
Abstract
Background:
Advance care planning (ACP) improves end-of-life care and communication; however, its long-term effects on bereaved family members remain underexplored.
Objectives:
This study aimed to (1) examine how bereaved family members’ participation in a deceased cancer patient’s ACP influenced their own ACP behavior and (2) explore its impact on their interpersonal relationships and values regarding life and death.
Design:
A nationwide, cross-sectional, anonymous questionnaire survey was conducted as part of the Japan Hospice and Palliative Evaluation Study 4.
Setting/Subjects:
Participants were bereaved family members of cancer patients who had received care at designated palliative care units in Japan and had died before January 31, 2018.
Measurements:
The survey assessed bereaved individuals’ ACP behavior (thinking about, discussing, or documenting preferences), discussion partners, and psychological outcomes. Logistic regression analyses identified factors associated with ACP engagement.
Results:
Of the 639 questionnaires returned (response rate: 63.5%), 544 valid responses were analyzed. Among respondents, 75% had thought about their own ACP, 42.1% had discussed it, and 7.9% had documented it. Participation in a loved one’s ACP was significantly associated with thinking about (odds ratio [OR] = 5.07) and discussing (OR = 2.46) one’s own ACP. Conversations were linked to increased trust, emotional understanding, and reduced anxiety.
Conclusions:
Participation in a loved one’s ACP was associated with greater engagement in bereaved individuals’ own ACP, along with enhanced interpersonal trust and reflection on life and death. These findings support viewing ACP as a relational and life-oriented process.
Key Messages
Engagement in advance care planning (ACP) was associated with psychological benefits among bereaved individuals, including enhanced trust, emotional understanding, and reduced anxiety. These findings underscore the relational and identity-affirming dimensions of ACP, positioning it as a reflective, meaning-making process that extends beyond its clinical and legal functions.
Introduction
Advance care planning (ACP) is associated with improved goal-concordant care and quality of life for patients with advanced illness, as well as enhanced trust, communication, and emotional preparedness among family caregivers.1–3 However, evaluating ACP outcomes remains challenging, and findings have been heterogeneous across studies. 4 Systematic reviews suggest consistent improvements in proximal outcomes, such as readiness to engage in ACP and documentation of preferences, whereas evidence for more distal outcomes—including psychological well-being and family adjustment—remains limited and inconsistent. 5
Few studies have examined how participation in a loved one’s ACP affects bereaved family members over time, although existing evidence suggests that those involved in ACP with someone close are more likely to engage in their own ACP.6,7 This gap is particularly relevant given contemporary perspectives that conceptualize ACP as an ongoing, multistage process of reflecting on, discussing of, and documenting personal values, rather than a single end-of-life conversation. 8 This process-oriented view suggests that engagement in one stage may influence subsequent behaviors and relational outcomes.
In Japan, ACP is commonly practiced in a family-centered manner, reflecting cultural norms of relational decision-making.9,10 Discussions are often embedded in ongoing family communication rather than formal documentation, highlighting the central role of close relationships in end-of-life planning. Such family-centered practices may influence how bereaved individuals subsequently engage in their own ACP.
Despite growing recognition of the relational and process-oriented aspects of ACP, little empirical research has examined the long-term impact of participation in a loved one’s ACP on bereaved family members themselves, particularly in family-centered cultural contexts. The present study therefore examined two questions:
How does participation in a deceased cancer patient’s ACP affect bereaved family members’ own ACP behavior (e.g., thinking about, discussing, or documenting preferences)? How does such participation affect their relationships with others and their views on life and death?
Methods
Design
This study employed a nationwide, cross-sectional, anonymous, self-administered questionnaire survey. It aimed to investigate bereaved family members’ participation in the ACP of deceased cancer patients, as well as their own ACP behaviors and interpersonal and psychological outcomes.
Setting and subjects
This study was part of the Japan Hospice and Palliative Care Evaluation Study 4 (J-HOPE4),
11
a nationwide project by
Eligible participants were bereaved family members of cancer patients who had received inpatient care at palliative care units throughout Japan and had died before January 31, 2018. Each participating institution was asked to identify up to 80 bereaved family members using the following inclusion criteria:
The deceased patient was diagnosed with cancer. The patient was aged ≥20 years at the time of death. The bereaved family member was aged ≥20 years.
Exclusion criteria were as follows:
The patient received palliative care for fewer than three days. The contact information of the family caregiver was unavailable. The patient died due to an acute medical or surgical event or in an intensive care unit. The primary physician judged that the bereaved caregiver was experiencing severe psychological distress. The bereaved caregiver was unable to complete a self-administered questionnaire due to health issues or disability.
Questionnaires were mailed to the identified bereaved family members along with a cover letter explaining the purpose and procedures of the J-HOPE4 study. Return of the completed questionnaire was considered consent to participate. A reminder was sent one month later to nonrespondents. Data collection and management were conducted by Tohoku University.
Measurements
The questionnaire included the following three domains:
Bereaved individuals’ ACP-related behaviors
To ensure a common understanding of ACP, the questionnaire began with a short explanation adapted to the Japanese cultural context, describing ACP as preparation for serious illness or loss of decision-making capacity, including discussion of future treatment preferences and desired ways of living or dying. This framing reflected how ACP is typically practiced in Japan—as an informal, relational process embedded in family communication. Respondents’ interpretations of ACP were therefore expected to include both personal reflection and interpersonal dialogue.
Participants were asked whether they had been involved in the deceased patient’s ACP discussions, and whether they had thought about, discussed, or documented their own ACP. The indicator “thought about ACP” captured the initial reflective stage of ACP—considering one’s values and treatment preferences before explicit discussion or documentation. Subsequent items assessed whether respondents had discussed ACP, how frequently, and with whom. The degree of discussion was measured using a five-point scale, and participants identified all relevant discussion partners. They were also asked to indicate which individual had the greatest influence on their ACP thinking.
Psychological outcomes of ACP discussions
Four psychological outcomes were assessed using four-point Likert scales: (1) increased trust in the discussion partner, (2) easier to communicate thoughts and feelings, (3) a stronger sense of being understood by the discussion partner, and (4) reduced anxiety about the future. These variables were chosen based on prior research identifying them as core relational and emotional effects of ACP engagement.3,6,12,13
Quality of end-of-life care and death
The Care Evaluation Scale (CES) 14 and Good Death Inventory (GDI) 15 were included as covariates to account for the perceived quality of end-of-life care and death in relation to bereaved individuals’ ACP engagement.
Statistical analysis
Descriptive statistics were calculated for demographic characteristics, experiences of participating in the deceased patient’s ACP, bereaved individuals’ own ACP behaviors (thinking, discussing, and documenting), attributes of discussion partners, and psychological outcomes.
Univariate analyses were conducted to examine associations between participation in the patient’s ACP and bereaved individuals’ own ACP behaviors. Logistic regression analyses (stepwise method) were then performed to identify factors associated with thinking about one’s own ACP. Predictor variables included the following:
Bereaved individuals’ demographics: age, sex, relationship to the patient, education, religious belief, availability of caregiving support, psychiatric history, and participation in the patient’s ACP. Deceased patients’ demographics: age, sex, length of treatment, involvement of palliative care teams, overall evaluation of end-of-life care (via CES), and perceived quality of death (via GDI).
Spearman’s rank correlation coefficients were calculated to assess associations between the degree of ACP discussion and psychological outcomes. One-way analysis of variance (ANOVA) was conducted to compare psychological outcomes by discussion partner. All analyses were conducted using the statistical software HAD (version 16.302). 16
Ethical considerations
This study was approved by the Ethics Committee of Tohoku University Hospital (approval number: 2017-2-236-1), as well as by the ethics committees of all participating institutions.
Results
Participant characteristics
Questionnaires were sent to 1,006 bereaved family members, of which 639 were returned (response rate: 63.5%) (Table 1). After excluding incomplete responses, 544 valid questionnaires (33.6% male; mean age = 64.6 years) were analyzed (valid response rate: 54.1%).
Demographics of Patients and Caregivers
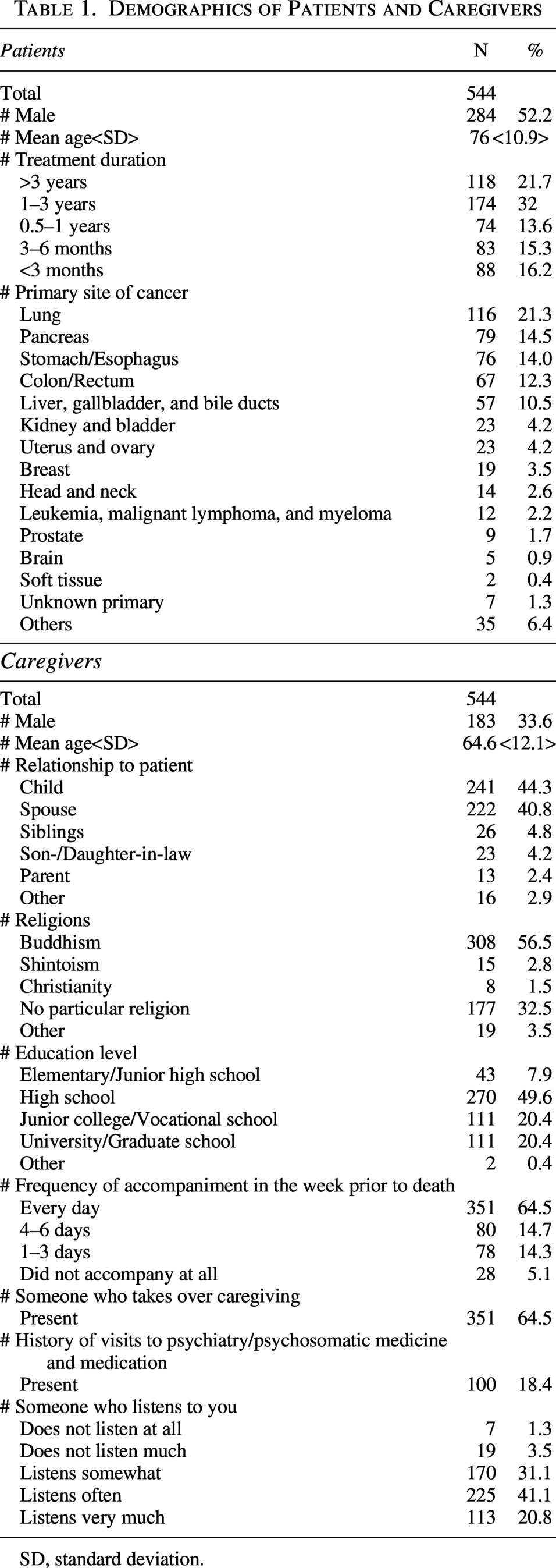
SD, standard deviation.
Of the participants, 275 (51.4%; 95% confidence interval [95% CI]: 47.2–55.7) reported having engaged in discussions with the deceased patient regarding their wishes for treatment or preferred end-of-life care.
Impact on bereaved individuals’ own ACP behavior
Among the 535 respondents who provided complete responses for this domain, 401 (75.0%; 95% CI: 71.1–78.4) reported having thought about their own ACP. Of these, 225 (42.1%; 95% CI: 37.9–46.3) had discussed their ACP with someone, and 42 (7.9%; 95% CI: 5.9–10.4) had documented their wishes.
Among the 396 participants who had thought about ACP and had no missing data, the most common pattern was having thought about ACP and discussed it with someone, but not having documented it (n = 189, 47.7%; 95% CI: 42.9–52.6) (Table 2). This was followed by those who had only thought about ACP without discussing or documenting it (n = 165, 41.7%; 95% CI: 36.9–46.6). A smaller group had both discussed and documented their ACP (n = 36, 9.1%; 95% CI: 6.6–12.3), while only six participants (1.5%; 95% CI: 0.7–3.3) reported documenting their ACP without any discussion.
Frequency of Discussion and Documentation Among Bereaved Family Members Who Had Considered Their Own Advance Care Planning
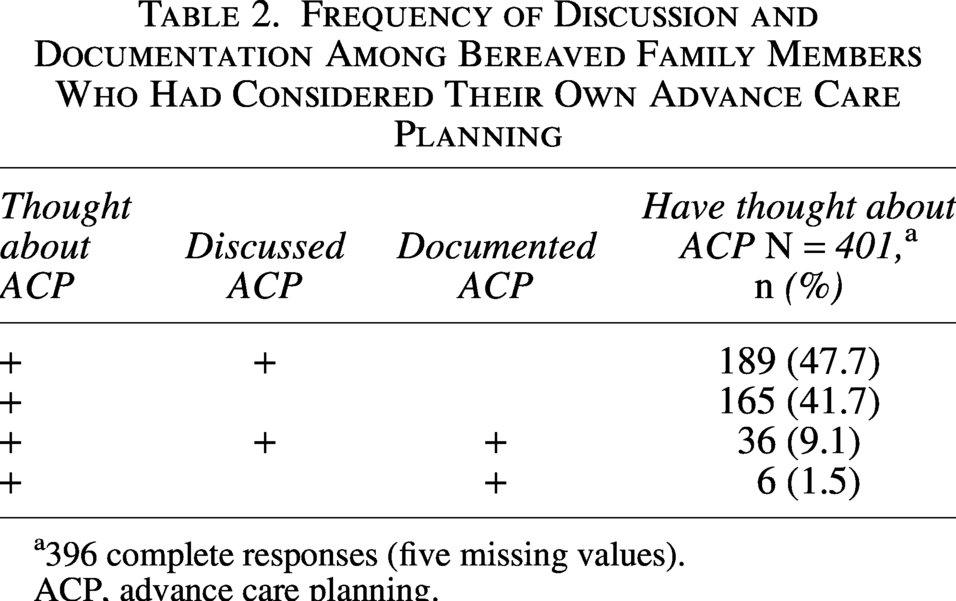
396 complete responses (five missing values).
ACP, advance care planning.
Among the 496 respondents who answered both questions about participation in the patient’s ACP and their own ACP behaviors, univariate analyses revealed that those who had discussed ACP with the patient were significantly more likely to have thought about their own (odds ratio [OR] = 5.07, 95% CI: 3.20–8.03, p < 0.01) and to have discussed it with someone else (OR = 2.46, 95% CI: 1.60–3.80, p < 0.01), although this was not significantly associated with documentation (OR = 1.61, 95% CI: 0.78–3.32). Those who had discussed ACP with others were more likely to have documented their wishes (OR = 2.01, 95% CI: 1.48–2.72, p < 0.01).
Multivariate logistic regression analyses identified two significant predictors of thinking about one’s own ACP: (1) having participated in the patient’s ACP (OR = 4.79, 95% CI: 2.83–8.09, p < 0.01) and (2) being a family member other than the patient’s sibling (OR = 0.26, 95% CI: 0.08–0.87, p < 0.05) (Table 3). Neither CES nor GDI scores showed significant associations with ACP-related behaviors; therefore, detailed results are not presented.
Predictors of Bereaved Family Members’ Consideration of Their Own Advance Care Planning: Univariate and Multivariate Analyses
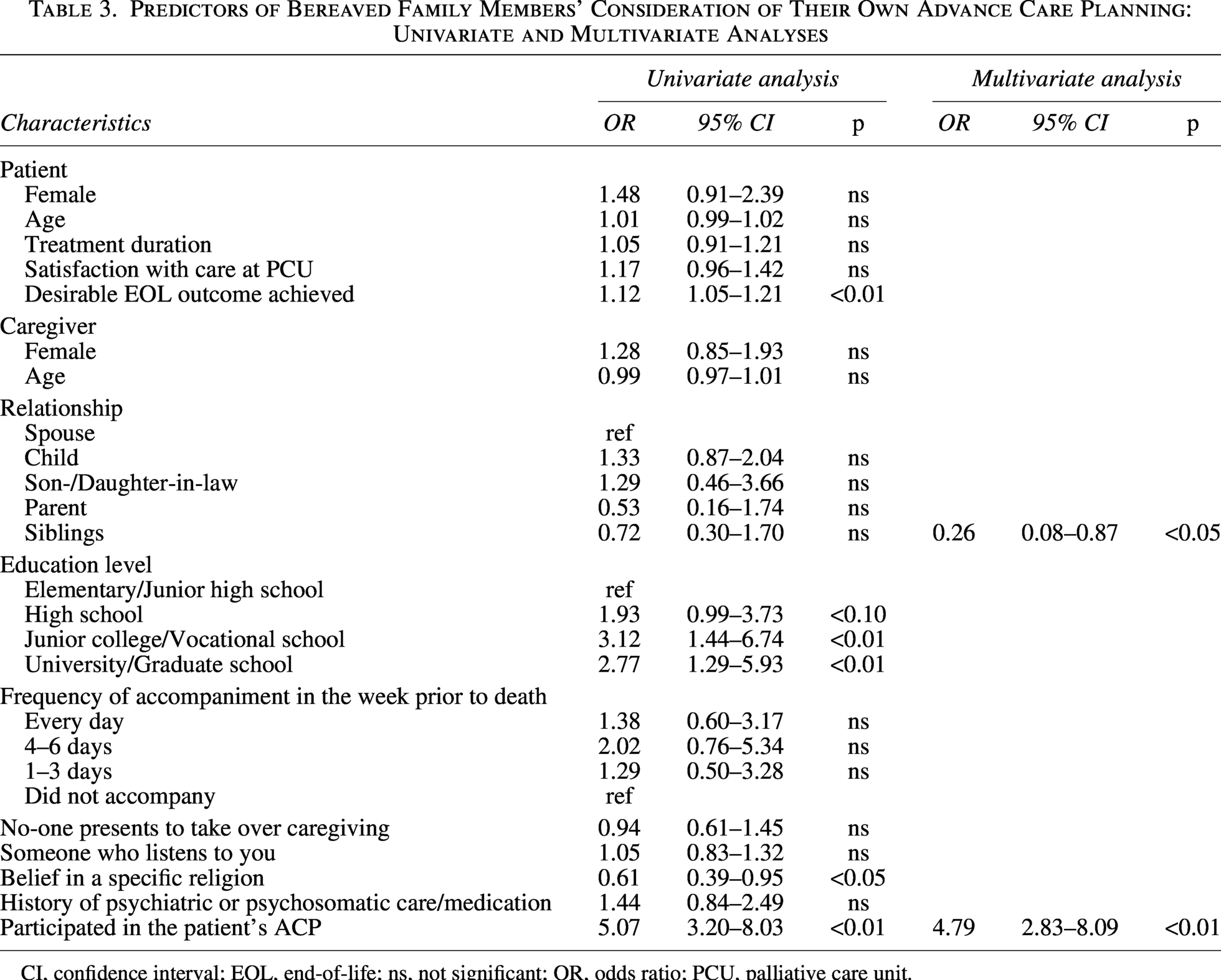
CI, confidence interval; EOL, end-of-life; ns, not significant; OR, odds ratio; PCU, palliative care unit.
ACP discussion partners
Among the 225 respondents who had discussed ACP with someone, the most common discussion partners were children (n = 146, 38.2% of 382 multiple-selection responses), followed by spouses (n = 98, 25.7%), siblings (n = 55, 14.4%), friends (n = 39, 10.2%), and parents (n = 14, 3.7%) (Table 4). Among the 211 complete responses, children were also most frequently identified as the most influential discussion partners (47.9%), followed by spouses (34.1%), siblings (9.5%), friends (3.3%), and parents (2.4%).
Distribution and Impact of Conversation Partners in Bereaved Family Members’ Own Advance Care Planning Discussions
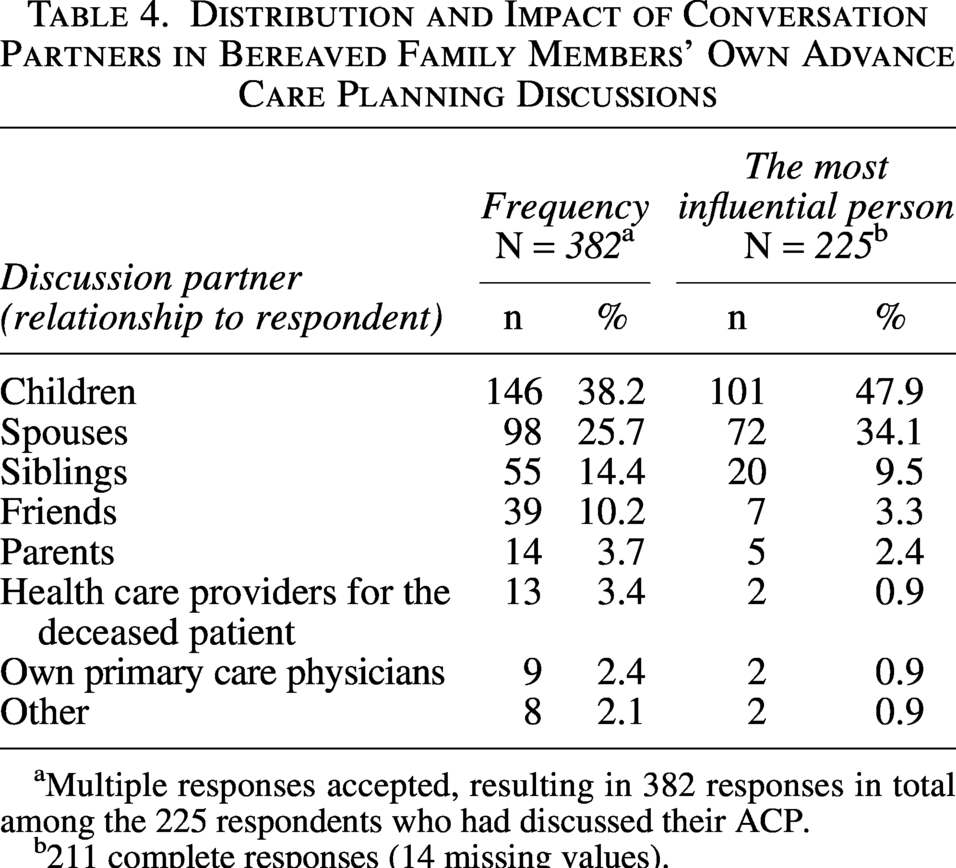
Multiple responses accepted, resulting in 382 responses in total among the 225 respondents who had discussed their ACP.
211 complete responses (14 missing values).
Health care providers, including participants’ own physicians (n = 9, 2.4%) and the deceased patient’s health care providers (n = 13, 3.4%), were less frequently selected as discussion partners and were perceived as less influential. On average, participants who had discussed ACP reported speaking with approximately 1.7 individuals.
Psychological impact of ACP discussions (n = 206)
Among participants who had discussed their own ACP with someone, a majority reported experiencing positive psychological effects. Specifically, 74.8% indicated that their trust in the discussion partner had increased, 79.1% reported that it became easier to communicate their thoughts and feelings, 86.9% experienced a stronger sense of being understood, and 62.1% reported reduced anxiety about the future. Figure 1 shows the impact of ACP discussions with the person considered most influential by bereaved family members across four assessed psychological outcomes.
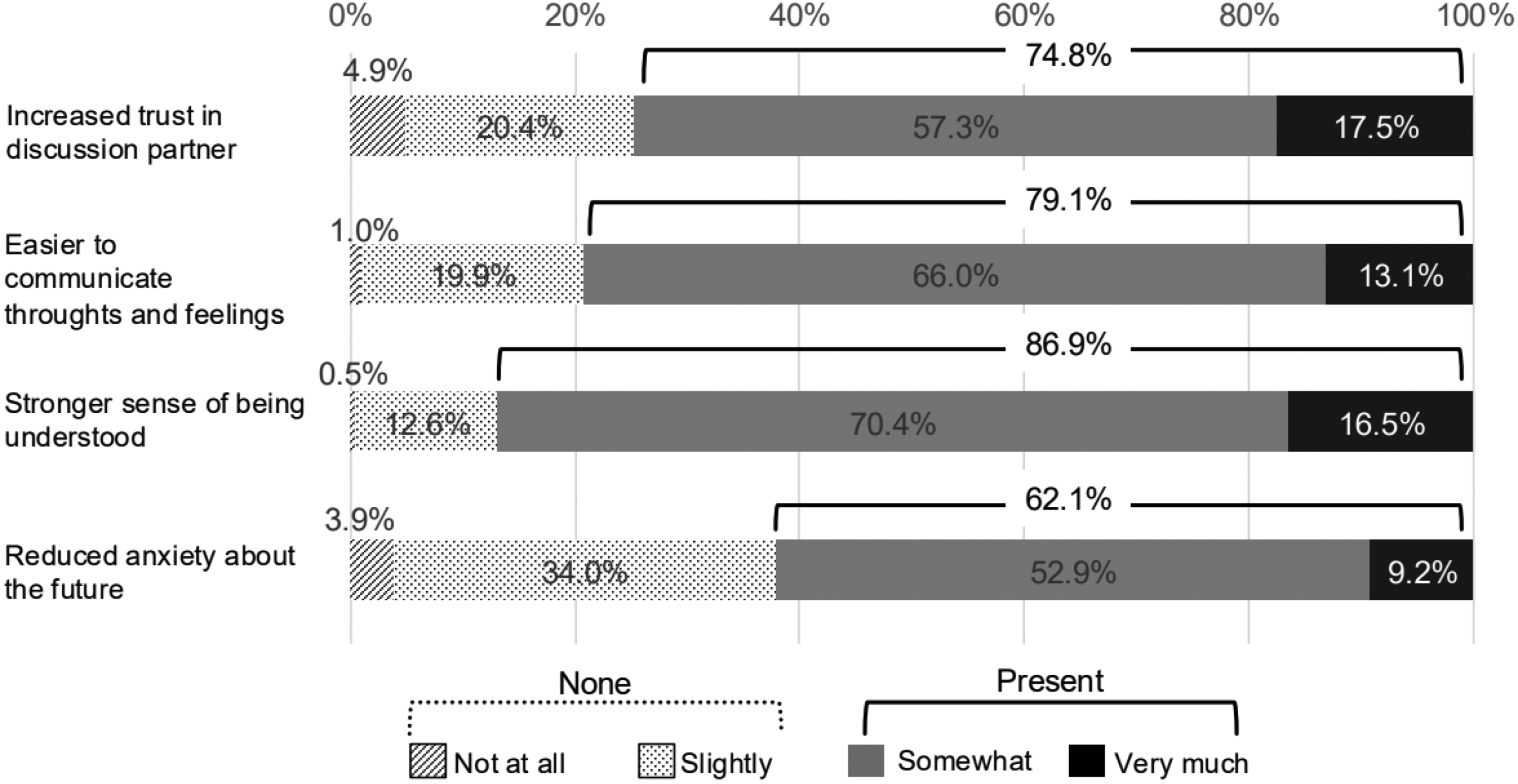
Impact of ACP discussions with the person considered most influential by bereaved family members. ACP, advance care planning.
Spearman’s rank correlation analysis was conducted to assess the relationship between the degree of ACP discussion and each of the four psychological outcomes. Significant positive correlations were observed for all outcomes: increased trust (ρ = 0.17, p < 0.01), ease of communication (ρ = 0.16, p < 0.01), a stronger sense of being understood (ρ = 0.21, p < 0.01), and reduced future-related anxiety (ρ = 0.22, p < 0.01).
Additionally, a one-way ANOVA was performed to compare these psychological outcomes based on the type of discussion partner, categorized as spouse, child, other relatives, and others (including friends and health care professionals). The analysis revealed no statistically significant differences across partner types for any of the psychological outcomes: trust [F(3, 187) = 2.37, p = 0.072, η2p = 0.037], ease of communication [F(3, 189) = 1.24, p = 0.29, η2p = 0.019], or sense of being understood [F(3, 193) = 0.703, p = 0.55, η2p = 0.011].
Discussion
This study identified four key findings regarding the experiences and implications of ACP among bereaved family members of cancer patients. First, bereaved individuals who had participated in the patient’s ACP were more likely to think about and discuss their own ACP. Second, those who had discussed their ACP with others were more likely to document their preferences. Third, among the various ACP discussion partners cited, health care professionals rarely featured and had limited influence on surrogate decision-making. Fourth, engaging in ACP discussions was associated with positive psychological outcomes, such as greater trust, ease of communication, a stronger sense of being understood, and reduced anxiety about the future, regardless of the identity of the discussion partner.
Multivariate analyses indicated that, aside from participation in the patient’s ACP, factors such as the gender or age of the patient and bereaved individual, length of illness, familial relationship, religious belief, or psychiatric history were not significantly associated with ACP engagement. The inclusion of CES and GDI scores as covariates indicates that the associations between ACP participation and bereaved individuals’ behaviors were independent of the perceived quality of care or death.
These findings are consistent with prior work by Fried et al.,6,7 which demonstrated that previous exposure to ACP—especially in the context of a loved one’s illness—can act as a behavioral trigger for personal ACP engagement. These results also correspond to recent studies emphasizing the central role of families in ACP, particularly in cultures where family-centered decision-making predominates.17,18 In Japan, where ACP is often practiced as an informal, family-centered process, participating in such discussions may normalize planning for the future and help family members view it as a natural part of communication around life and death.
Similarly, a nationwide study by Hamano et al. 8 reported that, while a substantial proportion of older patients in Japan had discussed ACP in primary care settings, documentation of those preferences remained infrequent, suggesting a persistent gap between verbal engagement and formal planning. Hamano et al. 9 also highlighted that insufficient involvement of health care professionals in ACP documentation may be a contributing factor to this gap. This aligns with our own finding that bereaved individuals rarely chose clinicians as ACP discussion partners. Taken together, these findings suggest that participation in a loved one’s ACP may serve as a potent experiential catalyst for reflection and dialogue, but formal documentation may require additional supportive mechanisms, such as proactive facilitation by clinicians or structured, system-level interventions.
Our study also confirms the stepwise relationship between thinking about ACP, discussing it, and ultimately documenting it—an observation that resonates with the ACP behavioral model proposed by Sudore et al. 8 This multistage view aligns with contemporary frameworks highlighted in recent scoping and narrative reviews,4,19 which emphasize evaluating ACP as a process encompassing both reflection and action, rather than focusing solely on medical outcomes.
Nonetheless, we identified a small subset of individuals who had documented their preferences without prior discussion. Although the effect size was small and of limited clinical relevance, this deviation from the conventional linear pathway suggests emerging forms of nondialogic, self-initiated planning. Such behavior, while seemingly inconsistent with ACP’s communication-centered philosophy, may reflect evolving social contexts in which digital technologies, pandemic-related restrictions, and reduced in-person interaction increasingly shape how individuals prepare for the end of life.
Furthermore, over 80% of ACP discussions in this study occurred with family members, particularly children and spouses, rather than with health care providers. This finding is consistent with those of Hamano et al. 9 and Musa et al., 20 both of whom reported that individuals tend to prioritize family and close social networks over clinicians when it comes to end-of-life decision-making conversations. These patterns highlight the need to recognize and support ACP not only as a clinical task but also as a relational and cultural process situated within everyday life.
Unlike previous studies that mainly focused on family members involved in ACP during the patient’s life, a distinctive contribution of our study is the demonstration that engaging in ACP discussions—particularly with someone close—can foster sustained psychological and relational benefits even after the patient’s death. Increased trust, a stronger sense of being understood, and reduced anxiety were reported by bereaved individuals, suggesting that ACP may help reinforce relational resilience and emotional preparedness beyond its medical or legal functions. These findings complement prior randomized and controlled evaluations of ACP interventions,4,5 which have consistently shown improvements in proximal outcomes but mixed results for more distal endpoints. Our cross-sectional results thus provide descriptive evidence for these distal and relational domains, particularly within a cultural context in which family dialogue and mutual understanding are central to end-of-life decision-making.
Extending this perspective, recent work has underscored the broader psychosocial value of ACP across diverse populations and contexts. For example, Wiener et al. 13 emphasized the psychosocial value of ACP in their study of adolescents and young adults, who engaged in a nonclinical, expressive ACP document titled “How I Wish to Be Remembered.” In their findings, the majority of participants reported that the document was emotionally supportive, with 95% finding it helpful and none experiencing it as stressful. This suggests that ACP conversations—particularly those that allow for personal expression, emotional connection, and legacy building—can be empowering across age groups and care contexts. Such evidence supports the notion that ACP is not merely an act of planning for death but also an opportunity to reflect on life, affirm relationships, and communicate identity and values. Future research should explore whether integrating such expressive elements into ACP for adults and bereaved caregivers could similarly enhance emotional well-being, increase engagement, and extend the relational benefits of ACP to broader populations.
Limitations
Several limitations should be acknowledged. First, this study relied on retrospective self-report data from bereaved family members, introducing the possibility of recall bias. Second, participants were limited to those whose loved ones received inpatient palliative care, potentially restricting generalizability to community- or home-based settings. Third, analyses of ACP behaviors (particularly documentation and discussion) were restricted to respondents who had already thought about their own ACP, preventing comparison with individuals who had not engaged in ACP at all.
Finally, given the study’s cross-sectional design, the observed associations should be interpreted as correlational rather than causal. Future longitudinal or interventional studies are needed to clarify these temporal and causal relationships and to examine whether exposure to ACP discussions truly facilitates later engagement.
Clinical and policy implications
These findings suggest a potential association between family involvement in ACP and subsequent engagement in ACP among bereaved individuals. While the present results should be interpreted within the context of an observational design, they raise the possibility that family-centered experiences of ACP may be relevant when considering approaches to promote ACP engagement.
Clinicians may wish to remain attentive to the relational dimensions of ACP, particularly in cultural contexts in which decision-making is embedded within family communication. From a policy perspective, these findings may inform ongoing discussions about community-based or family-inclusive approaches to ACP promotion and normalization as part of life planning.
Conclusion
This study demonstrates that participation in a cancer patient’s ACP can influence bereaved individuals’ own engagement with ACP, including thinking about, discussing, and, to a lesser extent, documenting preferences. Beyond these behavioral effects, ACP discussions were associated with positive psychological outcomes such as increased trust, emotional understanding, and reduced anxiety. These findings underscore the importance of ACP not only as preparation for dying but also as a process fostering connection, reflection, and shared meaning in life. Promoting reflection on prior caregiving experiences may offer one potential avenue for supporting future ACP engagement in clinical and public health contexts.
Authors’ Contributions
Conceptualization and study design: Y.U.-M., M.S., S.T., and T.M. Data collection: K.M. and M.M. Data analysis and interpretation: Y.U.-M., M.S., and T.M. Drafting of article: Y.U.-M., M.S., and M.M. Critical revision for important intellectual content: Y.K. and Y.S. And final approval and accountability: All authors approved the final version and agreed to be accountable for all aspects of the work.
Footnotes
Acknowledgments
The authors would like to thank Mr. Oliver Stanyon for editing this paper.
Author Disclosure Statement
All authors declare that they have no financial or personal interests that could have influenced the work reported in this article.
Funding Information
This study was conducted as part of the Japan Hospice and Palliative Evaluation Study 4 (J-HOPE4) and was funded by the Japanese Foundation for Hospice and Palliative Care Research.