
Abstract
Background:
In Israel, several policies have supported the growth of home-based hospice through a unique public–private care delivery and financing system. Yet, little is known about trends in home hospice use in Israel.
Objective:
To describe 10-year trends in diagnosis, length of stay (LOS), and discharge patterns among home hospice patients in Israel.
Design:
We conducted a retrospective cohort study of all patients admitted to Sabar Health’s home hospice program between 2014 and 2023. Demographic and clinical data were analyzed by primary diagnosis: Cancer, dementia, end-organ failure, frailty, and neurodegenerative disease. Trends in enrollment, LOS, and live discharge rates were assessed over time.
Results:
Among 25,673 patients, the proportion with cancer annually declined from 88.6% in 2014 to 57.8% in 2023, while admissions for dementia rose from 0% in 2014 to 19.6% in 2023. Median LOS increased from 20 to 35 days, with the longest durations observed among patients with dementia and neurodegenerative disease. Live discharge rates also rose, particularly in the dementia group from 12.2% to 20% over the observed period, with a growing share occurring after ≥180 days.
Conclusions:
Home hospice care in Israel has evolved significantly over the past decade, with increasing enrollment of patients with prolonged and uncertain illness trajectories. These trends emphasize the need for more adaptable eligibility frameworks, improved prognostic tools, and expanded caregiver support to meet the needs of a diversifying hospice population.
Key Message
Over a decade, home hospice use in Israel has shifted beyond cancer toward dementia and other chronic conditions, with longer stays and higher live discharge rates. Hospice models must adapt eligibility, prognostication, and caregiver support to meet increasingly prolonged and uncertain illness trajectories.
Introduction
Hospice provides comfort-focused care for individuals with terminal illnesses and a life expectancy of six months or less, prioritizing symptom relief, psychosocial support, and quality of life.1–3 In many countries, hospice care is primarily delivered at home, enabling patients to remain in familiar environments and retain a sense of autonomy during the final phase of life.4,5 Historically, hospice services in most developed nations were oriented around the needs of cancer patients, whose disease trajectories were relatively predictable and aligned well with time-limited hospice benefit structures.6,7 Late referrals were common, often occurring only in the final weeks of life, largely driven by rapid deterioration in the performance status of cancer patients. 8
Over time, however, the hospice model has evolved to encompass a broader range of terminal conditions, including advanced cardiac disease, chronic obstructive pulmonary disease, and neurodegenerative illnesses such as amyotrophic lateral sclerosis (ALS) and dementia. 9 This shift reflects a growing recognition of the considerable symptom burden, prolonged functional decline, and significant caregiver strain associated with incurable noncancer conditions, factors that similarly benefit from an interdisciplinary palliative approach. 10 Among these diagnoses, dementia has emerged as a leading indication for hospice referral in aging populations, especially in high-income countries. 11 In the United States, for example, dementia has surpassed cancer as the most common primary diagnosis among hospice enrollees. 12 This expansion in hospice care eligibility has required health systems to rethink traditional hospice models, both in terms of prognostication and care delivery, and to shift the underlying professional approach—from focusing on cure and prolonging life toward prioritizing comfort, quality of life, and holistic support for patients and their families.
In Israel, health care is publicly funded under a national health insurance framework established by the National Health Insurance Law of 1995. 13 Health care is delivered through four Health Maintenance Organizations (HMOs), which operate across both community clinics and hospital systems. 14 Despite this universal coverage, access to hospice services remained limited for many years. Prior to 2009, hospice care in Israel was primarily restricted to adult cancer patients and was inconsistently available, often serving only a few dozen individuals at any given time. 15 This landscape shifted significantly in 2009, when the Israeli Ministry of Health issued a national directive aimed at expanding and formalizing hospice care services. The directive established an interprofessional model of palliative care, mandating that any individual with a terminal diagnosis and a prognosis of six months or less would be eligible for continuous support from a multidisciplinary team. 16 These teams, typically composed of physicians, nurses, and social workers, could deliver care in hospitals, nursing homes, or the patient’s own home, depending on preference and clinical need. The service is required to be accessible to all populations, regardless of place of living and with no co-payment. By embedding hospice within the broader publicly funded system, the novel directive aimed to ensure equitable access and consistent standards of care across settings. 15
Interestingly, the 2009 directive initially excluded patients with dementia from hospice eligibility, reflecting uncertainty at the time about the appropriateness of hospice for individuals with protracted and unpredictable disease courses.17,18 This exclusion was later challenged by growing clinical evidence demonstrating that individuals with advanced dementia experience significant symptoms, including pain, agitation, and feeding difficulties, and that their caregivers report high levels of emotional, physical, and financial stress. 19 A study by Sternberg and colleagues at Maccabi Health Services, the second largest Israeli HMO, showed that home-based palliative care for patients with dementia led to measurable benefits, including improved symptom control, reduced caregiver burden, and fewer hospitalizations near the end of life. 20
In response to this accumulating evidence, the Israeli HMOs started referring advanced dementia patients to hospice treatment in 2015, expanding access and signaling the legitimacy of dementia as a terminal condition warranting palliative care. Following this change, hospice services in Israel experienced significant growth in both capacity and utilization. While exact national data remain unavailable, current estimates suggest that several thousand patients receive home hospice care at any given time, representing a substantial increase over the previous decade. 21
Despite national policy reforms and rapid expansion of home hospice services, there are no published longitudinal data describing how the Israeli hospice population has changed over time in terms of diagnosis mix, length of stay (LOS), and discharge patterns. Understanding these trends is critical for informing eligibility criteria, workforce planning, and payment structures in a publicly funded system facing increasing enrollment of patients with prolonged and uncertain illness trajectories. The objective of this study was to characterize the home hospice population in a large home-based health care system from 2014 to 2023.
Methods
Study design and setting
This retrospective cohort study examined patients enrolled in the Sabar Health home hospice program between January 1, 2014, and December 31, 2023. Sabar Health is a national provider of home-based hospice services in Israel, operating under agreements with all four national HMOs. The program serves individuals with serious illnesses who are eligible for hospice care and prefer to receive services at home. At any given time, Sabar Health’s home hospice unit cares for approximately 1000 patients nationwide, making it a substantial indicator of national hospice use trends and practice patterns. 22
Study population
The study population included all patients admitted to the home hospice program during the study period. Patients were eligible for inclusion if they had complete administrative and clinical records and a qualifying primary diagnosis. A total of 635 patients were excluded due to unclear diagnosis coding.
Data sources and variables
Administrative and clinical data were extracted from Sabar Health’s centralized electronic medical record system. Variables collected included age (in years), sex, primary diagnosis, LOS in hospice, and discharge disposition. Primary hospice diagnoses were categorized into five mutually exclusive groups: (1) Cancer; (2) dementia, including Alzheimer’s disease, vascular dementia, Lewy body dementia, and Parkinson’s disease with dementia; (3) neurodegenerative diseases, including ALS, stroke, epilepsy, multiple sclerosis, familial dysautonomia, progressive supranuclear palsy, Creutzfeldt–Jakob disease, and ataxia; (4) end-organ failure, including renal, hepatic, cardiac, and pulmonary conditions; and (5) frailty, previously labeled “general deterioration.” This approach increased the representation of noncancer conditions, enabling more robust comparison of care trajectories and service utilization patterns across diagnostic groups.
LOS was calculated in days from the date of hospice enrollment to the date of death or live discharge. LOS was further categorized into three groups: Short (0–7 days), intermediate (8–180 days), and long (>180 days). Discharge disposition was classified as death at home, death in the hospital, or live discharge. Live discharges were defined as those resulting from clinical stabilization, family request, or organizational decisions that led to discharge back to the HMO. Long-stay live discharges were defined as those occurring after more than 180 days in the program.
Longitudinal analyses focused on cancer and dementia, as these diagnoses together accounted for the majority of hospice admissions and the greatest absolute growth over the study period.
Data cleaning and exclusion criteria
All patients admitted to home hospice in the study period were included in the analysis. Patients who were still enrolled at the end of 2023 were excluded because their LOS and discharge outcomes were right-censored and not yet observable.
Statistical analysis
Descriptive analyses were conducted using Microsoft Excel and IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY). Patient data were sorted by date of admission and analyzed by age, sex, diagnosis, LOS, and discharge disposition. We compared LOS and discharge trends by diagnostic group. We assessed trends in diagnostic group proportions, live discharge rates, and long stays by year. Temporal trends in diagnosis mix and utilization patterns were formally assessed using nonparametric and regression-based tests for trends. Changes in the proportion of patients with specific diagnoses, long hospice stays (≥180 days), and live discharges over time were evaluated using logistic regression with year modeled as a continuous variable. Trends in LOS were assessed using nonparametric tests for trend due to right-skewed distributions. Statistical significance was defined as a two-sided p < 0.05.
Ethical approval
This study was approved by the Duke University Health System Institutional Review Board and granted a waiver of informed consent due to its retrospective nature and use of deidentified patient data (Pro00116539).
Results
A total of 25,673 patients were included in the analysis (mean age of 73.2 years, 53% female). The majority had a cancer diagnosis (n = 18,772, 73.1%), followed by dementia (n = 2881, 11.2%), end organ failure (n = 2277, 8.9%), frailty (n = 997, 3.9%), and neurodegenerative disease (n = 747, 2.9%).
Age varied by diagnosis and was highest among patients with dementia (mean 87.7 years) and frailty (89.7 years). Median LOS ranged from 13 days among patients with frailty to 38 days among those with neurodegenerative disease. The proportion of patients discharged alive ranged from 14.0% in the frailty group to 23.2% among those with end organ failure (Table 1). Ethnic composition differed modestly across diagnostic groups, as presented in Table 1; these differences were not a primary focus of the current analysis.
Demographic and Clinical Characteristics of Home Hospice Patients by Diagnosis Group (N = 25,673)
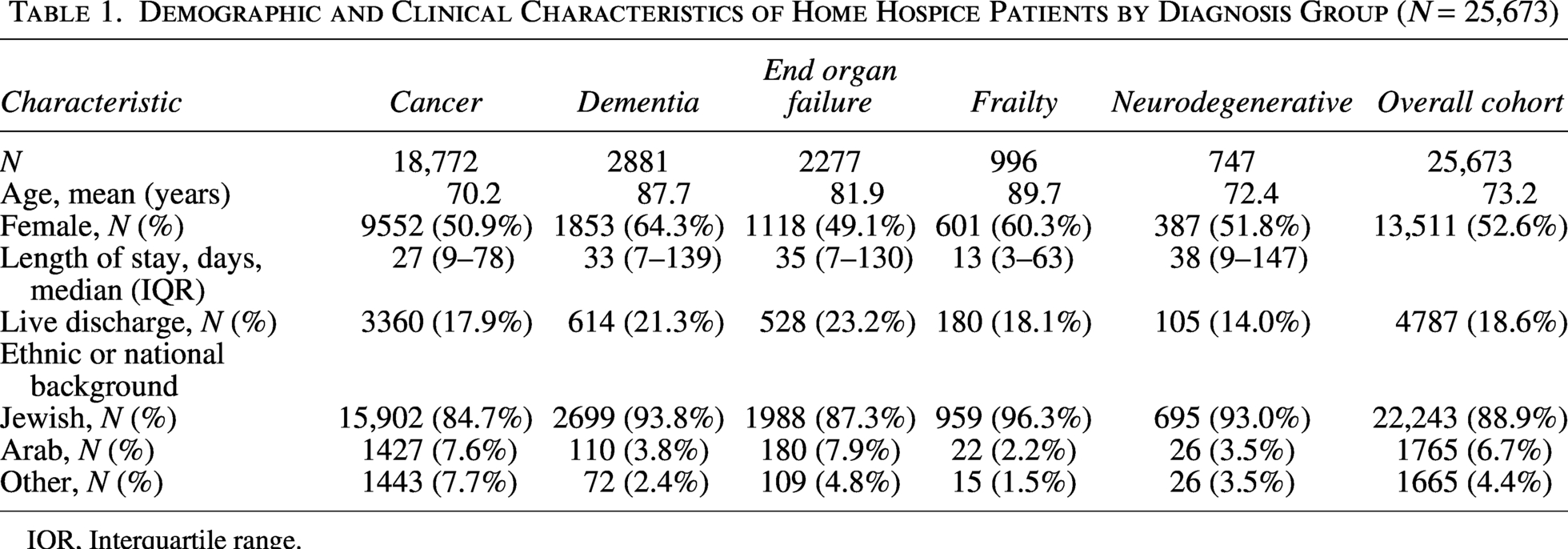
IQR, Interquartile range.
The number of hospice patients increased substantially over the study period, particularly among those with cancer and dementia (Fig. 1). The proportion of hospice patients admitted with cancer declined from 88.6% in 2014 to 57.8% in 2023, while admissions for dementia rose from 0% to 19.6% accordingly. Formal trend testing demonstrated a statistically significant increase in the proportion of patients admitted with dementia over time, alongside a significant decline in cancer admissions (p for trend < 0.001 for both). These changes were consistent across the study period and not driven by isolated years.
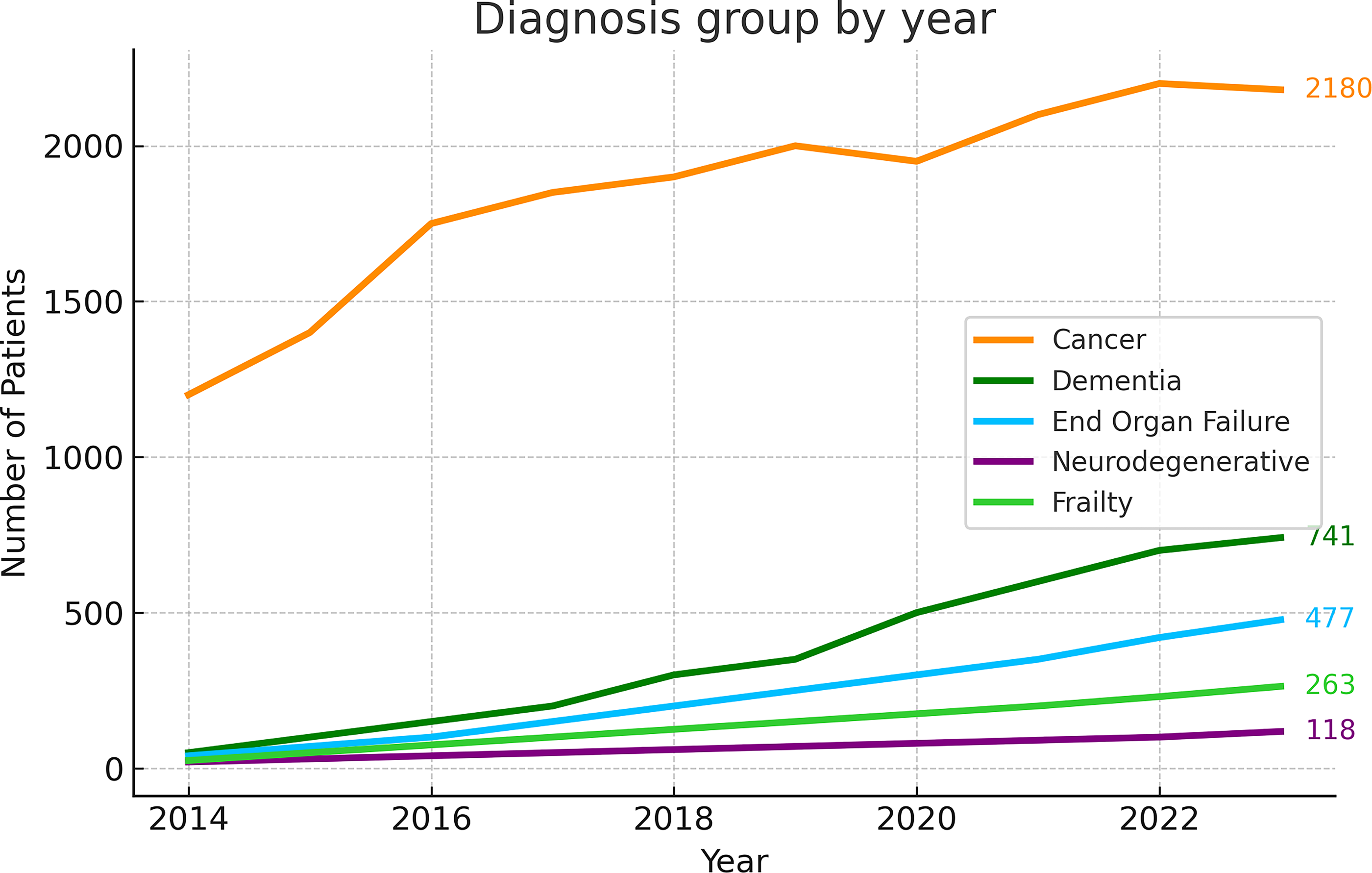
Patients admitted to home hospice by year and diagnosis group.
Median LOS also increased, especially for these two groups. In 2015, the median LOS was 20 days for both cancer and dementia; by 2023, it had risen to 33 days and 52 days, respectively. The interquartile range for LOS was consistently wider in the dementia group compared to cancer (Fig. 2). Across all diagnoses, the median LOS rose from 20 days in 2014 to 35 days in 2022. Nonparametric trend testing demonstrated a significant increase in LOS over time among both cancer and dementia patients (p for trend < 0.001 for both groups). The magnitude of increase was greater among patients with dementia, consistent with the widening interquartile range observed in later years.
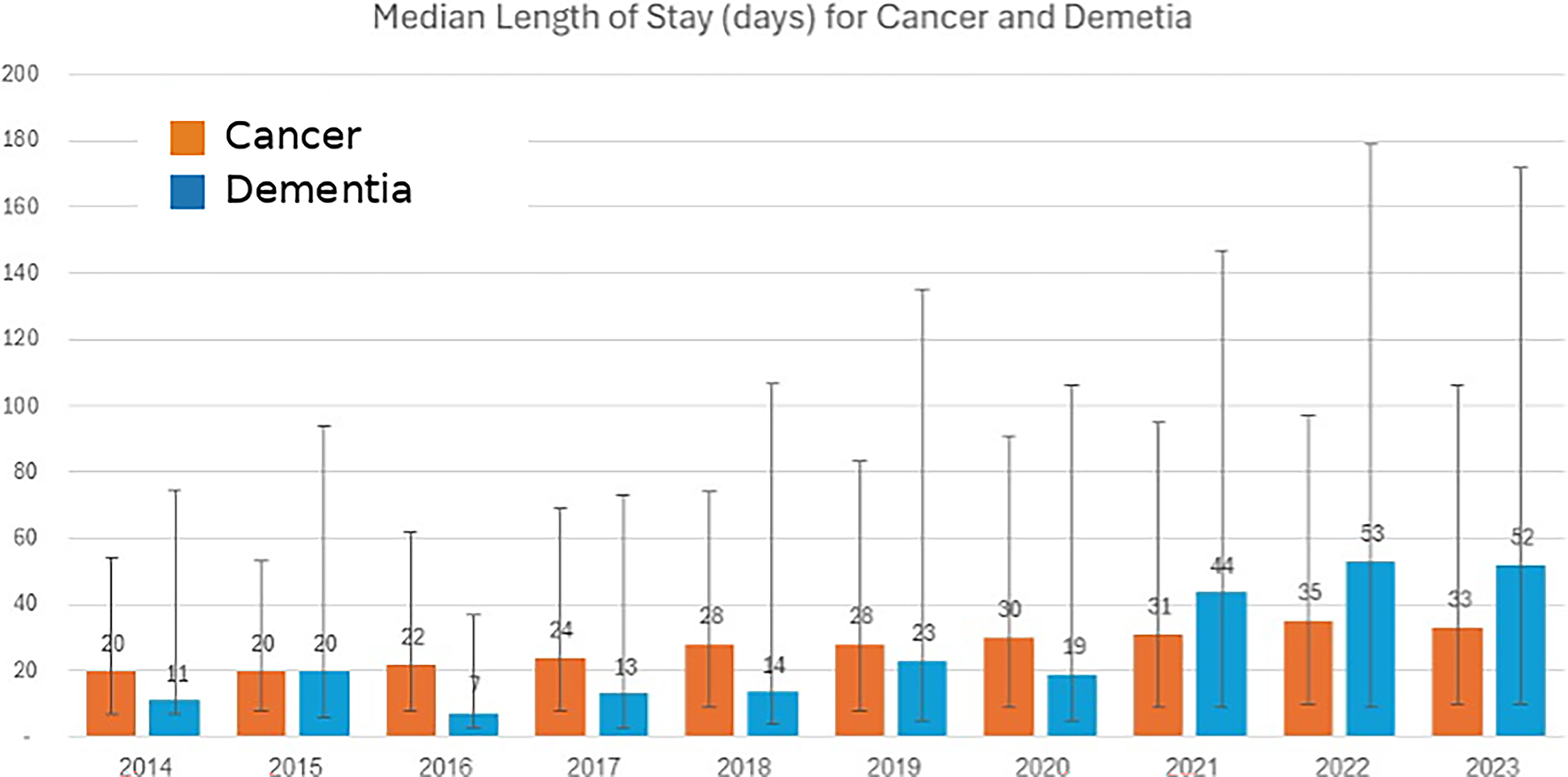
Median length of stay (days) by diagnosis group and year (median, interquartile range).
During the same period, live discharge rates increased. Among cancer patients, the rate rose from 14.9% in 2015 to 19.2% in 2023. Among dementia patients, it increased from 12.2% to 20%, though annual rates fluctuate, likely due to smaller sample sizes. Trend testing demonstrated a significant increase in live discharge rates over time among patients with dementia (p for trend < 0.01). Annual fluctuations were observed, likely reflecting smaller sample sizes in earlier years.
The proportion of patients with long hospice stays (≥180 days) increased significantly over time overall (p for trend < 0.001), driven primarily by patients with dementia and neurodegenerative disease. In contrast, no consistent temporal trend was observed among patients admitted with frailty, whose rates of long stays fluctuated across years (Table 2).
Proportion of Patients with Long Hospice Stays (>180 Days) by Year and Diagnosis Group
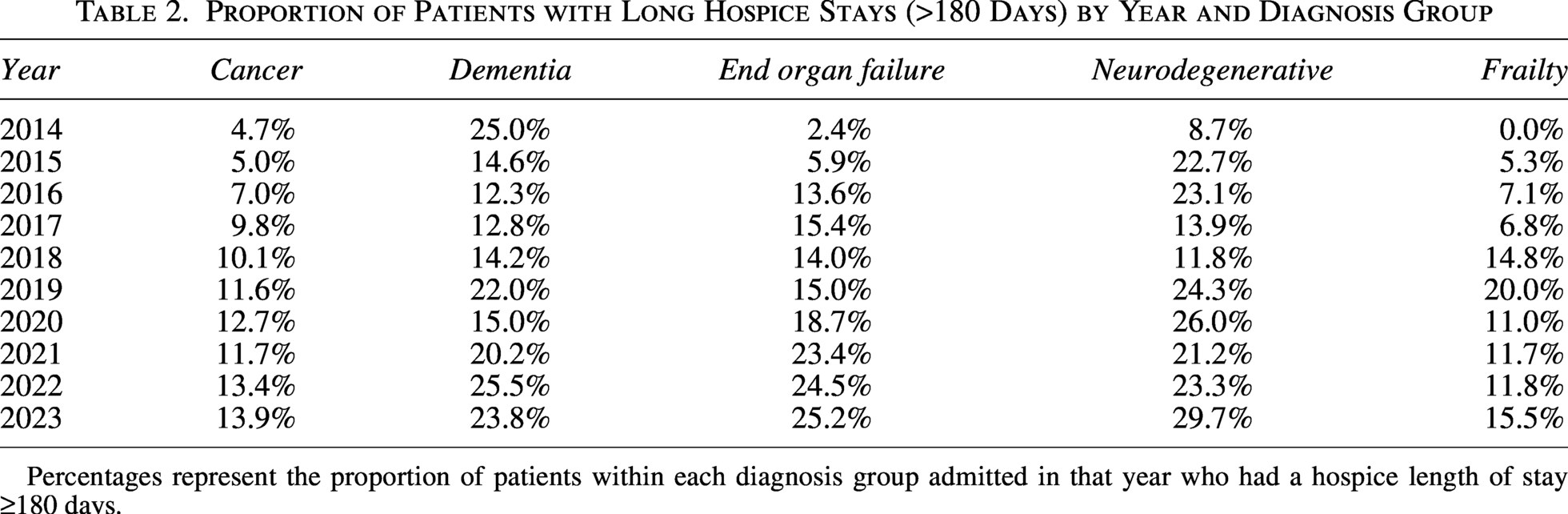
Percentages represent the proportion of patients within each diagnosis group admitted in that year who had a hospice length of stay ≥180 days.
Discussion
This study provides a 10-year overview of evolving home hospice utilization patterns in Israel, reflecting major national policy reforms alongside changes in clinical practice. Since the 2009 policy expansion that broadened eligibility for hospice to all terminal diagnoses, and particularly after the inclusion of patients with advanced dementia in 2015, hospice utilization increased steadily as well as LOS and diagnostic diversification among home hospice patients. Formal trend testing confirmed that these changes reflect statistically significant temporal trends rather than visual patterns alone.
This transformation was enabled, in part, by Israel’s unique model of hospice care delivery. Unlike many countries with universal health coverage, such as France, England, and Scandinavia, where hospice services are typically delivered by public or nonprofit providers embedded within state-run frameworks, the Israeli HMOs contract with a private provider, in this case, Sabar Health, to deliver this core public service under the National Insurance financing scheme. 22 This partnership allowed for rapid expansion and flexibility, serving as a catalyst to help the system scale up quickly following policy reforms and pilot new care models in response to changing patient needs. The agility of this arrangement can be especially valuable when the public sector lacks the infrastructure to meet rising demand. However, integrating private providers into publicly funded systems also raises concerns around equity, regulation, and alignment with public health goals.
Although cancer remains the most common diagnosis in this cohort, its share has declined from 88.6% in 2014 to just 57.8% in 2023. Concurrently, patients with dementia, end-stage organ failure, neurodegenerative diseases, and geriatric frailty have constituted an increasing proportion of admissions, with dementia growing from 0% to 19.6% over the same period of time.
This trajectory is not unique to Israel. Similar patterns have been observed in countries with more mature hospice systems. In the United States, where hospice systems are more mature, dementia has become the most common primary hospice diagnosis, while cancer accounts for a smaller proportion of admissions. 12 Other published data suggest that a dementia diagnosis is found in over 50% of hospice enrollees. 23 This shift reflects an expanded understanding of palliative care as relevant across a range of progressive, life-limiting conditions, not just oncologic disease, and a recognition of the symptom burden and caregiving needs that accompany prolonged declines in function. The persistently higher proportion of cancer patients in Israeli hospice likely reflects the relative youth of Israel’s palliative care system and the more recent expansion of eligibility beyond oncology. Recent international literature further supports these observations, with population-based studies demonstrating increasing use of palliative and hospice care among patients with noncancer diagnoses, including dementia, across diverse health systems. Contemporary reviews and policy analyses similarly emphasize the growing prominence of chronic illness and prolonged care trajectories in end-of-life care, reinforcing the relevance of these trends beyond the Israeli context.24,25
Nevertheless, as the diagnostic mix of hospice patients changes, new clinical and operational challenges emerge. Prognostication, for instance, becomes more complex. While cancer trajectories are often characterized by more rapid functional decline, prognostication has become increasingly complex even in oncology due to advances in disease-modifying therapies. In contrast, conditions like dementia, frailty, or end-stage organ failure are marked by longer, more variable courses, punctuated by exacerbations that may or may not signal imminent death. Several studies have demonstrated the difficulty in applying a six-month prognosis framework to noncancer diagnoses, especially in patients with cognitive impairment.19,26 The result is that patients with these conditions often enter hospice too late or are subject to premature disenrollment when their course does not align with expected trajectories.
Our findings reflect this complexity. Median LOS increased from 20 days in 2014 to 35 days in 2022 over the study period, suggesting earlier referrals and better integration of palliative care into chronic illness management. However, this aggregate measure masks important variation by diagnosis. Patients with dementia had disproportionately longer stays, with a substantial subset (25.5% in 2022) remaining in hospice beyond 180 days. This mirrors international literature showing that dementia is associated with longer hospice durations and a lower likelihood of dying within six months of enrollment. 27 In contrast, no consistent temporal trend was observed among patients admitted with frailty, whose rates of long stays fluctuated across years. While these longer stays may benefit patients and families, they raise concerns for policymakers and funders about prognostic accuracy, appropriate resource use, and potential overextension of services.
The rise in live discharges among dementia patients in our cohort, due either to clinical stabilization or administrative disqualification, defined as termination of hospice enrollment by HMOs when patients no longer meet reimbursement eligibility criteria, is another phenomenon that aligns with international experience. 28 In the United States, the issue of “live discharges” has been widely discussed as a marker of prognostic uncertainty and system-level tension between eligibility criteria and disease reality. This is particularly salient in publicly funded systems such as Israel’s, where an increase in demand without proportional expansion of resources can lead to stricter gatekeeping practices. Disqualification of patients who exceed the presumed six-month prognosis threshold may reflect an attempt to preserve access for others, but it can also undermine continuity of care and erode trust among families and clinicians.
Recent trends highlight growing tension between traditional hospice delivery frameworks and the realities of caring for patients with prolonged and uncertain illness trajectories. There is a growing international consensus that eligibility criteria based solely on diagnosis and time-based prognostication are inadequate. Alternative models have been proposed, including functional and symptom-based eligibility criteria, tiered benefit structures, and risk-based payment models that account for variability in care needs over time. 29 Israel’s experience supports the urgency of these reforms. As more patients with dementia, frailty, and multimorbidity enter hospice care, systems must evolve to support care delivery that is longer in duration, more uncertain in trajectory, and heavily reliant on caregiver involvement. These findings should be interpreted in the context of Israel’s broader home care system, which provides ongoing support for patients with long-term illness trajectories outside of hospice eligibility.
Beyond eligibility and access, these shifts demand significant adaptation in care delivery models to ensure sustainability. Caring for patients with longer and less predictable trajectories requires different tools, workflows, and team configurations than those built around terminal cancer. Interdisciplinary teams must be trained to manage fluctuating functional status, complex comorbidity, and behavioral symptoms of dementia. Prognostic tools that incorporate functional status and symptom burden may help guide decision-making. Support for caregivers, often providing round-the-clock care for months or even years, becomes even more critical. These elements are already central to good hospice care, but the growing complexity of patients’ needs demands renewed investment and refinement.
In the United States, where most hospices are for-profit, similar public–private arrangements have come under scrutiny. 30 Concerns have been raised about enrolling patients with uncertain eligibility and maintaining disproportionately long lengths of stay, practices that may inflate reimbursement without clear clinical benefit. As patient populations grow more complex, systems must carefully balance innovation with strong oversight to ensure quality and fairness.
Our study has several limitations. First, it is based on data from a single provider, albeit the largest home hospice provider in Israel, and may not be fully representative of national patterns. Second, we lacked data on functional status, symptom burden, and caregiver strain. Those are key variables that would enrich understanding of hospice appropriateness and experience. Third, our analysis is descriptive and cannot establish causal relationships between policy changes and observed trends. Lastly, hospice enrollment may not fully capture clinical evolution over time.
Despite these limitations, this study offers important insights into the transformation of hospice care in Israel and its alignment with global trends. The diversification of the hospice population, increase in noncancer diagnoses, and emergence of geriatric syndromes as referral indications all suggest that the next phase of hospice development must embrace greater complexity, flexibility, and person-centeredness.
Authors’ Contributions
I.M.: Conception, data analysis, writing the article, editing the article, and preparing the article for publication. B.H.: Conception, data analysis, and writing the article. G.Y. and G.K.: Conception and editing the article. O.D., S.G.-R., and L.J.H.: Editing the article and preparing the article for publication. R.S.: Conception, editing the article, and preparing the article for publication.
Footnotes
Author Disclosure Statement
No competing financial interest exist.
Funding Information
No funding was received for this article.