
Abstract
Background:
Pain is a common symptom for children and adolescents with treatment-refractory cancers at the end of life (EoL). Palliative radiotherapy (RT) is a noninvasive, outpatient therapy with an acceptable safety profile that helps to mitigate physical pain. It has been proven as an essential treatment modality for symptom control at EoL in the adult population. While the efficacy of palliative RT is well-established in adults, evidence in the pediatric population remains limited. This systematic review aimed to identify and evaluate the current evidence on palliative RT for the treatment of cancer pain in children and adolescents.
Five databases were searched for pediatric empirical quantitative studies. Inclusion criteria include children and adolescents aged ≤21 years old with terminal cancer who received palliative RT for pain relief, single- or multicenter studies with ≥10 cases published in English. The primary outcome was pain control postpalliative RT, and secondary outcomes included reduction in opioid usage.
Results:
Seven observational retrospective studies (n = 63 patients/235 metastatic sites/139 palliative RT courses), published between 2003 and 2024, were included. Palliative RT was associated with a 77.9% (95% confidence interval [CI] 71.2–84.6, p = 0.4) reduction in pain when used as an adjuvant therapy across all seven studies. A reduction in opioid use was observed in 43.2% (95% CI 31.8–54.7, p = 0.4) across two studies (n = 52 patients/17 palliative RT courses). These were not statistically significant results. The subgroup analysis showed that it was associated with 80.0% (95% CI 69.9–90.1, p = 0.9) reduction of pain in patients with bony lesions across two studies (n = 19 metastatic sites/41 courses).
Conclusion:
While our meta-analysis does not provide sufficient evidence to show that palliative RT reduced pain in children and adolescents with terminal cancer, it adds to the growing body of evidence supporting integrated approaches to symptom control in pediatric oncology. Further research is needed to substantiate its clinical benefits in augmenting and facilitating optimal EoL care in children and adolescents with advanced malignancies.
Introduction
A diagnosis of terminal illness in a child is profoundly distressing for families worldwide, with childhood cancer remaining a leading cause of death among children and adolescents.1,2 Despite therapeutic advances, significant global disparities persist, with five-year survival rates as low as 40% in low- and middle-income countries and an estimated 11.1 million children and adolescents projected to die from cancer over the next three decades.3,4 Consequently, pediatric palliative care has become an essential component of oncology care, addressing the substantial symptom burden experienced by children and adolescents with life-limiting malignancies.5,6
Pain is the most common and distressing symptom encountered in pediatric oncology patients, particularly at the end of life (EoL).7–9 It is often multifactorial, arising from tumor progression, metastatic disease, and treatment-related effects, and is best understood within the framework of “total pain,” encompassing physical, emotional, social, and spiritual dimensions.10,11 Up to 70% of children and adolescents with advanced cancer experience significant pain alongside other debilitating symptoms, underscoring the need for effective symptom control strategies. 12 Despite an expanding armamentarium of multimodal analgesia, including opioids, adjuvant medications, and supportive therapies, inadequate pain control continues to be reported due to systemic, clinical, and logistical barriers.5,7,13
Palliative radiotherapy (RT) has been widely utilized in adult oncology as an effective modality for pain relief, particularly in cases of bone and soft tissue metastases. 14 Its mechanism of targeting malignant cells to reduce tumor burden can alleviate pain both directly and indirectly by relieving mass effect and associated complications. 12 The median time to pain relief in metastatic disease is approximately one to four weeks. 15 Hypofractionation regimens comprising single, short but high dose regimens are deemed particularly effective in painful metastatic disease. 16 There can be a temporary worsening of symptoms, commonly due to pain flares, after palliative RT. 17 Adjuvant chemotherapy is usually avoided when administering palliative RT due to possible toxicity potentiation. 18 In pediatric populations, RT has similarly been described as a potentially valuable adjunct to pharmacological analgesia, with reported benefits including pain reduction, decreased opioid requirements, and improved quality of life.19,20 However, its integration into pediatric palliative care remains inconsistent and underutilized, as it has not been as well studied as in the adult population. 21
The use of palliative RT in children and adolescents is challenged by several factors, including concerns regarding acute and long-term toxicity, the need for general anesthesia in younger patients, logistical complexities, and variability in clinician practice.22–24 Additionally, utilization rates remain low, ranging from 1% to 28% across institutions, reflecting uncertainty regarding its role and effectiveness in this population. 9 Importantly, current clinical practice is largely extrapolated from adult data, as pediatric-specific evidence remains limited and heterogeneous. 25
A major limitation in the field is the lack of high-quality, synthesized evidence evaluating the efficacy of palliative RT specifically for pain control in pediatric oncology patients. Existing studies are predominantly retrospective, with small sample sizes and variable outcome measures, making it difficult to draw definitive conclusions or establish standardized treatment protocols.20,22 Furthermore, no validated, evidence-based guidelines currently exist to inform the use of palliative RT as an adjuvant therapy for pain management in children and adolescents at the end of life.
Given these gaps, a systematic review and meta-analysis are warranted to critically evaluate the available evidence on the role of palliative RT as an adjuvant therapy for pain control in pediatric oncology patients. By synthesizing current data on treatment efficacy, outcomes, and associated factors, this study aims to provide a more robust evidence base to guide clinical decision making and optimize palliative care strategies for this vulnerable population.
Methods
This systematic review (SR) and meta-analysis (MA) were registered with PROSPERO (CRD42024494929) and conducted in accordance with the Cochrane Handbook for Systematic Reviews of Interventions and reported following the PRISMA guidelines.26,27
Search strategy and study eligibility
A comprehensive literature search was conducted across five databases (MEDLINE, EMBASE, Web of Science, CINAHL, and the Cochrane Library) from database inception to February 3, 2025. The search strategy was developed in consultation with a medical librarian and incorporated Medical Subject Headings and keywords related to “radiotherapy,” “palliative,” “pediatric,” “cancer,” and “pain.” Searches in MEDLINE and EMBASE were limited to studies involving humans and published in English.
The primary outcome was pain relief following palliative RT, defined as either complete or partial improvement in pain after treatment. Pain relief could be reported using validated assessment tools or subjective evaluations by patients, caregivers, or clinicians. Surrogate markers, including reductions in opioid use, were also accepted as indicators of pain improvement.8,19,20 Patients with stable or worsening pain, or with unchanged or increased opioid requirements, were classified as nonresponders.
Secondary outcomes included time to pain relief, duration of response, changes in opioid consumption, palliative care or hospice involvement, length of hospital or hospice stay, location of death, and mortality. Treatment-related toxicity was assessed using the Radiation Therapy Oncology Group and Common Terminology Criteria for Adverse Events classifications.28,29
Eligible studies included pediatric oncology patients aged 21 years or younger who received palliative RT for pain control at the end of life, with reported pain-related outcomes. Randomized controlled trials (RCT), observational studies, and case series (≥10 patients) were included. Currently, there is no clear definition of the age cutoff for young adults. For example, in the United Kingdom, young adults with palliative care needs were transitioned to adult services even up to 24 years old. 30 While acknowledging variability in international definitions of young adults, 31 21 years old was chosen as the upper age limit in this study, as the age of majority in the corresponding author's country of origin is 21 years old.
Studies were excluded if they included only adult populations or if >20% of participants were aged >21 years, RT given was with curative or salvage intent, included fewer than 10 patients, or were nonprimary research articles (e.g., editorials, conference abstracts, or post hoc analyses). Small case series (<10 patients) were excluded due to concerns regarding internal validity and imprecision. 32
Data extraction and quality assessment
After removal of duplicates, titles and abstracts were screened independently by two reviewers (P.R.R. and M.Y.C.) against predefined eligibility criteria. Full-text articles were subsequently reviewed for inclusion. Discrepancies were resolved through discussion or adjudication by a third reviewer (M.L.).27,33
Extracted data included patient and treatment characteristics (tumor type, anatomical site, indication for RT, RT modality, dose and fractionation, use of anesthesia, and concurrent therapies), as well as clinical outcomes (pain response, pain assessment methods, time to and duration of response, opioid use, palliative care involvement, length of stay, mortality, and treatment-related toxicity). Corresponding authors were contacted to obtain missing or unpublished data where necessary.
As no randomized controlled trials were identified, risk of bias was assessed using the Newcastle–Ottawa Scale for observational studies.34,35 The overall certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.36,37
Data synthesis and analysis
All outcomes were pooled using the DerSimonian–Laird random-effects model. 38 The primary and secondary outcomes were reported as a pooled proportion with a 95% confidence interval (CI). Subgroup analysis was done if there were sufficient studies to support the analysis. An overall pooled result was also reported to determine the impact on pain relief and decreased opioid usage, pooled from patients, metastatic sites, or courses of palliative RT. Heterogeneity was calculated to account for interstudy variability. The risk of bias was mitigated or accounted for in the MA by including the GRADE score.
A funnel plot for pain relief was used to assess publication bias, and a bubble plot was created to establish if there was a trend between better pain outcomes (i.e., a decrease in pain with palliative RT) and more recently published studies as compared to older studies to evaluate the temporal trend of response to palliative RT.
All tests were two-sided; a p value < 0.05 was considered statistically significant. All statistical analyses, including the meta-analysis, were conducted using R version 4.4.0 (2024-04-24 UCRT) with the “meta” package.
Results
Study and patient characteristics
The initial search across the five databases yielded 1468 studies before duplicates were excluded. Seven studies, comprising five cohort studies20,39–42 and two cross-sectional studies8,43 fulfilled the criteria for inclusion in the SR. No RCTs were identified (Fig. 1).
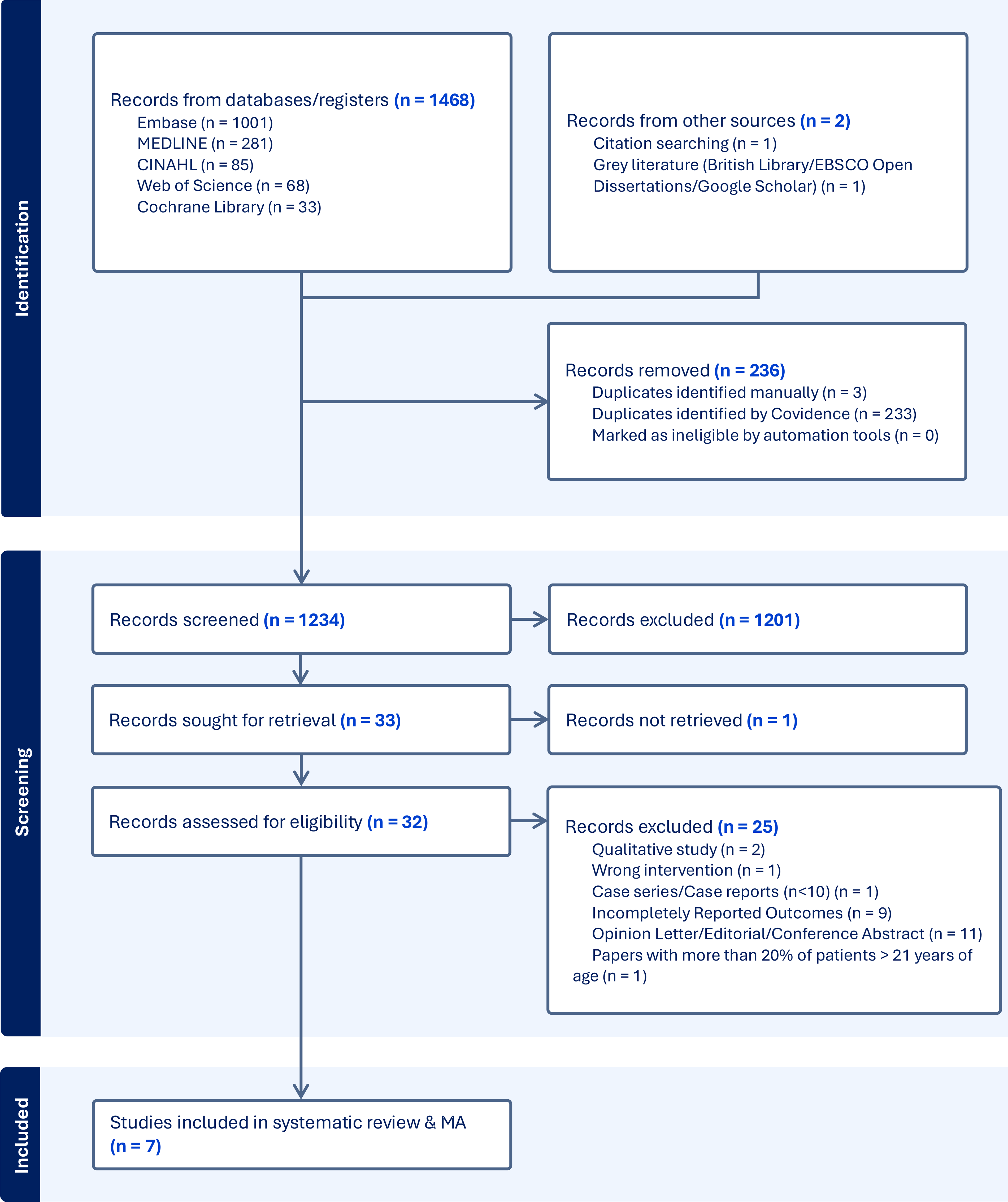
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart for this study.
All studies were retrospective and observational in nature. All studies were conducted in North8,20,39–42 and South America. 43 Four studies20,40,42,43 included patients until 21 years old.
One study 43 described pain control data in terms of the absolute number of patients (n = 63 patients) who received palliative RT for pain control. Three studies20,39,40 described pain control data in terms of the number of metastatic sites (n = 235 sites), which received palliative RT for pain control. Three studies8,41,42 described pain control data in terms of the number of RT courses (n = 139 palliative RT courses) received to achieve pain control.
Three studies8,39,40 focused on patient populations with specific malignancies, while the remainder included patients with various malignancies. The most common malignancies studied, with data available relevant to this study, are osteosarcoma in two studies,8,40 and neuroblastoma in one study. 39 Data on possible confounders, such as adjuvant chemotherapy, were described in two studies20,40 and were also collated.
Bone pain was the most common indication for palliative RT in children and adolescents, as described in three studies,20,39,41 although complete data on pain relief was only available for two studies.39,41 Since there was no standardized dose or fractionation regimen across all studies, only descriptive data of institutional regimens were used to compare efficacy in pain relief.
In summary, the studies included 63 pediatric oncology patients with pain at EoL, 235 metastatic sites that received palliative RT for cancer pain, and 139 palliative RT courses administered for cancer pain. The characteristics of all studies are summarized in Supplementary Table S1.
Primary outcome—pain control
Across seven studies, the pooled proportion of pediatric oncology patients achieving pain relief following palliative RT was 77.9% (95% CI 71.2–84.6, p = 0·37) (Fig. 2), with moderate heterogeneity (I2 = 61.3%). None of the included studies reported the use of validated pain assessment tools.
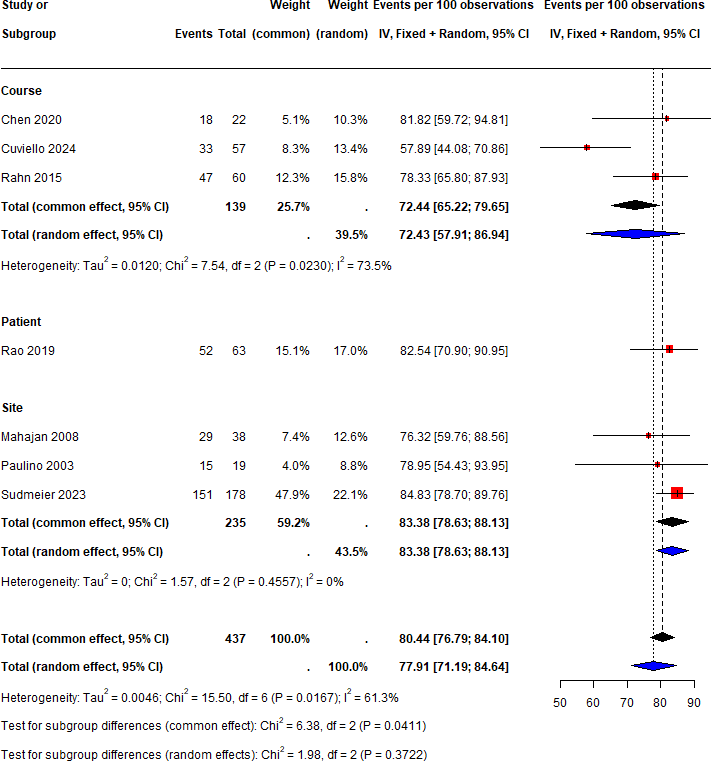
Pain relief with palliative RT. RT, radiotherapy.
A bubble plot analysis (Fig. 3) was done to visually represent the cumulative trend of pain improvement in pediatric oncology patients who received palliative RT through the years and to show if other factors such as advancements in technology or accessibility to health care would have an impact on the overall trend over time. This did not show a significant improvement in the trend of pain reduction with palliative RT through the years but rather a declining trend over time. The size of the bubbles was proportional to the total number of patients/sites/courses recruited into the study.
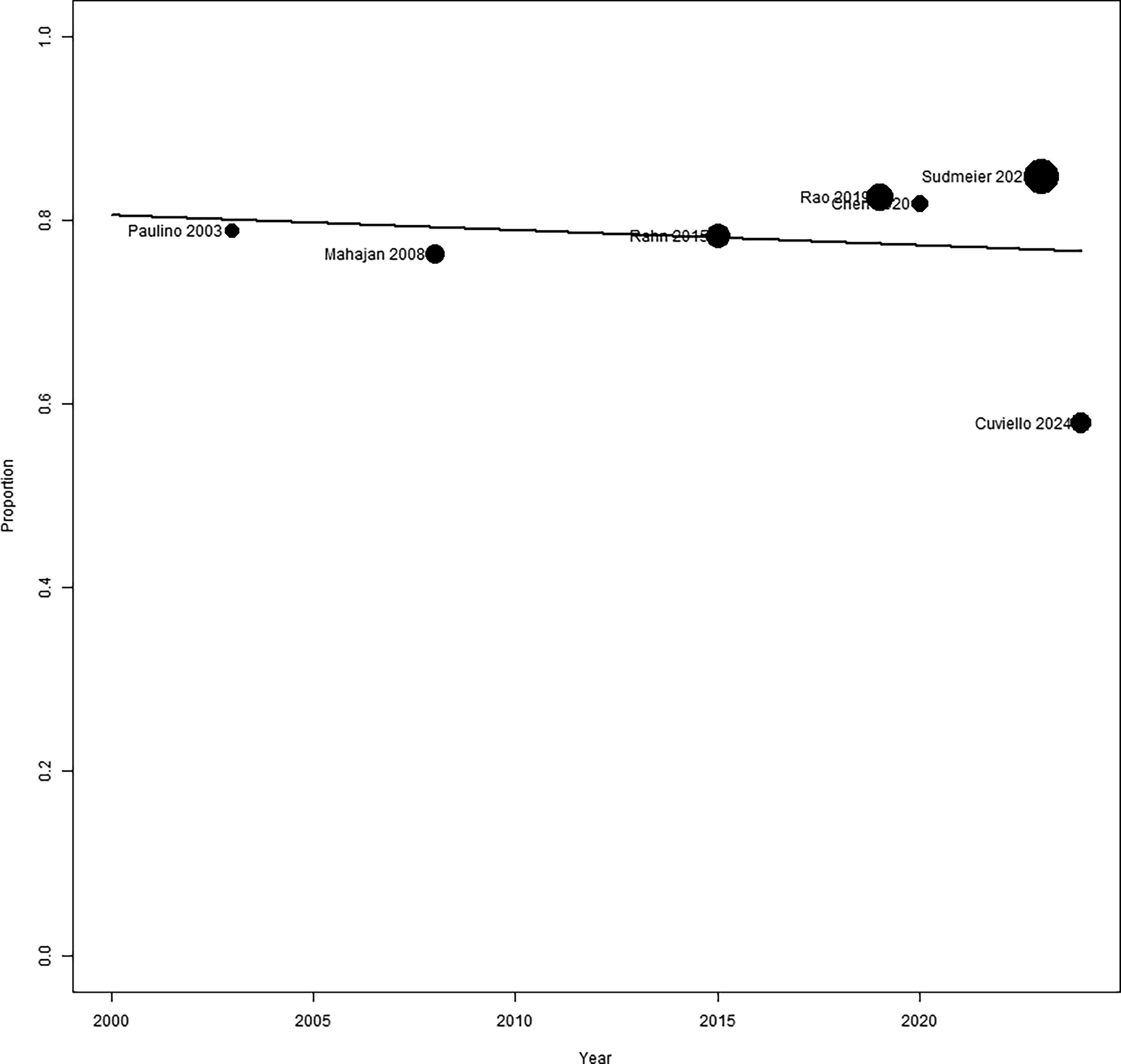
Bubble plot showing proportion of pain improvement from palliative RT against year of study publication.
Subgroup analysis—location of pain
Two studies39,41 had complete data on improvement of bone pain with palliative RT. There was an 80.0% (95% CI 69.89–90.14, p = 0.89) reduction in bone pain in children and adolescents receiving palliative RT (n = 19 metastatic sites/41 courses) (Fig. 4). There was no heterogeneity across these two studies (I2 = 0%).
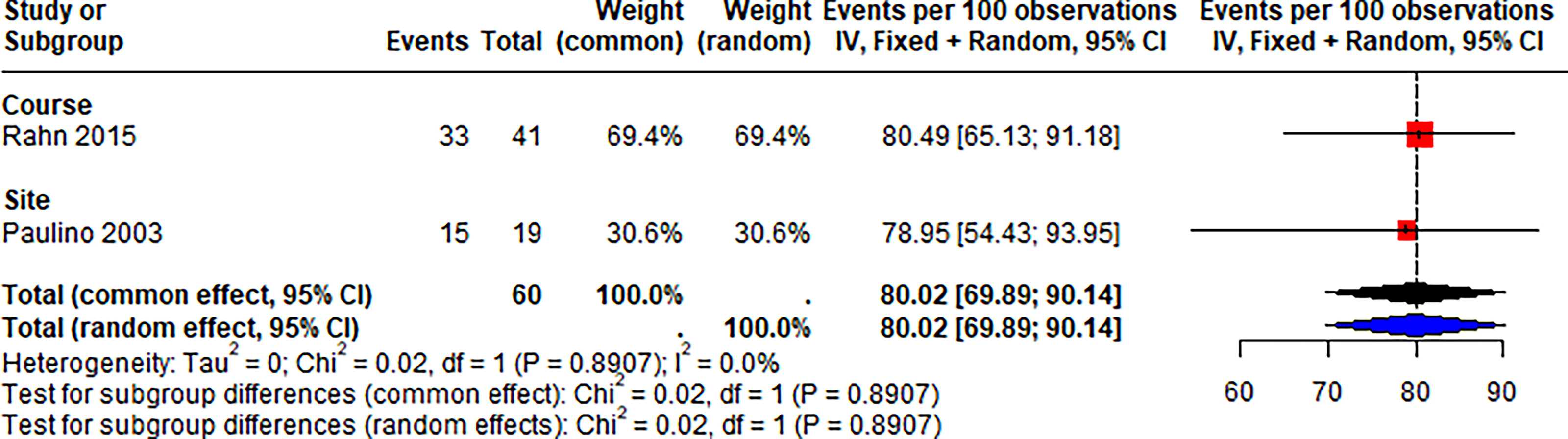
Pain relief in patients with bone pain receiving palliative RT.
Secondary outcome—opioid use reduction
Decreased opioid use was described in two studies8,43 (n = 52 patients/17 palliative RT courses). There was an overall 43.2% (95% CI 31.76–54.73, p = 0.41) reduction in opioid use in children and adolescents with malignancies receiving palliative RT (Fig. 5). There was no heterogeneity across the studies (I2 = 0%).
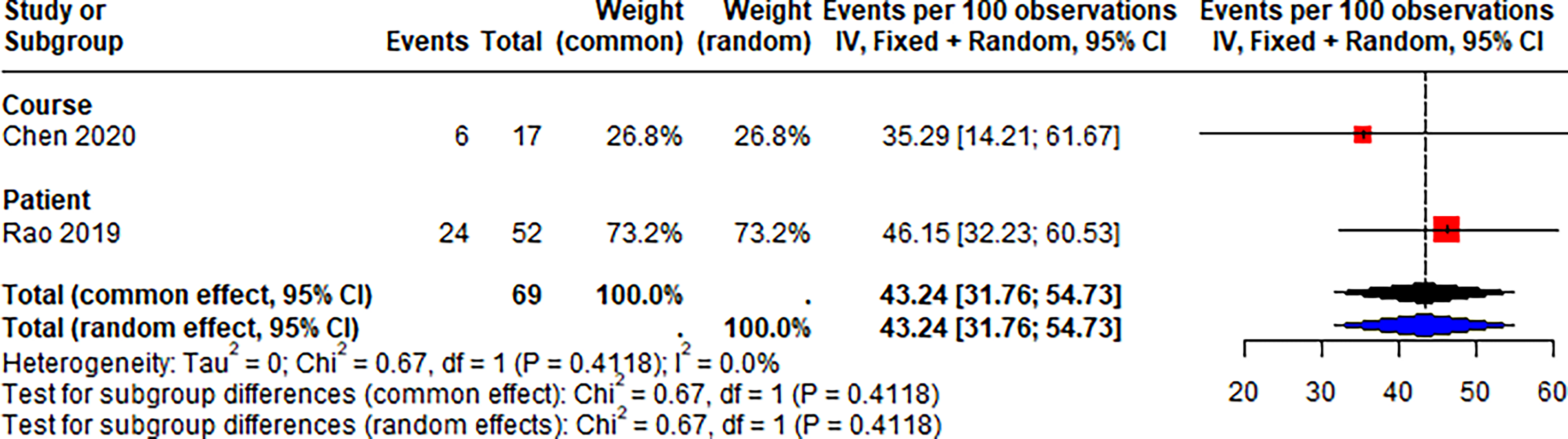
Patient-related outcome of decreased opioid use with palliative RT.
Secondary outcome—safety profile of palliative RT
Side effects were documented, although data specific to the pain subgroup were not provided.20,39,41,42 Due to the limited data on toxicity in the group of children and adolescents receiving palliative RT, no conclusion could be drawn from this MA.
Risk of bias in included studies
Four studies8,39,41,42 were deemed good-quality studies (57.1%), and three studies20,40,43 were deemed fair-quality studies (42.9%) (Supplementary Table S2). Lower scores were associated with limited follow-ups.
The overall GRADE evidence across all seven studies was moderate.8,20,39–43 Supplementary Table S3 shows the GRADE assessment of the studies. The risk of bias was deemed to be low to moderate across most studies, as they were retrospective reviews from single-center institutions with inherent selection bias.
Visual inspection of the funnel plot for publication bias did not show any evidence of significant publication bias (Supplementary Fig. S4).
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis evaluating palliative RT as an adjuvant modality for pain control in pediatric oncology, incorporating evidence up to February 2025. Overall, 77.9% of patients experienced partial or complete pain relief, supporting a clinically meaningful role for palliative RT in alleviating cancer-related pain in children and adolescents. Although this response appears lower than that reported in adult populations, 44 such comparisons should be interpreted cautiously given the heterogeneity of pediatric malignancies, developmental considerations, and differences in treatment intent. The moderate heterogeneity implied that there was variability among the studies, and this would affect the overall generalizability of the results.
From a palliative care perspective, the primary value of palliative RT lies not solely in measurable analgesic response but in its contribution to overall quality of life. In children and adolescents with advanced malignancies, pain is often multidimensional, encompassing physical, psychological, and existential components, and typically requires multimodal management. The modest and heterogeneous evidence base identified in this review therefore reflects not only methodological limitations, but also the inherent complexity of evaluating symptom-directed interventions in pediatric palliative care.
The absence of statistical significance in this analysis should not detract from its clinical implications. Unlike adult studies,14,45,46 pain outcomes in children and adolescents were largely assessed subjectively, often without validated tools, which is particularly challenging in younger children who may be unable to reliably self-report symptoms. This limitation is not merely methodological but reflects a broader challenge in pediatric palliative care: The difficulty of capturing outcomes that are meaningful to patients and families. Future research should prioritize standardized, developmentally appropriate, and patient-centered outcome measures.
Decision making around palliative RT in children is inherently preference-sensitive. Clinicians must balance uncertain benefits against treatment burden, including repeated hospital visits, the need for general anesthesia, and potential toxicities. 42 Importantly, these decisions occur within the broader context of family values, goals of care, and the child’s remaining life expectancy. Early integration of palliative care and radiation oncology may facilitate shared decision making and ensure that interventions are aligned with the goals of care, particularly at the end of life. 42
Our findings suggest that palliative RT may be most beneficial for bone pain, with response rates approaching 80%, consistent with both adult and pediatric literature.13,22,47–49 From a palliative standpoint, this highlights an opportunity for more targeted use of RT in scenarios where the likelihood of symptomatic benefit is greatest. Stratifying patients based on symptom burden, disease trajectory, and expected prognosis may support more individualized and goal-concordant care, particularly in resource-constrained settings.
The observed reduction in opioid use (43.2%) should be interpreted cautiously. While decreased opioid requirements may reflect improved pain control, opioid use in palliative care is influenced by multiple factors, including psychosocial distress, disease progression, and clinician prescribing practices.12,50,51 Moreover, opioid reduction may not always align with patient-centered goals, particularly if analgesic adequacy is compromised. These findings reinforce the need to evaluate outcomes beyond pharmacological surrogates and to prioritize symptom relief and patient comfort.
Concerns regarding toxicity remain a significant barrier to the use of palliative RT in pediatric populations.9,42 However, available evidence suggests that treatment is generally well tolerated, and parental perceptions of outcomes are favorable. 52 Within a palliative framework, the acceptability of toxicity must be considered in relation to anticipated benefit, life expectancy, and the child’s overall experience of care. Proactive symptom management and careful treatment planning are essential to minimize harm while preserving quality of life. 53
Barriers to access, including logistical challenges, financial burden, and clinician hesitancy, further limit the use of palliative RT.20,42 Moreover, pediatric radiotherapists have also described palliative RT in children as challenging, as children are uncooperative. 23 This might prompt the use of general anesthesia (GA) for younger children, which is a huge consideration and at times a hindrance for the implementation of palliative RT in children, based on a study by Rao et al. across six international pediatric centers 9 where it was perceived by clinicians that pediatric patients would benefit more from an optimized narcotics regimen as compared to anesthesia for daily palliative RT. Ntoukas and colleagues (2020) from the Princess Margaret Cancer Centre in Toronto, Canada, did a retrospective cohort study of 779 patients to determine the frequency of GA use in children requiring RT and found that 90% of children under 3 years old and 28% of children aged 3–6 years old required GA. 24 GA can be both emotionally and logistically taxing for patients, parents, and radiation therapists. 23 Children who receive frequent doses of palliative RT and who must fast prior to GA may face other challenges at end-of-life, including compromised nutrition. 53
These barriers may disproportionately affect children in resource-limited settings, where access to specialized services is constrained. Enhancing awareness of the potential role of palliative RT, alongside early multidisciplinary involvement, may help address these inequities and support more timely, goal-directed care. 54
The timing of palliative RT is particularly important in the context of limited life expectancy. Evidence suggests that treatment delivered close to the EoL may offer limited benefit, given the delayed onset of analgesic effect. 55 This raises important ethical considerations regarding the appropriateness of initiating RT in the final weeks of life, when the focus may shift towards comfort and minimizing intervention burden.7,56 Early identification of patients who are most likely to benefit is therefore critical.
Despite its potential, palliative RT remains underutilized in pediatric oncology.21,57 This likely reflects a combination of limited high-quality evidence, uncertainty regarding benefit, and the unique challenges of delivering RT to children. From a palliative care perspective, this underutilization may represent missed opportunities to alleviate suffering, particularly when RT is considered late or not at all.
Importantly, the distinction between statistical and clinical significance is especially relevant in palliative care research. 58 Interventions that do not meet conventional thresholds for statistical significance may still provide meaningful improvements in symptoms, function, or quality of life. In this context, palliative RT should be viewed as a potentially valuable component of holistic, multidisciplinary care for children with advanced cancer.
Although the results of this systematic review were not statistically significant, this work still adds to the growing body of evidence supporting integrated approaches, including the use of palliative RT, to symptom control in pediatric oncology. Rather than being reserved as a late or last-line intervention, palliative RT should be considered earlier in the disease trajectory for children with refractory pain, particularly when pain is localized and attributable to sites such as bone metastases. Early referral to radiation oncology, alongside specialist palliative care, may facilitate timely, goal-concordant interventions and reduce the risk of unmanaged or escalating symptom burden. 42
Clinical decision making should remain individualized and grounded in the principles of pediatric palliative care, with careful consideration of prognosis, symptom severity, treatment burden, and family preferences. Importantly, the potential benefits of palliative RT must be weighed against its logistical and procedural demands, including the need for repeated hospital visits and GA. In this context, shared decision making is essential, ensuring that families are supported to make informed choices aligned with their goals of care.
There is a clear need for prospective, multicenter studies using standardized, developmentally appropriate, and patient-centered outcome measures. Future research should prioritize not only pain response but also broader domains such as quality of life, functional status, and caregiver-reported outcomes. Given the ethical challenges of conducting randomized trials in this population, well-designed observational studies and pragmatic trial approaches may offer the most feasible path forward. Additionally, greater attention should be paid to health system factors, including access to RT and disparities in utilization across settings.
Limitations
This study has several limitations that are particularly relevant in the context of palliative care research. The small sample size and reliance on observational studies limit statistical power and increase susceptibility to bias. 59 Analyses conducted at the level of metastatic sites and RT courses, rather than individual patients, may overestimate treatment effects and do not fully capture patient-centered outcomes.
Heterogeneity in tumor types, treatment regimens, and outcome measures further complicates interpretation and limits generalizability. The absence of randomized controlled trials reflects ethical and practical challenges in pediatric palliative care, including difficulties in establishing equipoise and prioritizing patient-centered outcomes.60,61 Similar limitations have been reported in other pediatric meta-analyses, where small study numbers and variability in practice contribute to imprecision.62–64 Finally, exclusion of non-English studies may have introduced language bias.
Conclusion
Palliative RT appears to offer clinically meaningful pain relief for a substantial proportion of pediatric oncology patients, particularly those with bone-related pain, despite the limitations of the current evidence base. Although statistical significance was not consistently demonstrated, these findings should be interpreted within the broader context of palliative care, where the primary goal is the alleviation of suffering rather than cure.
Incorporating palliative RT into multidisciplinary care pathways has the potential to improve symptom control and enhance quality of life for children with advanced cancer. However, its use remains limited and often delayed. A shift toward earlier, more integrated, and patient-centered use of palliative RT, supported by improved evidence and clearer clinical pathways, may help address this gap and better align care with the needs of children and their families at the end of life.
Statement of Ethics
No ethical approval was required because this study is based exclusively on published literature.
Data Sharing Statement
All of the individual study data collected, study protocol, and statistical analysis done are available for sharing indefinitely. Proposals should be directed to
Authors’ Contributions
P.R.R. and R.F. were responsible for the conception and design of this study. P.R.R. and M.Y.C. were responsible for performing the search. P.R.R. was involved in extracting data. P.R.R. and R.S. planned the statistical approach, and R.S. conducted all statistical analyses. P.R.R. was responsible for drafting the article. P.R.R., M.L., M.Y.C., R.S., G.C.W.Y., and F.R. revised the article, approved its final version, and have agreed to be accountable for all aspects of the work to ensure its accuracy.
Footnotes
Acknowledgments
The authors acknowledge Dr. Looi Wen Shen, a radiation oncologist and a visiting consultant to KK Women’s & Children’s Hospital, for his advice on radiotherapy definitions and Dr. Mala Mann, a systematic reviewer and librarian from the University Hospital of Wales, for her guidance during the formulation of the search strategy.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding required for this study.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.