
Abstract
Objectives:
To provide detailed characteristics of advanced malignant bone and soft tissue tumors at the end of life.
Design:
A retrospective case series analysis.
Subject:
We included 24 patients who presented to our department between 2014 and 2024, were diagnosed with malignant bone or soft tissue tumors, and died from tumor-related causes.
Results:
The mean age was 57.8 ± 15.6 years at death. Acute-onset events requiring emergency admission within three months before death occurred in 91.7%. The reasons for emergency admission included dyspnea due to malignant pleural effusion, sepsis, paraplegia, gastrointestinal bleeding, bone marrow dysfunction, difficulty moving due to pain, acute renal failure, and pulmonary thromboembolism.
Conclusions:
Patients with advanced sarcoma experience an exceptionally high rate of acute-onset events and emergency admissions in their final months. Emergency hospitalization provides an opportunity to consider transitioning to palliative care.
Key Message
In the terminal stages of bone and soft tissue sarcomas, emergency hospitalization provides an opportunity to consider transitioning to palliative care.
Introduction
The clinical course of advanced malignant bone and soft tissue tumors at the end of life remains insufficiently characterized. The overall condition of patients with malignant tumors remains relatively stable for an extended period, followed by rapid deterioration in the final one to two months before death. 1 Elucidating the clinical course of end-of-life care is crucial for determining whether the attending physician should continue aggressive treatment or consider hospice or palliative care; it is also important for patients and their families to decide how to spend this remaining time.
The objective of this study was to provide an exploratory and detailed characterization of the terminal clinical manifestations and imaging findings in patients with advanced bone and soft tissue sarcoma. Malignant bone and soft tissue tumors are rare mesenchymal malignancies, accounting for only 1% of adult malignant tumors; while existing international prognostic indicators—such as the palliative prognostic score and palliative prognostic index—are valuable, they rarely include or reflect the unique clinical courses of malignant bone and soft tissue tumors.2–4 Therefore, characterizing the descriptive trajectory of these patients at the end of life is essential.
Bone and soft tissue sarcomas most commonly metastasize to the lungs, and pulmonary metastasis is considered one of the most important prognostic factors. 5 Previous studies have demonstrated that the number and size of pulmonary metastases, as well as the disease-free interval before their development, are strongly associated with survival outcomes. 6 At our institution, chest computed tomography (CT) scans are routinely performed every three months for patients with advanced malignant bone and soft tissue tumors, which enabled consistent imaging data collection. The strength of our report lies in the detailed description of the terminal course in a sarcoma-specific cohort, including imaging findings and clinical findings.
Patients and Methods
Twenty-four patients with malignant bone and soft tissue tumors who visited our department between 2014 and 2024 died of disease (DOD) by December 2024. To ensure data integrity and minimize selection bias arising from attrition in the elderly, we restricted our analysis to patients under 80 years of age. This demographic often experienced loss to follow-up due to hospitalizations at external institutions for comorbidities unrelated to sarcoma or general age-related difficulties in maintaining clinical visits.
We retrospectively examined the following items based on electronic medical record data and reports from transferring institutions: place of death (hospice, home palliative, palliative care unit, or acute care unit), time from full transition to palliative care (hospice admission or full transition to home palliative care) to death, whether the patient had a history of emergency admission to our acute care ward within three months of death, and the reason for such admission.
The presence or absence of lung metastases was discerned by simple chest CT, lung metastases in ≥10 locations, pleural effusion >1 cm on CT (unilateral or bilateral), or paraplegia, and the durations from their appearance until death were recorded. Because bone and soft tissue sarcomas most frequently metastasize to the lungs, and pulmonary metastasis has been reported as one of the most important prognostic factors, 5 chest CT scans are routinely performed every three months at our institution for patients with advanced malignant bone and soft tissue tumors. Paraplegia was also recorded because of its association with spinal cord compression and rapid functional decline. Because of the limited number of cases and incomplete imaging data, metastases at sites other than the lungs were not included in this study. Performance status data were not consistently documented in a standardized format at the relevant time points in the medical records; therefore, they could not be reliably included in the analysis.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Hamamatsu University School of Medicine on April 27, 2026 (approval number: 26-067). Due to the retrospective nature of this study, the requirement for individual informed consent was waived by the IRB. Instead, the opportunity to opt out was provided through our hospital’s website.
Results
The study included 24 patients (15 males and nine females) with a mean age of 55.5 ± 16.4 (range: 24–77) years at initial presentation and a mean age of 57.8 ± 15.6 (range: 28–78) years at death. The primary tumors were malignant bone tumors in 10 patients (Ewing sarcoma: four, chondrosarcoma: three, chordoma: one, osteosarcoma: one, and leiomyosarcoma: (1) and malignant soft tissue tumors in 14 (five undifferentiated pleomorphic sarcomas, three dedifferentiated liposarcomas, two leiomyosarcomas, one epithelioid sarcoma, one myxofibrosarcoma, one radiation-induced sarcoma, and one unclassifiable sarcoma). The place of death was hospice care in 12 cases (50%), home palliative care in eight (33%), palliative care unit in one (4%), and our hospital’s acute care unit in three (12.5%). The average number of days from complete transition from palliative care (admission to hospice or home palliative care) to death was 25.5 days (median: 22; range: 3–69 days) (Table 1).
Patient Characteristics
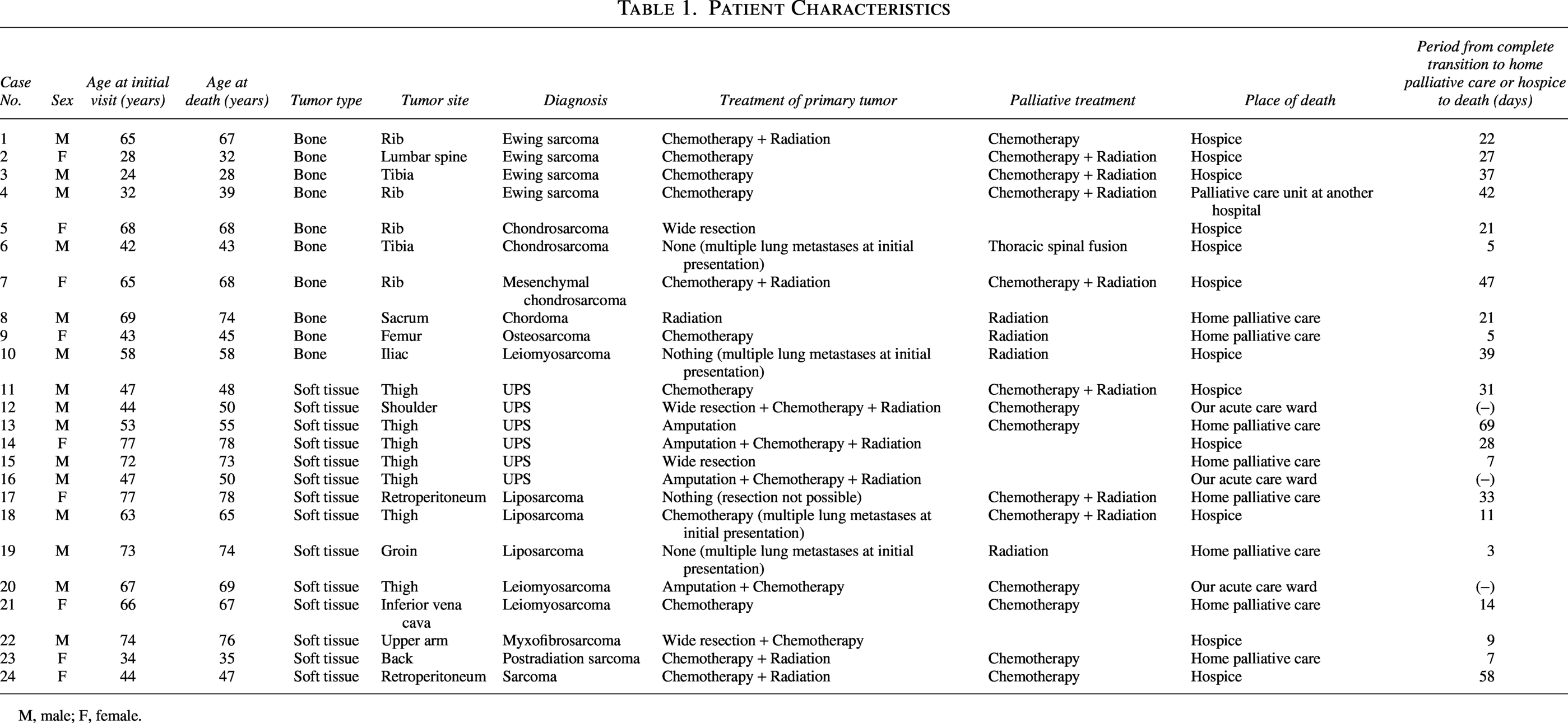
M, male; F, female.
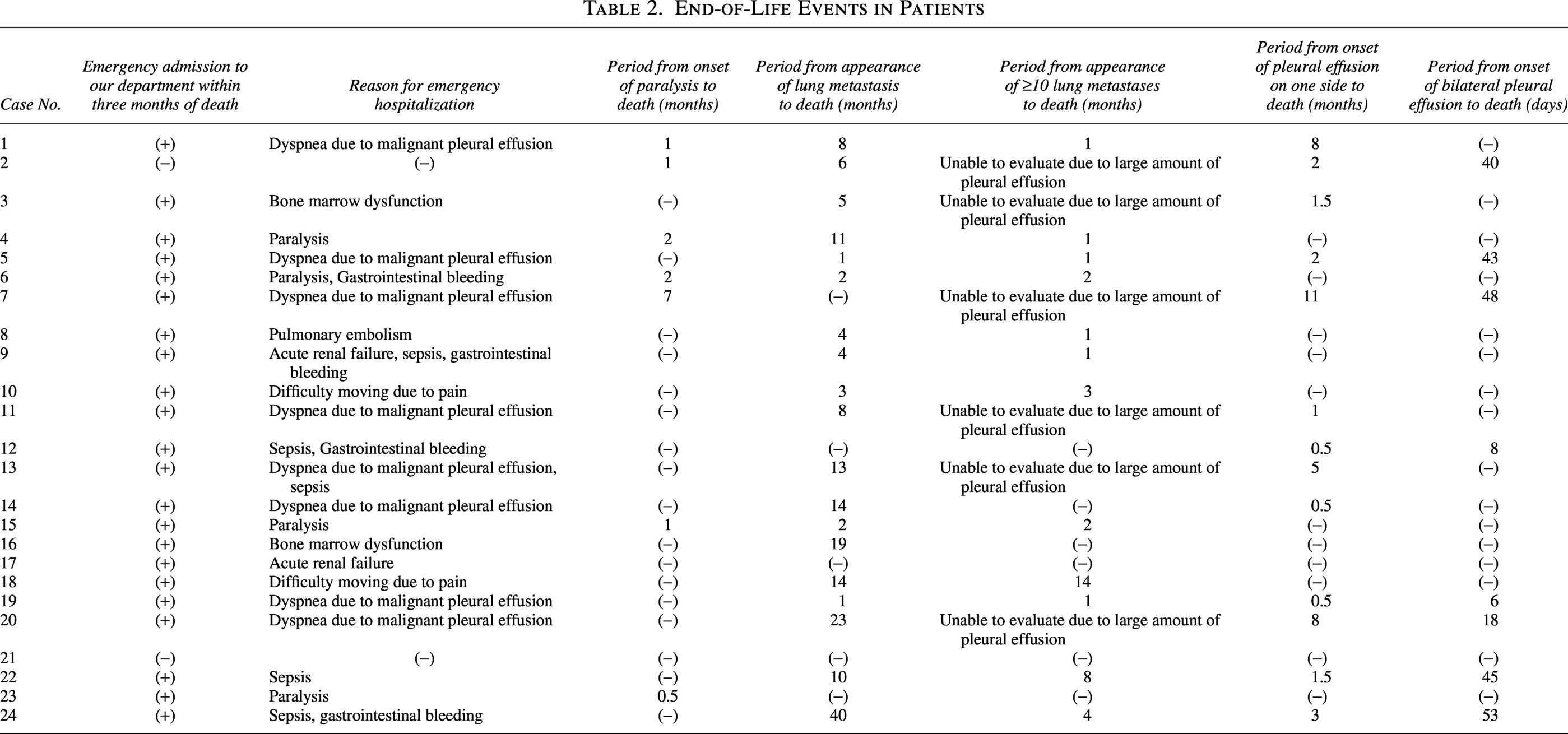
Among the 24 patients, 22 (91.7%) had a history of emergency admission to our acute care ward within three months of death. The reasons for emergency admission included dyspnea due to malignant pleural effusion (eight), sepsis (five), paraplegia (four), gastrointestinal bleeding (four), bone marrow dysfunction (two), difficulty moving due to pain (two), acute renal failure (two), and pulmonary thromboembolism (one) (Table 2 and Fig. 1).
End-of-Life Events in Patients
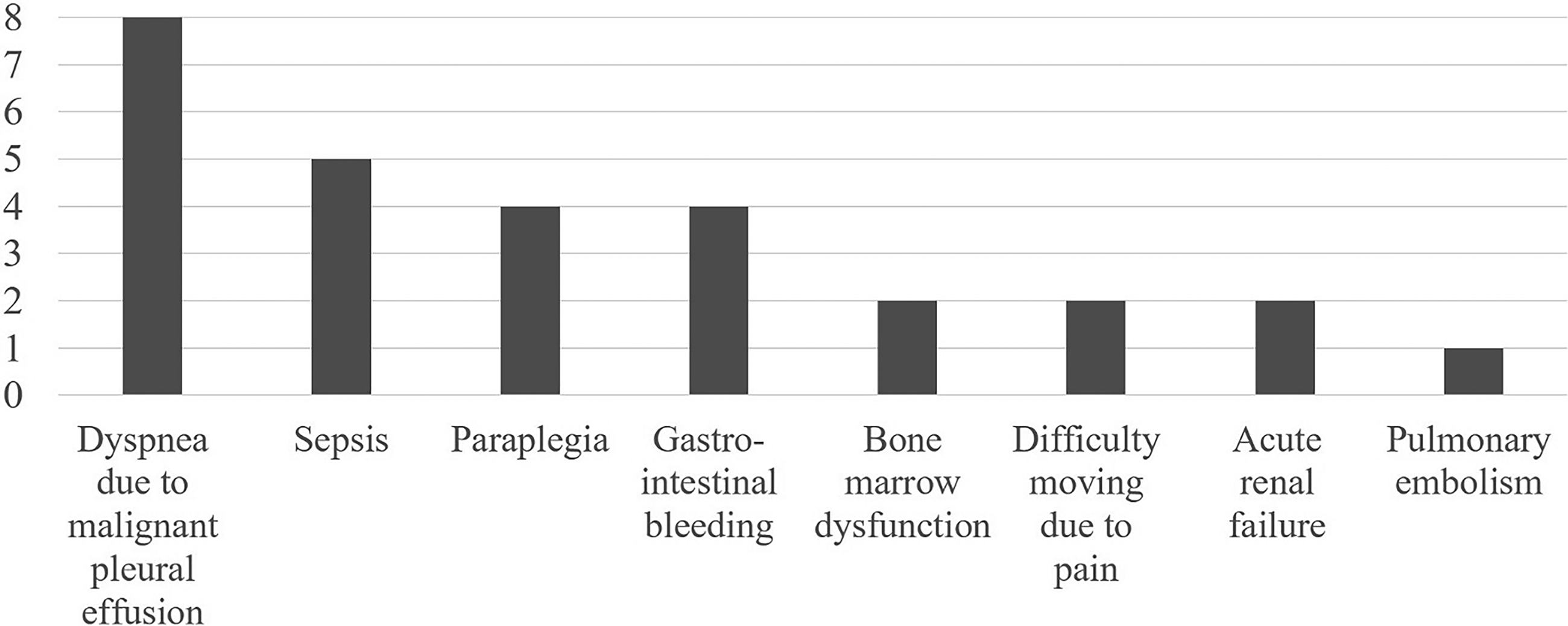
Reasons for emergency hospitalization within three months of death.
At death, 19/24 patients (79.2%) had lung metastases detectable on chest CT, with an average of 9.9 (median: 8; range: 1–40) months from lung metastases diagnosis to death. Six cases were unevaluable due to massive pleural effusion, but at least 12 cases (50%) had ≥10 pulmonary metastases; the average survival time from the appearance of ≥10 pulmonary metastases to death was 3.25 (median: 1.5, range: 1–14) months. Unilateral pleural effusion measuring ≥1 cm on chest CT was present in 13/24 cases (54.2%), with an average of 3.4 (median: 2, range: 0.5–8) months from onset to death; bilateral pleural effusion was present in eight cases (33%), with an average of 32.6 (median: 41.5, range: 6–53) days from onset to death. Paraplegia was present in seven cases (29.2%), with an average of 2.1 (median: 1, range: 0.5–7 months) from onset to death; causes were spinal metastasis with intraspinal progression in 4 cases, spinal cord metastasis in 1, and direct infiltration of the spinal canal by a primary tumor of the ribs in 2 (Tables 2 and 3).
Period from the Occurrence of End-of-Life Events to Death
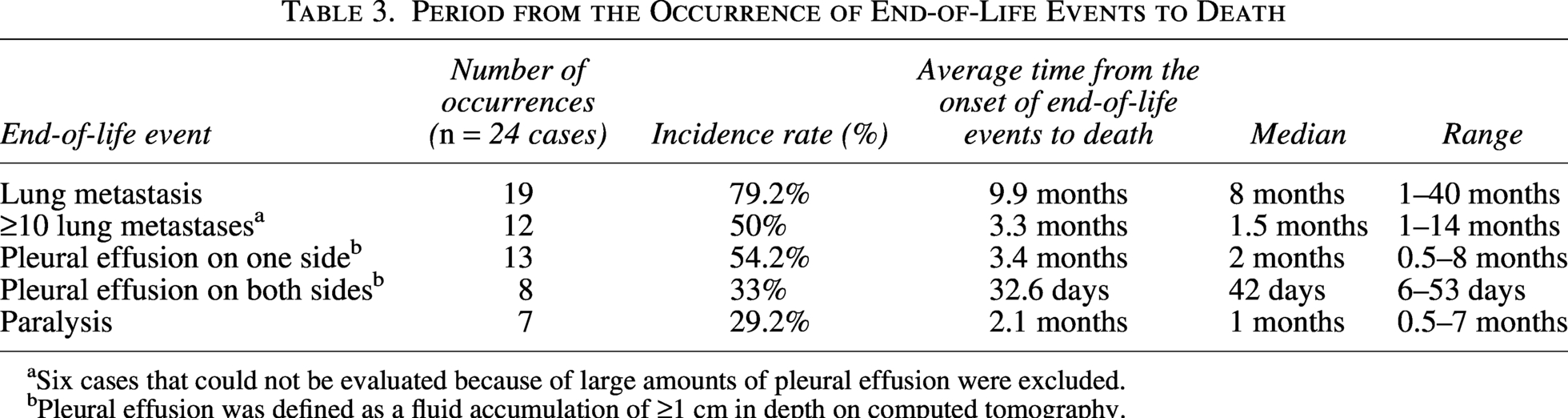
Six cases that could not be evaluated because of large amounts of pleural effusion were excluded.
Pleural effusion was defined as a fluid accumulation of ≥1 cm in depth on computed tomography.
Discussion
Reports on the clinical presentation of advanced malignant bone and soft tissue tumors in the terminal stages are limited. In these stages, issues such as dyspnea and pain arise, and the necessity and importance of specialized end-of-life palliative care, including hospice and home-based palliative care, are high.7–9 Kawashima reported that in the final 2 weeks of life, pain was present in 93% of patients with advanced musculoskeletal sarcomas and dyspnea in 78%, with 98% requiring opioid use, 83% receiving corticosteroids for dyspnea relief, and 39% undergoing sedation for uncontrollable refractory symptoms. This emphasizes the importance of palliative care, with palliative sedation and active symptom management being essential. 8 Brandes reported that in the terminal stage of advanced malignant bone and soft tissue tumors, specialized palliative care interventions significantly reduced pain and distress levels. 9 However, McMahon reported that only 2.8% of 7,498 patients with osteosarcoma received palliative care, indicating a low utilization rate for bone and soft tissue tumors. 10
In the present study, 22/24 cases (91.7%) had a history of emergency admission to our acute care ward within three months of death, with the reasons for emergency admission including dyspnea due to malignant pleural effusion, paraplegia, sepsis, gastrointestinal bleeding, bone marrow dysfunction, difficulty moving due to pain, acute renal failure, and pulmonary thromboembolism. To cope with the total suffering associated with sudden changes in condition, such as dyspnea, pain, and paraplegia, specialized end-of-life palliative care is considered essential in the terminal care of patients with malignant bone and soft tissue tumors.
Specialized end-of-life palliative care is available in hospices and home-based palliative care facilities. Using these services during the terminal phase of malignant tumors is important for symptom relief, better pain management, patient and caregiver satisfaction, and reduction of medical costs.11–13 To fully benefit from symptom management and end-of-life care, a timely referral is preferable.13–15 Earle reported that only 23.3% of patients with terminal malignant tumors received hospice care, and 14.3% of all hospice inpatients died within three days of hospice admission, highlighting the need for more appropriate referrals to ensure that patients receive the full benefits of hospice care. 15 Shepperd reported that within one month of end-of-life home palliative care intervention, patients receiving home palliative care had higher patient and caregiver satisfaction than those receiving hospital care (odds ratio: 3.37); however, in cases where patients survived for 30–60 days or longer, patient anxiety increased and caregiver well-being decreased. 13 Timely referral to hospice or home palliative care for end-of-life palliative care is important.
In this report, in 91.7% of the cases of advanced bone and soft tissue tumors that DOD, emergency admission to an acute care ward was required within three months of death due to an acute-onset event. However, 83% of patients transitioned to hospice or home palliative care during the terminal phase, and the number of days from complete transition to palliative care (hospice admission or complete transition to home palliative care) to death was 25.5 days on average (median: 22, range: 3–69 days); this indicates that transition to end-of-life palliative care was achieved at an appropriate time. In patients with advanced malignant bone and soft tissue tumors admitted to an acute care hospital because of an acute event, there may be an opportunity to consider the timing of the transition to end-of-life palliative care.
Although our descriptive findings indicate that the presence of ≥10 lung metastases, pleural effusion on one or both sides, or paraplegia may be associated with life expectancy measured in months; these observations should be treated as exploratory markers of the transition to end-of-life palliative care rather than strict prognostic criteria. Nevertheless, recognizing these common radiological and clinical milestones can help clinicians anticipate impending complications, facilitate timely referrals to hospice or home-based palliative care, and ultimately improve the quality of end-of-life care for this patient population.
The strength of our report lies in the detailed description of the terminal course in a sarcoma-specific cohort, including the timing of hospice initiation and the correlation between imaging findings and clinical findings, which has been relatively underreported to date. However, this study has several limitations that should be acknowledged. First, the small sample size, owing to the rarity of malignant bone and soft tissue tumors and to the retrospective single-center design, limits statistical power. Second, the retrospective single-center design introduces the possibility of selection bias. Patient inclusion may have been influenced by institutional referral patterns, follow-up practices, or documentation variability, which could limit the generalizability of the findings to broader sarcoma populations. Third, there is overlap between our observations and prior observational studies that have described short-term prognostic factors in advanced or metastatic sarcoma. Although our study provides detailed descriptive data regarding end-of-life clinical trajectories findings, it may not substantially extend existing knowledge beyond what has already been reported. Therefore, our findings should be considered exploratory and hypothesis-generating rather than definitive. Future studies with larger, multicenter cohorts and prospective designs are warranted to validate and expand upon these observations.
Conclusion
In conclusion, this descriptive case series demonstrates that the terminal stage of malignant bone and soft tissue tumors is characterized by an exceptionally high rate of acute-onset events (91.7%) requiring emergency hospitalization, driven by complications such as dyspnea, paraplegia, and sepsis. The late-stage trajectory is also characterized by specific radiological and clinical findings, including extensive lung metastases, pleural effusions, and spinal cord compression. Because these acute events are highly prevalent and unpredictable, proactive advance care planning is essential to optimize palliative and end-of-life care for sarcoma patients.
Footnotes
Availability of Data and Materials
Data supporting the results of the present study are available from the corresponding author upon request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funds, grants, or other support were received.