
Abstract
Background/Objectives:
Injectable opioid use in home palliative care requires multiprofessional coordination, but regional implementation data are limited. We conducted a pilot survey to describe experience, task sharing, difficulties, and future willingness.
Methods:
We performed an anonymous web-based cross-sectional survey of multidisciplinary professionals involved in community-based palliative care in a Japanese regional health care area.
Results:
Among 159 respondents, 117 (73.6%) had prior opioid experience for cancer pain, and 73/117 (62.4%) had prior injectable opioid experience. Initiation was mainly attributed to hospital physicians, maintenance dose management to hospital and clinic/home care physicians, and solution or cassette exchange to nurses. Difficulties when starting or modifying injectable opioids were reported by 27/73 respondents (37.0%). Future willingness was higher with prior experience (41/72, 56.9%) than without prior experience (7/83, 8.4%).
Conclusion:
This pilot survey suggests that home injectable opioid practice is a multidisciplinary workflow with an experience-related readiness gap, supporting broader regional evaluation and implementation-focused support.
Keywords
Introduction
Injectable opioids given by continuous intravenous or subcutaneous infusion may be needed in community-based palliative care, especially in late-stage or end-of-life care when oral administration is not feasible, absorption is unreliable, or rapid symptom control is required. Here, “palliative care” denotes the broader setting, whereas late-stage palliative care or end-of-life care denotes situations in which parenteral opioids are considered. Continuous subcutaneous infusion has long been used for cancer pain, including in home care.1,2
In Japan, home parenteral opioid practice is generally organized around continuous infusion rather than routine intermittent injection, although this pilot survey did not evaluate national practice. Injectable opioid use requires coordination across the hospital-to-home transition, including opioid selection, dose conversion, maintenance adjustment, medication supply, infusion device handling, and communication among hospital physicians, clinic/home care physicians, nurses, and pharmacists. Prior studies suggest that continuity across settings, access to medicines and equipment, and standardized prescribing or infusion processes may influence the safety and timeliness of injectable medication use at home in late-stage palliative care and end-of-life care.3–6
Data on interprofessional role distribution within a local health care area and barriers remain limited. This pilot survey was part of a stepwise national project led by the Safety and Infection Committee of the Japanese Society for Palliative Medicine. Injectable opioid dilution had been identified in preceding project work as a background issue for later protocol development and standardization, but it was not a structured survey domain here. We, therefore, surveyed multidisciplinary professionals involved in community-based palliative care in one Japanese regional health care area to describe prior injectable opioid experience, task sharing, perceived operational difficulties, and future willingness.
Methods
Study design, setting, and participants
We conducted a cross-sectional web-based survey in a regional health care area in Japan. The area served approximately 260,000 residents and included a core hospital linked to regional clinics, visiting nursing services, pharmacies, and other community resources. The survey targeted professionals involved in the hospital-to-home transition or community support for patients with advanced cancer, including physicians, visiting nurses, community/dispensing pharmacists, care managers, hospital nurses, hospital physicians, hospital pharmacists, and dentists. These groups were included because home injectable opioid use in this setting depends on linked hospital-to-home support. Hospital-based professionals often contribute to transition planning and prescribing coordination, whereas community-based professionals provide ongoing care, and care managers and dentists may contribute to coordination or support.
Data collection and survey instrument
An anonymous questionnaire was developed in Google Forms and administered from October to December 2025 among health care professionals involved in community-based palliative care. The questionnaire was developed through clinical discussion and committee consensus; face validity was reviewed by regional clinicians, but formal psychometric validation was not performed. The survey link was disseminated through overlapping local professional networks and mailing routes; therefore, the invited denominator and response rate could not be determined reliably. The instrument covered respondent characteristics, professional role, prior opioid and injectable opioid experience, route-specific experience, reported responsibility for initiation, maintenance dose management, and solution or cassette exchange, operational barriers, written order formats, future willingness, and optional free-text comments. Injectable opioid dilution was not a structured survey domain, although it had been identified in preceding project work and could appear in free-text comments.
Ethical considerations
This anonymous questionnaire survey targeted health care and care professionals, involved no patients, and collected no identifiable or sensitive information. Under institutional policy at the University of Toyama, this type of anonymous health care professional survey for practice assessment and implementation planning did not require formal ethics committee review; therefore, no approval number was issued. Participation was voluntary, and completion of the anonymous web-based questionnaire was regarded as implied informed consent to participate.
Statistical analysis
Analyses were descriptive, with categorical variables summarized as frequencies and percentages; no inferential statistics were performed.
Results
Respondent characteristics are summarized in Table 1. Among 159 respondents, 92 (57.9%) were from Takaoka City, 54 (34.0%) were from Imizu City, and 13 (8.2%) were from Himi City. The largest professional groups were 52 community/dispensing pharmacists (32.7%), 49 care managers (30.8%), 17 visiting nurses (10.7%), and 16 clinic/home care physicians (10.1%). Prior opioid experience for cancer pain was reported by 117 respondents (73.6%); among them, 73 (62.4%) had prior injectable opioid experience. One respondent did not answer the route question. Route-specific analyses were, therefore, based on 72 respondents: Continuous intravenous only, 26 (36.1%); continuous subcutaneous only, 17 (23.6%); and both routes, 29 (40.3%).
Respondent Characteristics and Prior Experience
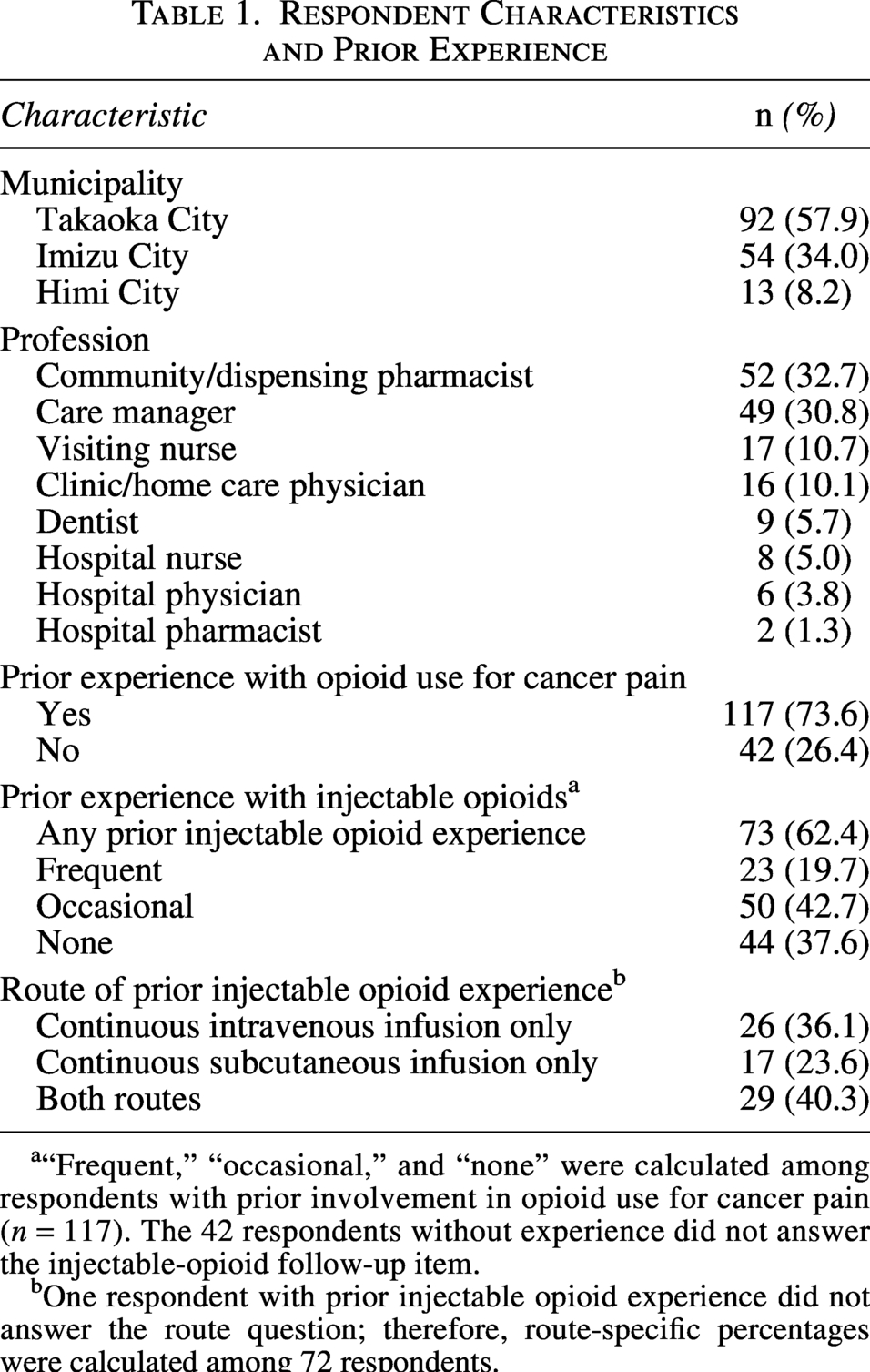
“Frequent,” “occasional,” and “none” were calculated among respondents with prior involvement in opioid use for cancer pain (n = 117). The 42 respondents without experience did not answer the injectable-opioid follow-up item.
One respondent with prior injectable opioid experience did not answer the route question; therefore, route-specific percentages were calculated among 72 respondents.
Among respondents with prior injectable opioid experience (n = 73), 50 (68.5%) attributed initiation to hospital physicians and 15 (20.5%) to clinic/home care physicians. Maintenance dose management was attributed to hospital physicians by 29 (39.7%), clinic/home care physicians by 25 (34.2%), nurses by 13 (17.8%), pharmacists by 4 (5.5%), and other roles by 2 (2.7%). One respondent did not answer the solution/cassette exchange item. Among the remaining 72 respondents, 49 (68.1%) reported nurses and 14 (19.4%) pharmacists as most likely to perform solution/cassette exchange. Future willingness and task sharing are shown in Table 2.
Future Willingness and Reported Task Sharing
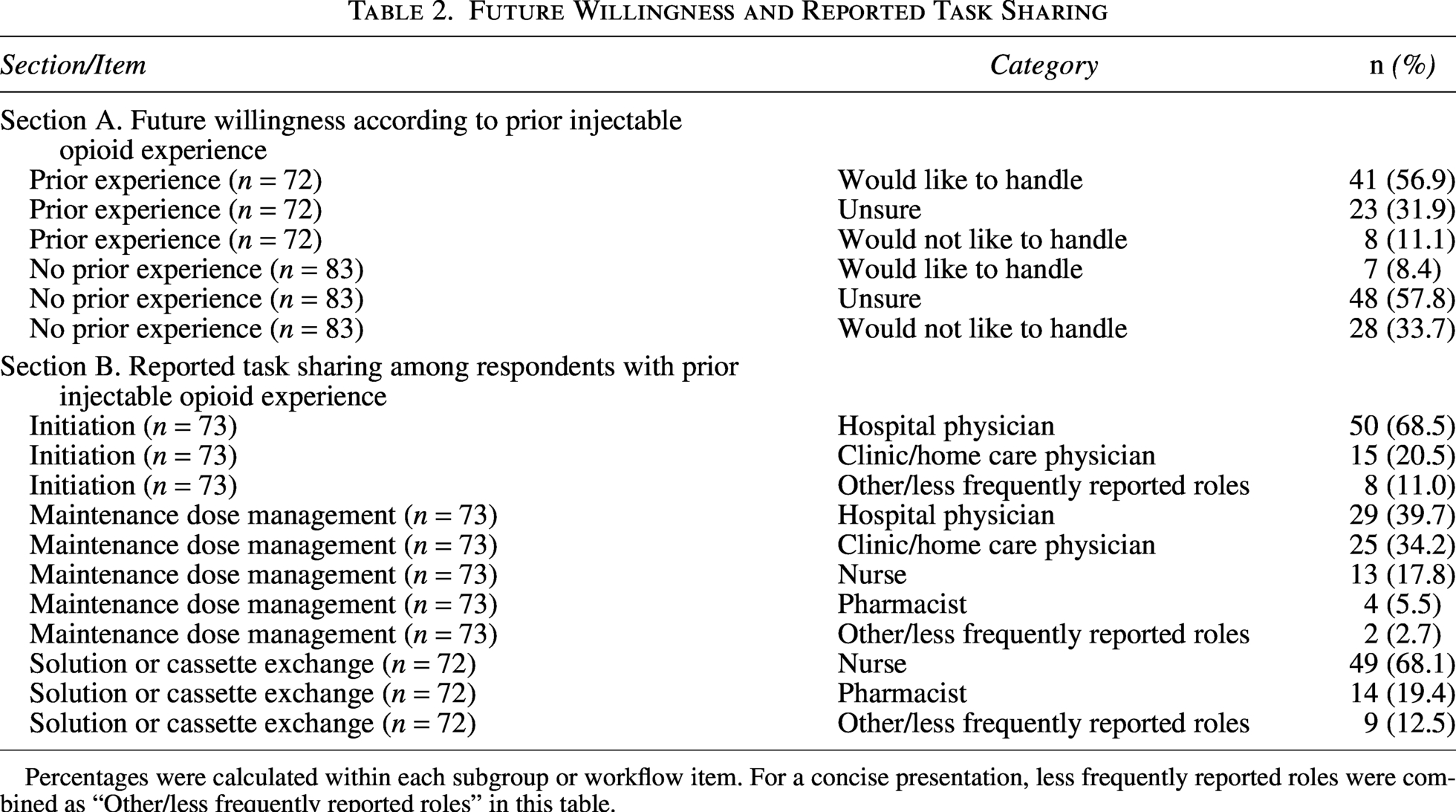
Percentages were calculated within each subgroup or workflow item. For a concise presentation, less frequently reported roles were combined as “Other/less frequently reported roles” in this table.
Difficulties when starting or modifying injectable opioids were reported by 27/73 respondents (37.0%). Free-text responses most often referred to opioid selection, dose conversion, infusion device or line handling, medication stock and aseptic compounding, and after-hours communication or role coordination. Incident narratives also described pump or route alarms, dilution or dose errors, and medication availability constraints. Preferences for written orders were dispersed across templates, with the most common format selected by 55/144 respondents (38.2%).
Future willingness remained limited overall: 48/155 respondents (31.0%) would like future involvement, 71 (45.8%) were unsure, and 36 (23.2%) would not. Willingness was higher among respondents with prior injectable opioid experience (41/72, 56.9%) than among those without prior experience (7/83, 8.4%); uncertainty predominated in the latter group (48/83, 57.8%).
Discussion
In this pilot survey, respondent-reported task distribution for home injectable opioid use in community-based palliative care, particularly in late-stage or end-of-life care, was consistent with a multidisciplinary workflow rather than a single-profession task. Among respondents with prior experience, initiation was mainly attributed to hospital physicians, whereas maintenance dose management was shared between hospital and clinic/home care physicians, with additional input from nurses and pharmacists. Solution or cassette exchange was mainly attributed to nurses, and future willingness differed markedly by prior experience. These findings describe perceived role distribution and an experience-related readiness gap, not the effectiveness of any regional process. Hospital teams and community providers appeared to function as linked systems. Hospital clinicians commonly contributed to transition planning and early prescribing decisions, whereas ongoing home care was delivered by clinic/home care physicians, visiting nurses, community pharmacists, care managers, and other local providers. In Japan, nurses do not have independent opioid prescribing authority, which may help explain why prescribing-related tasks remained physician-centered while operational tasks were more often attributed to nurses.
These patterns are clinically plausible. Prior work has shown that continuity across settings, access to medicines and equipment, and communication between prescribers and community teams are central to injectable medication use in community-based palliative care.3,4 Qualitative studies have similarly described physicians retaining prescribing responsibility while relying on nurses for ongoing assessment and administration-related decisions in late-stage palliative care and end-of-life care at home.7,8 Our findings suggest that limited experience may constrain perceived readiness psychologically and practically, including in dose design, solution exchange, device handling, medication supply, and after-hours coordination. Community pharmacists may also experience opioid management as both important and burdensome in community-based palliative care. 9 Although preceding work in the same project identified heterogeneity in opioid infusion dilution practices as a background issue for later protocol development, dilution was not a structured survey domain here. Respondents instead highlighted implementation needs, including shared workflows, written order formats, cross-setting communication, and regionally understood operating rules. Standardized written order templates, communication support, multiprofessional simulation or joint training, and regionally shared operating rules are reasonable future targets, although their effectiveness was not evaluated in this survey.5,6
This single-region pilot survey was a convenience sample with possible response bias. Because it was disseminated through overlapping local professional networks as an open web-based questionnaire, a strict denominator and formal response rate could not be established, and respondents with greater interest in or prior experience with home injectable opioid management may have been more likely to participate. The data were self-reported and reflect perceived roles and difficulties rather than independently verified practice. Home injectable opioid use is a high-risk intervention, yet this survey did not evaluate patient safety outcomes, adverse events, symptom control, or clinical effectiveness. The survey also did not capture whether respondents’ experiences related mainly to opioid-naïve patients newly started on injectable opioids or to opioid-tolerant patients already maintained on injectable opioids; this clinical context may have influenced the types of difficulties perceived by different professionals. Responses may also have been shaped by local service configuration, referral pathways, and professional mix. Future multisite studies should incorporate patient-centered and safety outcomes. Accordingly, generalization beyond similar settings should be cautious.
In summary, this pilot survey describes respondent-reported role distribution and an experience-related readiness gap for home injectable opioid use in one Japanese regional health care area. These findings support broader evaluation and may inform future work on shared protocols, communication, and multiprofessional training; patient-centered and safety outcomes should be assessed in subsequent studies.
Authors’ Contributions
Shinya K. and T.H. conceived the study. T.H. curated data. T.H., M.H., Shiro K., and N.M. contributed to data acquisition and interpretation. Shinya K. performed the analyses and drafted the article. R.H. critically revised the article. All authors have read and approved the final version of the article.
Ethics Review and Consent
This anonymous questionnaire survey of health care and care professionals in a regional health care area did not involve patients and did not collect personally identifiable or sensitive information. According to the policy of the Research Ethics Office for Human Subjects at the University of Toyama, formal ethics review was not required for this type of anonymous health care professional survey; therefore, no approval number was issued.
Data Availability
The de-identified dataset supporting the findings of this study is stored on secure institutional servers and is not publicly available due to concerns regarding participant confidentiality and institutional policies. Additional data may be shared by the corresponding author upon reasonable request, pending institutional approval and data-sharing agreements.
Declaration of Generative AI
During the preparation of this article, the authors used ChatGPT (Open artificial intelligence (AI) as an AI-assisted tool to improve language and readability. After using this tool, the authors reviewed and edited the content as required. The authors have full responsibility for the content of the published article.
Footnotes
Acknowledgments
The authors would like to thank all health care staff in the Takaoka region for their participation in this survey.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This work was supported in part by a research grant from the Kobayashi Cancer Research Foundation of Japan.