
Abstract
Introduction:
Physician-assisted dying (PAD) is legal in an increasing number of jurisdictions across the United States. Despite this, formal hospice and palliative medicine (HPM) fellowship curricula on PAD are lacking. To address this, a neutral (nonadvocacy) PAD pilot curriculum was developed and implemented in one large HPM fellowship program.
Methods:
A five-lecture curriculum was developed by an interdisciplinary group using Kern’s six-step method. Comfort, knowledge, and satisfaction were assessed.
Results:
17 fellows were eligible to complete curriculum assessments with a 76% response rate on the postcurriculum survey (N = 13). Self-reported comfort improved significantly across all measured domains. Ninety-two percent of respondents were very or somewhat satisfied; 85% of respondents agreed the curriculum maintained a neutral tone.
Conclusion:
HPM fellows value PAD education, even when practicing in a state where it is illegal. A neutral curriculum is feasible, improves comfort, and is well received. This offers a model for integrating PAD education into HPM training.
Introduction
In the United States, physician-assisted dying (PAD) describes situations where competent, terminally ill patients legally request and intentionally ingest a prescribed lethal medication to cause their own death. Other names for PAD include medical aid in dying and physician-assisted suicide. This practice is currently legal for approximately 25% of the U.S. population but remains a contentious topic. Although some groups in California and Canada have described curricula for trainees, they are largely focused on how to provide PAD in clinical practice.1–4 There is no standardized or even published approach on how to address the topic of PAD with hospice and palliative medicine (HPM) fellows. Even clinicians in states where the practice is not yet legal should be prepared to engage on the topic, since all terminally ill patients in the United States have access to PAD after the residency requirement was lifted in Vermont and Oregon.
We previously conducted a needs assessment, which showed that our HPM fellows believe formal PAD education in their fellowship curriculum is important even if they do not intend to provide PAD in their future career. 5 The majority of fellows reported having limited exposure to and no prior formal education on the topic. 5 Based on these findings, we developed a pilot curriculum on PAD for the HPM fellows at our institution. The goal of the curriculum was to provide them with basic knowledge of PAD and improve their comfort in responding to patient inquiries.
Methods
This educational study was exempted by the Institutional Review Board. All HPM and Geriatrics fellows at the study site participated in the curriculum, which took place between January and June 2025. Precurriculum assessments were administered before the first lecture, and postcurriculum assessments were administered after the final lecture. Attendance was self-reported by participants on the postcurriculum assessment.
A committee of interdisciplinary HPM clinicians (physician fellows, faculty physicians, bioethicists, and a chaplain) designed an intentionally neutral (nonadvocacy) curriculum to align with the American Academy of Hospice and Palliative Medicine position of studied neutrality and their related entrustable professional activities.6,7 Kern’s six-step method for curriculum development was used, and topics for the lectures were informed by data from a prior needs assessment.5,8 Learning objectives were then developed using the limited available literature and best practices on topics. The curriculum consisted of five, 60-minute sessions, delivered both virtually and in person, during regularly scheduled didactics, which fellows are required to attend. Topics and relevant learning objectives for each session are described in Table 1 along with relevant references, which are also cited below.9–35 Didactic, discursive, and role-playing educational strategies were used. Seventeen fellows were eligible to participate in the curriculum assessment. The content was taught by A.E., J.C., M.K., R.M.A., and L.B. Guest speakers were invited to share expertise on or experience with PAD for three of the lectures: “What Happens During PAD?,” “Conscientious Objection and Bereavement,” and “Ethical Considerations.”
Summary of Curriculum Content

PAD, physician-assisted dying.
We developed pre- and postsurveys to evaluate fellows’ knowledge about PAD and comfort with identified skills, based on the established learning objectives and best practices for educational assessment (Table 2). The postsurvey also included questions about satisfaction, usefulness, ongoing unmet needs, and future curriculum improvement. Surveys were administered anonymously through institutional email to all eligible fellows. The surveys were voluntary without incentive for participation. No demographic data was obtained to ensure anonymity. Given the small sample size and subsequent nonparametric data distribution, the Fisher’s exact test was used to compare comfort and knowledge scores as well as proportions of unmet needs. A significance value of ɑ < 0.05 was used, despite the small sample size.
Comfort and Knowledge Scores Pre- and Postcurriculum

Throughout the curriculum, a virtual anonymous comment box was made available for issues or concerns. This was shared at the beginning and end of every lecture and included as a quick response (QR) code on various slides during presentations. It was also available between lectures. A statement emphasizing the goal of the curriculum was read at the beginning of each lecture: “Prior to beginning today’s lecture, we would like to plainly acknowledge that we as presenters and educators aren’t advocating for or against PAD, clinically or legally. We hope to strike an important balance; one of “engaged neutrality.” Communities are legalizing PAD, our patients will inevitably ask about it, and occasionally there will be patients who believe it’s the right choice for them. In such situations, we need to be engaged with and aware of the topic, to best understand how to work with these patients effectively, ethically, and safely.”
Results
The precurriculum survey response rate was 59% (N = 10/17), and the postcurriculum survey response rate was 76% (N = 13/17). Fellows reported attending, on average, 3.3 (of the five) lectures each, and the median number of attended lectures was four per fellow. The most attended lecture was on responding to requests for hastened death, with all but one fellow attending.
Knowledge and comfort scores were compared before and after the curriculum (Table 2). Comfort in all five educational domains improved significantly after the curriculum. None of the changes in knowledge scores reached statistical significance except for an improvement in the understanding of definitions of various assisted-dying practices. On the postcurriculum survey, 92.3% (N = 12/13) of respondents were very or somewhat satisfied with the curriculum and 84.6% (N = 11/13) of respondents found the curriculum very or somewhat helpful. When compared to the initial needs assessment, there was a 39% increase in the number of respondents who thought that it was very important that palliative care fellowship training include teaching on assisted death, though this did not reach a level of statistical significance (Fig. 1, 67% vs. 92%, p = 0.1).
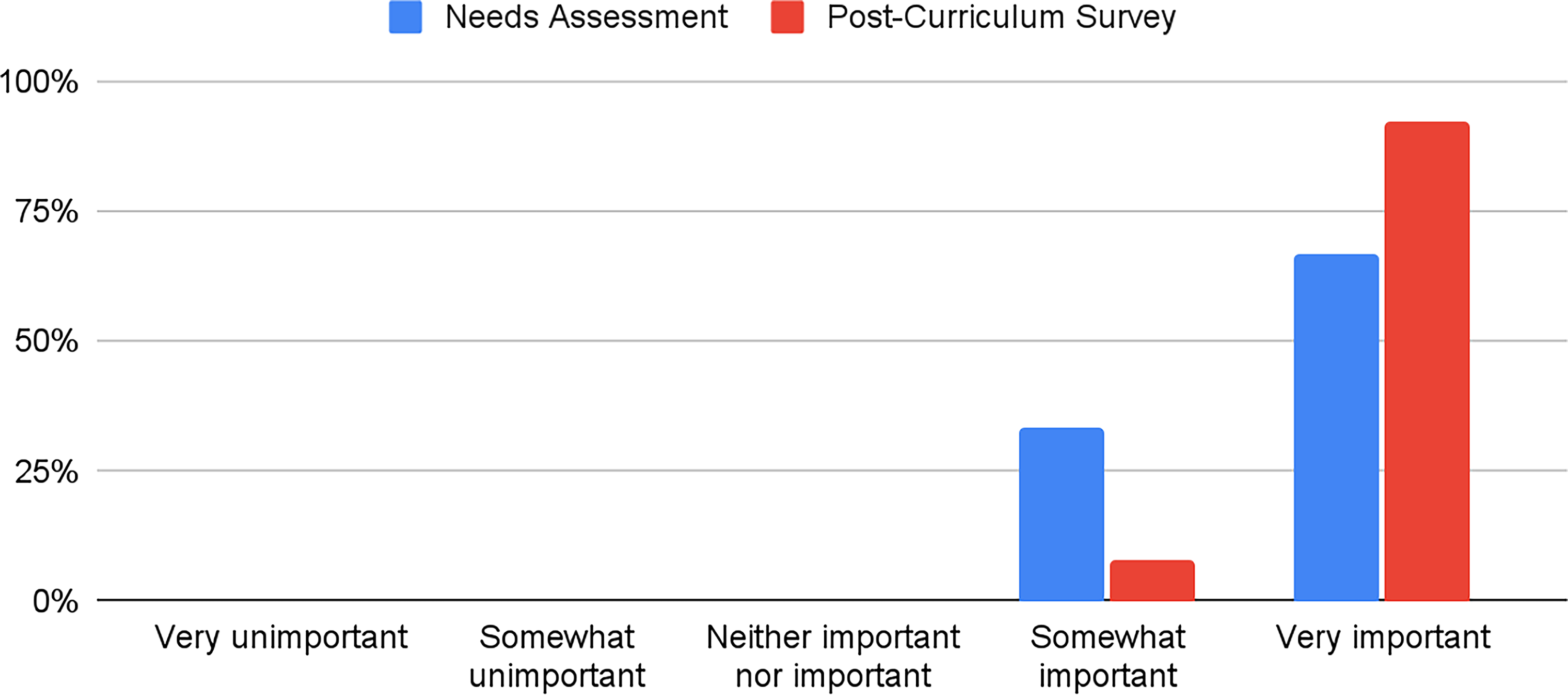
In your opinion, how important is it that your palliative care fellowship training includes teaching on assisted death?
On the initial needs assessment, three fellows had reported never thinking about whether or not they would provide assisted death in their future clinical practice. After the curriculum, all fellows had thought about the question, and the proportion of fellows considering providing PAD was the same (7.7% on the postassessment vs. 9.5% on the needs assessment). The other fellows were evenly split between not considering providing PAD (N = 6, 46.2%) and unsure about providing PAD (N = 6, 46.2%) after the curriculum. Almost all the fellows found the curriculum to be neutral regarding PAD (Fig. 2). One participant felt that “the disclaimer at the beginning was helpful.” Another participant felt there was “little time for constructive discussion given the organization of the lecture.”

How did you find the tone of the curriculum overall?
Discussion
This represents the first published pilot curriculum on PAD specifically for HPM fellows. Overall satisfaction with the pilot curriculum was high, and fellows reported improved comfort levels across all domains, though improvements in knowledge were not statistically significant. Most participants found the curriculum to be neutral, which reflects the care that was taken to create a curriculum that reflected an attitude of “engaged neutrality,” consistent with HPM professional society stances on the topic. The proportion of fellows considering practicing PAD remained unchanged from the initial needs assessment, and a substantial number continued to report they were still unsure about what they would do in the future. These findings further validate the neutral tone of the curriculum.
A significant limitation to this study is that change in knowledge was self-reported rather than objectively measured. Much of the curriculum focused on ethical issues and communication, domains of dynamic knowledge that are best evaluated with simulation and skill evaluation; however, these resource-intensive methods were beyond the budget or scope of this pilot study. Moreover, as of this writing, PAD is not yet accessible in our state, meaning that objective measurement using real patients was not a realistic goal. Other limitations to this study include lack of ability to assess individual-level changes since the surveys were anonymous. Additionally, a small sample size from a single academic institution limits its generalizability to other HPM fellowship programs with different trainee demographics, institutional cultures, or legal contexts. Finally, the study only evaluated short-term outcomes; whether improvements in comfort translate into sustained knowledge, clinical competence, or improved patient communication remains unknown.
Despite the limitations, we believe that this study represents an important first step in the HPM field in preparing clinicians to be able to thoughtfully and compassionately respond to inquiries or requests for hastened death, no matter one’s personal ideological stance. While responding to suffering and unmet needs of dying patients is already a part of HPM fellowship curricula, the changing legal paradigm around PAD now requires foundational knowledge of ethical, legal, and clinical considerations, as well as PAD-specific communication skills. This holds true for HPM programs in states where the practice is still illegal (such as ours when this curriculum was made), since patients may still inquire about it, and since fellows may become attendings in states where the practice is legal. This feasible pilot curriculum can serve as a model for other HPM training programs to build upon. Future directions should include a larger sample size with diverse HPM programs from various geographical locations and development of an Objective Structured Clinical Examination to objectively measure fellows’ competencies in developing these important skills.
Ethical Considerations
This educational study was deemed exempt by the Mount Sinai Institutional Review Board.
Consent to Participate
All participating fellows provided written informed consent prior to the pre- and postcurriculum evaluation surveys. The language of these consent forms was approved by the Mount Sinai Institutional Review Board.
Data Availability
The small amount of data from this pilot educational study is not publicly available.
Authors’ Contributions
A.E. and L.B. contributed to study conception and design, data collection, data analysis, and drafting and revisions of the article. J.C., M.K., and R.M.A. contributed to study conception and design, data collection, and revisions of the article. E.M., M.A.B., and A.B. contributed to study conception and design and revisions of the article.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was provided for this project.
Conflict of Interest
R.M.A. reports royalties from UpToDate and serving on the Board of UpToDate.