
Abstract
Background:
Sudden unexpected death can occur even among patients with advanced cancer receiving hospice and palliative care. How bereaved families perceive this remains unclear.
Objectives:
To investigate the prevalence of sudden unexpected death from bereaved family perspectives, the level of agreement with physician perspectives, and their association with bereaved families’ mental health.
Design/Setting/Subjects:
We analyzed longitudinally linked data from a prospective cohort of advanced cancer patients in 23 palliative care units in Japan and a nationwide survey of bereaved families.
Measurements:
Sudden unexpected death was assessed using previously reported definitions: (1) “surprise death” and (2) “rapid decline death,” evaluated from both physician and bereaved family perspectives, and (3) “performance status-defined sudden death,” evaluated only by physicians. Agreement among definitions was analyzed using kappa statistics. Bereaved families’ mental health was evaluated using the Patient Health Questionnaire-9.
Results:
Among 611 cases, “surprise death” and “rapid decline death” were more frequent from bereaved family (46.5% and 51.2%, respectively) than physician (8.2% and 16.5%, respectively) perspectives. Agreement between family and physician perspectives was low (κ = 0.04–0.14). The bereaved family-perceived “rapid decline death” was significantly correlated with depression (adjusted odds ratio = 1.75, p = 0.028), whereas physician-perceived sudden unexpected death showed no significant correlation.
Conclusions:
Compared with physicians’ perspectives, bereaved family members perceive death to be sudden or unexpected more frequently and differently, and their perceptions are associated with postbereavement mental health. Further research is needed to explore strategies to improve communication and support families’ psychological preparedness when a patient’s death may be sudden and unexpected.
Key Message
Bereaved families perceive death to be sudden or unexpected more frequently than physicians. Addressing this discrepancy is critical for improving the quality of both palliative care and bereavement support.
Introduction
In the general population, bereaved family members who unexpectedly lose loved ones face a significantly higher risk of developing major depressive disorder, panic disorder, and post-traumatic stress disorder.1,2 Prolonged grief disorder (PGD) is an atypical grief response recently included in diagnostic guidelines worldwide, characterized by severe and persistent yearning or preoccupation; emotional pain; identity disturbance; loss of meaning and purpose; other cognitive, physical, or behavioral disruptions; and functional impairment beyond social, cultural, and religious norms. A recent meta-analysis confirmed that unexpected death is among the most consistent predictors of PGD.3,4
Patients with advanced cancer typically experience a predictable functional decline, including gradual decreases in performance status (PS) and oral intake, ultimately leading to death. 5 However, some patients experience rapid clinical deterioration, resulting in sudden unexpected death, even in the terminal phase. 6 Even in palliative care settings where the life expectancy of patients is often expected to be short, sudden unexpected death could have a negative impact on patients, families, and health care providers. 7 Sudden unexpected death could not only complicate end-of-life decision-making for patients, families, and health care providers 8 but also impose marked psychological burdens on bereaved families, as the lack of preparedness for death has been identified as a distinct risk factor for complicated grief in palliative care settings in Japan. 9 Witnessing life-threatening events such as suffocation or fatal bleeding may further exacerbate their emotional distress. 7 For some family members, these experiences may be traumatic, warranting individualized psychological support, such as trauma-focused therapy or bereavement-oriented counseling.
Previous studies on sudden unexpected deaths in terminally ill patients with cancer within hospice/palliative care units were mostly limited to small case studies, and the definition of sudden unexpected death varies across studies, leading to a wide range of reported frequencies, ranging from 0.5% to 42%.8,10–13 In our prior multicenter prospective cohort study, we evaluated the incidence of sudden unexpected death of patients with advanced cancer using four proposed definitions: (1) rapid decline death, defined as a sudden death preceded by rapid (one to two days) functional decline 8 ; (2) surprise death, defined if the primary responsible palliative care physician answered “yes” to the question: “Were you surprised by the timing of the death?” (surprise question) 12 ; (3) unexpected death, defined as a death that occurred earlier than expected by the primary responsible palliative care physician8,11; and (4) PS-defined sudden death, defined as a sudden death that occurred within one week of functional status assessment with an Australia-modified Karnofsky Performance Status (AKPS) of 50 or greater, 13 within a large single cohort. 6 We found that 30-day cumulative incidences of sudden unexpected death varied widely, ranging from 6.4% to 16.8% depending on the definitions. 6
In all these studies, sudden unexpected death was determined based on the physicians’ perspectives or objective criteria, without considering the perspectives of patients and family members. It remains unknown how bereaved families perceive sudden unexpected death or whether sudden unexpected death affects the psychological well-being of bereaved family members. The aims of this study were to address these gaps by investigating (1) the frequency of sudden unexpected death in hospice/palliative care units in Japan from the perspective of bereaved family members, (2) the agreement between bereaved family members and health care providers regarding whether patients’ deaths were sudden and unexpected, and (3) the relationship between sudden unexpected death and mental health of bereaved family members. This study clarifies potential perception gaps between physicians and bereaved families, helping to promote strategies that improve communication and support families’ emotional preparedness for the end of life.
Methods
Study design and participants
We conducted two large surveys in hospice/palliative care units in Japan 14 : (1) a multicenter prospective cohort study to clarify the dying process of patients with advanced cancer (East Asian Collaborative Cross-Cultural Study to Elucidate the Dying Process: EASED, UMIN000025457), and (2) a nationwide questionnaire survey of bereaved family members of deceased patients with cancer (the Japan Hospice and Palliative Care Evaluation study [J-HOPE 4]). We longitudinally linked the EASED patients’ data and corresponding bereaved families’ data from the J-HOPE 4 study, ensuring that both datasets referred to the same patient population. This allowed us to longitudinally examine the relationship between patients’ clinical course before death and perspectives of their bereaved families after death.
In the EASED study, consecutive eligible patients with advanced cancer admitted to 23 hospices/palliative care units between January 2017 and June 2018 were enrolled. 15 Inclusion criteria were (1) adult patients (aged ≥18 years), (2) patients diagnosed with locally extensive or metastatic cancer, and (3) patients admitted to inpatient hospices/palliative care units. Patients who were scheduled to be discharged within a week or did not want to participate were excluded. All enrolled patients were followed up for up to six months or until death.
In the J-HOPE 4 study, we conducted a nationwide questionnaire survey of bereaved family members of deceased cancer patients between May and June 2018. The inclusion criteria were (1) bereaved family of patients with cancer who died before January 2018 and (2) adult family members (aged ≥20 years). The exclusion criteria were (1) received < 3 days of palliative care, (2) unavailability of bereaved family members, (3) death associated with treatment or that occurred in an intensive care unit, (4) bereaved family members’ history of severe psychological distress, and (5) bereaved family members’ inability to complete a self-reported questionnaire because of a health issue, such as cognitive impairment or visual disability. We sent a self-reported questionnaire to bereaved families asking them to respond within a month.
Data collection
We evaluated sudden unexpected death using definitions adopted from previous studies, based on the physicians’ assessments in the EASED study and bereaved family assessments in the J-HOPE 4 study. Importantly, both datasets referred to the same cohort of patients, allowing for direct comparison between physicians’ and families’ perspectives on sudden unexpected death.
In the EASED study,
6
primary responsible palliative care physicians assessed whether patients’ deaths were sudden unexpected death using four different definitions proposed in the literature to ensure methodological consistency and comparability. These definitions were “rapid decline death,” “surprise death,” “unexpected death,” and “PS-defined sudden death.” Because “surprise death” and “unexpected death” are conceptually similar, we chose “surprise death” as the representative subjective definition in the current analysis. Consequently, we used three definitions for the current analysis, as follows:
“Surprise death,” defined if the primary responsible palliative care physician answered “yes” to the following question: “Were you surprised by the timing of the death?”
12
“Rapid decline death,” defined as a sudden death following rapid (one to two days) functional decline.
8
“PS-defined sudden death,” defined as a death that occurred within one week of functional status assessment with AKPS of 50 or greater.
13
AKPS is a measure of the patient’s overall PS, ranging from 10 to 100, assigned by a clinician based on observations of a patient’s ability to perform common tasks relating to activity, work, and self-care. An AKPS of 50 or greater indicates that the patient requires considerable assistance and medical care but is not completely bedridden.
16
In the J-HOPE4 study, we asked bereaved families to evaluate whether a patient’s death was a “surprise death” or “rapid decline death” using the same definitions as in the EASED study. “Surprise death” was assessed by asking family members to respond on a 4-point scale to the question: “Were you surprised by the timing of the patient’s death compared with your expectations?” The four response options were “agree,” “slightly agree,” “slightly disagree,” and “disagree.” Responses of “agree” or “slightly agree” were classified as “surprise death.” “Rapid decline death” was assessed by a binary question: “Did the patient experience a sudden deterioration and pass away within 1–2 days?” They chose between “applicable” and “not applicable,” and those who answered “applicable” were categorized as “rapid decline death.”
Additionally, we collected their demographic data, including age, sex, relationship with the patient, education level, and a history of mental illness. To evaluate the psychological distress of bereaved families, we used the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 is a self-assessment questionnaire commonly used to screen for and assess the severity of depression in clinical practice and research. 17 The reliability and validity of this scale, including its Japanese version, have been established. 18 It consists of nine questions, and responses are rated on a scale of 0–3, with total scores ranging from 0 to 27. A total score of more than 10 indicates that the responder is likely to develop major depressive disorder. 17
Statistical analysis
We summarized the baseline demographic data using descriptive statistics and calculated the frequency of sudden unexpected deaths using different definitions. Agreement among definitions was assessed using kappa statistics. To examine the relationship between sudden unexpected death and bereaved family psychological distress, we conducted univariate and multivariate logistic regression analyses, with a PHQ-9 score of ≥10 as the dependent variable. Sudden unexpected death, as perceived by health care providers and bereaved family members, was included as an independent variable. The multivariate model was adjusted for bereaved family members’ age, sex, relationship with the deceased, and preexisting and/or prior mental illness to control for potential confounders. A p value < 0.05 was considered significant. All statistical analyses were performed using JMP® Pro 14 (SAS Institute Inc., Cary, NC).
Ethical considerations
In the EASED study, we followed the ethical guidelines for human research of the Ministry of Health, Labour, and Welfare in Japan. Informed consent from the patients was waived because of the observational nature of the study. The EASED study was approved by the institutional review board of Seirei Mikatahara General Hospital (the coordinating institution; research no. 16-22) and the institutional review boards of all participating institutions. In the J-HOPE 4 study, we sent a document informing of the aims and procedures of the study along with the questionnaire. The return of a completed questionnaire constituted consent to participate. The J-HOPE4 study, including combined data analysis with the EASED study, was approved by the institutional review board of Tohoku University Hospital (the coordinating institution; approval no. 2017-2-236-1) and institutional review boards of all participating institutions.
Results
A total of 1324 bereaved families were contacted, and 865 (65.3%) returned the questionnaires. After excluding incomplete responses, 611 (46.1%) were included in the final analysis. The baseline characteristics of bereaved families and patients are summarized in Tables 1 and 2. The mean age of bereaved family members was 61.0 years old (SD: 12.4), and 62.5% were female. The most common relationships with the patient were spouse (44.2%) and child (40.3%). Preexisting and existing mental illnesses were reported in 12% of bereaved family members.
Characteristics of Bereaved Families
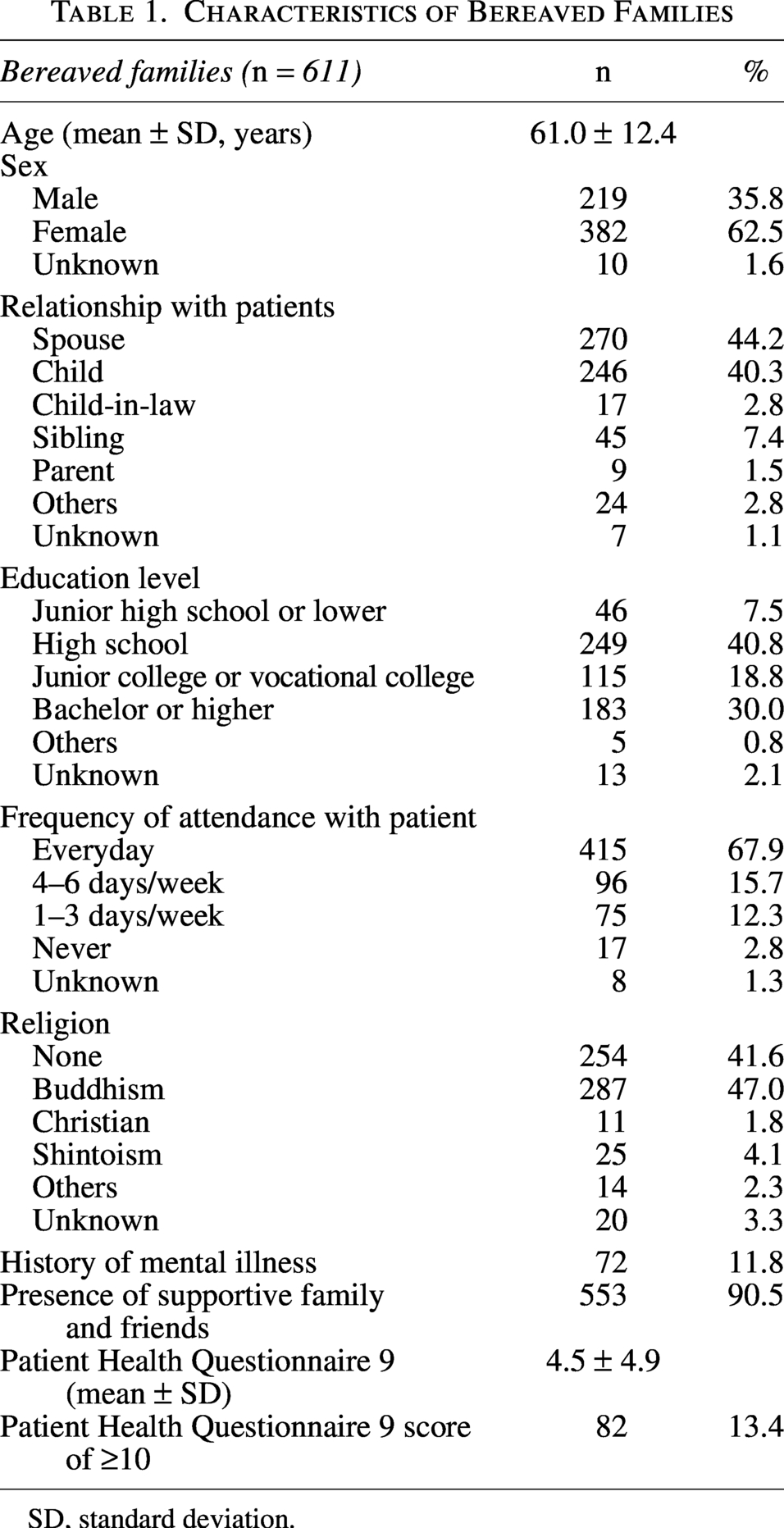
SD, standard deviation.
Patient Characteristics
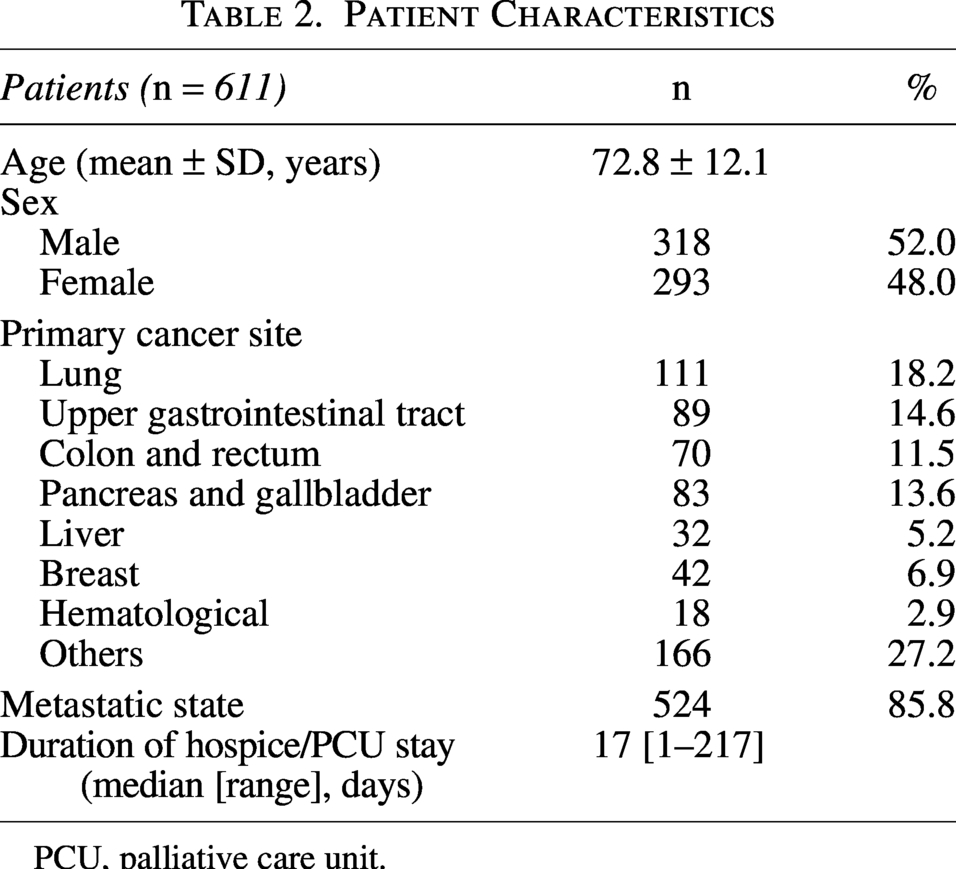
PCU, palliative care unit.
Prevalence of sudden unexpected death based on bereaved family and physician perspectives
Table 3 shows the prevalence of sudden unexpected death from the perspectives of bereaved family members and responsible physicians. From the bereaved family perspective, 51.2% (95% CI: 47.3–55.2) of cases were classified as “rapid decline death,” while 46.5% (95% CI: 42.6–50.4) were categorized as “surprise death.” In contrast, physicians identified only 16.5% (95% CI: 13.8–19.7) of cases as “rapid decline death” and 8.2% (95% CI: 6.3–10.6) as “surprise death.” The prevalence of “PS-defined sudden death,” which is based on an objective clinical definition, was the lowest at 6.5% (95% CI: 4.9–8.8).
Prevalence of Sudden Unexpected Death by Definitions
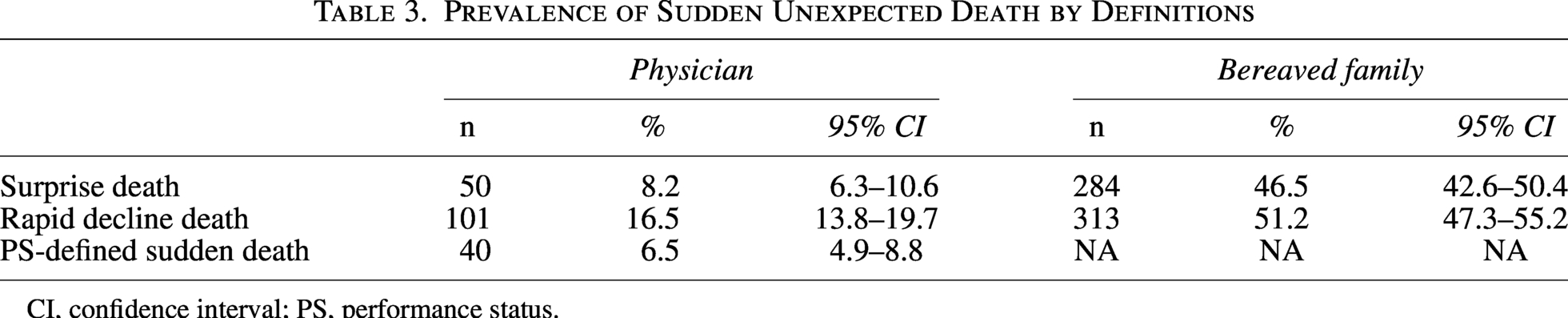
CI, confidence interval; PS, performance status.
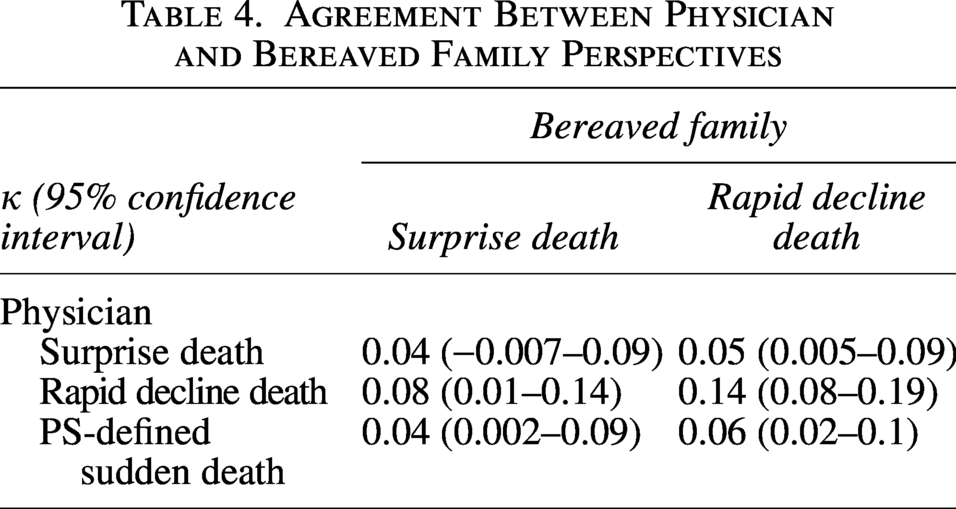
Agreement between bereaved family and physician perceptions of sudden unexpected death
The agreement between bereaved family and physician perceptions was evaluated using kappa statistics (Table 4). Across all definitions, agreement was consistently low, with κ values ranging from 0.04 to 0.14.
Agreement Between Physician and Bereaved Family Perspectives
Relationship between sudden unexpected death and PHQ-9 score
Among all bereaved family members, 82 (13.4%) had PHQ-9 scores of 10 or higher, suggesting probable major depressive disorder. In the univariate analysis (Table 5), bereaved family members with a PHQ-9 score of ≥10 were significantly more common in families who reported that patients had experienced a “rapid decline death” (17% vs. 11%, respectively, p = 0.030) and those who reported that the patients had a “surprise death” (17% vs. 11%, respectively, p = 0.029). In contrast, none of the three physician-defined sudden unexpected deaths were significantly correlated with the prevalence of depression among bereaved family members. Bereaved family members who classified the death as a “rapid decline death” had a mean PHQ-9 score of 5.0 ± 5.3, compared with 3.9 ± 4.3 among those who did not perceive the death as a “rapid decline death.” Similarly, those who classified the death as a “surprise death” had a mean PHQ-9 score of 5.3 ± 5.2, compared with 3.8 ± 4.5 among those who did not perceive the death as a surprise. In the multivariate analysis, after adjusting for age, sex, relationship with the deceased, and history of mental illness, a bereaved family-perceived “rapid decline death” remained significantly correlated with a higher risk of postbereavement depression (adjusted odds ratio = 1.75, 95% CI: 1.06–2.93, p = 0.028). In contrast, none of the physician-defined sudden unexpected deaths (i.e., “rapid decline death,” “surprise death,” and “PS-defined sudden death”) were significantly correlated with higher PHQ-9 scores.
Relationship Between Sudden Unexpected Death and Patient Health Questionnaire 9 Score
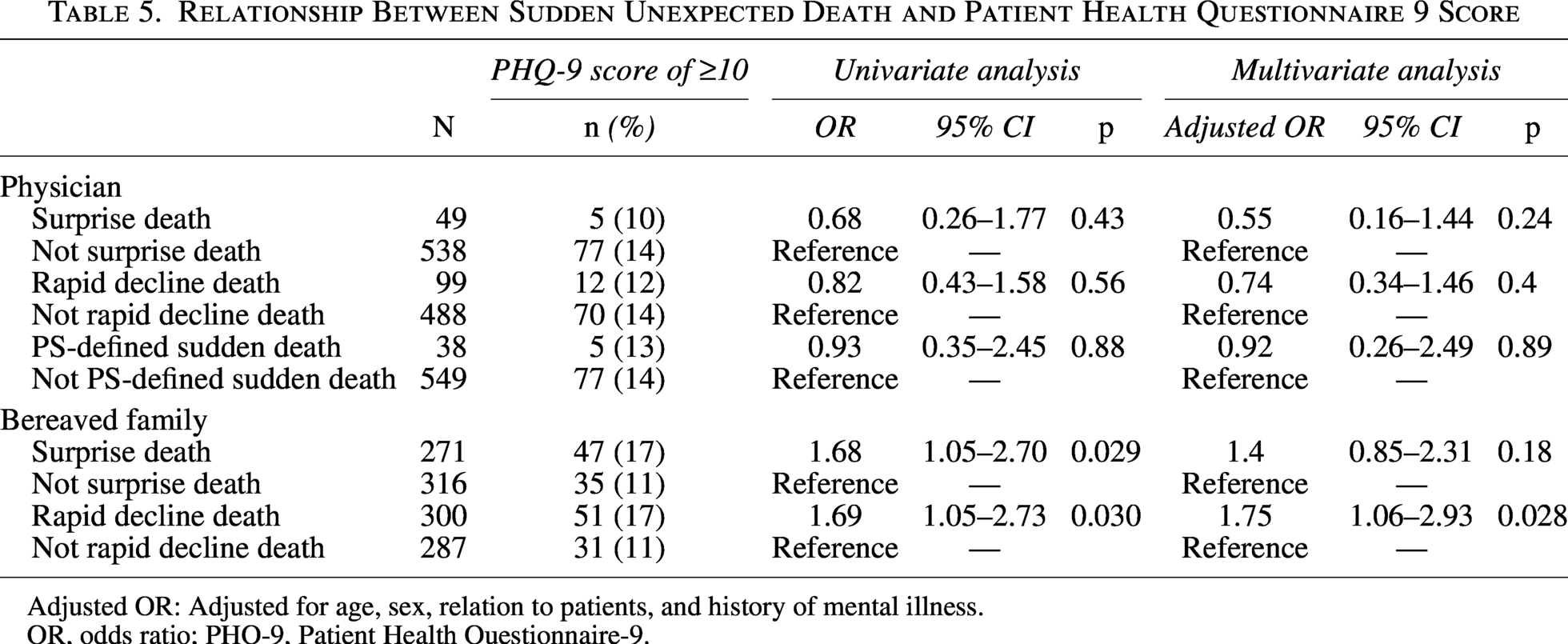
Adjusted OR: Adjusted for age, sex, relation to patients, and history of mental illness.
OR, odds ratio; PHQ-9, Patient Health Questionnaire-9.
Discussion
To the best of our knowledge, this study is the first to evaluate bereaved family perspectives on sudden unexpected death in hospices/palliative care units. By integrating a prospective observational study with a bereaved family survey in a single cohort, we were able to assess the prevalence of sudden unexpected death from the bereaved families’ perspective and examine the level of agreement between bereaved families and physicians. This approach allowed us to gain a clearer understanding of the end-of-life experience from both health care providers’ and bereaved families’ perspectives.
One of the key findings of this study was that nearly half of bereaved families perceived the patients’ death as sudden and unexpected. In contrast, the physician-assessed incidence of sudden unexpected death was comparable with previous reports, indicating that the frequency of sudden unexpected death as perceived by bereaved families is markedly higher than that reported by health care providers.6,8,11–13 This finding indicates that the incidence of sudden unexpected death in hospice/palliative care settings differs according to the perspectives and definitions and emphasizes the importance of clearly specifying the perspective selected in future research.
Another important finding of this study was the significant discrepancy between how bereaved families and physicians perceived sudden unexpected death. This discrepancy likely reflects the fact that physician-defined and family-perceived sudden deaths capture different aspects of the dying process or reflect different levels of preparedness for death. In Japan, it is recommended that end-of-life discussions with patients and their families include not only prognosis predictions but also the possibility of sudden unexpected death. 19 However, it is well-documented that there is a discrepancy in prognoses among patients, family members, and physicians.20,21 Our findings suggest that similar gaps are present in perceptions of sudden, unexpected death. Effective communication and psychosocial support are central components of end-of-life care and known to improve families’ preparedness for the dying process, highlighting the importance of addressing these perceptual gaps in clinical practice.22–24 When discussing the possibility of sudden unexpected death, health care providers should acknowledge that the concept of sudden unexpected death itself lacks a standardized definition and its interpretation may vary depending on the criteria used and perspectives of physicians and families, ensuring careful and thorough communication. Especially in inpatient hospices and palliative care units, family members often spend limited time with the patient, making it more difficult for families to observe gradual changes in the dying process. Providing families with a clearer picture of the patient’s day-to-day condition in inpatient settings may help them better understand the dying process and feel more emotionally prepared. Although our study did not identify strong associations between demographic variables and family-perceived sudden unexpected death (shown in Supplementary Table), additional studies are needed to identify factors associated with families’ perceptions of sudden unexpected death.
Our exploratory analysis revealed that bereaved family members who perceived the death as sudden and unexpected had higher PHQ-9 scores, indicating major depressive symptoms. Since the J-HOPE 4 study is a cross-sectional survey, this relationship cannot be interpreted as causal. It remains unclear whether perceiving the death as sudden and unexpected contributed to psychological distress or whether family members with preexisting vulnerability to depression were more likely to interpret the death as sudden. Moreover, although our multivariable analysis adjusted for several family characteristics, including age, sex, relationship with the patient, and mental health conditions, bereavement outcomes are also influenced by factors such as emotional closeness to the deceased, economic hardship, and religious or spiritual coping.25–27 While the influence of religious involvement and economic disparities may be relatively modest in Japan, these factors could still be potential confounders.28,29 In contrast, physician-defined sudden unexpected death showed no association with depressive symptoms. This finding may be supported by prior research indicating that bereaved family members who feel less prepared for a loved one’s death are at higher risk of major depression and complicated grief, suggesting that families’ subjective sense of preparedness may be more relevant to psychological outcomes than the clinical or prognostic unexpectedness recognized by health care providers. 9 Additionally, “PS-defined sudden death” is not associated with the PHQ-9 score. This finding might be explained by the Japanese attitude toward death. Not being a burden to others and maintaining a sense of control are well-documented contributing factors to achieving a good death in Japan.30,31 The rapid PS decline itself may not place a significant burden on caregivers. Further observational studies and qualitative research involving physicians, patients, and their families are needed to better understand the factors that lead families to perceive a death as sudden and unexpected, as well as the causal relationship between such perceptions and bereavement outcomes. Understanding these factors will allow health care providers to address concerns proactively during the patient’s care, ensuring that families are better prepared and supported throughout the end-of-life and bereavement process. Thus, patient- and family-centric care models will be essential for improving communication and emotional support in palliative and bereavement care. Additionally, broader questions such as how best to support families in preparing for death, whether through public health-level interventions or targeted support for those at risk of prolonged grief, are important but beyond the scope of this study. Future research will be needed to determine when and how such interventions should be implemented to optimize bereavement outcomes.
This study had several limitations. First, participants were limited to those who had lost family members due to advanced cancer in hospices/palliative care units in Japan. Therefore, our findings may not be generalizable to other settings. Future research on sudden unexpected death in other settings, such as home care settings, general hospital wards, and noncancer patients, should be considered. Our findings highlight the fact that it will be essential to clearly define assessment measures and specify whose perspectives will be used for evaluation. Second, the J-HOPE 4 was an after-death survey among bereaved family members with a moderate response rate (65.3%), which may have introduced some selection bias. However, similar response rates were reported in previous national surveys from both the United States and Japan,32,33 suggesting that this limitation is justifiable. Third, there might be recall bias due to the timing of the questionnaire survey. However, several previous studies conducted from 3 to 12 months after the death of the patient suggested that this interval is reasonable for both recall bias and the grieving process.34,35 Fourth, distressed or psychologically troubled families may be less likely to reply to this questionnaire survey. Fifth, possible depression and complicated grief were evaluated using PHQ-9. This is a screening tool and is not intended for definitive diagnoses. Sixth, we could not account for all potential confounders. Thus, the possibility of unmeasured or unknown confounding remains. Last, data were collected in 2018 from patients who died in 2017, which may limit the timeliness of our findings. However, these data remain among the most comprehensive and nationally representative sources available for evaluating end-of-life care in Japan.
In conclusion, we evaluated sudden unexpected death in patients with advanced cancer in hospice/palliative care units from the perspective of bereaved families. Compared with physicians’ perspectives, bereaved families perceive patients’ death as sudden and unexpected more frequently and differently. Our findings emphasize the importance of recognizing and addressing the gap between physicians’ and families’ perceptions of sudden unexpected deaths and highlight the need for enhanced communication and psychological preparation of families during end-of-life care. Integrating these perspectives may help health care providers anticipate and mitigate the emotional impact of sudden unexpected death on bereaved families, ultimately improving both palliative and bereavement care.
Footnotes
Funding Information
This study was part of the EASED and J-HOPE 4 studies, funded by the Japan Hospice Palliative Care Foundation. This study was partially supported by grant JP23K27830.
Disclosure Statement
The authors declare no conflicts of interest.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.