
Abstract
Check-in check-out (CICO) is a widely implemented program aimed at increasing prosocial behavior. Aligned with the logic of Tier 2 supports, CICO has a standard protocol meant to be implemented in a standardized fashion across all students. However, as CICO is not effective for all at-risk students, it is quite common to find researchers implementing adapted versions of CICO. The purpose of this review was to explore the types of, rationale for, and timing of adaptations made to CICO. Results showed that 71% of studies using CICO made adaptations to core components. While most of these adaptations were made at the onset of treatment, we found little evidence to suggest researchers had a systematic process for selecting adaptations. As schools continue to seek the most efficient and effective means to provide behavior supports to students, adaptive intervention planning is an important process to consider.
Schoolwide Positive Behavior Support (SWPBS) is a framework organized as a continuum of evidence-based supports aimed to target a variety of behavioral concerns (Sugai & Horner, 2010). The three tiers of the framework, each with increasing levels of intensity of support, include Tier 1 (universal), Tier 2 (targeted), and Tier 3 (intensified, individualized). Schools collect and use data to determine the necessary level of support students need and allocate resources along the continuum as appropriate. Ideally, schools implement this framework flexibly within the context of their individual school system. As such, SWPBS is a conceptual framework rather than a curriculum standardized across all schools. Historically, much of the SWPBS literature centers around effectiveness of Tier 1 (Colvin, Kameenei, & Sugai, 1993; Simonsen, Fairbanks, Briesch, Myers, & Sugai, 2008) or Tier 3 supports (Gage, Lewis, & Stichter, 2012). More recently, however, research on Tier 2 interventions has expanded (Bruhn, Lane, & Hirsch, 2014; Rodriguez et al., 2015).
Tier 2 Interventions
Within the SWPBS framework, Tier 2 interventions provide targeted support to students who are nonresponsive to Tier 1 universal supports. The importance of Tier 2 interventions is not trivial given that up to 15% of a school’s population may need Tier 2 supports (Sugai & Horner, 2010). Tier 2 interventions are provided in the form of standardized programs aimed to address the needs of multiple students at once, making them highly efficient and feasible (C. M. Anderson & Borgmeier, 2010). Examples of Tier 2 behavioral interventions include Check-In Check-Out (CICO; Crone, Hawken, & Horner, 2010), Check and Connect (A. R. Anderson, Christenson, Sinclair, & Lehr, 2004), social skills training (C. R. Cook et al., 2008), and self-monitoring (Bruhn et al., 2014).
Traditionally, students receive Tier 2 supports when they are nonresponsive to Tier 1 supports. In a similar fashion, students who are nonresponsive to Tier 2 supports are recommended for Tier 3 supports. However, recent conceptualizations in the literature describe Tier 2 as a continuum within itself that can provide a range of supports, from group to individualized, that still align with Tier 2 practice (Wehby & Kern, 2014). We propose that the process of adapting Tier 2 interventions, and documenting empirical evidence that supports those adaptations, represents best practice in multitiered systems of behavioral support.
Adaptive Interventions
One method for implementing a continuum of supports within Tier 2 is through the use of adaptive interventions. Adaptive interventions are grounded in the concept of data-based individualization (DBI). Originating from work by Deno and Mirkin (1977), a DBI process uses data to modify academic and behavioral supports for students who are nonresponsive to standardized programs. In the context of Tier 2 behavioral interventions, the DBI process begins by adapting elements of the standard protocol (Kern & Wehby, 2014). The use of adaptations allows school staff to adjust or tailor a standard Tier 2 protocol before the need for an intensive, individualized program arises. Recently, Fuchs, Fuchs, and Malone (2017) proposed a framework for intensifying standard protocol Tier 2 interventions that is consistent with the concept of adapting interventions to promote within tier intensification. While the framework proposed by Fuchs et al. focuses mainly on academic interventions, the same principles can be applied to Tier 2 interventions that target social behavior in schools.
Adapted Tier 2 Versus Tier 3
Despite a recent focus on individualizing Tier 2 interventions, historically, researchers applied such individualizations to Tier 3 interventions. Tier 3 behavioral interventions typically start with a functional behavioral assessment (FBA) and result in a behavior intervention plan that consists of many individualized behavioral supports (Crone, Hawken, & Horner, 2015). This process often requires additional personnel for assessments plus added time for training and implementation of the interventions. In summary, Tier 3 requires resources above and beyond what is offered at Tier 2. However, adapted Tier 2 programs rely on the notion that small, but meaningful changes can be made to enhance existing programs, often requiring little to no added resources. Therefore, adapted Tier 2 interventions use the logic of Tier 3 individualizations while maintaining the feasibility and efficiency of Tier 2 supports.
CICO and Adaptations
CICO, also referred to as the Behavior Education Program (BEP; Crone et al., 2010), is a commonly studied Tier 2 intervention (Bruhn et al., 2014). The core components of CICO include a daily morning check-in session with an adult mentor, the use of a daily progress report (DPR) outlining behavioral expectations and a daily point goal, teacher feedback on the DPR after each class period, a daily afternoon check-out with the mentor, and parent communication.
Current research shows CICO can increase appropriate classroom behavior (Campbell & Anderson, 2011; Dart et al., 2015; Miller, Dufrene, Sterling, Olmi, & Bachmayer, 2015) and decrease problem behavior (Campbell & Anderson, 2011; Hawken & Horner, 2003; Miller et al., 2015). For example, Miller, Dufrene, Olmi, Tingstrom, and Filce (2015) implemented CICO with three elementary school students and reported a functional relation between the implementation of CICO and a decrease in participants’ problem behavior and an increase in participants’ academic engagement. Although the majority of research has been conducted in elementary school settings, the published literature base also shows effectiveness across middle school grade levels (Hawken, Bundock, Kladis, O’Keeffe, & Barrett, 2014). In one such study, Simonsen, Myers, and Briere (2011) implemented CICO with students in an urban middle school. Authors selected students based on high rates of office discipline referrals (ODRs) or teacher referral for exhibiting problem behavior in the classroom. Teachers implemented manualized CICO with 21 students. After 6 weeks, the students who received CICO exhibited significantly less off-task behavior than the control group.
Despite examples of CICO effectiveness for groups of students, the literature includes examples of studies where 22% or more participants are considered nonresponders to standard CICO (Fairbanks, Sugai, Guardino, & Lathrop, 2007; Swoszowski, McDaniel, Jolivette, & Melius, 2013). Based on these findings, it is unsurprising that researchers are implementing adapted versions of CICO. One strategy for adaptation is to link CICO to the function of problem behavior. For example, Fairbanks et al. implemented manualized CICO with 10 second graders. After initial implementation, four out of 10 students were nonresponsive to the standard protocol. The researchers used FBA data to make function-based adaptations for this subset of students. Compared with standard CICO, the function-based CICO led to further reductions in problem behavior.
In another example, McIntosh, Campbell, Carter, and Dickey (2009) explored the differential effectiveness of CICO for students with escape- versus attention-maintained problem behavior. Teachers implemented the manualized CICO program for 8 weeks with 34 elementary students. Using the Functional Assessment Checklist for Teachers and Staff (FACTS; March et al., 2000), authors analyzed pretest and posttest data using a mixed model multivariate analysis of variance. On measures of problem behaviors, prosocial skills, and ODRs, students with attention-maintained problem behavior exhibited a statistically and clinically significant decrease in problem behaviors and ODRs and exhibited a statistically and clinically significant increase in prosocial behavior. On these measures, researchers did not find any statistically significant changes for students with escape-maintained problem behavior. Finally, Boyd and Anderson (2013) implemented the Breaks are Better (BrB) program within the context of CICO to teach elementary students with problem behavior maintained by escape from academic tasks how to appropriately request breaks from work. For all three participants, this adaptation resulted in the lowest level of problem behavior.
In addition to using function of problem behavior to make adaptations to CICO, researchers have adapted Tier 2 interventions to address social skills deficits (Collins, Gresham, & Dart, 2016; Ross & Sabey, 2015) or internalizing problem behaviors (Dart et al., 2015). Collins et al. (2016) utilized a peer-mediated version of CICO for students whose scores on a sociometric rating scale indicated they were socially neglected. To help improve social skills and social status, teachers assigned the students to attend check-in and check-out with a student who had a popular sociometric rating. This peer-mediated adaptation of CICO resulted in increased scores on the sociometric rating and consistently more points earned on the DPR for all students than during baseline.
Purpose
Given the presence of adaptations to CICO described in the literature, as well as the potential for such interventions to bridge the gap between Tiers 2 and 3 and reduce the need for highly intensive Tier 3 intervention, it is important to understand (a) the strength of the research base and (b) when and how researchers make decisions about adaptations. Although three recent CICO reviews (Klingbeil, Dart, & Schramm, 2019; Maggin, Zurheide, Pickett, & Baillie, 2015; Wolfe et al., 2016) provided detail on the presence of function-based adaptations, none systematically explored the presence of additional adaptations or document parameters of implementation. Therefore, the purpose of this review was to evaluate the entire CICO research base to ascertain the type of adaptations made, the timing and rationale for adaptations, and the quality of studies implementing adaptations. We sought to answer the following research questions:
Method
Search Procedures
Article identification
This review was a collaborative effort across researchers at two universities (Vanderbilt University [Site A] and Lehigh University [Site B]). Due to access to different electronic databases (Lemons et al., 2016), each site conducted independent searches using the same search terms and procedures to ensure they identified all potential articles. In the fall of 2017, researchers at Site A searched PsycINFO, ERIC, and ProQuest Central Education using search terms “tier 2” OR “BEP” OR “Behavior Education Program” OR “CICO” OR “Check In Check Out” OR “Check-In-Check-Out” OR “Check-In/Check-Out” OR “Check-In, Check-Out.” After eliminating duplicates, this search produced a total of 1,407 articles. At Site B, researchers searched PsycINFO, ERIC, and Education Research Complete using the same search terms. Again, eliminating duplicates, the search yielded a total of 1,053 articles (see Figure 1). Both sites also looked for additional studies from the reference lists of recent reviews on Tier 2 or CICO (Bruhn et al., 2014; Maggin et al., 2015; Wolfe et al., 2016). This led to the identification of three additional records at Site A and 46 additional records at Site B. Based on the feedback from reviews, Site A conducted an additional search to identify studies implementing Check, Connect, and Expect (CCE) because that intervention is a close variation of CICO. To locate these articles, researchers conducted an electronic database search using the same procedures outlined above and including the terms “Check, Connect, and Expect” to ensure they located all relevant articles. This search yielded one additional article.

Diagram showing the screening process.
Abstract screening
At each site, doctoral students served as coders to independently review the abstract of each article identified from the initial search (see Figure 1). Researchers included articles for further screening if the abstract mentioned BEP, CICO, Tier 2 programs, or an intervention that used a DPR. Furthermore, the coders excluded articles if the abstract indicated it was a medical study, an academic intervention study, or was unrelated to CICO or BEP. Two coders at each site independently screened abstracts according to these inclusion criteria to ensure interrater reliability (IRR). A third coder reviewed all disagreements and made the final decision to include or exclude. This procedure resulted in a total of 169 articles eligible for full-text screening at Site A and 104 at Site B.
Full-text screening
At each site, two coders independently screened full texts to determine whether they met the inclusion/exclusion criteria. Included articles had to implement CICO/BEP. Therefore, researchers included studies utilizing the CCE program. Researchers excluded studies examining one or partial components of CICO/BEP/CCE (e.g., Daily Behavior Report Card) without implementing the full program. In addition, studies had to include at least one dependent variable measuring student behavior. Researchers excluded studies if the sole dependent measure was fidelity of CICO/BEP/CCE implementation or a similar teacher outcome. Finally, researchers excluded any dissertations or non-peer reviewed articles. Following the full-text screening, researchers at both sites cross-referenced the lists of studies, yielding 45 articles eligible for coding.
Content Coding
Coding procedures and training
Researchers developed a codebook with operational definitions for each coded variable (full operational definitions are available from first author). Next, researchers coded all articles for (a) adaptation type, (b) adaptation timing, (c) adaptation rationale, and (d) Council for Exceptional Children (CEC) quality indicators (QIs; B. Cook et al., 2014). For quality coding, researchers coded on the study level. For coding of adaptations, coders marked each participant as a separate unit in single-case design (SCD) studies (e.g., a study with three participants would have three columns of data, one for each participant). For group design, researchers considered the entire treatment group one unit.
The first author trained research coders on the codebook during a 1-hr training session. During this session, the first author reviewed the codebook and provided coders with definitions for each variable. Subsequently, coders practiced coding one article during the training, comparing responses with the trainer after coding. Coders then coded training articles independently until they met the criterion of at least 90% on one training article before coding independently. Researchers double-coded all articles for accuracy purposes. Coders settled all disagreements using consensus coding. The mean IRR across all studies was 95.57% agreement (range = 81.4%–100%).
Adaptation type
Researchers coded adaptations when variations were made to any of the five components of standard CICO/BEP protocol as described by Crone et al. (2010). The first component is a daily morning check-in with an adult mentor. During this meeting, the mentor reviews the behavioral expectations and sets a daily goal for the day (i.e., 80% of possible points). The second component is the student’s DPR, which is a sheet that outlines the behavioral expectations. These expectations are based on the SWPBS expectations or classroom rules and consistent across all students receiving CICO. The third component is teacher feedback at the end of each class/period throughout the school day. The fourth component is an afternoon check-out with the mentor to debrief and evaluate the day. During this meeting, the mentor tallies up the student’s points to determine whether the student met his or her goal and, if so, provides positive reinforcement/verbal praise and a reward. The final component includes parent communication. The DPR is sent home nightly for a parent/caregiver to sign and the student returns it the next day.
Using this definition of the standard protocol noted above, researchers coded all adaptations to the standard protocol. Following the initial coding of adaptations, researchers categorized all adaptations by CICO component (i.e., check-in or check-out, DPR, teacher feedback, parent communication). Researchers used these categories to report the presence of adaptations in the CICO literature.
Check-in or check-out
Researchers coded an adaptation to the check-in or check-out procedure if there was any change to the procedures or individuals present during these meetings. This included a change to a peer mentor, an increase or decrease in the frequency of the meetings (e.g., addition of a midday check-in, only a check-out session provided), or a change in the process of daily goal setting (i.e., if goals varied from 80%). This adaptation did not include variations to the teacher feedback provided after each class/period.
DPR
Researchers coded an adaptation to the DPR when the behavioral expectations on the DPR were altered or if any additional information was added to the DPR (e.g., routines for taking a break or asking for help).
Teacher feedback
Researchers coded an adaptation to teacher feedback when the frequency of the feedback from the teachers was altered. This included an increase in teacher feedback (e.g., the DPR was filled out every 30 min) or a decrease in teacher feedback (e.g., the DPR was filled out every other period instead of every period).
Parent communication
Researchers coded an adaptation to parent communication when a change to the procedures for sending the DPR home was made. This included removing the parent communication or training parents in methods to provide behavior-specific feedback to their child.
Adaptation timing
Researchers also coded timing and rationale for selecting each adaptation. Researchers coded the timing of the adaptation as Onset of Intervention if the adaptation was implemented during the initial intervention phase in a study, After Inadequate Response if the adaptation was implemented following student nonresponsiveness to an initial intervention phase (typically standard protocol), or After Successful Intervention if the adaptation was implemented due to student responsiveness to the intervention (e.g., intervention fading).
Adaptation rationale
Researchers coded the rationale, or decision as to why researchers chose each adaptation, as Data-Based at Baseline when the decision was based on formal assessment or observational data collected at baseline (e.g., direct observation, FBA, standardized assessments or rating scales, DPR data, or ODR data); Nonresponsiveness to Intervention when data (e.g., direct observation, formal assessment, FBA, standardized assessments or rating scales, ODR data, or DPR data) indicated a student was nonresponsive to initial intervention; Responsiveness to Intervention when the aforementioned data indicated responsiveness; and Research Related when adaptations were selected a priori as part of a specific research design or replication study.
Study Quality
The CEC quality standards include ratings across the following eight domains: (a) context and setting, (b) participants, (c) intervention agent, (d) description of practice, (e) implementation fidelity, (f) internal validity, (g) outcome measures, and (h) data analysis (B. Cook et al., 2014). Each domain is made up of one or more sub-categories—each representing one QI (see Table 2 for a list of all QIs). In total, the CEC standards include 28 QIs. The QIs are tailored to address either group design or SCD research. While the CEC criteria are typically a 0 for “did not meet” and a 1 for “did meet”, this is a highly conservative approach and does not capture any partial implementation of a QI. Researchers in previous reviews have adapted the quality criteria for the CEC standards (e.g., Lane, Kalberg, & Shepcaro, 2009). In this study, we defined a coding scale of 0 to 2 for each indicator. We assigned a score of 0 when the indicator was not present or was present at an unacceptable level. We assigned a score of 1 when an indicator was present but not at the highest quality level. Finally, we assigned a score of 2 when the QI was present and met or exceeded the CEC standard. For example, the QI 2.1 asks for a description of demographic variables relevant to the review. If a study provided descriptions of age, race, gender, and socioeconomic status for all participants, it received a score of 2. If the study failed to include at least one of those items, it earned a score of 1. If the study failed to describe two or more of the items, it received a score of 0. Researchers coded each QI for each study and summarized the results on the study level and the QI level.
Two independent coders evaluated all studies for quality. The first author calculated IRR using an exact agreement method and all agreements reflect an exact match in QI score between the coders. The mean IRR across all QIs was 86.07% (range across QIs: 60.0%–100%). The QI with the lowest IRR was QI 6.9, which required coders to determine whether differential attrition between groups was low or controlled for in the statistical analyses. Due to low IRR across some QIs, coders used consensus agreement to code all discrepancies between the two coders.
Results
We identified a total of 45 articles that implemented CICO. Of those articles, 33 experiments across 32 articles made adaptations to the standard protocol of CICO.
Overall Summary of Articles Identified
It is important to note that most studies implemented multiple adaptations to the standard protocol of CICO simultaneously. As a summary, across identified studies, 29 studies made changes to the check-in and/or check-out component, 12 studies made changes to the DPR component, 16 studies made changes to the teacher feedback component, four studies made changes to the parent component, and five studies added a component to CICO that was not part of the standard protocol (e.g., self-monitoring).
Adaptations by Participant
Several studies implemented different combinations of adaptations to CICO across participants. In addition, many participants experienced multiple adaptations to a single component of CICO (e.g., two adaptations to the check-in component). For ease of interpretation, we also aggregated adaptations at the participant level. Across 33 included experiments, there were 106 total participant units (note: for group design studies, each treatment group was considered one unit). Similar to results on a study level, Figure 2 shows most participants experienced more than one adaptation to the standard protocol of CICO. As Figure 3 shows, participants most commonly experienced adaptations to the check-in component, teacher feedback component, and check-out component of CICO. On a global level, studies made a total of 304 adaptations across CICO components. Coders found adaptations to the check-in component for 92 participants (86.8%) and adaptations to the check-out component for 48 participants (45.3%). In addition, coders found adaptations to the DPR component for 32 participants (30.2%), the parent or home communication component for 12 participants (11.3%), and a component added to the standard protocol of CICO for 15 participants (14.2%). It is important to note that many participants received multiple adaptations per component (e.g., two adaptations to teacher feedback). Therefore, counting multiple adaptations per component category for each participant, researchers made a total of 304 adaptations across participants.
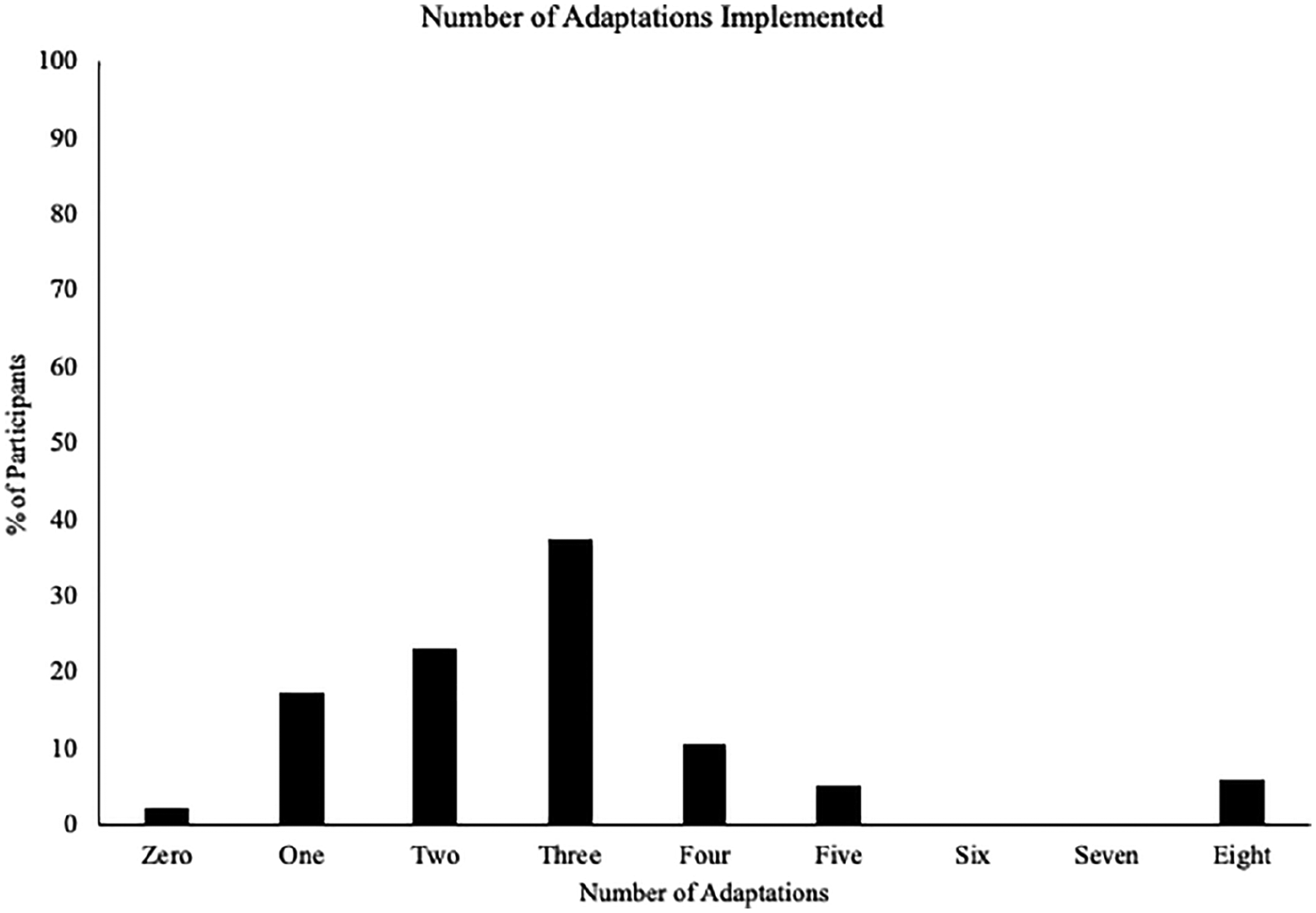
Total participant units =105.
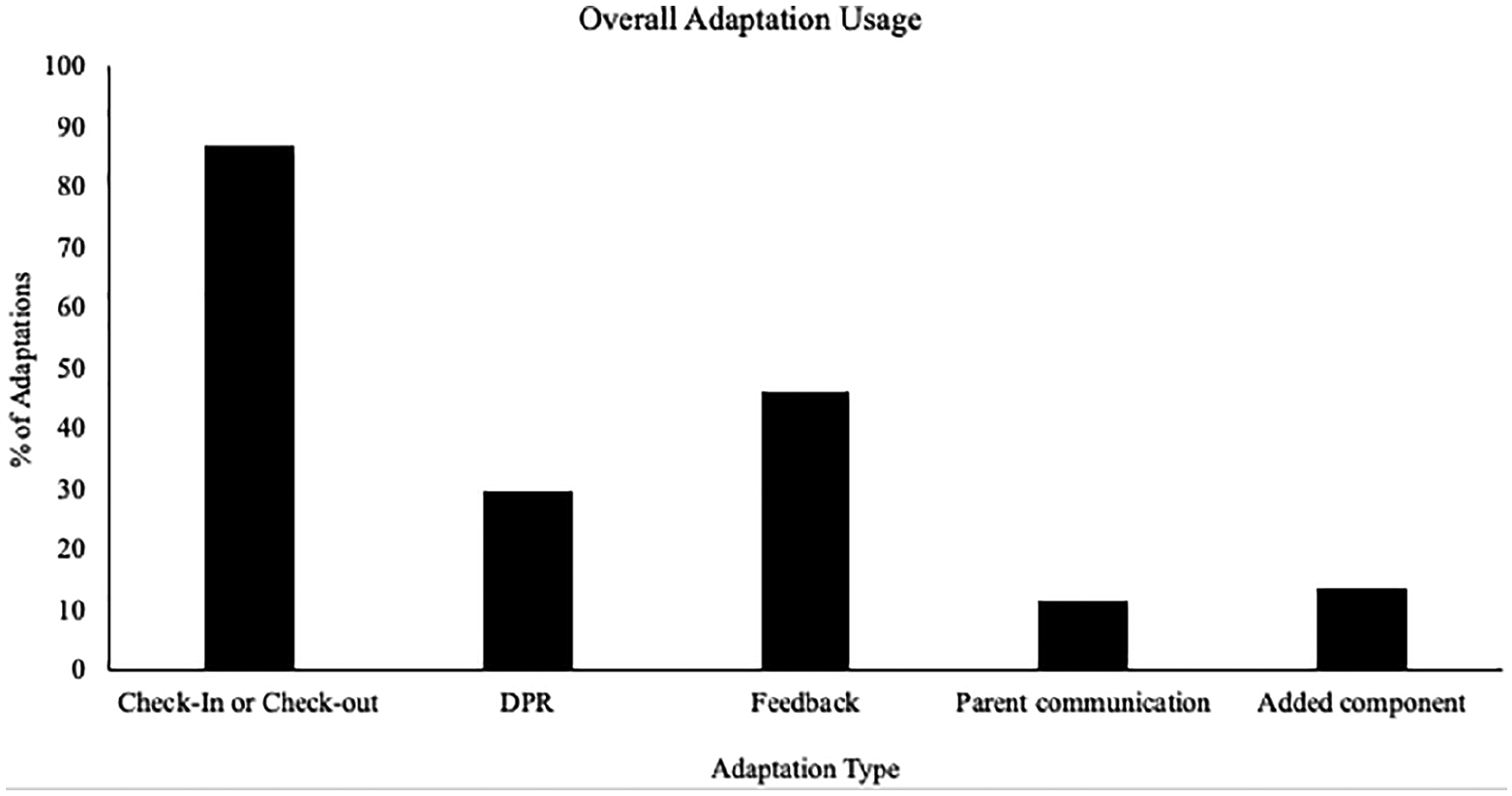
These numbers reflect a global analysis of adaptations made to each component by participant (n = 196 adaptations).
Adaptation Timing
As noted above, most participants experienced multiple adaptations to the standard protocol of CICO. For this reason, researchers coded the timing and rationale for each individual adaptation made in a study. The cumulative 106 participants experienced 304 total adaptations to the standard protocol of CICO. Of these adaptations, it was most common for adaptations to occur at the onset of treatment (74.3% of adaptations, n = 226). Researchers made a smaller number of adaptations (15.5%, n = 47) after successful treatment (e.g., fading) or after inadequate response (9.9%, n = 30; see Figure 4). The timing of one adaptation was not reported.

Reported by adaptation units (n = 300).
Adaptation type: Before implementation
Of adaptations made at the onset of treatment, researchers made changes to check-in or check-out sessions most often (64.6% of adaptations, n = 146; see Table 1). Researchers also made adaptations to the teacher feedback component (12.8% of adaptations, n = 29), the DPR (11.9% of adaptations, n = 27), and the home component (6.2% of adaptations, n = 14) at the onset of treatment.
Adaptations by Timing.
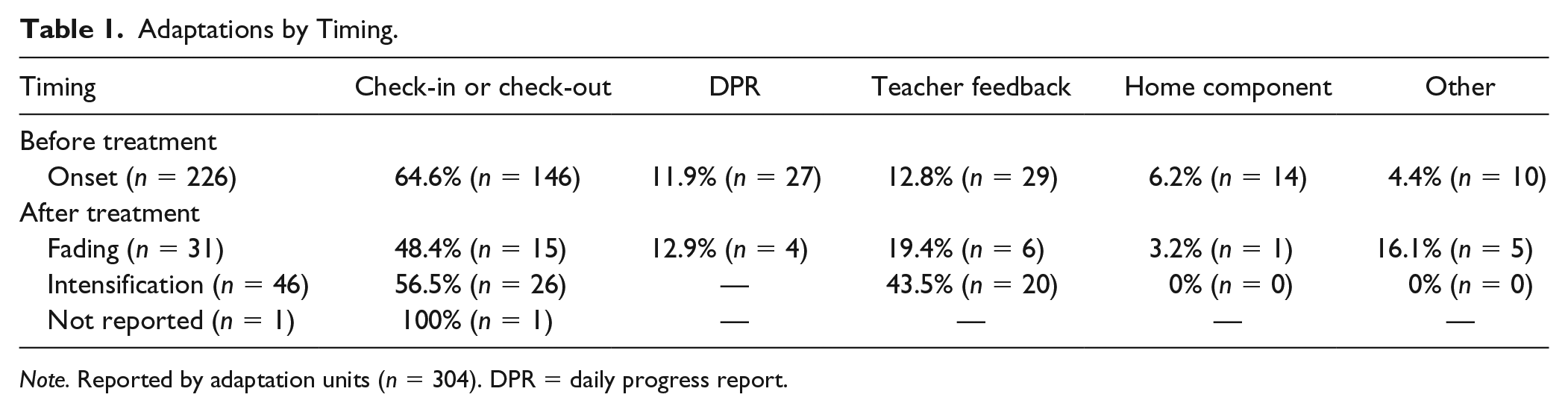
Note. Reported by adaptation units (n = 304). DPR = daily progress report.
Check-in or check-out
Across adaptations made at the onset of treatment, the most common procedure for adapting check-in was the use of a peer mentor (e.g., Collins et al., 2016; Dart et al., 2015; Melius, Swoszowski, & Siders, 2015; Sanchez, Miltenberger, Kincaid, & Blair, 2015; Smith, Evans-McCleon, Urbanski, & Justice, 2015). In these studies, a peer rather than an adult in the school served as the mentor and conducted check-in and check-out sessions with the target student.
Aside from using a peer mentor, several studies added a component to the check-in sessions. Examples included a brief social skills lesson (e.g., C. R. Cook et al., 2015), a homework check or time for students to complete homework before going to class (e.g., Turtura, Anderson, & Boyd, 2014), and reinforcement for attending check-in sessions or having materials ready for class (e.g., Boyd & Anderson, 2013; Mong, Johnson, & Mong, 2011). Another component adapted during check-in was the goal-setting procedure. Some studies modified students’ point goals from the 80% of points specified in the CICO manual (e.g., Dart et al., 2015).
Adaptations made to check-out sessions, such as the use of peer mentors, were in many cases similar to those made to check-in sessions. In addition, some studies added components to check-out sessions such as a homework planner check (e.g., Turtura et al., 2014). A final adaptation made to check-out sessions included altering the rewards provided to students at check-out, such as adding longer term contingencies or providing function-based rewards.
DPR
Several studies altered DPR behavioral expectations, tailoring the expectations to address individual concerns of target students (e.g., Collins et al., 2016; Hunter, Chenier, & Gresham, 2014; Miller, Dufrene, Olmi, et al., 2015; Miller, Dufrene, Sterling, et al., 2015; Smith et al., 2015; Sobalvarro, Graves, & Hughes, 2016; Turtura et al., 2014). For example, Collins and colleagues (2016) worked with students’ teachers to select five target behaviors for each student based on items from the Social Skills Improvement System-Rating Scales (SSIS-RS; Gresham & Elliot, 2008). Additional adaptations to the DPR included adding components to the DPR form (e.g., Boyd & Anderson, 2013). Boyd and Anderson (2013) taught students with escape-maintained problem behaviors a routine for requesting a break. Researchers printed this break routine on the back of the DPR for students to refer to during class.
Teacher feedback
Some studies adapted the teacher feedback component of CICO at the onset of treatment. For example, in one study, teachers provided praise and feedback to students based on completion of a homework tracker. Teachers provided this feedback in addition to feedback on behavioral expectations at the end of each class period (Turtura et al., 2014).
Parent communication
A small number of studies made adaptations to the parent component of CICO. Adaptations to this component included providing explicit training to caregivers about CICO (e.g., Turtura et al., 2014), asking parents to provide home-based incentives based on CICO points (Campbell & Anderson, 2011), or removing this component in schools in which parent involvement was low (McDaniel & Bruhn, 2016).
Adaptation type: After treatment
As with adaptations made at the onset of treatment, researchers made changes to check-in or check-out sessions most often across adaptations made after the start of treatment (53.2% of adaptations, n = 42). Researchers also made adaptations to the teacher feedback component (33.8% of adaptations, n = 26), the DPR (5.2% of adaptations, n = 4), and the home component (1.3% of adaptations, n = 1) after treatment.
Check-in or check-out
Several studies adapted check-in or check-out sessions due to student responsiveness. Across adaptations made after treatment, researchers commonly adjusted students’ goals over time based on performance (e.g., Collins et al., 2016; Dart et al., 2015; Fairbanks et al., 2007; Lane, Capizzi, Fisher, & Ennis, 2012; McDaniel & Bruhn, 2016; Pool, Carter, & Johnson, 2013). In addition, some studies added a midday check-in to the CICO standard protocol. For example, Swoszowski and colleagues (2013) added a midday check-in for students who were nonresponsive to the standard protocol of CICO.
DPR
Some studies altered DPR behavioral expectations after initial treatment (e.g., Fairbanks et al., 2007; Pool et al., 2013). For example, Fairbanks and colleagues (2007) adapted expectations based on the function of students’ problem behavior after students showed initial nonresponsiveness to the standard protocol of CICO.
Teacher feedback
Several studies adapted the feedback component of CICO after initial treatment by altering the frequency of feedback or the person delivering feedback (e.g., Campbell & Anderson, 2011). For example, Campbell and Anderson (2011) conducted a component analysis, gradually reducing the amount of teacher feedback students received as a method of fading the CICO intervention following student responsiveness. Several studies adapted CICO by having students rate their own behaviors on the DPR as a form of self-monitoring, rather than receiving direct feedback from a teacher (e.g., Cheney et al., 2009; Miller, Dufrene, Olmi, et al., 2015; Miller, Dufrene, Sterling, et al., 2015). In each of these studies, students self-monitored their behavior on the DPR after they showed responsiveness to CICO.
Parent communication
One study made an adaptation to the parent component of CICO after treatment. Sanchez and colleagues (2015) removed the parent component of CICO after students received at least 80% of their points on the DPR for 5 consecutive days.
Adaptation Rationale
Of 304 adaptations, researchers made the largest percentage (47%, n = 143) of adaptations based on data collected during baseline (typically multiple sources). Of these 143 adaptations, 44.1% (n = 63) used FBA data, 33.6% (n = 48) used standardized assessments such as the Social Skills Rating System (SSRS; Gresham & Elliot, 1990) or Systematic Screening for Behavior Disorders (SSBD; Walker & Severson, 1992), 14% (n = 20) used DPR data, 2.8% (n = 4) used a combination of direct observation and DPR data, and 5.6% (n = 8) used other forms of data to inform adaptations. For a smaller number of adaptations, researchers chose based on student nonresponsiveness (8.9%, n = 27) and student responsiveness (12.5%, n = 38) to intervention. Across these studies, the measurement for student nonresponse consisted of direct observation data (33.3%, n = 9), DPR data (33.3%, n = 9), a combination of school data and DPR data (3.7%, n = 1), or a combination of direct observation data and clinical judgment (29.6%, n = 8). The measurement of student responsiveness to CICO consisted of direct observation data (28.9%, n = 11), DPR data (60.5%, n = 23), and a combination of direct observation and DPR data (10.5%, n = 4). Finally, researchers made 31.3% of adaptations (n = 95) without a data-based rationale. Researchers made 25 of these adaptations for research-related reasons (e.g., systematic replication, to address a specific research question, social validity). The remaining 70 adaptations were not reported or did not fall into one of our coded categories.
Study Quality
Researchers present the average QI score across studies in Table 2. Researchers applied self-established criterion for determining whether a study was of high quality. To be considered high quality, a study needed to earn at least 75% of possible points across all QIs (44 possible points for SCD studies and 46 possible points for group design studies). Using this researcher created threshold, 12.5% of single-case studies (n = 4) were considered high quality. None of the group design studies exceeded the 75% criterion. On average, across QIs, studies received lower scores for setting descriptions, descriptions of the role of the interventionist, and descriptions of the training required for the intervention. Across these indicators, more than half of included studies received a quality score of 0. Studies received higher quality scores for descriptions of dependent variables and indicators related to reporting outcomes.
Average Across QIs.
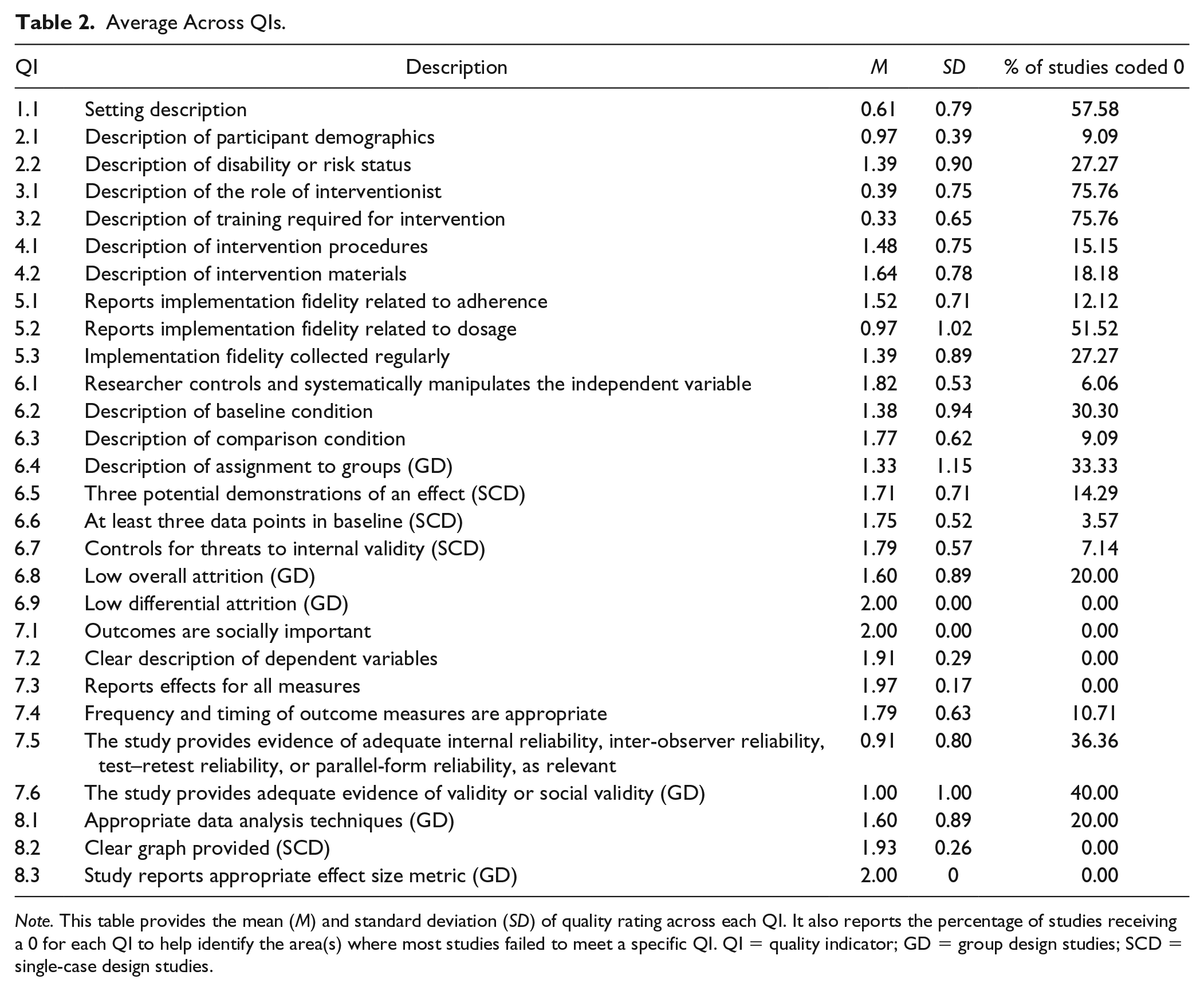
Note. This table provides the mean (M) and standard deviation (SD) of quality rating across each QI. It also reports the percentage of studies receiving a 0 for each QI to help identify the area(s) where most studies failed to meet a specific QI. QI = quality indicator; GD = group design studies; SCD = single-case design studies.
Discussion
The purpose of this review was to evaluate the existing literature base on CICO to determine the type of adaptations made to the core components of CICO (check-in, DPR, teacher feedback, check-out, parent communication), the timing and rationale of each adaptation, and the overall quality of studies implementing adaptations. Our work extends the literature base by providing a deeper examination into how and why adaptations are selected for a commonly implemented Tier 2 intervention.
Although Tier 2 interventions are primarily intended to be delivered as a manualized program that is standardized across all students, we found the overwhelming majority of CICO articles published to date made adaptations to the standard protocol (71%). Of the studies that made an adaptation, researchers made 304 adaptations across the 106 participant units. This indicates that researchers were most likely to implement CICO with multiple adapted components. The majority of adaptations were embedded within the core components of CICO and could be implemented with few additional resources. Examples included changes to the goal-setting procedures, an alteration to the physical content of a DPR by adding visual aids (e.g., a box reminding students of the steps required for asking for and taking a break during class), or tailoring the definitions of the behavioral expectations. These adaptations were embedded within preexisting CICO components. On the contrary, some adaptations maintained the structure of the standard components but required additional training. Examples included training a peer to serve as the mentor or training the target student to self-monitor. Although less common, a few studies added programs or components that required an increase in the amount of time a mentor spent with a student. Examples of these adaptations included adding a midday check-in, extending the length of check-in time to include a mini social skills lesson, or use of an activity-based reward for achieving long-term goals (e.g., 15 min to play basketball with a peer).
When evaluating the timing of each adaptation, we found most adaptations were made at the onset of treatment, rather than due to student nonresponse or successful response to intervention. This finding raises an interesting point. Given that a majority of the participants in CICO studies received an adapted version of the program at the onset of intervention, it may be difficult to accurately estimate the number of nonresponders to the standard version of CICO. Furthermore, these results may corroborate evidence to suggest that researchers use an assessment of student characteristics, such as function of behavior, to adapt interventions prior to the start to increase the likelihood of response (March & Horner, 2002; McIntosh et al., 2009); thus, applying adapted procedures from the start may be an efficient way to implement Tier 2 programs such as CICO.
Evidence from our evaluation of the rationale for selecting adaptations from the onset of treatment corroborates the use of student-level variables to guide adaptation selection and implementation. About half of the studies used student data (e.g., function of problem behavior, social skills ratings, or baseline DPR data) to choose an adaptation, both at the onset of intervention and due to student nonresponse. For example, Boyd and Anderson (2013) evaluated function to make adaptations (i.e., request breaks from instruction) for students with escape-maintained behavior. In addition to being an adaptation from the onset, this also highlights the use of data to inform the selection of an adaptation.
Another subgroup of studies implemented adaptations during treatment. Some studies developed a priori decision rules to systematically monitor data and apply adaptations due to student response or nonresponse. These adaptations aimed to intensify the procedures due to student nonresponse or fade the procedures due to student response. For example, Cheney and colleagues (2009) increased the intensity of CICO by adding academic tutoring sessions and social skills lessons for students who did not meet their daily point goal for 2 consecutive weeks. On the contrary, they decreased the intensity of CICO by implementing self-monitoring when a student met his or her goal on more than 80% of days over the course of 8 weeks. This exemplifies the use of adaptations to address student response patterns in either direction (i.e., response or nonresponse).
A final purpose of this review was to evaluate the quality of the literature base implementing an adapted version of CICO. Broadly, only a handful of studies met criteria for high quality while most fell below the threshold of 75% of points across QIs. The majority of SCD and group design studies failed to report sufficient information about the setting, intervention agents and training, and treatment fidelity.
Limitations
The results from this review should be interpreted with the following limitations in mind. To begin, the review of adaptations was descriptive in nature and looked at the entire CICO literature base, regardless of quality or design. A second limitation was the common implementation of multiple adaptations as a package rather than as individual components. Therefore, many researchers did not create experimental conditions that would allow for the analysis of effectiveness for individual adaptations. This inhibited our ability to determine the effectiveness of each type of adaptation (e.g., through visual analysis or calculation of effect sizes). A third limitation was the assessment of quality using the rigorous CEC standards. Although we coded all QIs on a scale of 0 to 2, our coding was highly conservative as we attempted not to infer any information from the studies. Finally, our assessment of adaptations, and more specifically the timing and rationale of adaptations, was limited to what was reported in the articles. Due to publication space constraints, authors may not have fully described their process for when and how they selected, implemented, and monitored adaptations.
Implications for Research and Practice
Despite the aforementioned limitations, the results provide valuable information about the large presence of adaptations in the CICO literature. Tier 2 behavioral interventions are intended to be delivered as a standard program and implemented in a similar manner across students (C. M. Anderson & Borgmeier, 2010). As such, these interventions are often touted as highly efficient and effective. Although CICO is a commonly used Tier 2 intervention, the standard protocol may be insufficient for as many as 22% of students (Swoszowski et al., 2013). Prior to jumping to a costlier and resource intensive intervention, it may be more pragmatic for practitioners to think broadly about ways to adapt CICO for students.
In most studies, researchers applied multiple adaptations to each participant’s CICO program. The application of adaptations as a package prohibits the determination of each adaptation’s effectiveness. Future, high-quality research is needed to individually evaluate the relative effectiveness of each adaptation. More specifically, based on our evaluation of study quality and rationale for selecting adaptations, we recommend reporting of adaptations should include more thorough descriptions of (a) the intervention agents and procedures used to train intervention agents on the interventions and adaptations, (b) the treatment fidelity of the adaptations, and (c) the decision-making process for selecting and monitoring the adaptations.
Finally, researchers overwhelmingly made adaptations in isolation without the use of a systematic process to guide decision making (i.e., DBI). Future research is also needed to develop and evaluate a systematic process to guide teams through decision making when making adaptations. As schools continue to seek the most efficient and effective means to provide behavior supports to students, adaptive intervention planning is an important process to consider.
Footnotes
Action Editor: Dan Maggin
Authors’ Note
Caitlyn E. Majeika, PhD, is now affiliated with University of North Texas and Colleen E. Commisso, PhD, is now affiliated with West Chester University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This review was supported by IES research grant # R324A160096.