
Abstract
Background:
The Life-Sustaining Treatment (LST) Decisions Act in South Korea was implemented to promote patient-centered end-of-life (EoL) care.
Objectives:
To evaluate the impact of this legislation on LST practices for patients dying in the emergency department (ED).
Design:
A single-center retrospective study using interrupted time series (ITS) analysis.
Setting/Subjects:
Adult nontraumatic deaths in the South Korean ED between 2014 and 2024.
Measurements:
Changes in LST practices were assessed between pre- and post-Act groups (implemented February 4, 2018). Subgroup analyses by advanced cancer status were conducted, and interaction terms between ITS variables and advanced cancer status were evaluated using analysis of variance.
Results:
Among 1,058 patients (median age 77.0), rates of cardiopulmonary resuscitation (CPR) (26.8% vs. 15.1%, p < 0.001) and intubation (31.6% vs. 22.1%, p = 0.002) decreased after the Act, whereas antibiotic administration (60.6% vs. 69.3%, p = 0.009) and LST withdrawal (0.7% vs. 5.2%, p = 0.002) increased. The Act was associated with a decreasing postimplementation trend in intubation (p = 0.046). In patients with advanced cancer, CPR and intubation rates were similar before and after the Act, while a significant interaction between the Act and advanced cancer status was observed for CPR (p = 0.007).
Conclusions:
Following the legislation, the provision of invasive LST, such as CPR and intubation, at the EoL phase in the ED decreased. These shifts, primarily observed in patients without advanced cancer, indicate that the Act successfully catalyzed EoL discussions and promoted goal-concordant care for this population.
Key Message
Following South Korea’s Life-Sustaining Treatment Decisions Act, the provision of invasive end-of-life interventions, such as cardiopulmonary resuscitation and intubation, significantly decreased in the emergency department. Crucially, these reductions were confined to patients without advanced cancer, highlighting that legislative impacts on end-of-life care vary significantly by underlying clinical profiles.
Introduction
The end-of-life (EoL) phase is a critical period that completes a personal narrative. 1 The contemporary medical environment often prioritizes life-prolonging interventions,2,3 which can lead to the medicalization of death.4,5 Nevertheless, the provision of patient-centered EoL care remains essential for a dignified passage.6,7 Although death within the emergency department (ED) is infrequent,8,9 the ED inevitably becomes the final setting of care for some individuals. The primary focus of emergency care is on the rapid resuscitation and stabilization of acute medical conditions.10,11 Consequently, aggressive life-sustaining treatment (LST) that may be futile is frequently administered to patients at the EoL, making the ED a potentially suboptimal setting for the dying process.12,13 Because some deaths in the ED are unavoidable, the ED represents a critical front line where acute care and palliative care principles must be integrated. Accordingly, the ED must be equipped for the provision of high-quality EoL care.10,12,14
To enhance EoL care within the ED, characterizing LST practices for dying patients in this setting is crucial. This has become particularly important after a major legislative change in South Korea. Reflecting global trends toward palliative care principles, South Korea established “The Act on Hospice and Palliative Care and Decisions on Life-Sustaining Treatment for Patients at the End-of-Life” (hereafter referred to as the LST Decisions Act), which came into effect in February 2018. The Act aims to protect human dignity by respecting self-determination regarding LST. This legislation enabled the withholding or withdrawal of LST as a legally protected option for patients in the EoL phase.15,16 Specifically, the Act establishes a hierarchical process to verify patient preferences: (1) existing advance directives, (2) Physician Orders for Life-Sustaining Treatment (POLST) for capable patients, or (3) surrogate decision-making based on family testimony of consistent prior preferences or unanimous family consensus.
After implementation, studies have reported increased rates of self-determination regarding LST and earlier decision-making, particularly among cancer patients.16–18 However, the Act’s specific influence on LST practices within the ED context has not been thoroughly examined. Given this background, this study aimed to explore long-term temporal trends in LST provision for patients dying in the ED and evaluate their association with the LST Decisions Act. In addition, we explored whether the Act’s impact differed between patients with and without advanced cancer.
Methods
Study design and population
This single-center retrospective cohort study was conducted at a tertiary academic hospital’s ED in South Korea, with approximately 60,000 annual visits. Adult patients aged 18 years or older who presented to the ED from January 2014 to December 2024 and subsequently died in the ED were included. Patients who received cardiopulmonary resuscitation (CPR) upon ED arrival or those who died due to trauma were excluded. The study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (approval No. B-2504-969-102). The requirement for informed consent was waived due to the retrospective nature of this study.
Study measures
Data were extracted from the electronic medical records by physician researchers. We collected demographic information (age and sex) and clinical variables, including underlying comorbidities. For comorbidities, advanced cancer was defined as metastatic, recurrent, or progressive locally advanced malignancies, consistent with prior literature descriptions.19,20 We also collected the documentation status of advance care planning (ACP) forms, including Do-Not-Resuscitate (DNR) orders, advance directives, or POLST forms both prior to and after ED presentation. Under the Act, legitimately withholding treatment requires finalizing documentation during the imminent dying phase, even if prior directives exist. Thus, these two timing categories are not mutually exclusive. Since advance directives and POLST forms are legal documents established by the LST Decisions Act, they were only available after its implementation. Before this law, only the DNR order was in use. Following the implementation, a standardized flowchart for ACP form documentation was distributed and the documentation process based on this flowchart was structurally integrated into the hospital’s electronic medical record system to guide clinical decision-making and ensure legal compliance. The cause of death for each patient was determined by physician researchers based on a review of medical records. Identified causes were then classified using the classification system from the Cause-of-Death Statistics by Statistics Korea, which is based on the World Health Organization’s International Classification of Diseases guidelines. 21
The primary outcomes were the proportions of patients who received each LST measure and the proportion of patients who withdrew any LST measures. According to the LST Decisions Act, LST includes CPR, endotracheal intubation, hemodialysis, chemotherapy, extracorporeal life support, transfusion, and vasopressors. Among these, chemotherapy and extracorporeal life support are not performed in our ED and were excluded. Furthermore, although antibiotic administration is not defined as an LST under the Act and its classification varies internationally, 22 we included it based on the ongoing interest in the appropriateness of antibiotic use during the EoL phase.23–25
Statistical analysis
Continuous variables were expressed as medians and interquartile ranges (IQR), whereas categorical variables were presented as absolute counts and percentages. Patients were classified into two groups based on presentation date, using the LST Decisions Act’s implementation date (February 4, 2018) as the dividing point: a pre-Act group (presented before this date) and a post-Act group (presented on or after this date). An adjustment period (January 1–April 30, 2018) was set to account for the law’s transitional phase, and patients presented during this period were excluded. To compare the two groups, we used the Student’s t-test or the Mann–Whitney U-test for continuous variables, and the chi-square test or Fisher’s exact test for categorical variables, as appropriate.
To evaluate the association between the Act’s implementation and the changes in LST practices, an interrupted time series (ITS) analysis was employed. The study period was aggregated into 4-month intervals. The intervention was defined as the implementation of the LST Decisions Act. A generalized linear model was selected to assess the effect of the intervention. The model included terms to estimate the baseline trend (pre-Act slope), an immediate level change following the intervention, and the post-intervention trend change (slope change). The absence of systematic autocorrelation was confirmed by examining the autocorrelation function plots (which revealed only isolated spikes) and performing Ljung–Box tests for multiple lags (all p > 0.05). Furthermore, we conducted subgroup analyses stratified by advanced cancer status. To explore the differential impact of the law by subgroup, we added interaction terms between the ITS variables and advanced cancer status. The significance of this overall interaction was assessed by comparing the models with and without these interactions using an analysis of variance (ANOVA). In addition to ITS analysis, locally estimated scatterplot smoothing was used to visualize continuous, nonlinear temporal trends in LST provision across the entire 11-year period, including the adjustment period to capture the full trajectory.
Statistical analyses were performed using R (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria) and RStudio (version 2025.05.1 + 513; Posit Software, PBC, Boston, MA, USA). p-Value < 0.05 indicated statistical significance.
Results
Study population characteristics
A total of 510,061 adult patients visited the ED during the study period, among whom 2,956 (0.58%) died in the ED. An initial cohort of 1,088 patients was established after excluding patients with cardiac arrest upon arrival (n = 1,831) and trauma-related death (n = 37). An additional 30 patients who presented during the adjustment period were also excluded, resulting in a final cohort of 1,058 patients for analysis (median [IQR] age 77.0 [65.8–85.0] years, 424 [40.1%] female) (Fig. 1 and Table 1). Of this final cohort, 269 patients (25.4%) presented before the LST Decisions Act’s implementation and 789 (74.6%) presented after. The post-Act group was significantly older (p = 0.004) than the pre-Act group, and the sex distribution did not differ significantly (Table 1). Underlying comorbidities were similar between the groups, except for diabetes and chronic renal disease. The proportion of patients with ACP forms documented prior to ED presentation was significantly higher in the post-Act group (23.7%) compared to the pre-Act group (4.8%) (p < 0.001). Similarly, the proportion of patients who completed ACP forms during their ED stay also increased significantly following the Act’s implementation (85.1% vs. 91.5%, p = 0.003) (Table 1). Causes of death in the cohort are presented in Supplementary Table S1. Malignant neoplasm was the most prevalent cause of death (36.0%), followed by pneumonia (27.9%) and sepsis (11.7%). When comparing the pre- and post-Act groups, the distribution of causes of death differed significantly only for other digestive and circulatory diseases (p = 0.008 and 0.04, respectively).
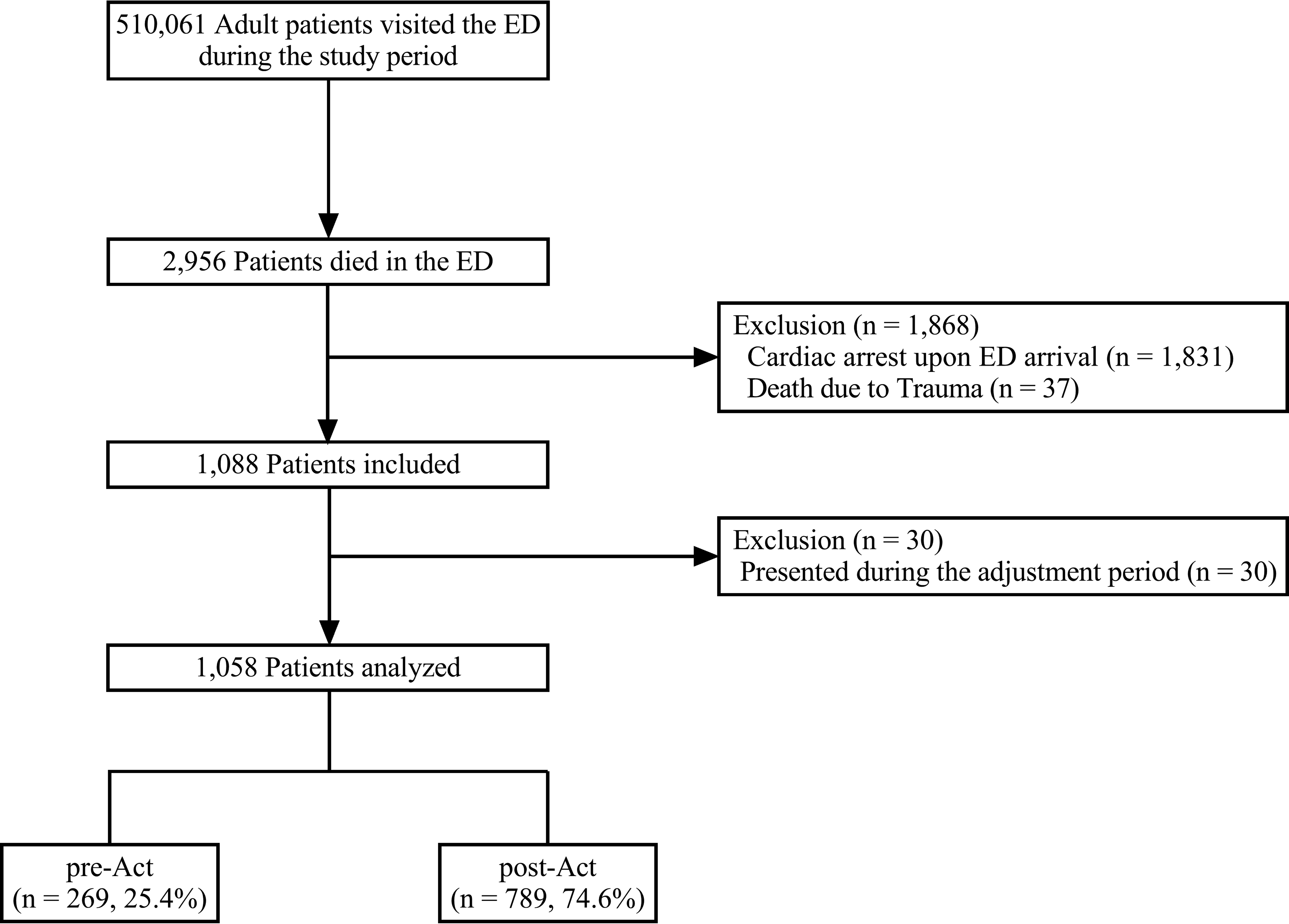
Study flowchart. The cohort was divided into a pre-Act group and a post-Act group based on the implementation date of the Life-Sustaining Treatment Decisions Act (February 4, 2018). ED, emergency department.
Characteristics of Patients
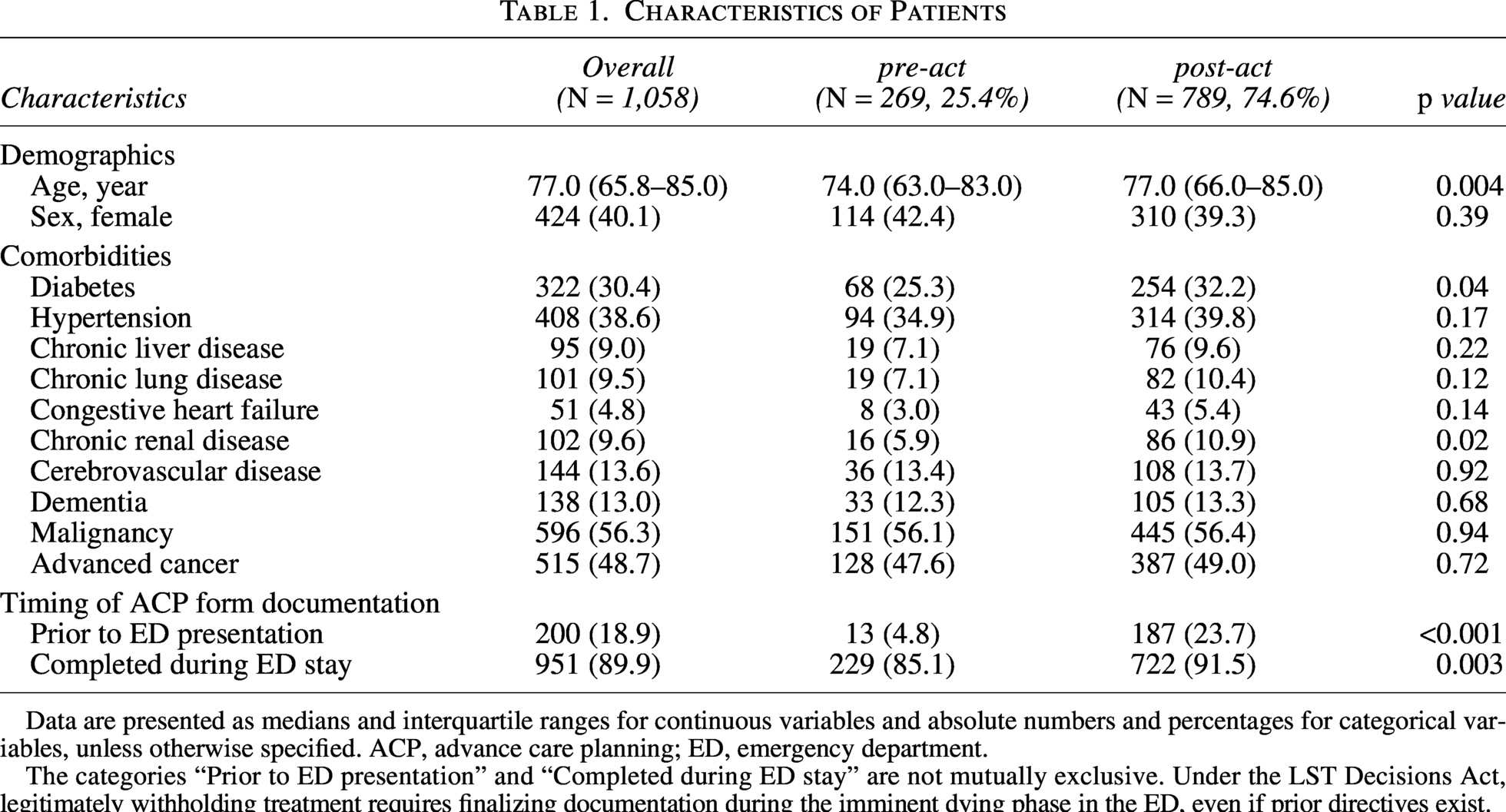
Data are presented as medians and interquartile ranges for continuous variables and absolute numbers and percentages for categorical variables, unless otherwise specified. ACP, advance care planning; ED, emergency department.
The categories “Prior to ED presentation” and “Completed during ED stay” are not mutually exclusive. Under the LST Decisions Act, legitimately withholding treatment requires finalizing documentation during the imminent dying phase in the ED, even if prior directives exist.
Temporal trends in life-sustaining treatment practices
Regarding LST practices, the rates of CPR and intubation were significantly lower in the post-Act group compared to the pre-Act group (CPR: 26.8% vs. 15.1%, p < 0.001; Intubation: 31.6% vs. 22.1%, p = 0.002), while no significant differences were found for the use of vasopressor, hemodialysis, or transfusion (Table 2). Conversely, antibiotics were administered more frequently in the post-Act group (60.6% vs. 69.3%, p = 0.009). The withdrawal of any LST measures was also significantly more common in the post-Act group (0.7% vs. 5.2%, p = 0.002).
Provision of Life-Sustaining Treatments
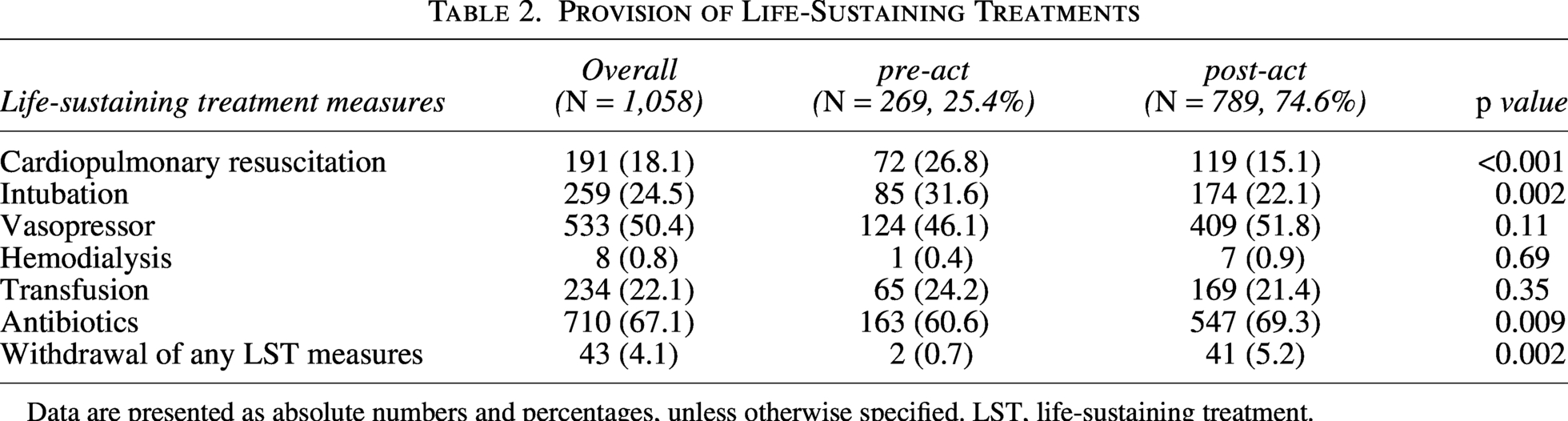
Data are presented as absolute numbers and percentages, unless otherwise specified. LST, life-sustaining treatment.
The temporal trends for each LST measure, based on ITS analysis, are presented in Figure 2, with the ITS coefficients shown in Table 3. Hemodialysis was excluded from the ITS analysis due to the low number of cases. The analysis of the pre-Act period revealed no significant trends for any LST measure. Regarding the immediate level change after the adjustment period, only antibiotic use showed a significant increase (p = 0.04). For the pos-tintervention trend change, only intubation showed a significant result (p = 0.046), indicating a decreasing trend after the implementation. Additionally, the continuous temporal trends of LST provision over the entire 11-year study period, including the adjustment period, are illustrated in Supplementary Figure S1.
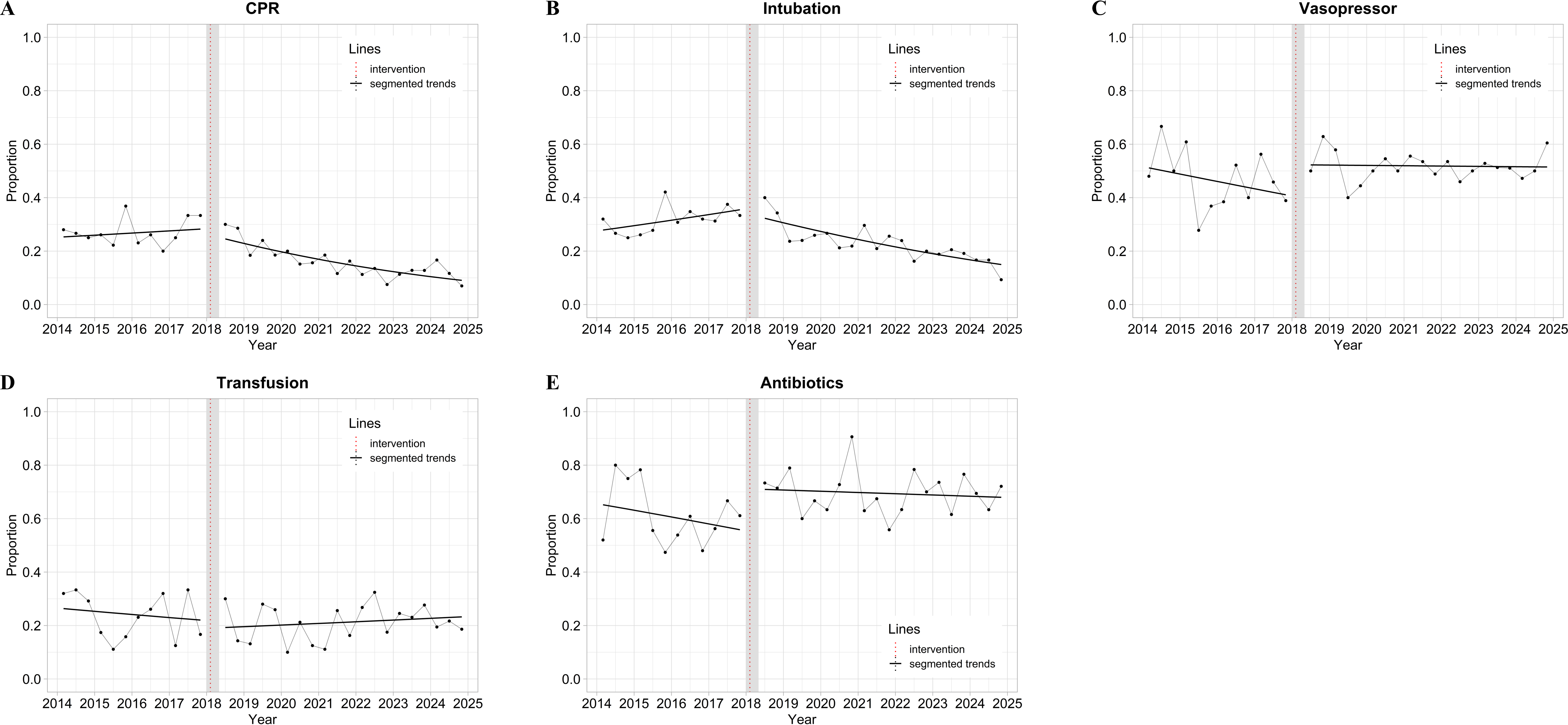
Temporal trends in the provision of life-sustaining treatments. Interrupted time series analyses for the proportion of patients receiving.
Interrupted Time Series Analysis Coefficients
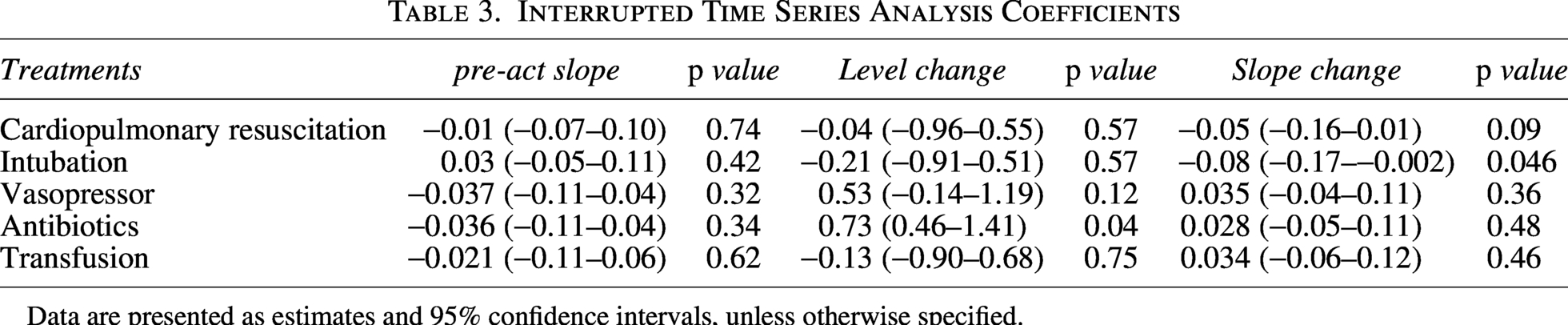
Data are presented as estimates and 95% confidence intervals, unless otherwise specified.
Subgroup analysis (stratified by advanced cancer status)
The characteristics of patients stratified by advanced cancer status are presented in Supplementary Tables S2 and S3. Regarding the timing of ACP form documentation, both groups showed a significant increase in the proportion of patients with forms documented prior to ED presentation after the Act (without advanced cancer: 0.7% vs. 15.7%, p < 0.001; with advanced cancer: 9.4% vs. 32.0%, p < 0.001). Regarding the proportion of patients who completed ACP forms during their ED stay, there was no significant difference in the advanced cancer group (96.9% vs. 95.1%, p = 0.47), whereas a significant increase was observed in the group without advanced cancer (74.5% vs. 88.1%, p < 0.001). For LST provision (Table 4), the rates of CPR, intubation, and transfusion significantly decreased in the group without advanced cancer (p < 0.001, p = 0.003, and p = 0.03, respectively), whereas no significant changes in these measures were observed in the group with advanced cancer. Conversely, antibiotic administration significantly increased in the advanced cancer group (p = 0.01) but not in the group without advanced cancer (p = 0.24). Finally, the withdrawal of LST significantly increased in the group without advanced cancer (p = 0.01) but not in the advanced cancer group (p = 0.09). The temporal trends for each LST measure from the ITS analysis, stratified by advanced cancer status are presented in Figure 3. The ANOVA results, comparing models with and without interaction terms for advanced cancer status, showed a significant effect for CPR (p = 0.007) but not for intubation (p = 0.32), vasopressor (p = 0.09), antibiotics (p = 0.52), or transfusion (p = 0.22).

Temporal trends in the provision of life-sustaining treatments stratified by advanced cancer status. Interrupted time series analyses for the proportion of patients receiving.
Provision of Life-Sustaining Treatments (Stratified By Advanced Cancer Status)
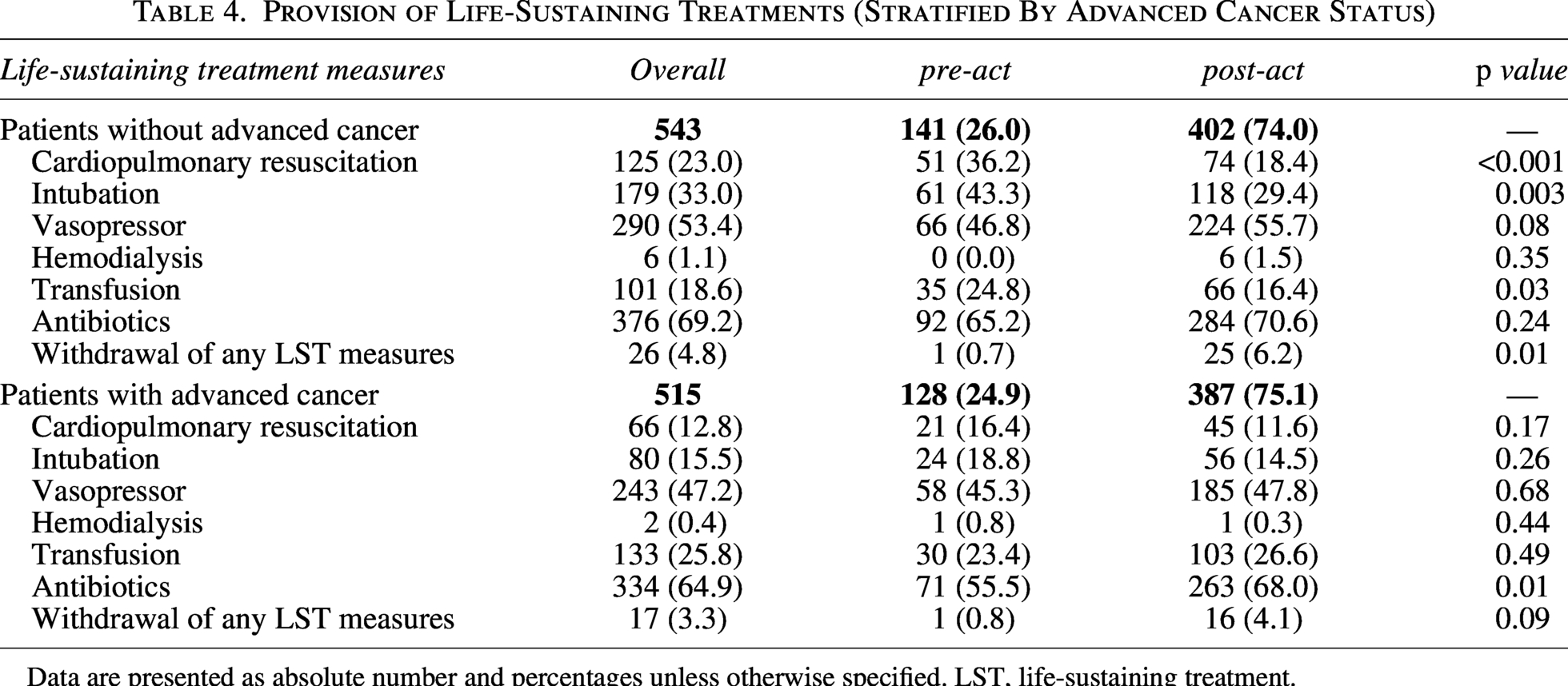
Data are presented as absolute number and percentages unless otherwise specified. LST, life-sustaining treatment.
Discussion
This study demonstrates that the implementation of the LST Decisions Act was associated with a significant reduction in invasive LST, such as CPR and intubation, during the EoL phase in the ED. However, this legislative impact was not uniform across all patient groups. While a distinct decrease in invasive care was observed in patients without advanced cancer, practice patterns for those with advanced cancer remained largely unchanged.
A previous study analyzing cancer deaths found no significant changes in the provision of CPR (2.8% vs. 3.2%) and mechanical ventilation (8.4% vs. 8.5%) within 1 month of death before and after the law. 16 While this finding is consistent with our results, their study was not specific to the ED setting. Other studies investigating patients who died in the ED yielded similar findings. One study found that patients with cancer received CPR less frequently than those without cancer (23.4% vs. 48.4%). 9 Another study found that cancer patients received significantly less CPR (22.7% vs. 35.8%, p = 0.035) and mechanical ventilation (28.4% vs. 49.4%, p = 0.002) compared with noncancer patients. 26 The latter study also reported decreasing trends in the proportion of patients receiving CPR (from 39.0% in 2018 to 22.0% in 2020) and mechanical ventilation (from 39.0% to 35.0%). 26 However, because these analyses were restricted to the post-Act period, they could not evaluate the direct impact of the legislation.
Our study focused on deaths within the ED, thereby characterizing LST practices during the immediate EoL phase and reflecting the real-time decision-making dynamics unique to this acute care setting. Furthermore, we examined each LST measure separately and found that the Act’s impact was selective, mainly affecting invasive measures. We utilized ITS analysis to distinguish the Act’s specific effect from potential pre-existing trends that might have arisen from both a broader societal shift toward palliative care and the gradual accumulation of EoL care experience within our institution. We observed no significant pre-existing trends for any LST measure, and isolated the Act’s specific impact, confirming a significant decreasing trend for intubation, thereby demonstrating how such legislation can reshape clinical practices. Furthermore, subgroup analyses revealed that the Act’s impact differed between patients with and without advanced cancer. While the overall rate of ACP form completion during the ED stay was already high before the legislation (85.1%), this baseline was primarily driven by patients with advanced cancer (96.9%). For these patients, invasive LST was already provided less frequently, suggesting that EoL discussions were sufficiently established regardless of the legislation. Conversely, the Act demonstrated a pronounced effect among patients without advanced cancer. Given that palliative and EoL care discussions were traditionally less established for this population,27,28 the legislation appears to have catalyzed these conversations. In the acute ED setting, while physicians often catalyze EoL discussions, the Act functions as an ethical guide and a legal safeguard. It ensures that clinical decisions prioritize patient autonomy, thereby preventing unilateral physician paternalism. When a patient lacks decision-making capacity, the legislation guides a shared decision-making process with family members, shifting the paradigm toward patient-centered care. Furthermore, this legally protected framework alleviates families’ profound psychological burden and guilt during surrogate decision-making. This shared security may have facilitated goal-concordant care, driving the observed reduction in invasive interventions, particularly for noncancer patients.
Notably, the Act’s impact on CPR differed by advanced cancer status, whereas its effect on intubation did not. This may reflect a hierarchical perception of invasiveness. CPR is often considered the most aggressive intervention and was likely already withheld in patients with a clear terminal trajectory. In contrast, intubation is commonly perceived as a reversible, time-buying measure, and thus may have been used more liberally in advanced cancer patients before the legislation. The legislation likely reframed intubation as an invasive LST requiring deliberate consideration, leading to a uniform reduction across groups and no differential effect. In addition, antibiotic administration increased, despite no rise in infection-related deaths. This pattern may reflect a compensatory tendency to “do something” while withholding invasive LST. Given that antimicrobial therapy at the EoL may prolong the dying process without ameliorating symptoms, 29 closer antibiotic stewardship is warranted to ensure patient-centered palliative goals. Although patients and caregivers often present to the ED seeking acute management and full life-saving treatments, emergency physicians must provide care that balances medical intervention with the preservation of patient dignity. 11 The decrease in invasive LST in our study highlights the ED’s expanding role not only in life-saving care but also in EoL discussions. With legal support and cultural change, the ED can support goal-concordant care. To sustain this shift, policies must provide resources and strengthen communication training for clinicians to conduct sensitive EoL discussions, particularly for non-cancer patients whose illness trajectories are often less predictable.
This study has several limitations. First, as a retrospective, single-center analysis, our findings may have limited generalizability. As a tertiary referral center, our cohort included a substantial proportion of patients with advanced cancer (48.7%), which may not represent general EDs. Consequently, the observed LST practices may reflect our ED’s extensive experience in caring for cancer patients and may differ at other institutions. Also, potential changes in institutional factors could act as confounders because of the long study period. However, we utilized ITS analysis to control for pre-existing trends resulting from institutional factors. Furthermore, the discrepancy in outcomes by advanced cancer status suggests that the observed changes are more likely attributable to the legislative intervention than to generalized institutional evolution. Second, despite the 11-year study period, the rarity of death in the ED resulted in a limited number of events, especially for subgroup analyses, which may have reduced statistical power. This may explain the failure to detect statistically significant trend changes for CPR or certain interaction effects.
Conclusions
Following the implementation of the LST Decisions Act, the provision of invasive LST, specifically CPR and intubation, during the EoL phase in the ED decreased. These reductions, primarily observed in patients without advanced cancer, indicate that the legislation effectively catalyzed EoL discussions and promoted goal-concordant care for this population, thereby bridging a critical gap in emergency palliative care.
Ethical Approval and Informed Consent Statements
The study protocol was reviewed and approved by the Institutional Review Board of Seoul National University Bundang Hospital (approval No. B-2504-969-102). The requirement for informed consent was waived due to the retrospective nature of this study.
Data Availability Statement
The datasets presented in the current study are available by the corresponding author on reasonable request.
Authors’ Contributions
Y.W.U.: Writing—original draft, writing—review and editing, methodology, conceptualization, investigation, formal analysis. H.E.K.: Writing—review and editing, data curation, formal analysis. J.E.H.: Writing—review and editing, investigation. S.H.K.: Writing—review and editing, data curation, formal analysis. J.H.L.: Writing—review and editing, methodology, supervision. Y.H.J.: Writing—review and editing, methodology, conceptualization, supervision. All authors made final approval of the version to be submitted.
Footnotes
Author Disclosure Statement
All authors declare that they have no competing interests.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.