
Abstract
Objective:
To compare end-of-life (EOL) care quality indicators for patients with gynecologic malignancies whose primary oncologist spoke their preferred language (language-concordant care) versus those who did not (language-discordant care).
Methods:
We conducted a retrospective chart review of patients with gynecologic malignancies who died between March 1, 2020, and May 30, 2024. The primary outcome was performance on National Quality Forum (NQF) quality indicators, a composite of six measures of aggressive EOL care. We used multivariable logistic regression to examine associations between language-discordant care and aggressive EOL care, adjusting for age, insurance status, and cancer stage at diagnosis.
Results:
Briefly, 83 patients met inclusion criteria; 60 (72.3%) received care from a language-concordant oncologist and 23 (27.7%) from a language-discordant oncologist. Discordant patients were more likely to identify as Hispanic or Asian and to have Medicaid insurance. Aggressive EOL care, defined as an NQF score ≥1, occurred in 87.0% of discordant patients compared with 60.0% of concordant patients (p = 0.0174). After adjusting for age, insurance, and cancer stage, language-discordant care was associated with more than six-fold higher odds of aggressive EOL care (adjusted odds ratios: 6.05, 95% confidence intervals: 1.38–26.53).
Conclusion:
Language discordance between patients and oncologists was associated with greater likelihood of aggressive EOL care in gynecologic oncology. Addressing language barriers is essential to improving equity and aligning care with patients’ goals at the end of life.
Key Message
Language discordance between gynecologic oncology patients and their oncologists is significantly associated with more aggressive end-of-life care. After adjusting for age, insurance, and cancer stage, language-discordant patients were over six times more likely to receive aggressive EOL care, highlighting a meaningful disparity that warrants targeted interventions and future multi-institutional study.
Introduction
Compared to their English-fluent counterparts, patients with limited English proficiency are less likely to know and understand their cancer diagnosis and more likely to overestimate the probability of a cure.1,2 This disparity stems partly from communication barriers across language preferences. Studies examining interpreter use in cancer care demonstrate that these interactions involve fewer total words, more direct advising, less time spent on information sharing, and less attention to psychosocial issues that may impact end-of-life (EOL) decisions.3,4 Similarly, in the critical care setting, compliance with national standards for providing language services remains poor, resulting in inconsistent interpreter use and limited availability of translated materials. 5 In intensive care unit (ICU) family meetings, interpreted encounters are shorter, convey less information, and include fewer supportive statements from clinicians, reducing opportunities for shared understanding and emotional support. 6
Within gynecologic oncology, EOL conversations between patients and their primary oncologists have been shown to decrease the likelihood of chemotherapy and/or ICU admission within 30 days of death, decrease the length of hospital admissions, and increase the utilization of palliative care.7,8 Lopez-Acevedo et al. demonstrated that EOL conversations occurring at least 30 days before death improve performance on National Quality Forum (NQF) quality indicators, 9 a validated set of six metrics identifying overly aggressive EOL care. 10 Poor NQF performance has been correlated with higher health care costs,9,11 and lower quality of life for patients, caregivers, and families.12,13
This study explored the impact of patient-provider language concordance on the quality of EOL care. Care was defined as language-concordant when the patient’s documented preferred language was spoken fluently by their primary oncologist. We compared NQF performance scores between language-concordant and language-discordant groups among patients with gynecologic malignancies who had been cared for at our institution and who had died. We hypothesized that having language concordance between patients and their oncology providers would be associated with improved NQF performance, reflecting more patient-centered, goal-aligned care.
Methods
We conducted a retrospective chart review of adult patients with a gynecologic malignancy who received care within our division and died between March 1, 2020, and May 30, 2024. Eligible patients were identified through the institution’s electronic medical record (EMR) system. We excluded patients who died at an outside hospital, had a cause of death unrelated to their cancer diagnosis, had missing data for preferred language, and/or did not have a documented office visit with a gynecologic oncologist from our division. Demographic and clinical data were obtained via chart abstraction.
Language concordance was determined by comparing the patient’s documented preferred language with the primary oncologist’s known language proficiency. The patient’s preferred language was obtained from a standardized, discrete field within the EMR, which is completed at the time of registration. Physician language fluency was determined by known language proficiencies and confirmed by division leadership. Care was classified as language concordant when the patient’s preferred language matched a language in which the oncologist was known to be fluent; otherwise, the patient’s care was classified as language discordant.
We compared baseline characteristics between language-concordant and language-discordant groups using chi-square or Fisher’s exact tests for categorical variables and t tests for continuous variables.
The primary outcome was performance on the NQF quality metric, quantified as a single numerical score (0–6) derived from the sum of the six variables: (1) chemotherapy in the last 14 days of life, (2) >1 ED visit in the last 30 days of life, (3) >1 hospitalization in the last 30 days of life, (4) ICU admission in the last 30 days of life, (5) cancer-related death in an acute care setting, and (6) no palliative care or palliative care initiated within three days of death. Of note, patients who died while admitted to inpatient hospice and/or the comfort care team were not considered to have died within the acute care setting. Each quality indicator was scored as 0 for nonoccurrence and 1 for occurrence. Accordingly, a higher score reflects more aggressive EOL care.
We used multivariable logistic regression to examine associations between language discordance and aggressive EOL care, defined as an NQF score ≥1. The model was adjusted for patient age, insurance payor, and cancer stage at the time of diagnosis. Results are presented as odds ratios (ORs) and adjusted odds ratios (aORs) with 95% confidence intervals (CIs). Analyses were performed using SAS, with two-sided p values of <0.05 considered statistically significant.
This study was deemed exempt from Institutional Review Board approval due to its retrospective design. All data were stored in a Health Insurance Portability and Accountability Act (HIPAA) compliant secure research environment, and no identifiable patient information was used in the analysis.
Results
We identified 98 patients with gynecologic malignancies who received care within our division and died during the study period. A total of 15 patients were excluded, including 2 who died at an outside hospital, 3 whose cause of death was unrelated to a gynecologic malignancy, and 10 without a documented office visit in our division within six months of death. Our cohort (n = 83) included 60 patients (72.3%) who received language-concordant care and 23 (27.7%) who received language-discordant care (Table 1).
Characteristics of Patients in the Language-Concordant and Language Discordant Groups
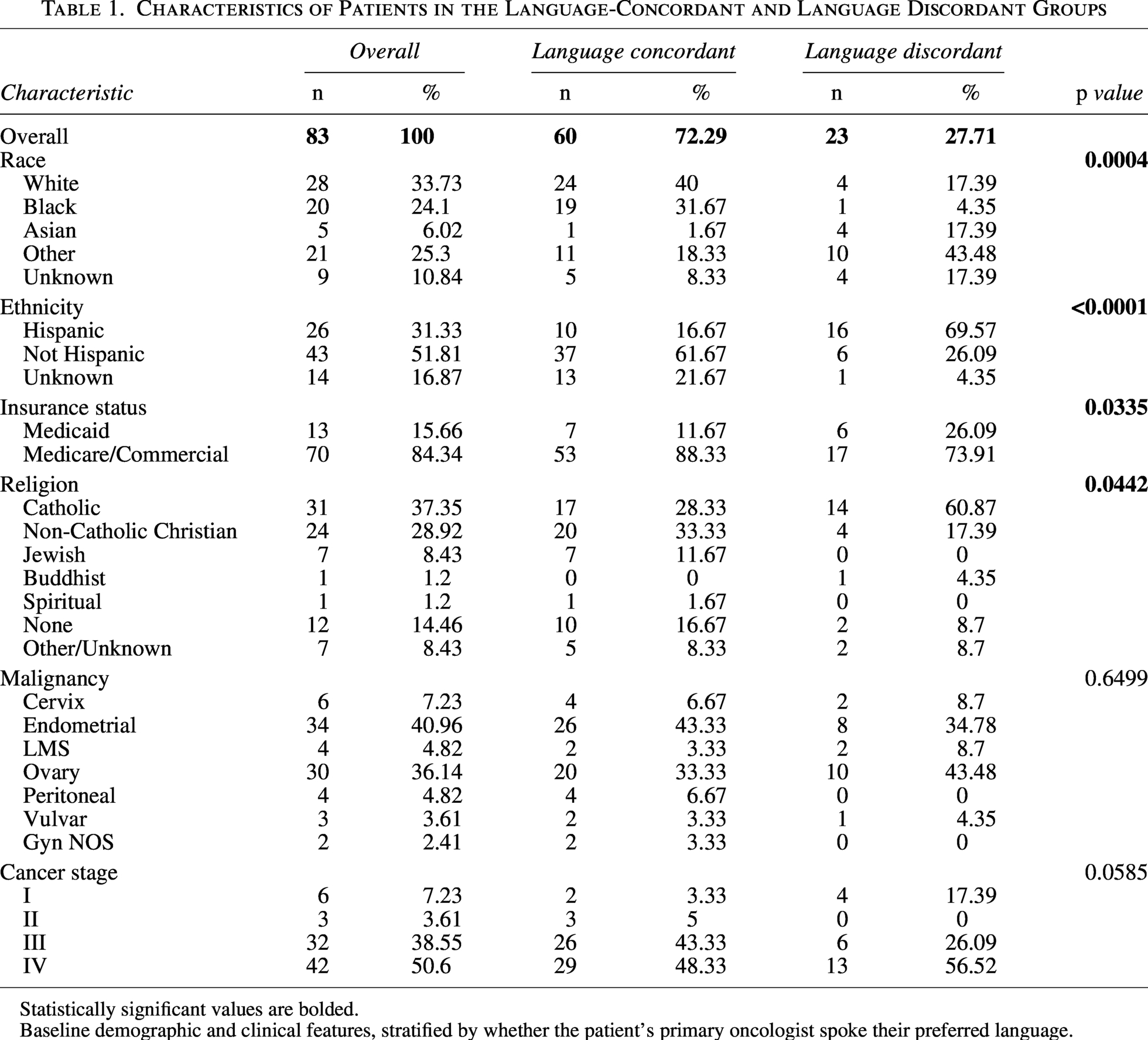
Statistically significant values are bolded.
Baseline demographic and clinical features, stratified by whether the patient’s primary oncologist spoke their preferred language.
Patients in the language-discordant group were more likely to identify as Hispanic (69.6% vs. 16.7%, p < 0.0001) and Asian (17% vs. 1%, p = 0.0004), though notably with a small overall sample size of Asian-identifying patients (n = 5). Groups also differed by insurance payor, with language-discordant patients more likely to have Medicaid insurance (26% vs. 12%, p = 0.0335), and religious affiliation, with language-discordant patients more likely to identify as Catholic (61% vs. 28%, p = 0.0004). There were no significant differences in the distribution of primary malignancy. Cancer stage at time of diagnosis approached but did not meet statistical significance (p = 0.0585).
Overall, 56 patients (67.5%) had NQF scores of ≥1, consistent with aggressive EOL care (Fig. 1). Patients who received language-discordant care were more likely to have an NQF score of ≥1 (87.0% vs. 60.0%, p = 0.0174). In an unadjusted comparison, there were no statistically significant differences between the two groups within each individual performance measure (Table 2). However, we observed a trend toward a difference in the likelihood of dying in the hospital, with this being more common for our patients receiving language-discordant care (61% vs. 40%, p = 0.08). The groups had similar rates of do not resuscitate (DNR) and do not intubate (DNI) at the time of death (Fig. 2).
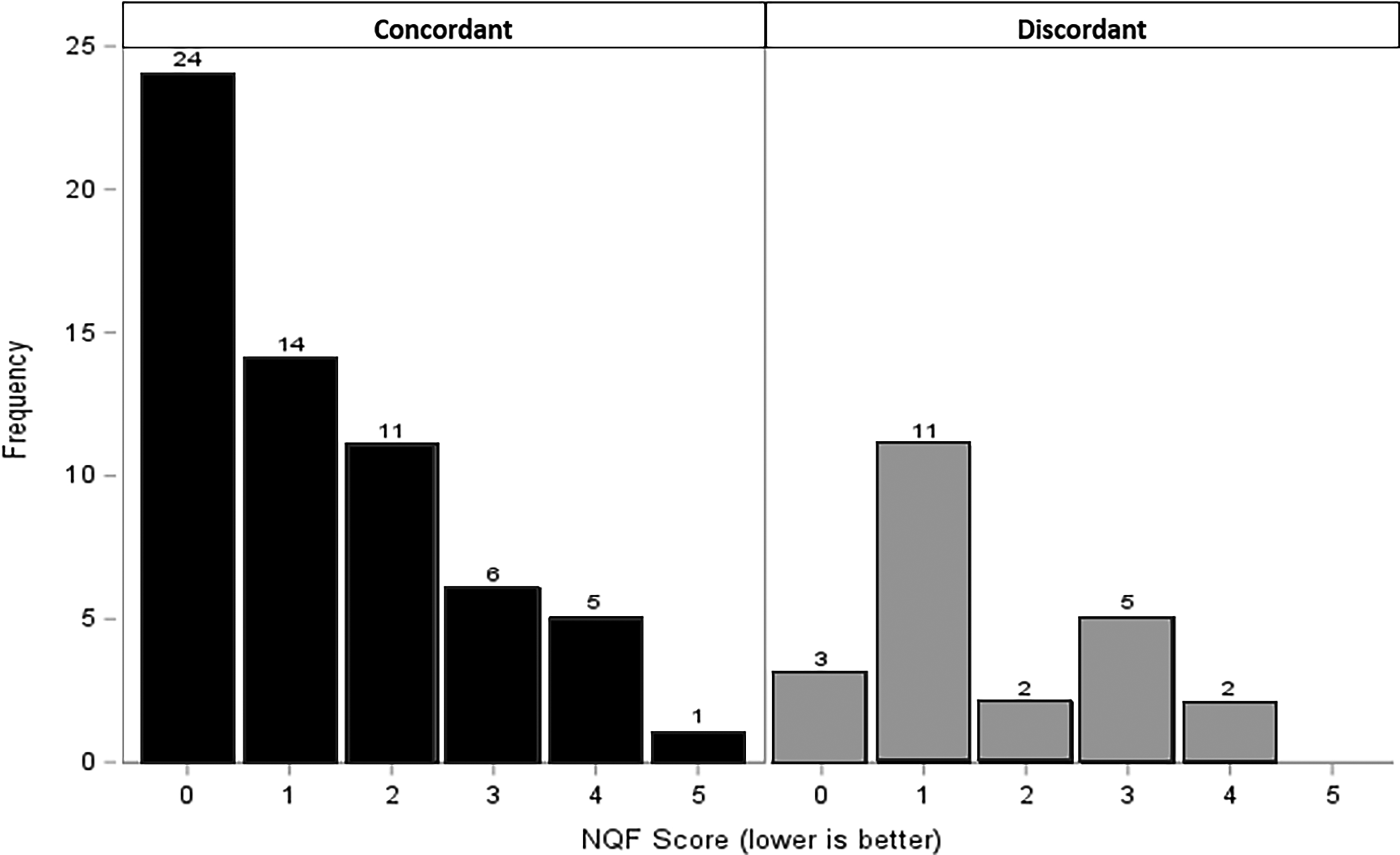
Distribution of National Quality Forum (NQF) performance scores stratified by language concordance. A higher score corresponds with more aggressive end-of-life care.
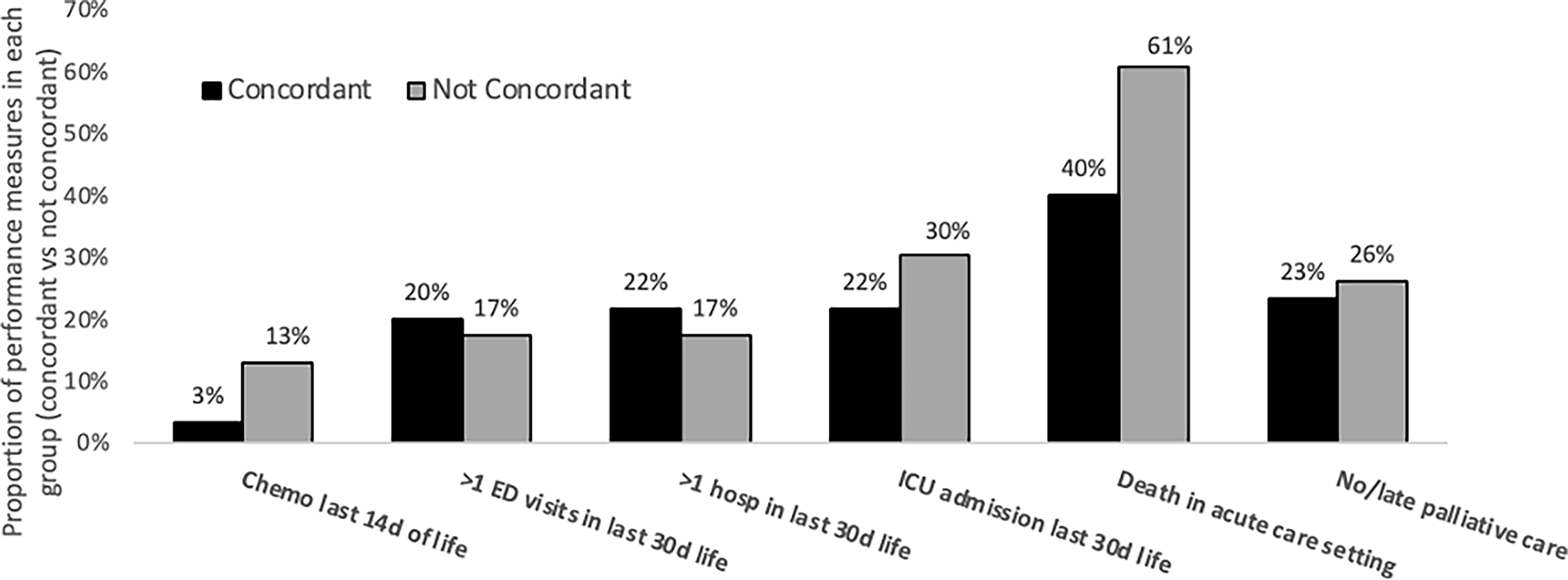
Breakdown of aggressive care by the 6 NQF metrics, concordant versus discordant. ED, emergency department; ICU, intensive care unit.
Performance on National Quality Forum End-of-Life Care Metrics
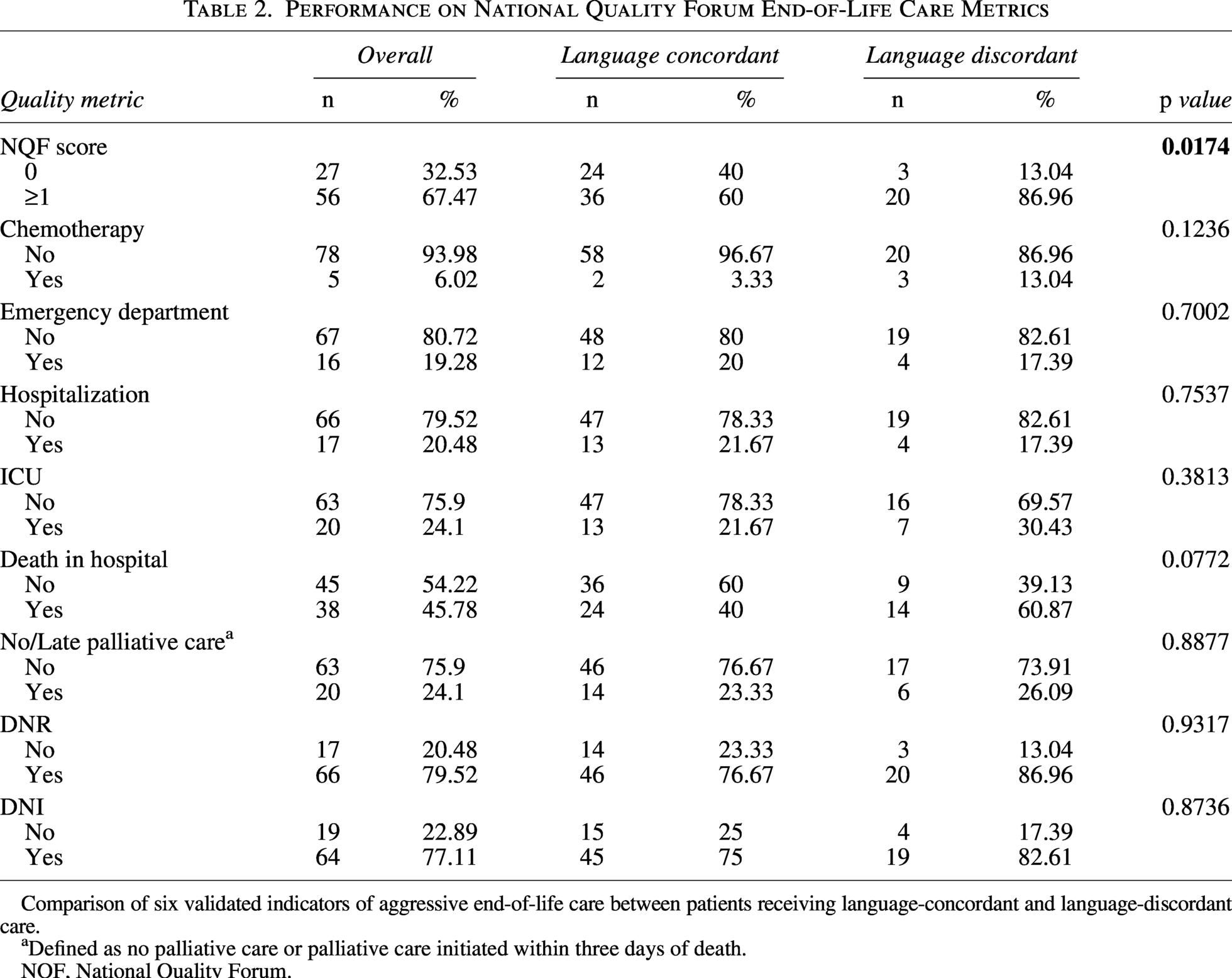
Comparison of six validated indicators of aggressive end-of-life care between patients receiving language-concordant and language-discordant care.
Defined as no palliative care or palliative care initiated within three days of death.
NQF, National Quality Forum.
In both simple and multivariable logistic regression models, language-discordant care maintained a statistically significant association with aggressive EOL care (Table 3). After adjusting for patient age, insurance payor, and stage at diagnosis, patients receiving language-discordant care were more than six times more likely than their language-concordant counterparts to receive aggressive EOL care (aOR: 6.05, 95% CI: 1.38–26.53).
Unadjusted and Adjusted Odds of Receiving Aggressive End-of-Life Care
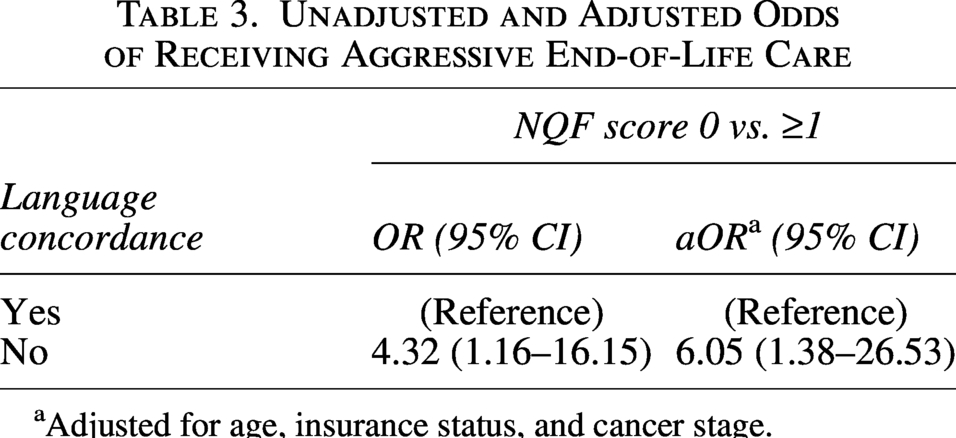
Adjusted for age, insurance status, and cancer stage.
Discussion
Among patients with gynecologic malignancies, language discordance between a patient and their primary oncologist is associated with an increased risk of aggressive EOL care, even after adjusting for patient age, insurance payor, and cancer stage at diagnosis.
Our findings align with existing literature demonstrating the contribution of language discordance to lower-quality EOL care. Prior works have demonstrated that patients requiring interpreters have less comprehensive communication with oncologists, resulting in greater unmet needs in palliative care and advance care planning (ACP), as well as higher rates of in-hospital death.1,3,14 A recent meta-analysis by Dookie and Martin concluded that language discordance limits adequate ACP and has a negative impact on palliative care, EOL care, and hospice care across multiple settings. The reviewers identified several factors contributing to this disparity, including limited access to skilled interpreters, variation in providers’ cultural competency and experience, and lack of alternate language options in patient resources. 15 Our study builds upon these findings, focusing specifically on gynecologic oncology.
The impact of aggressive EOL care can be profound for patients, caregivers, and the health care system. Aggressive interventions and lack of comfort measures—such as ICU admission, repeated hospitalizations, late chemotherapy, and short or absent hospice enrollment—have been shown to worsen patient quality of life near death, lower family satisfaction with care, and increase psychiatric morbidity among bereaved caregivers based on patient- and family-reported ratings. 16 Furthermore, family members of patients who received aggressive EOL care were less likely to feel that the care aligned with the patient’s preferences and more likely to report symptoms of major depressive disorder in bereavement.13,16 At the health care system level, aggressive EOL care drives greater health care utilization and costs, with disproportionate spending on life-sustaining treatments that often provide little or no benefit to patients.17,18 Further, a recent The Journal of the American Medical Association (JAMA) study demonstrated that clinicians exposed to aggressive EOL care report profound emotional distress and feelings of powerlessness, particularly when their efforts to deescalate nonbeneficial treatments are overridden by institutional pressures, leading to burnout and reduced willingness to advocate for less aggressive care in the future. 19 Understanding the impact of aggressive care on patients, caregivers, health care providers, and the health care system, as well as the association between overly aggressive EOL care and language discordance, does not only illuminate a disparity in care but also an opportunity for understanding and addressing the difference.
Although we examined aggressive EOL care as a composite NQF score to preserve statistical power, each individual component likely reflects distinct clinical and systemic drivers. For example, chemotherapy administration near death may be determined by communication of prognosis and shared decision-making, whereas ICU admission or in-hospital death may be influenced by communication of symptom management plans, late or incomplete goals of care discussions, or access to home hospice resources. Similarly, late or absent palliative care referral may reflect variability in institutional practice patterns, provider comfort with EOL care discussions, or patient and family preferences. The absence of statistically significant differences across individual markers in our study may reflect limited power; however, the composite finding suggests a broader pattern of increased EOL care aggressiveness that warrants further investigation in larger cohorts.
Our study is strengthened by its diverse patient cohort and validated NQF metrics, allowing for national benchmark comparisons. However, we recognize several limitations. First, this was a single-institution retrospective study with a relatively small sample size, limiting generalizability and precluding subgroup analyses by cancer type or specific language. Given the small cohort of patients, there was a paucity of patients with primary cervical and vulvar cancers and leiomyosarcoma. Second, language concordance was defined by EMR documentation and did not fully capture the variation in patients’ English proficiency or the quality of interpreters in language-discordant encounters. Furthermore, while our institution uses health care-trained interpreters, we did not have reliable data on interpreter utilization. As a result, we were unable to distinguish between encounters supported by professional interpreters and those without formal interpretation services. This limits our ability to assess how interpreter use may have affected the association between language discordance and the quality of EOL care. Third, unmeasured confounders, including cultural norms, caregiver involvement, and provider practice style, may have influenced the observed outcomes. For example, cultural norms surrounding disclosure of prognosis and decision-making may influence how information is conveyed within families and how decisions surrounding EOL care are made. Furthermore, we were unable to characterize the structure of EOL care discussions, including whether communication occurred directly with patients or indirectly through family members, and our retrospective design did not allow us to assess patient comprehension, use of teach-back techniques, and other communication dynamics that may have contributed to differences in EOL care decisions. Lastly, language discordance may be closely linked to other unmeasured social determinants of health, including socioeconomic status, health literacy, and immigration status. Although we adjusted for insurance status, this does not fully account for differences in income, education, or access to resources that may independently influence EOL decision-making. For example, the observed trend toward higher rates of in-hospital death among language-discordant patients may reflect limited access to home hospice resources, differences in understanding of hospice care, or cultural or religious preferences on place of death, rather than language alone.
In conclusion, we demonstrate that language discordance between patients and their gynecologic oncologists is associated with more aggressive EOL care. Conversely, our findings suggest that language concordance between patients and their primary oncologists leads to more patient-centered, goal-aligned EOL care. Future multiinstitutional studies with larger sample sizes are warranted to validate these findings and to evaluate interventions aimed at mitigating language-based disparities. Efforts to expand language-concordant care by standardizing timely, high-quality interpreters with cultural competency may improve both the quality and equity of EOL care in gynecologic oncology.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.