
Abstract
Background:
Providing and measuring goal-concordant care is a priority.
Objective:
Determine the effect of a nurse and social worker palliative telecare team intervention on goal concordance and participants’ understanding of care focus.
Design:
Randomized clinical trial of a palliative telecare intervention called Advancing Symptom Alleviation with Palliative Treatment (ADAPT). As part of ADAPT, a study nurse and/or social worker had a serious illness conversation via phone.
Setting/Subjects:
Participants had cardiopulmonary disease and poor quality of life in two VA health systems.
Measurements:
Goal concordance was measured with two questions modified from the SUPPORT study, using a Likert scale from 0 (I prefer medical care that focuses on extending life) to 10 (I prefer medical care that focuses on relieving pain and discomfort). Participants could choose, “I am unsure” when asked about the focus of their current medical care. Goal concordance was defined when participants reported the same preference and focus of care. Using linear mixed modeling, changes in proportions of concordant and unsure participants were examined from baseline to six months.
Results:
The 306 participants enrolled in the ADAPT trial were predominantly white (80.1%) and male (90.2%), with a mean age of 68.9 (standard deviation: 7.7) years. There was no difference in the change in proportions of concordant participants in the intervention group compared to usual care (adjusted difference in change in proportions: 4.2%; p = 0.67) or the change in proportions of unsure participants (adjusted difference in change of proportions: 6.2%; p = 0.42).
Conclusion:
The intervention did not influence goal concordance or the proportion of participants unsure of care focus.
Key Statements
What is already known about this topic?
Providing goal-concordant care is essential for high-quality medical care. Interventions to facilitate serious illness communication have shown mixed results in the outcome of goal concordance.
What this paper adds
A randomized clinical trial of a nurse and social worker palliative telecare team intervention, including a telephonic serious illness conversation, did not influence goal concordance or the proportion of participants reporting they were unsure of the focus of their health care.
Implications for practice, theory, or policy
Measuring and achieving goal concordance is challenging in patients whose goals include elements of both life prolongation and comfort. A more specific focus for goal concordance may need to be measured, such as having patients prioritize goals and values and determine alignment with current health care priorities or decisions. Including questions about goal concordance in serious illness communication guides should be considered.
Introduction
Providing health care matched to patient values and goals, or “goal-concordant care,” is essential for high-quality medical care.1–4 Goal-concordant care is facilitated by communication between patients, their caregivers, and clinicians in which a patient’s illness understanding, preferences, values, and medical decisions are addressed. These kinds of conversations are termed “serious illness communication (SIC).” 5 Prior studies of interventions to facilitate SIC have demonstrated mixed effects in patient- and family-reported goal concordance,6–12 with some studies showing an improvement in goal-concordant care, 8 others not, 12 and other studies finding that likelihood of goal-concordant care differed by patient goal (e.g., comfort versus life-prolonging treatment). 13
In this report, we describe the effect of the Advancing Symptom Alleviation with Palliative Treatment (ADAPT) intervention on goal concordance, a prespecified secondary outcome. In the ADAPT intervention, a nurse and social worker (SW) team provided a palliative telecare intervention including symptom management and counseling sessions. 14 One session used a structured SIC guide, 15 which was created by following recommendations for best practices for SIC and prior research on patients’ end-of-life preferences.16–18 In a conceptual model based on earlier work by Street et al., 19 goal-concordant care is a downstream outcome of SIC. 5 The objective of this study was to determine the effect of the ADAPT intervention on (1) the proportions of participants reporting goal-concordant care, (2) the proportions of participants unsure of the focus of their care, and (3) a composite outcome of both (1) and (2) from baseline to six months.
Methods
The ADAPT study was a randomized clinical trial that compared a nurse and SW palliative telecare team to usual care for participants with chronic obstructive pulmonary disease (COPD), heart failure (HF), or interstitial lung disease (ILD) at two Veterans Health Administration health systems in the United States. This study was registered at clinicaltrials.gov (identifier: NCT02713347, https://clinicaltrials.gov/ct2/show/NCT02713347). The study was funded by VA HSR&D IIR 14–346 (Bekelman, Principal Investigator). The study protocol was approved by the Colorado Multiple Institutional Review Board (15-1891) and the Veteran’s Administration Puget Sound Multiple Institutional Review Board (00857). All participants provided informed consent for the study.
ADAPT intervention
At the start of the intervention, a registered nurse (RN) helped participants choose a target symptom (e.g., fatigue, dyspnea, and depression) and then over six months used motivational interviewing and a symptom-specific algorithm to help the patient manage the symptom. An SW provided psychosocial counseling based on components of interpersonal psychotherapy. Each SW visit focused on a specific topic: Self-care, deep breathing and relaxation, how to ask for and accept help from others, and setting goals. The RN and SW met weekly with a team of a primary care clinician, a palliative care specialist, and, as needed, support from cardiology or pulmonary specialists. During these meetings the RN and SW would present to the group. If medical recommendations were made (e.g., ordering a test, a medication, a referral to another subspecialist such as physical therapy), the RN would discuss the orders with the patient, and the study nurse would place these orders for the primary care clinician to sign. In one telephone visit, the RN and/or SW used a structured SIC guide, which explored participants’ illness understanding and preferences for future care (Supplementary Data). 15 The communication guide explored the patient’s preferences for medical care (e.g., focusing on comfort, knowing this may mean not living as long, versus focusing on living longer and tolerating more procedures). Notably, the guide did not explore patient perceptions of the focus of their current medical care nor the alignment between their preferences for care and the focus of their current care. The conversations were documented by the RN and/or SW in the electronic medical record, and participants completed an advance directive, if appropriate. Study accrual occurred between October 2016 and April 2020, ending when the goal sample size was accrued. The intervention continued until October of 2020. The intervention lasted an average of 115.1 days (standard deviation of 33.4 days). 14 The data collection ended in 2021.
Measures/analysis
Goal concordance was assessed based on two questions modified from the SUPPORT study 20 , 21 (Supplementary Data and Brief Communication). The RN and SW did not ask these questions as part of the intervention. Participants self-reported responses to research assistants at baseline and six months. We collected all outcomes by patient report via mail or phone survey by research assistants at baseline and six months for consistency. Further, the research assistants who collected outcomes by phone were blinded to randomization, and the nurse and SW were not involved in outcome collection to minimize bias. The six-month follow-up was chosen to be close to the intervention, and we were concerned with loss to follow-up with a longer interval.
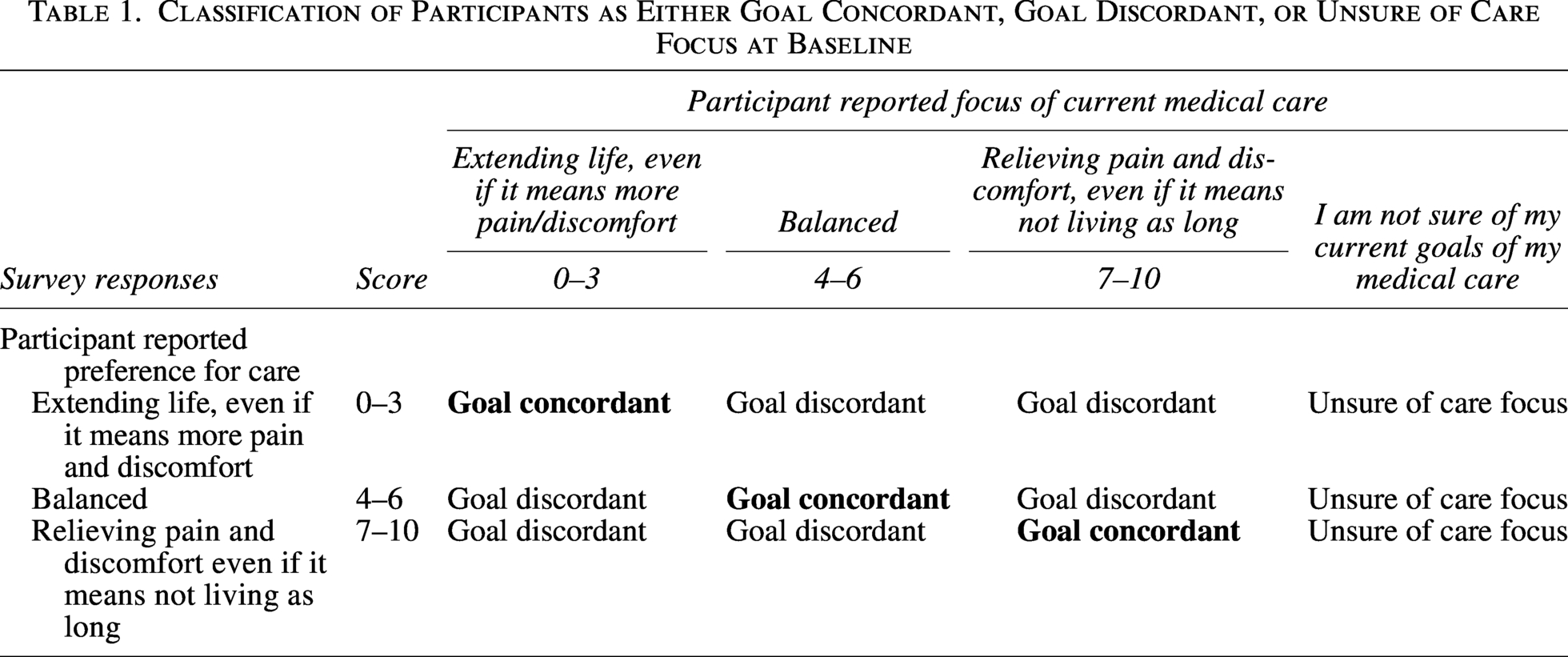
Classification of goal-concordant versus discordant versus unsure of care focus
Prior to analysis, each participant was classified as goal concordant, unsure of care focus, or goal discordant (Table 1). Participants who answered, “I am not sure of my current goals of my medical care” were not considered concordant or discordant and were labeled “unsure of care focus.” We performed an exploratory sensitivity analysis to determine the effect of changing the cutoffs for what was considered concordant (changing cutoffs, Supplementary Tables S3A-D; numbers of participants in each group with changing cutoffs, Supplementary Tables S4A-D). Models testing the change in proportion of participants reporting goal-concordant care and the change in proportion of participants unsure of the focus of their care were fit using a linear mixed model, including treatment status, time, a treatment status by time interaction, and disease status (COPD, CHF, ILD, or CHF and/or COPD) as covariates, with a random intercept for participant. The model testing a change in the composite outcome of both (Model 3) was fit as a linear model with treatment status and disease status as covariates. Additional statistical analysis details are in the Supplementary Data.
Classification of Participants as Either Goal Concordant, Goal Discordant, or Unsure of Care Focus at Baseline
Results
Among the 306 participants enrolled in the ADAPT trial, participants were predominantly white (80.1%) and male (90.2%). The mean age of participants was 68.9 years. Participants had COPD (58%), HF (22%), COPD and HF (16%), or ILD (4%). In the intervention group, 122/154 (79.2%) had a SIC visit documented during the intervention. 21 Intervention fidelity data are available in Table 2 and the Supplementary Data.
Serious Illness Communication Session Fidelity Data in Advancing Symptom Alleviation with Palliative Treatment Intervention Group

Baseline
Among those who reported a care preference, 60.4% prioritized pain relief, 27.3% were balanced, and 12.2% prioritized extending life (Supplementary Table S1). Among those who reported a focus of care, 25.9% prioritized pain relief, 25.2% were balanced, 11.2% prioritized extending life, and 37.8% were unsure of the focus of their care (Supplementary Table S1). Among those who described a focus of their care, 36.6% reported care that was concordant with their preferences. At baseline, the proportions of goal-concordant participants were similar between the intervention and usual care groups (Table 3, adjusted difference in proportions: −5.7%, 95% CI: −20.5% to 9.2%, p = 0.45).
Goal-Concordant Participants at Baseline and Six Months in Intervention and Usual Care Groups
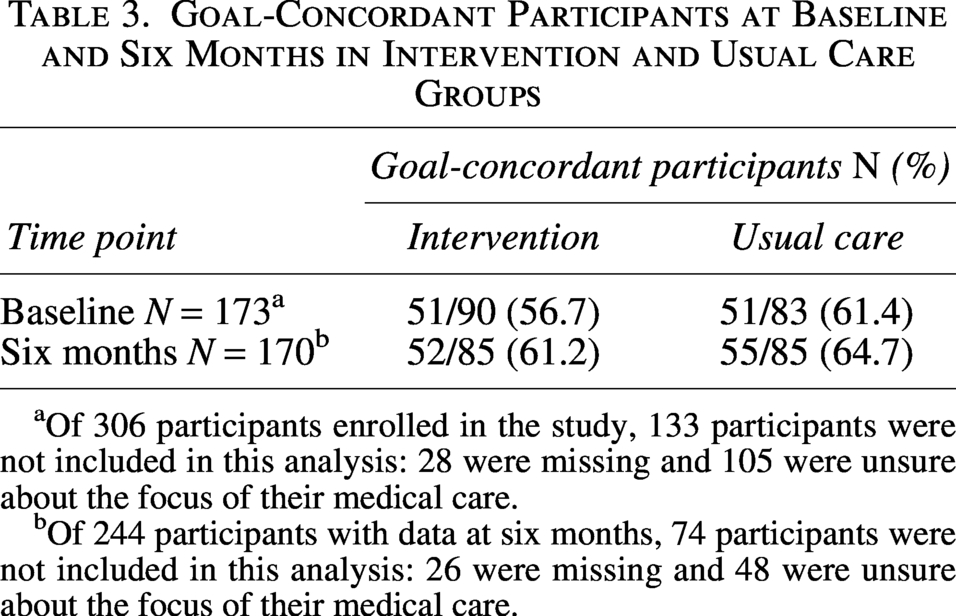
Of 306 participants enrolled in the study, 133 participants were not included in this analysis: 28 were missing and 105 were unsure about the focus of their medical care.
Of 244 participants with data at six months, 74 participants were not included in this analysis: 26 were missing and 48 were unsure about the focus of their medical care.
Six month follow-up
Among those who reported a care preference, 56.4% prioritized pain relief, 31.2% were balanced, and 12.4% prioritized extending life (Supplementary Table S2). Among those who reported a focus of care, 29.4% prioritized pain relief, 33.0% were balanced, and 15.6% prioritized extending life, and 22% were unsure of the focus of their care (Supplementary Table S2). Among those who described a focus of their care, 49% reported care that was concordant with their preferences.
Results of hypothesis testing
There was no significant difference between intervention and usual care in the change in proportions of concordant participants from baseline to six months (adjusted difference in proportions: 4.2%, 95% CI: −14.7% to 23.0%, p = 0.662). These findings did not change significantly in the exploratory sensitivity analyses (Supplementary Tables S4A-D).
Among all participants at baseline,37.8% said they were unsure of care focus, which decreased to 22.0% at six months (Supplementary Tables S1and S2). Proportions of participants unsure of care focus were similar at baseline between the intervention and usual care groups (adjusted difference in proportions: −6.5%, 95% CI: −17.8% to 4.8%, p = 0.26, Table 4). There was no significant difference between intervention and usual care in the change in proportion of participants unsure of care focus from baseline to six months (difference in proportions: −6.2%, 95% CI: −21.4% to 9.0%, p = 0.423, and Supplementary Fig. S2).
Proportions of Participants Who Reported Being Unsure of Care Focus at Baseline and Six Months
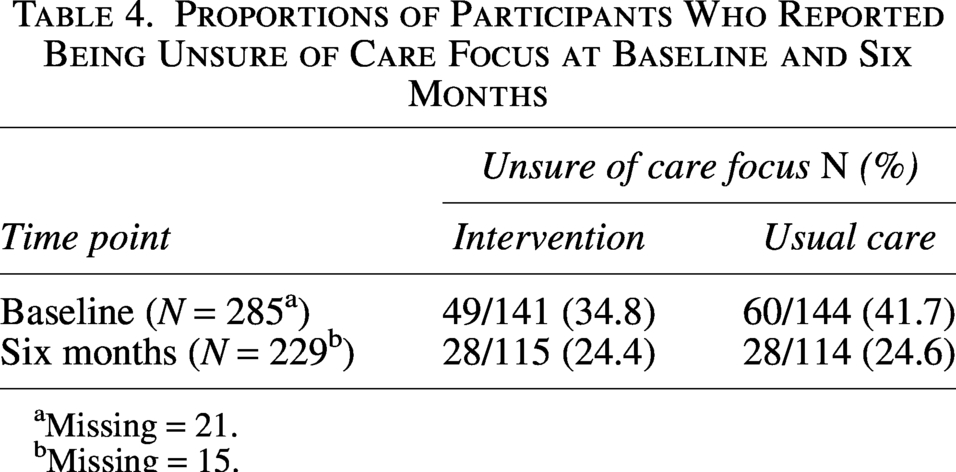
Missing = 21.
Missing = 15.
There were 13/46 (28.3%) participants in the intervention group and 12/43 (27.9%) participants in the usual care group who either moved from goal discordant to concordant or moved from unsure of care focus to goal concordant between baseline and six months. There was no significant difference between intervention and usual care in the proportions of participants who moved from discordant to concordant or unsure of care focus to concordant from baseline to six months with an estimated difference of 0.3% (95% CI: −19.2% to 19.8%, p = 0.978). The sample size for this analysis was 89 participants (46 participants in the intervention group and 43 participants in the usual care group having complete data at both time points; Supplementary Fig. S3).
Discussion
This study sought to determine the effect of the ADAPT intervention on the proportions of participants reporting goal-concordant care, the proportions of participants unsure of the focus of their care, and a composite outcome of both proportions from baseline to six months. A nurse and SW palliative telecare team did not increase the proportion of participants receiving goal-concordant care, decrease the proportions of participants who were unsure of their care focus, or change the proportion of participants who moved from discordant to concordant or from unsure of care focus to concordant from baseline to six months. At baseline, 60% of participants prioritized relieving pain and discomfort, similar to two prior studies9,20 and lower than another study in which 79% prioritized relief of pain and discomfort. 13 We highlight that most patients in our study preferred a focus on relieving pain and discomfort because this contrasts with the medical system that tends to prioritize life prolongation.
This study advances the science of goal concordance by (1) using a measure of whether patients were unsure about their care focus, (2) hypothesizing an intervention would reduce the unsure proportion, and (3) measuring goal concordance prospectively. Prior studies have not measured a proportion of unsure patients, 9 have measured a proportion of unsure patients but not reported on change over time, 8 and others have not prioritized this as an important outcome of SIC.13,20 The proportion of participants unsure of their care focus in our study was higher at baseline (37.8%) compared to other studies. Other studies reported a prevalence of being unsure around 24%,13,20 similar to the prevalence of being unsure at the end of our study. One of these studies included patients with heart and lung diseases and was conducted in a similar area of the United States. 13 In one study of patients in a neurological intensive care unit, the proportion of families unsure of the care focus actually increased over six months (in the absence of an intervention). 22 We found that a substantial proportion of participants in this study did not understand the focus of their medical care and that this proportion decreased over time (24% in both groups at six months). In clinical practice, a discussion of the goals of specific therapies with patients is a part of shared decision-making and may clarify understanding and help patients make decisions aligned with their goals. We recommend a patient’s understanding of their medical care be an outcome of SIC and part of the measurement of goal concordance given the importance of this concept in clinical practice.
There are several potential reasons why the intervention was not associated with an increase in goal concordance or a decrease in the number of participants unsure of care focus. First, the question about a patient’s health care preferences did not allow participants to choose that they were unsure of their preferences. Therefore, our study may not have captured patients’ uncertainty about their health care preferences because the question forced patients to choose along a continuum. Future versions of this question could reveal patient uncertainty by including a response option of “I’m not sure of my current health care preferences.” Second, asking about care focus and preferences in outcome measures may have influenced all participants (Hawthorne effect). Third, asking participants about whether a specific treatment decision is goal concordant (e.g., to pursue antifibrotic therapy for ILD or to pursue an implantable cardioverter defibrillator for HF) instead of their “medical care” overall may yield a clearer question for participants to answer and a discrete task for an intervention to address with targeted communication. A potential future research direction could include creating and testing a concordance matching form in which patients compare their top three goals (such as maintaining functional independence, longevity of life, and living at home) to specific documented care plans (such as using antibiotics for pneumonia). Fourth, the SIC guide and the measures used to determine goal concordance were not well aligned. As a result, it is difficult to determine if the lack of association between the ADAPT intervention and goal concordance is due to a problem with the SIC guide or the outcome measures. The single intervention session on SIC was often devoted to identification of the patient’s values and completion of advance directive documentation, rather than helping patients align current health care with their values and goals. The SIC guide did not specifically direct the nurse or SW to identify goal concordance or resolve discordance. A potential future direction could include modifying the SIC guide to include questions about goal concordance or having multiple SIC sessions, one of which could focus on goal concordance. The SIC sessions were a median of 52 minutes in length, so perhaps adding an additional session would be better than lengthening the existing guide. The patient interviews to collect outcomes after the intervention were not done by the same nurse and SW who conducted the telephone SIC. Therefore, it is possible that the nurse and SW contributed to goal concordance, but this was not captured either because the outcomes were not collected personally by the nurse and SW, and/or the communication guide and the outcome questions were not well-aligned. It is also possible that the nurse and SW SIC discussion had other positive impacts. Other measures would be needed to capture these impacts, such as a measure of whether patients feel “heard and understood. 23
This study has several limitations. First, our study measured participants’ perception of the focus of their care, and clinician perception of the focus of care may have differed from how patients perceived it. Second, the results may not be generalizable to other populations. For example, there may be different results in persons who have historically experienced medical disenfranchisement and overlook of their health care goals. Third, the time interval of six months may be too short to observe a change in care focus for this patient population.
Conclusion
A nurse and SW palliative telecare team intervention did not influence the proportion of participants receiving goal-concordant care, the proportion of participants who were unsure of the focus of their care, or a combination of these two from baseline to six months between the intervention and usual care groups among participants with cardiopulmonary illnesses and poor quality of life.
Authors’ Contributions
A.V.L.: Conceptualization, methodology, writing—original draft, and visualization. E.H.: Conceptualization, methodology, software, validation, formal analysis, data curation, and writing—review and editing. A.E.B.: Methodology, writing—review and editing, and supervision. G.P.: Visualization and writing—review and editing. B.M.: Investigation, resources, data curation, writing—review and editing, and project administration. L.D.: Visualization and writing—review and editing. E.G.C.: Methodology and writing—review and editing. D.B.B.: Conceptualization, methodology, visualization, writing—review and editing, supervision, and funding acquisition.
Footnotes
Acknowledgments
The authors would like to thank Laura Scherer, PhD, for her assistance with goal concordance definition and statistical analysis planning.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
The ADAPT trial was funded by VA HSR&D IIR 14-346 (Bekelman, PI). The funder of the study had no role in study design, data collection, analysis, interpretation of the data, writing this article, or deciding to submit this report for publication.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.