and religious narratives of meaning.36–38 Reflecting on the beginnings of hospice and palliative medicine, Cicely Saunders said:
It soon became clear that each death was as individual as the life that preceded it and that the whole experience of that life was reflected in a patient’s dying. This led to the concept of “total pain,” which was presented as a complex of physical, emotional, social, and spiritual elements. The whole experience for a patient includes anxiety, depression, and fear; concern for the family who will become bereaved; and often a need to find some meaning in the situation, some deeper reality in which to trust. 38
This is complemented by the 2020 International Definition of Pain, which emphasizes the distinction between pain and nociception, underscoring that pain is a personal experience richly painted in biopsychosocial colors. 39 In other words, a holistic approach to pain resists categorical reductions both into the objectivity of data and the subjectivity of patient report. Pain as experience, while enveloping these subjective and objective elements, belongs rather to the category of consciousness—persisting amid illness that lowers consciousness—and thus the category of meaning. Total pain requires a personal response of compassion, a response of care, from one person to another. In other words, it calls for total care and invokes a whole philosophy of care. This is what is at stake when AI enters pain management.
Now we are prepared to begin outlining hazards inherent in employing AI for pain management. What follows are three necessarily broad areas of clinical and ethical friction that can help begin defining the boundaries of automation in pain management, with the goal ultimately to identify the opportunity areas for AI tools.
Clinical epistemic issues
This first hazard is largely a practical one: How well do data used by AI represent what we mean by pain in the real world? As the Stochastic Parrot critique shows, the answer to this question will also dictate how well the outputs—pain management recommendations—correspond to what we mean by compassionate pain relief in the real world. So, the question is how do pain scores, ECOG scales, behavioral data like facial expressions, neurophysiological data like heart rate variability, imaging, pathology, and more relate to what we understand when we say “pain,” and what kind of triangulation would be required to translate those data into our pain concept above? Additionally, what biases are encoded within training data, such as nonclinical datasets that, at present, tend to over-represent healthy White patients in acute pain from western democratic societies or clinical datasets that likely demonstrate the racial, economic, and other biases latent in pain management today? As the Stochastic Parrot makes clear, data are partial in multiple senses.34,40,41
It may seem unfair with such diverse applications in the literature to lump their varying data inputs into a single hazardous area here; however, the point largely stands regardless of the specifics of those inputs, as will be made clear by contrasting pain with blood sugar. The bionic pancreas was approved in 2022 after studies showed it offered superior glycemic control and safety than prior insulin pumps. 42 Instead of manually programming an insulin infusion regimen, the bionic pancreas learns to adjust insulin doses automatically based on the patient’s prior needs to control their blood sugar. The only figure the patient has to enter is their body weight. With no carb counting required, it leans exclusively on blood sugar to learn how much insulin the patient needs in real time.
Here there is a wide berth between pain and blood sugar. Blood sugar is a purely empirical data point such that the number of blood sugar that we measure in grams per deciliter is a direct representation of blood sugar. In other words, the data point of blood sugar directly matches the concept of blood sugar. Data points for pain, however, do not signify in the same fashion. It is quite obvious that a rapid heart rate is not pain; a grimace is not pain; and a pain score is not pain. Each of these phenomena surely manifests pain to us, but they are not pain themselves. This epistemic and semiotic problem presents a serious, although not insurmountable, hazard.
The problem of (embodied) consciousness
The second hazard is more principled: What does it take for an agent to understand pain? Scott Graham rightly glosses the international definition of pain that understands pain as experience by stating, in his words, pain is a quality instead of a quantity.30,40,41,43 Pain is an embodied conscious experience, and this means it requires an equally embodied conscious clinician to appreciate it. Again, pain is equally subjective and objective while resisting reduction to either. As Cicely Saunders has emphasized, caregiver’s and patient’s personal narratives intersect to form a kind of co-narrative made possible by the fact that embodied conscious human caregivers who have experienced pain themselves can understand, at least a little, what a patient means when they describe their pain and also share that pain to some extent.36–38 It is clear enough that AI lacks the kind of embodied consciousness that even higher mammals like dogs have, so it is fair to say AI cannot understand pain any more than a disembodied brain in a vat or a parrot. 32 Put differently, big data cannot cross the categorical divide between data and experience; it cannot reconcile quantities and qualities. At best an algorithm’s access to an embodied patient’s conscious experience of pain is derivative of human access to that experience.
The common objection to this concern is to disregard its relevance by invoking something like the Turing Test. As we pointed out, Turing attempted to sidestep this problem completely, arguing that what matters is not whether AI could truly understand pain the way a human could, but whether its output is indistinguishable from a human. That is, what counts is whether AI can technically perform pain assessment and/or management at a human level. Accepting this assumption, however, would undermine holistic concepts of pain.
The problem of meaning
“Because it is not capable of pathos, artificial intelligence is not capable of thinking. Suffering and enduring are conditions that no machine can realize,” as Korean-born philosopher Byung-Chul Han has said. 44 Much more than a technical problem, the problem of pain presents a moral and existential problem encapsulated by the aphorism pain is the start of poetry. Pain generates an experience, even a crisis, of meaning. Regardless of how precisely AI can measure pain, a stochastic parrot cannot sympathize with a patient’s weakness. There is no meaning in data, at least the kind found within a patient’s suffering. After surviving Auschwitz, Victor Frankl concluded we are not destroyed by suffering; we are destroyed by suffering without meaning, going so far as to say “without suffering and death, human life cannot be complete.” 45 Suffering is one of the primary routes to find meaning, so to the extent that data takes the place of embodied conscious experience, it threatens to liquidate meaning from pain. This would amount to ersatz pain management in palliative medicine.
There is no shortage of enthusiasm that AI may help make health care human again. 46 Yet these three hazardous areas bear remembering lest the founding principles in hospice and palliative medicine be compromised. We are vulnerable creatures fueled by meaning, subject to countless illnesses, indignities, and dependence—total pain—standing in need of care, in need of a morally rich response to suffering. These three hazardous areas help to clarify what can be expected from AI in pain management and explicate the difficulties that leaders in applying AI for pain have encountered, for example, surrounding the distinct pathophysiology between acute and chronic pain or the challenge of integrating the subjectivity of pain. 47 To summarize, AI threatens to evaporate meaning from palliative care by collapsing total pain into abstract data. To the extent we believe AI fulfills our moral responsibility to patients in pain, we may forget that moral responsibility in the first place, reifying systemic illnesses in how medicine approaches pain today.
Toward AI Implementation
To be clear, there remain plentiful opportunities for AI to improve pain management within the conceptual boundaries outlined in this article, opportunities for automation that serve, rather than invert, holistic approaches to pain, though caution is warranted in future speculation. Large language models, for example, could be utilized to deliver concise, individualized written and graphic education for patients, and their training, further, could be tailored by “listening” to palliative clinicians educating patients at the bedside. With appropriate privacy and informed consent protections, such data could be gleaned from ambient AI scribes utilized to reduce documentation burdens. One patient-facing mobile application in development enhances patient self-management of chronic pain via improved tracking and trending of pain, triaging of symptoms, and providing education curated by clinicians. Initial evidence suggests improved pain scores and reduced hospitalizations when adding the mobile app to usual outpatient palliative care. 18 Additionally, there is fertile ground for pain prediction and clinical decision support. 19 Lastly, pain research may stand to gain the greatest benefits from machine learning, identifying previously undetected clinical patterns and correlations in pain phenotypes as well as basic science work in drug discovery and repurposing. 6 This is a call to action for further AI research and development with the goal of preserving and advancing the core values of palliative medicine, rather than technology for its own sake. Tools always bear the image of their makers, and AI tools for pain embody, even if subtly, values and concepts of pain assumed by their creators. For this reason, technology companies generally recognize the value of end users like palliative clinicians contributing at every stage of development. Even more so, however, the AI tools that will best advance the core principles of palliative medicine will be made with and for palliative clinicians from the earliest stages of development.
The time is ripe for palliative clinicians to steer AI implementation locally and nationally by speaking into policy for these emerging technologies, anticipating that such a task will often cut against the grain. 48 Such a task involves discerning products wisely alongside data scientists and administrators and setting boundaries to guard appropriate use. It also entails post-implementation assessment of AI tools in both technical and moral values. Not only does algorithm accuracy drift over time, but also clinicians and health care systems drift in their application. I have focused on pain in this article; however, palliative pain management in many ways is paradigmatic of the goals of medicine, meaning palliative clinicians are uniquely positioned to steer AI implementation generally. It would be shortsighted for modern health care to imagine AI as a simplistic solution to problems confronting medicine. AI might just as easily—perhaps more easily—reify those problems in the first place by leaving their root causes unaddressed.
Footnotes
Acknowledgments
Thanks to Sara Graham, Tommy Petros, and John Rhee, who offered dialogue and commentary on this project in various stages.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.