
Abstract
The aim of this study was to examine the factor structure of the Male Body Attitudes Scale (MBAS) among a sample of 212 adolescent males by conducting a confirmatory factor analysis. The data revealed that while muscularity and low body fat factors were appropriate for the male sample, the height factor was not supported. The composite MBAS-Spanish version (MBAS-S) and its two factors had high internal consistency and were not significantly related to the traditionally used measure of body image (Eating Disorder Inventory–Body Dissatisfaction [BD]), confirming that this subscale only appears to evaluate female body concerns. Correlations with psychological well-being variables (anxiety, emotional regulation, and self-esteem) supported the concurrent validity of the instrument. These findings provide further evidence in support of the hypothesis that BD in males has been inappropriately evaluated by measures designed specifically for females. Despite the fact that our results did not replicate the original factorial structure of the instrument, the MBAS-S presents adequate psychometric properties and can be considered as a valuable assessment tool for BD among adolescent males.
Keywords
Introduction
Research regarding body image has shown that women consistently report greater body image concerns than men (Sepúlveda, Botella, and León 2001; Cash et al. 2004; Cash and Pruzinsky 2002). When asked about their ideal body shapes, men have been found to express concerns regarding their muscle mass and a desire to increase it (McCreary and Sasse 2000; Thompson and Cafri 2007), contrary to the desire for slimness and weight loss that are more commonly expressed by women (McCreary and Sasse 2000).
Among female populations, body dissatisfaction (BD) has been associated with adverse psychosocial effects such as eating disorders (Calado et al. 2011), depression (Noles, Cash, and Winstead 1985), or poor quality of life (Cash and Pruzinsky 2002). Cafri and Thompson (2004) highlighted that there were inadequate instruments available to evaluate BD in males, as the questionnaires that were being used had been originally developed and validated for female samples, such as the Body Satisfaction Questionnaire (Cooper et al. 1987) or the subscales for Drive of Thinness or BD on the Eating Disorder Inventory (EDI-2; Garner 1998). In short, it is necessary to reconsider the way in which male BD, and its associated health consequences, has previously been assessed (Murray et al. 2010; Ricciardelli and McCabe 2004).
In this regard, several self-report instruments specifically designed to assess BD among males have been developed over the last fifteen years. The first instruments developed were the Swansea Muscularity Attitudes Questionnaire (Edwards and Launder 2000) and the Drive for Muscularity Scale (DMS; McCreary and Sasse 2000), followed by the Male Body Attitudes Scale (MBAS; Tylka, Bergeron, and Schwartz 2005), all of which were administered in male college-age samples. Other instruments that have been developed specifically for male populations are the Muscle Appearance Satisfaction Scale (Mayville et al. 2002), which used a male weight lifting sample, and the Muscle Dysmorphic Disorder Inventory (Hildebrandt, Langenbucher, and Schlundt 2004), which used three separate samples of men and women to measure the psychometric properties of the instrument. These instruments have all shown adequate psychometric properties.
Negative physical and psychological effects associated with higher levels of drive for muscularity and BD have been reported by both gay and heterosexual men in studies using the above-mentioned instruments. Among the negative effects, high levels of depression, low self-esteem (Cafri, Strauss, and Thompson 2002), eating pathology, anabolic-androgenic steroid use, and other associated health problems, such as kidney and liver problems (Olivardia et al. 2004), as well as social physique anxiety (Duggan and McCreary 2004), have been mentioned.
A recent review of epidemiological studies in Spain found that the prevalence rates of eating disorders were similar to those seen in other developed nations: around 1–3 percent in adolescent populations for both males and females and 4–5 percent for adolescent girls (Peláez Fernández, Raich Escursell, and Labrador Encinas 2010). There is also reason to believe that rates of eating disorders and body image disturbance among males in Spain could be skewed, given that no instruments are currently available which have been developed with specific body image concerns of males in mind. Just as research on body image in other countries has shown that body image dissatisfaction is distinct for men and women, the same is suspected to be true in Spain. For instance, in a large-scale study on gender differences related to body image, it was found that 22.1 percent of the male adolescents participating in the study viewed themselves as slightly or very thin, whereas the girls tended to view themselves as slightly or too fat (Valverde, De Los Santos, and Rodriguez 2010).
All this evidence suggests that there is a need for validating an instrument for use in Spanish populations, capable of detecting body image concerns expressed by males and associated distress.
The MBAS
BD assessed by the MBAS offers a more comprehensive picture of men’s body image by including muscle, body fat, and height dimensions, each one of them being associated with different aspects of men’s psychological well-being (Blashill 2010). It consists of twenty-four items grouped into three subscales measuring muscularity (ten items), low body fat (eight items), and height (two items). It also includes four additional items that measure overall body build and are not included in any of the subscales but are included in the total score of the scale. This instrument has only been administered in English-speaking populations, and therefore, no translation or validation of this measure is available for Spanish-speaking populations.
The development and psychometric evaluation of the MBAS have been examined through three studies with independent samples of college males (Tylka, Bergeron, and Schwartz 2005). The MBAS factor structure has been verified through an exploratory and confirmatory factor analysis (CFA), and its psychometric evaluation has shown evidence for its convergent and concurrent validity as well as for its internal consistency. Internal consistency was adequate, with Cronbach’s αs varying among studies, from .90 to .91 for the total scale, from .90 to .94 for the low body fat subscale, from .89 to .91 for the muscularity subscale, and from .66 to .88 for the height subscale. The stability of the MBAS has also been studied over a two-week period presenting an adequate test–retest reliability (r = .91 for the total scale, r = .88 for the muscularity subscale, r = .94 for the low body fat subscale, and r = .81 for the height subscale). Likewise, Blashill and Vander Wal (2009) analyzed the factor structure of the MBAS, by using a confirmatory analysis, in a sample of 207 self-identified gay men. The authors found that the original three-factor solution, as well as a two-factor solution (body fat and muscle dissatisfaction), showed strong factorial validity. The original authors themselves also pointed out that the stability of height subscale could be questionable, considering that it only grouped two items and recommended further validation of the instrument with preadolescent and adolescent samples, athletes, and clinical samples (Tylka, Bergeron, and Schwartz 2005).
Aims of the Study
This article presents the first validation of the Spanish version of the MBAS with a male adolescent sample. The specific aims of the present study are as follows: (a) to test the validity of factor solutions proposed for the Spanish version of the MBAS via CFA and (b) to explore internal consistency estimates of the MBAS for each subscale score, as well as the discriminant validity with two subscales of the EDI-2, and the concurrent validity of the scale (anxiety, difficulties and difficulties with emotional regulation and self-esteem). We expect low associations between the MBAS-S and the Drive for Thinness (DT) and BD subscales of the EDI-2, given that the development of traditionally used scales to measure BD has been based only on concerns relevant to females (Tylka, Bergeron, and Schwartz 2005). Furthermore, we predict to find moderate inverse associations between the MBAS-S and self-esteem and moderate positive associations between the MBAS-S and anxiety and emotional dysregulation.
Material and Method
Participants
Two hundred and twenty-five adolescent males from a Secondary School in Madrid, Spain, were recruited for the study. The mean age was 14.4 years (SD = 1.5), ranging from twelve to seventeen years, with all of the students attending this school (seventh to twelfth grades) at the time of the study. The majority of their parents had a full-time job (95 percent of the fathers and 71 percent of the mothers), and around 55 percent of the parents reported having a university degree as the highest form of education achieved. The average body mass index (BMI) for the male adolescents was 20.5 (SD = 2.97); 46.7 percent had exercised in the past four weeks in order to lose weight and only 9.9 percent had followed a diet in the past three months, with the majority of those following a diet (n = 13) having lost less than five kilograms in the past month. “Of the 225 students who agreed to participate, thirteen of them (5.8 percent) left more than two items blank on the MBAS-S and they were therefore excluded from the statistical analysis.”
Measures
Demographics and health habits
Students completed a demographic questionnaire on which they indicated their age, grade, as well as the educational and employment status of their parents. Questions were also included to assess students’ eating and exercise habits, such as “have you exercised in the past four weeks in order to lose weight?” The BMI (BMI = weight [kg]/height [m]2) was also calculated for each participant based on self-reported height and weight.
Male BD
The MBAS (Tylka, Bergeron, and Schwartz 2005) assesses men’s dissatisfaction with their bodies. It consists of twenty-four items rated on a 6-point Likert-type scale, which ranges from 1 (never) to 6 (always). The original measure includes three subscales (low body fat, muscularity, and height) and subscale scores are averaged. Higher scores indicate greater male body image dissatisfaction.
BD
The EDI-2 (Garner 1998, 1991) is a sixty-four-item self-report questionnaire that assesses eating attitudes and behaviors associated with eating disorders. Each item includes six responses on a Likert-type scale, which ranges from 0 (never) to 5 (always). Before summing items to calculate subscale scores, they must be recoded so that 0–2 are 0, 3 is 1, 4 is 2, and 5 is 3. The instrument consists of eleven subscales. For the purpose of this study, only two subscales were used: EDI-DT (seven items) and EDI-BD (nine items), which assess ideal shape, weight concerns, and desire for thinness. The DT scale includes questions that reflect an excessive concern with dieting and eating in excess, preoccupation with weight and fear of weight gain, such as “I am preoccupied with the desire to be thinner.” The items on the BD scale reflect dissatisfaction with body parts that tend to be of concern to females (stomach, thighs, hips, and buttocks) and the individual’s figure as a whole. Test–retest reliability ranges between 0.41 and 0.97, and the instrument has demonstrated adequate construct validity. The Spanish version has shown good internal consistency (α = .80). For the current sample, Cronbach’s α was .44 for the EDI-DT subscale and .81 for the EDI-BD subscale.
Level of anxiety
The State and Trait Anxiety Inventory for Children (STAIC; Spielberger et al. 1973; Seisdedos 1990) is a self-report questionnaire divided into two subscales. Each one consists of twenty items rated on a 3-point Likert-type scale, ranging from 1 (almost never) to 3 (often). One subscale measures “State” anxiety (transitory, i.e., “I feel very upset, upset, or not upset”) and the other measures “Trait” anxiety (permanent; i.e., “I worry too much.” The internal consistency has been estimated to be from .78 to .87. The reliability coefficients of the Spanish version were satisfactory, falling between .85 for the Trait scale and .89 for the State scale. For the current sample, Cronbach’s αs were .87 and .88, respectively. Items are scored to calculate subscale scores, with higher scores suggesting higher levels of state and trait anxiety.
Problems in emotional regulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer 2004; Hervás and Jódar 2008) is a questionnaire containing thirty-six items rated on a 5-point Likert-type scale, ranging from 1 (almost never) to 5 (almost always). This scale aims to measure emotional regulation through a total score and six subscales (such as lack of emotional awareness). Example items include “I pay attention to how I feel” and “I’m aware of my feelings.” For this study, only the total score was used. The scale has shown adequate test–retest reliability during a period of six months. In regard to the internal consistency, Cronbach’s α was .93 for the original total scale and .94 for the Spanish total scale. For the current sample, Cronbach’s α was .92. Items are summed, and higher scores suggest greater difficulties with emotional regulation.
Level of self-esteem
Rosenberg’s Self-Esteem Scale (RSE; Rosenberg 1989; Echeburúa and Botella 1995) consists of ten statements regarding a person’s general beliefs about himself or herself. Each item is measured on a 4-point Likert-type scale, ranging from 4 (strongly agree) to 1 (strongly disagree). Five of the items are positively worded such as, “I feel good about myself,” and the other five items are negatively worded and are therefore reverse scored such as, “I certainly feel useless at times.” Items are summed to calculate a total score. Cronbach’s α of the original version is .93, while in prior studies, the Spanish version has obtained a coefficient α of .88. For the current sample, Cronbach’s α was .83. Lower scores suggest less self-esteem.
Procedure
The translation and cultural validation of the MBAS scale was carried out using a back translation procedure following international guidelines (Balluerka et al. 2007; Muñiz and Bartram 2007). First, the original English version was translated into Spanish by two independent expert translators with knowledge of psychology and psychopathology. Second, this version was translated back into English by another bilingual translator. Third, a focus group was formed by the translators who had participated in the back translation procedure, and a discussion among them was carried out in order to consolidate the forward and back-translated versions of the MBAS, to identify any discrepancies between them, and to develop what would be considered the definitive version of the questionnaire. In order to retain an item, the translated and back-translated versions of the item needed to be identical. In the case of discrepancies between the items, the contents were analyzed to determine the appropriate course of action. Finally, the definitive version of the MBAS was generated and used for the further objectives of this study as shown in Table 1.
Descriptive Information and Item Translations of the MBAS-S.
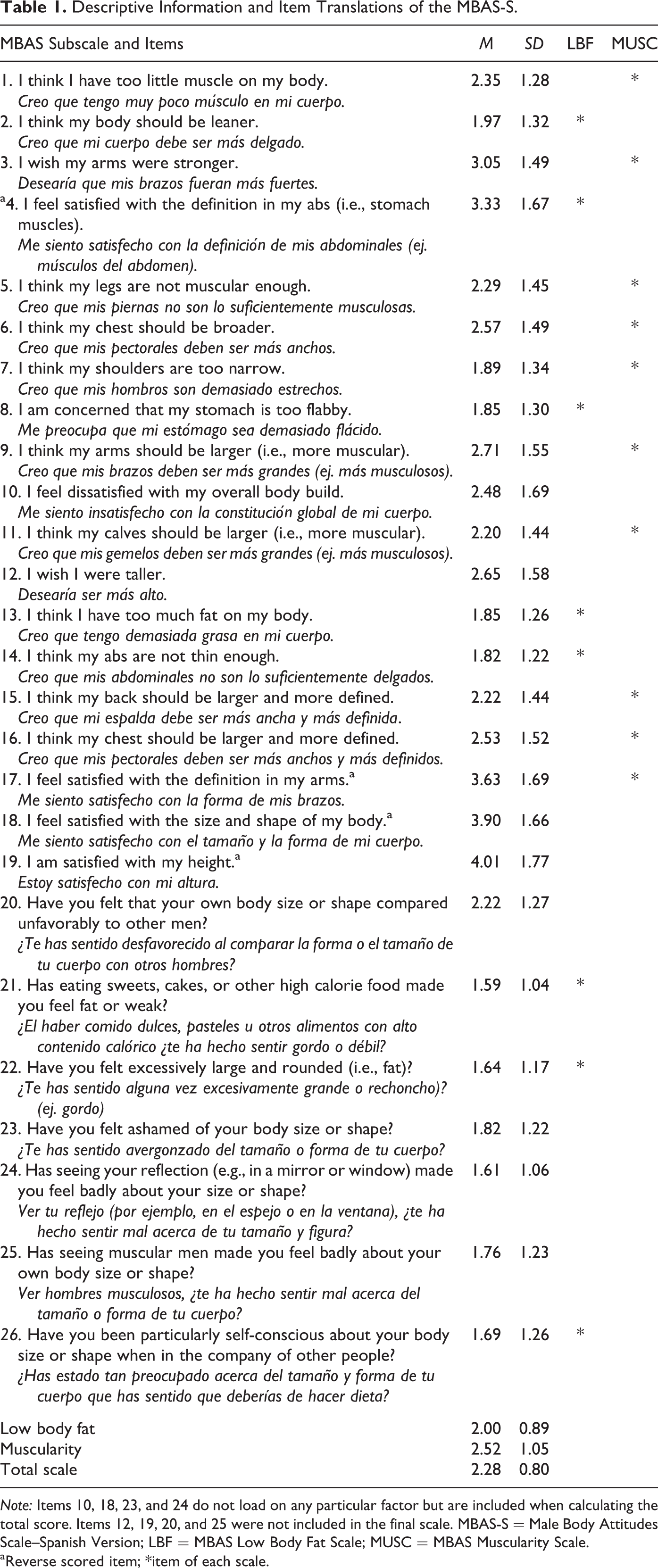
Note: Items 10, 18, 23, and 24 do not load on any particular factor but are included when calculating the total score. Items 12, 19, 20, and 25 were not included in the final scale. MBAS-S = Male Body Attitudes Scale–Spanish Version; LBF = MBAS Low Body Fat Scale; MUSC = MBAS Muscularity Scale.
aReverse scored item; *item of each scale.
The design of the study was cross sectional. All students attended a subsidized school in Madrid, Spain. The survey was carried out during the spring semester of the 2010–2012 academic school years. Parental consent was obtained. All participants signed the informed consent form and anonymity was guaranteed. Rate of nonparticipation in the study was 0.05 percent (primarily due to students being absent for medical reasons on the day the battery was administered). Participants were not granted course credit for their involvement. The research was reviewed and approved by the institutional board.
Statistical Analysis
PRELIS 2 and LISREL 8.71 softwares were used for the CFA, and SPSS 20.0 for Windows was used for the reliability and validity analyses.
In addition to the twenty-four items of the MBAS, the original authors (Tylka, Bergeron, and Schwartz 2005) included five additional items in the first prevalidated scale. We chose to translate two of these items, those that concerned social comparison, in order to examine their cross-cultural validity in our sample (item 20 “Have you felt that your own body size or shape compared unfavorably to other men?” and item 25 “Has seeing muscular men made you feel badly about your own body size or shape?”).
A structural equation model (SEM) was initially carried out for the model path, presented in Figure 1, followed by the addition of items 20 and 25 to the “low body fat” factor for the same model. In order to identify the model, the variances of the three latent variables were fixed to 1.0. In addition, any saturations in more than one factor were restricted to zero and covariances were not permitted, given that our theoretical model did not allow for items to load on more than one factor.
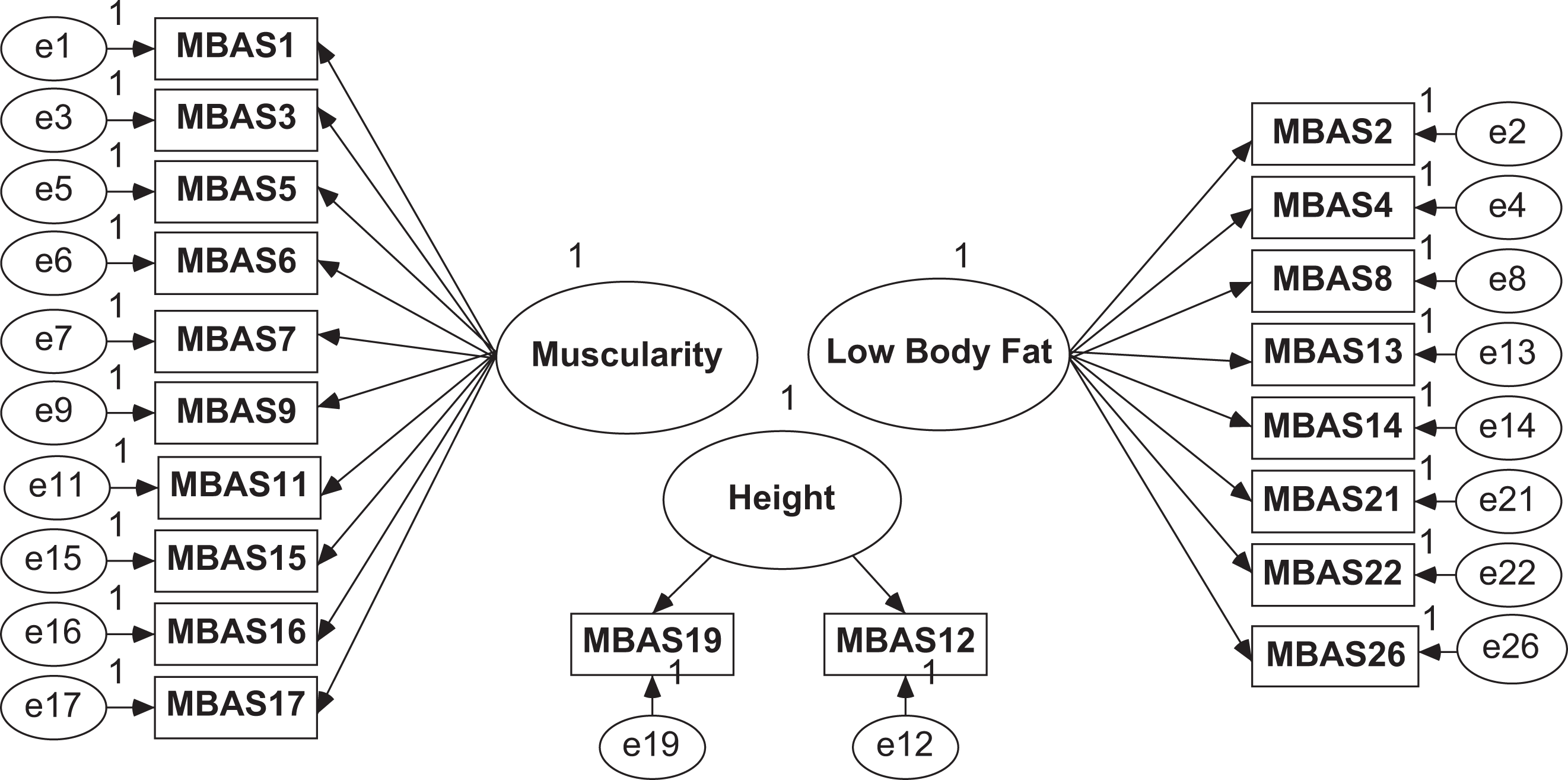
Path diagram corresponding to the initial model of fit.
A Robust diagonally weighted least squares estimation method was used, which adjusts the model to a matrix of polychoric correlations and requires a calculation of the asymptotic covariance matrix. This method is required when ordinal variables that do not follow a normal distribution are used (Jöreskog 2005, 1994). Tests of univariate normality as well as Mardia’s coefficient (Mardia 1970) produced results that permitted us to reject the null hypothesis of multivariate normality.
Following several authors’ recommendations (Hu and Bentler 1999), the fit of the model was determined by a combination of Satorra–Bentler Scaled χ2 (p > .05), root mean square error of approximation (<.08) with its confidence interval, comparative fit index (>.95), and nonnormed fit index (>.90).
Descriptive statistics were calculated for the validated MBAS–Spanish version (MBAS-S) and its subscales as well as for the other instruments used. Scale reliability was assessed with Cronbach’s α. Following a Kolmogorov–Smirnov test, data did not follow the normal distribution. Discriminant validity was examined with the subscales of EDI-DT and EDI-BD. The concurrent validity was also explored by examining the Spearman correlations between the MBAS-S and level of anxiety (STAIC), degree of emotional regulation difficulties (DERS) and level of self-esteem (RSE).
Results
CFA
A Heywood case was identified in both SEM analyses for the initial model path (Figure 1) and for the same model adding items 20 and 25, thus the model was not able to be considered to be well specified (Bentler and Chou 1987; Dillon, Kumar, and Mulani 1987). When Heywood solutions are generated in any SEM, the interpretation of the results is fully contraindicated. Accordingly, due to the fact that latent factors are independent and given the possibility of serious identification problems, the initial model adjustment with a two-factor structure was decided upon (considering that the Heywood case only appeared in the third factor). A unique factor model was also adjusted but yielded a poor fit.
Fit index values of the two-factor structural models are presented in Table 2; model 1 represents the initial model without the third factor (height) and model 2 represents the initial model without the third factor (height) and adding items 20 and 25. Both models have been respecified, allowing covariance between residual values in the following pairs of items: two to thirteen and three to nine in order to improve adjustment. These pairs of items can share some degree of variation apart from the variation associated with the two-factors (similarly worded items and in the same direction in terms of content).
Fit Index Values for the Tested Models.

Note: df = degrees of freedom; RMSEA = root mean square error of approximation; CI = confidence interval; NNFI = nonnormed fit index; CFI = comparative fit index.
The values obtained from the models indicated that the null hypothesis should be rejected (p < .01). However, it is worth examining the index χ2/df, which provides a suitable fit index (χ2 < 2). Fit indices are consistent with an appropriate overall model fit. When considering the residuals of model 1, less than 38 percent of them were located outside the desired range (−2, 2; Table 2). Results clearly show that both models offer a very similar reasonable fit. All parameters of both model 1 and model 2 were statistically significant. However, considering that only model 1 has been supported in prior studies (Blashill and Vander Wal 2009), we decided to use only this one in order to be consistent with prior findings. The resulting plot of the final model is shown in Figure 2 (model 1).
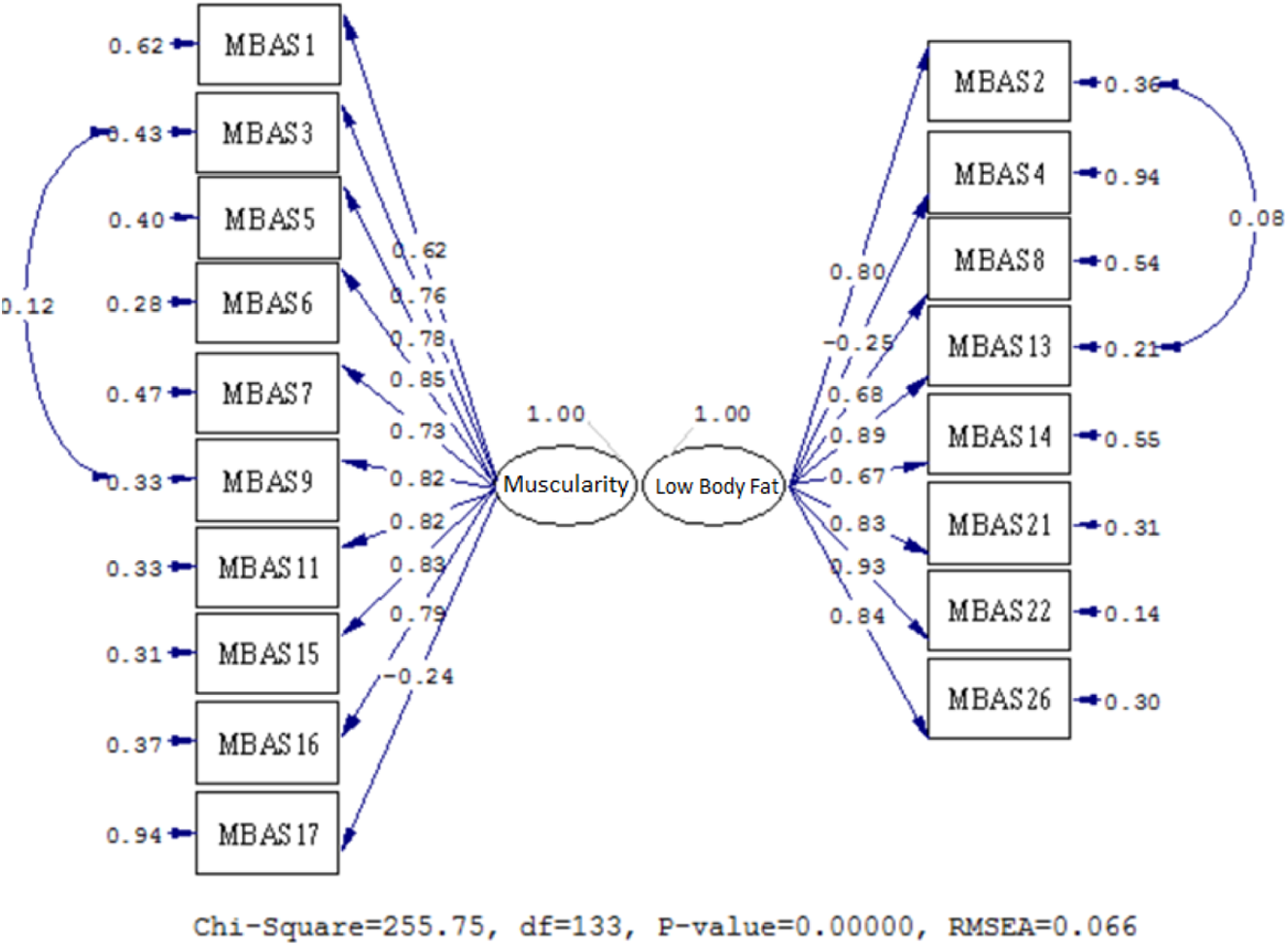
Results from confirmatory factor analysis to model 1 with corresponding standardized coefficients.
Descriptive Statistics and Reliability
Table 1 shows the descriptive statistics of the MBAS-S. A total score of the MBAS-S can be determined by averaging the twenty-two items, and individual subscale scores can be determined by averaging the items of the two subscales: Low Body Fat (eight items) and Muscularity (ten items). In addition, as in the case of the original MBAS, the total scale includes four items that measure overall body build and are not included in any subscale. The mean total MBAS-S score was 2.28 (SD = 0.80). The MBAS twenty-two-item scale demonstrated satisfactory reliability, with Cronbach’s α for the total scale of .90, for the Low Body Fat scale of .85, and for the Muscularity scale of .89.
Construct Validity
In order to test discriminant validity of the MBAS-S scale, Spearman correlations were calculated (see Table 3). No correlation was found between the MBAS-S total and its subscales and the EDI-BD. After a Bonferroni correction, only significant low positive correlations were found between the MBAS-S total and the EDI-DT (ρ = .22, p = .001) and between the Low Body Fat subscale and the EDI-DT (ρ = .32, p = .001). Regarding the concurrent validity, Table 3 shows significant positive correlations of low to slightly moderate strength between the MBAS-S Total, Low Body Fat, and Muscularity scores and the level of anxiety (STAIC; with MBAS-S Total, ρ = .34, p = .001 for the STAIC-State subscale and ρ = .39, p = .001 for the STAIC-Trait subscale) and the DERS (with MBAS-S Total, ρ = .37, p = .001), as well as significant negative associations with level of self-esteem (RSE; with MBAS-S Total, ρ = −.32, p = .001). In addition, those who reported more BD, in particular, dissatisfaction toward their level of body fat, showed a moderate and positive association with having dieted in the past three months, having practiced physical activity in the last four weeks with the goal of losing weight and had a higher BMI.
Descriptive Distribution and Correlations between the Male Body Attitudes Scale–Spanish Version (MBAS-S) and Other Instruments of Body Dissatisfaction (EDI-DT and EDI-BD) and Psychological Well-Being.
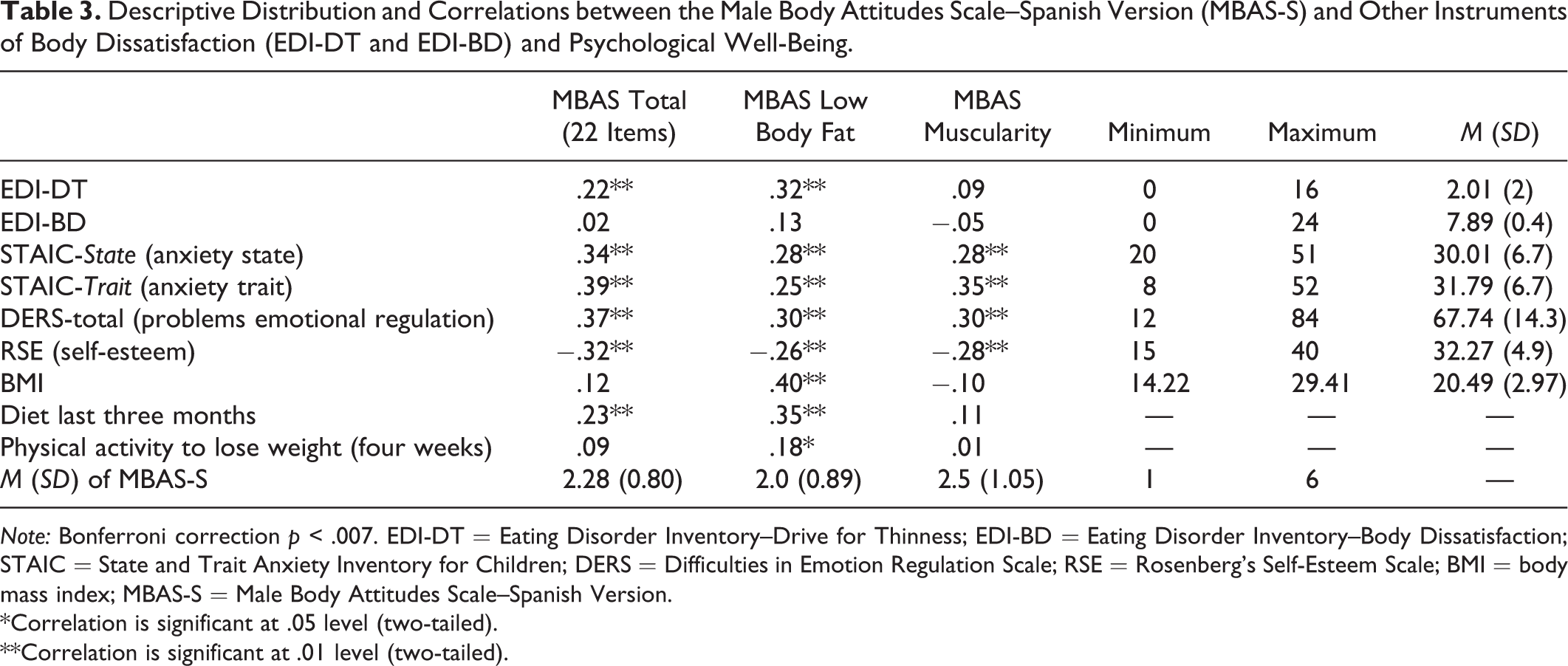
Note: Bonferroni correction p < .007. EDI-DT = Eating Disorder Inventory–Drive for Thinness; EDI-BD = Eating Disorder Inventory–Body Dissatisfaction; STAIC = State and Trait Anxiety Inventory for Children; DERS = Difficulties in Emotion Regulation Scale; RSE = Rosenberg’s Self-Esteem Scale; BMI = body mass index; MBAS-S = Male Body Attitudes Scale–Spanish Version.
*Correlation is significant at .05 level (two-tailed).
**Correlation is significant at .01 level (two-tailed).
Discussion
Given that there were no instruments validated in Spain that measure BD among males, the present study aimed to carry out a cross-cultural adaptation and validation of the MBAS using a CFA in a Spanish population. In contrast to the three-factor structure consisting of Muscularity, Low Body Fat, and Height subscales proposed by the original MBAS study (Tylka, Bergeron, and Schwartz 2005), the CFA carried out for the present study only provided support for the first two factors, resulting in the elimination of the Height subscale. However, this is not the first study to propose a factor model that does not include the height factor. Blashill and Vander Wal (2009), who also used a CFA to explore the factor structure of the MBAS among gay men, found that a two-factor model composed of muscularity and low body fat indicated a strong fit. These authors along with others (Ryan et al. 2011) have criticized the use of the MBAS Height subscale, pointing out that a factor with fewer than three items tends to be weak and unstable and that three to five items per factor is preferable (Costello and Osborne 2005).
In terms of the internal consistency, the MBAS-S total scale and subscales demonstrated similar α coefficients to those reported by the original validation study (Tylka, Bergeron, and Schwartz 2005). Regarding discriminant validity, as expected, the majority of the correlations between the MBAS total score and subscale scores and the BD subscale of the EDI-2 were nonsignificant. However, two small positive significant correlations were found between the EDI-DT subscale and the MBAS-S total score and the Low Body Fat subscale of the MBAS-S. Given the low internal consistency of the EDI-DT in the male sample, the reliability of this subscale may be questioned.
To date, there are no published studies comparing outcomes on the MBAS and EDI-2. However, studies using other instruments that evaluate male BD have examined their relationship with the EDI-2. For example, McCreary and Sasse (2000) found a small and significant negative correlation between the DMS and the EDI-BD. Tod, Morrison, and Edwards (2012) compared the relationship between four male BD instruments and the EDI-DT subscale, finding small positive significant correlations with the EDI-DT. These authors confirmed that these instruments measure a construct that was distinct from that of DT due to the fact that their correlations with the EDI-DT were much smaller than their correlations with one another.
Traditionally, BD has been evaluated with the EDI-BD subscale. However, the fact that the MBAS-S total and its subscales scores did not significantly correlate with the EDI-BD suggests that it is indeed evaluating a concept distinct to that of male body image. Numerous studies have used this subscale as a tool to evaluate body image concerns and/or to screen for eating disorders and have concluded that males exhibit less BD than their female counterparts (Kerremans, Claes, and Bijttebier 2010; Spillane et al. 2004). Nevertheless, the findings of the current study raise some questions about the appropriateness of using the same measures to evaluate BD in both males and females, thus supporting the importance of considering a gender-differentiated approach when constructing new instruments and identifying statements that best reflect BD as perceived by each gender.
Concurrent validity was established with moderate correlations with other reliable instruments developed to assess anxiety, self-esteem, and emotional regulation difficulties, which represent some of the most prevalent difficulties in adolescence. Both state and trait anxiety were found to significantly and positively correlate with the MBAS-S total score and subscales. Most previous studies exploring disordered eating and BD have tended to use measures that evaluate overall negative affect rather than specifically anxiety. McCabe and Vincent (2003) examined the influence of psychological factors on disordered eating in adolescent males, using the anxiety subscale of the Depression Anxiety Stress Scales (Lovibond and Lovibond 1995), and found that anxiety was one of the most consistent predictors of disordered eating in adolescent boys. In terms of self-esteem, significant negative correlations were found with the MBAS-S total score and subscales. Self-esteem has been proposed as an important factor influencing adolescent boys’ body image (Ricciardelli and McCabe 2004), and studies have shown that higher levels of steroid use are more common among adolescent males with lower levels of self-esteem (Irving et al. 2002; Kindlundh et al. 2001).
Finally, the DERS were also found to correlate positively and significantly with the MBAS-S total score and subscales, providing further support for the concurrent validity of this instrument. In a study employing both the DERS and MBAS in a sample of college men, Lavender and Anderson (2010) found that after accounting for BMI and negative affect, emotion regulation difficulties accounted for the unique variance in both disordered eating and BD.
Limitations and Future Research
Although this study advanced the research on factors related to male body image in several ways, there are limitations that should be noted. To begin with, the measures administered consisted of self-report questionnaires. It is possible that responses given may not reflect the true feelings of the individuals but are representative of social desirability. Along the same lines, prior studies have shown that self-reported height and weight in adolescents may also be subject to social desirability (Elgar et al. 2005). Future studies should aim to include actual measurements of height and weight in order to test the validity of self-reported BMI of Spanish male adolescents. In addition, the sample consisted in secondary school-aged males, thus the results may not be generalizable to other samples. It is important to determine whether this measure is reliable with other diverse groups of males including males from other socioeconomic classes, preadolescents, adult males, male athletes, or competitive male body builders.
Conclusions
Overall, the Spanish version of the MBAS, best represented by a two-factor structure, presents good reliability and satisfactory concurrent validity, while also raising some interesting questions regarding the discriminant validity of the instrument and the appropriateness of using measures specifically constructed for males to assess their gender-specific body image concerns and related distress. All this allows for the use of the MBAS-S in Spanish adolescent males who report body image concerns. It would be advisable in the future to conduct research aimed at testing the stability of the MBAS-S through an examination of its test–retest reliability as well as to generalize its use in other clinical samples.
Footnotes
Acknowledgments
Dr. Sepúlveda has a postdoctoral Ramon and Cajal scholarship from the Spanish Ministry of Science and Innovation (RYC-2009-05092). Dr. Anastasiadou was awarded with a Research Fellowship for students of PhD Programs distinguished with Mention of Excellence. Ms. Blanco was awarded with a Research Fellowship (FPU) for students of PhD Programs. We express our gratitude to all the students, school headmaster, and teachers who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.