
Abstract
Given the increasing number of individuals diagnosed with autism spectrum disorder (ASD), there is a critical need to develop programs that facilitate positive behavior outcomes during the transition to adulthood. Furthermore, many adults with ASD do not have access to intervention programs due to remote locations, lack of qualified personnel, and/or long waitlists. This study, conducted within the context of a combined multiple baseline and changing criterion design, examined the use of videoconferencing (VC) to provide intervention from a remote location. Results showed that following intervention participants were able to independently perform the targeted skills and all targeted skills maintained during follow-up probes. All participants rated the intervention highly and said that they would recommend the intervention to others. These results are discussed in relation to potential avenues to increase access to services for individuals with ASD, particularly in remote and underserved areas, using VC.
Keywords
As the population of adolescents and adults with autism spectrum disorder (ASD) continues to grow, so does the need for services and effective interventions that facilitate positive adaptive behavior outcomes in adulthood. Presently, only 17% of adults with ASD live independently (Cullen & Alber-Morgan, 2015). Unfortunately, many individuals with ASD display significant challenges with daily living skills (DLSs) relative to their cognitive abilities (Gray et al., 2014). Average DLS scores on the Vineland Adaptive Behavior Scales–Second Edition (VABS-II) are significantly lower compared with average IQ, and considerably below age expectations for adults with ASD (Bal et al., 2015; Duncan & Bishop, 2015; Farley et al., 2009). DLSs such as money management, personal hygiene, and meal preparation, are some of the crucial domains that are necessary for independent living and employment (Bal et al., 2015; Briggs et al., 1990).
Despite the wealth of literature elucidating these deficits for individuals with ASD, fewer studies have focused on interventions to ameliorate these challenges. Some notable publications include research by Smith and Belcher (1985), who adapted an intervention program for adolescents with intellectual disability (ID) (Horner & Keilitz, 1975) to guide adults with autism through task steps for tooth brushing, face washing, hair combing, cleaning the sink, and cooking spaghetti. Four out of five participants performed 100% of steps independently within 18 to 42 weeks (Smith & Belcher, 1985). More recently, Van Laarhoven and Van Laarhoven-Myers (2006) used a technology-mediated procedure (i.e., video rehearsal, photo prompts, and video prompts) to teach adolescents with ID and/or ASD in the school setting. While all three procedures were effective in improving target behaviors (i.e., cleaning a table, folding clothes, and microwaving a pizza), interventions with in vivo prompting led to faster acquisition, and participants completed the highest percentage of steps independently during video rehearsal/prompting conditions. Similarly, Mechling et al. (2009) used a personal digital assistant (PDA) and a system of least prompts procedure (i.e., task analysis, photo prompt, photo/audio prompt, video/audio prompt) to teach three adolescents with ASD to prepare recipes using a stovetop, microwave, and toaster oven. Participants performed less than 50% of steps independently at baseline and 100% of steps independently after intervention, requiring lower levels of prompting as the study progressed.
Such interventions encourage independent performance of DLS by shifting stimulus control from continuous caregiver management to individuals with ASD (Hume et al., 2009). However, further research is needed to develop strategies that will help adults with ASD improve DLS and use these skills independently in residential or employment settings once professional support is faded (Hume et al., 2009). For many programs, continued caregiver redirection or assistance is required for individuals with ASD to refrain from engaging in behaviors that interfere with daily living, work, or school activities and may be difficult to fade over time (Zandt et al., 2007). As a whole, the majority of DLS interventions for adolescents with ASD have been implemented in the school setting, using a classroom to simulate a home or work environment (Cullen & Alber-Morgan, 2015), leaving the issue of a lack of generalization unaddressed.
Telehealth, which employs internet and videoconferencing (VC) equipment to provide services from a distance (Higgins et al., 2017; Machalicek et al., 2016), has been used in recent years to increase access to behavioral services for individuals with ASD. Telemedicine programs, provided at a local telehealth studio with onsite assistance, have been used to assess individuals with ASD and train clinicians and family members to implement interventions (Barretto et al., 2006; Heitzman-Powell et al., 2014; Higgins et al., 2017; Parmanto et al., 2013; Reese et al., 2015; Schutte et al., 2015; Vismara et al., 2009; Wainer et al., 2017). While telemedicine programs are widely accepted, easy to use, and cost-effective compared with home-based services, limitations remain including the necessity to live near a telemedicine studio; expenses involving facility use, an onsite assistant, and family travel; and inability to deliver behavioral interventions in the natural setting (Aresti-Bartolome & Garcia-Zapirain, 2014; Lindgren et al., 2016; Machalicek et al., 2009). VC programs, which employ low-cost equipment and general-use software to provide community-based services without onsite assistance, have been used in home settings to assess children with ASD and provide parent training (Baharav & Reiser, 2010; Lindgren et al., 2016; McDuffie et al., 2013; Reese et al., 2015) and in school settings to provide staff training and follow-up consultation (Gibson et al., 2010; Machalicek et al., 2009). However, there is a scarcity of telehealth programs demonstrating techniques for providing direct interventions for individuals with ASD (Aresti-Bartolome & Garcia-Zapirain, 2014). To our knowledge, no previous studies have evaluated the usefulness of telemedicine or VC programs to deliver DLS interventions to individuals with ASD.
Therefore, the purpose of this study was to examine the usefulness of VC programs to help deliver DLS interventions to young adults with ASD. We asked the following research questions:
Method
Participant Selection
Three young adults diagnosed with ASD by a physician or neuropsychologist were referred to our university autism center for intervention and then selected to participate in this study due to their living arrangement and reliance on caregivers to complete DLS (see Table 1). Each participant had received services as a young adult through a state agency and exhibited challenges in the areas of communication, socialization, and perseverative or restricted interests. All participants were of average intelligence, could engage in conversation, and attended at least 80% of scheduled intervention sessions. The first author, who served as the clinician while enrolled as a PhD student in an education program, had received behavioral intervention training and had 6 years of experience implementing pivotal response treatment (PRT). Participants obtained study information from a flyer and met with the researcher before signing a university-approved human subjects consent form that specified use of a non-Health Insurance Portability and Accountability Act (HIPAA) compliant general-use VC software program (i.e., Skype). At no time during the intervention were the adults’ diagnoses mentioned or discussed. Pseudonyms were assigned for each participant.
Participant Characteristics.

Note. ASD = autism spectrum disorder.
Participant 1
Nolan, a Caucasian and Hispanic male, was 25 years old at the start of the study. He lived with his parents while working part-time and taking community college courses. Nolan’s mother described him as a “hoarder” and reported that he would not let anyone into his room; however, if guests were expected, he would allow one of his parents to come in his room and clean it with him. Baseline probes showed that Nolan was throwing trash and recyclable items on his floor and behind his desk. The floor was not visible in many areas, there was a large pile of items on top of his bed, and he was unable to access the back door of the room and the majority of his closet. Nolan was reluctant to get rid of items (e.g., an outdated schedule from a previous job, empty soda cans), and collected a number of old electronic items (for the unlikely possibility that they would be needed at a later time) including floppy disks, phone cords, and desktop computers. Nolan’s lack of organization skills had led to the loss of his online bank account password multiple times, resulting in late payments and overdrafts. Nolan also lost several items from work, including a set of keys and numerous receipts, leading to reported anxiety, loss of income, and lower job performance ratings from his supervisor.
Participant 2
Max, a Caucasian male, was 30 years old at the start of this study. Max attended a day program three mornings per week and lived with one roommate. He received 18 hr of support per day from support staff members in his home and community. Max’s mother reported that he was very fearful of burning himself on the stove/oven and using sharp knives and had never learned to cook. Baseline probes indicated that Max was able to pour contents from a bag into a bowl and microwave leftovers when prompted; however, he did not prepare any of his own meals independently. A food preference assessment revealed that more than half of his favorite foods (i.e., seafood) were not included in meals prepared by his support staff. Max’s roommate regularly used the oven to cook greasy foods (i.e., chicken/duck) and did not clean afterward, which had caused the smoke detector to alarm. Thus, his roommate dismantled the detector in place of cleaning the oven, leading to safety concerns for everyone in the house.
Participant 3
Peter, a Caucasian male, was 29 years old at the start of this study. He had received special education services throughout his life, but was mainstreamed in upper elementary school and received excellent grades in high school. After graduating from a 4-year university, Peter began working at a family business, living in a family member’s apartment during the week and staying with his parents on weekends. Peter reported that he had never done his own laundry. Despite anxiety about traffic, he drove several hours from his on-campus dormitory to bring laundry to his parents’ housekeeper each weekend. After graduation, he continued this practice despite repeated requests by his parents to wash his own laundry.
Setting
All sessions were implemented remotely through two free VC programs (i.e., Skype and FaceTime). The clinician used VC in her private office on a desktop computer with an external camera and speakers. Participants used VC in their home, which allowed them to engage in DLS learning in their natural settings and increased the likelihood of maintenance and generalization of the targeted behaviors. The VC program also eliminated the need for long-distance travel to access intervention at the clinic setting; round-trip mileage for Nolan, Max, and Peter was 38, 140, and 138 miles, respectively. Let alone, Nolan and Max did not drive, and public transportation to and from the clinic was limited.
Design
The VC intervention was conducted using a nonconcurrent multiple baseline (MBL) across participants design combined with a changing criterion design that ensured systematic advancement of each participant’s skills through treatment phases (Hartmann & Hall, 1976; R. L. Koegel et al., 2004). Baselines were carried out for three, five, and nine probes for the three adults, respectively. Progress to criterion was then replicated within the changing criterion portion of the design for each phase of the participants’ treatment plans.
Selection of DLS target behaviors
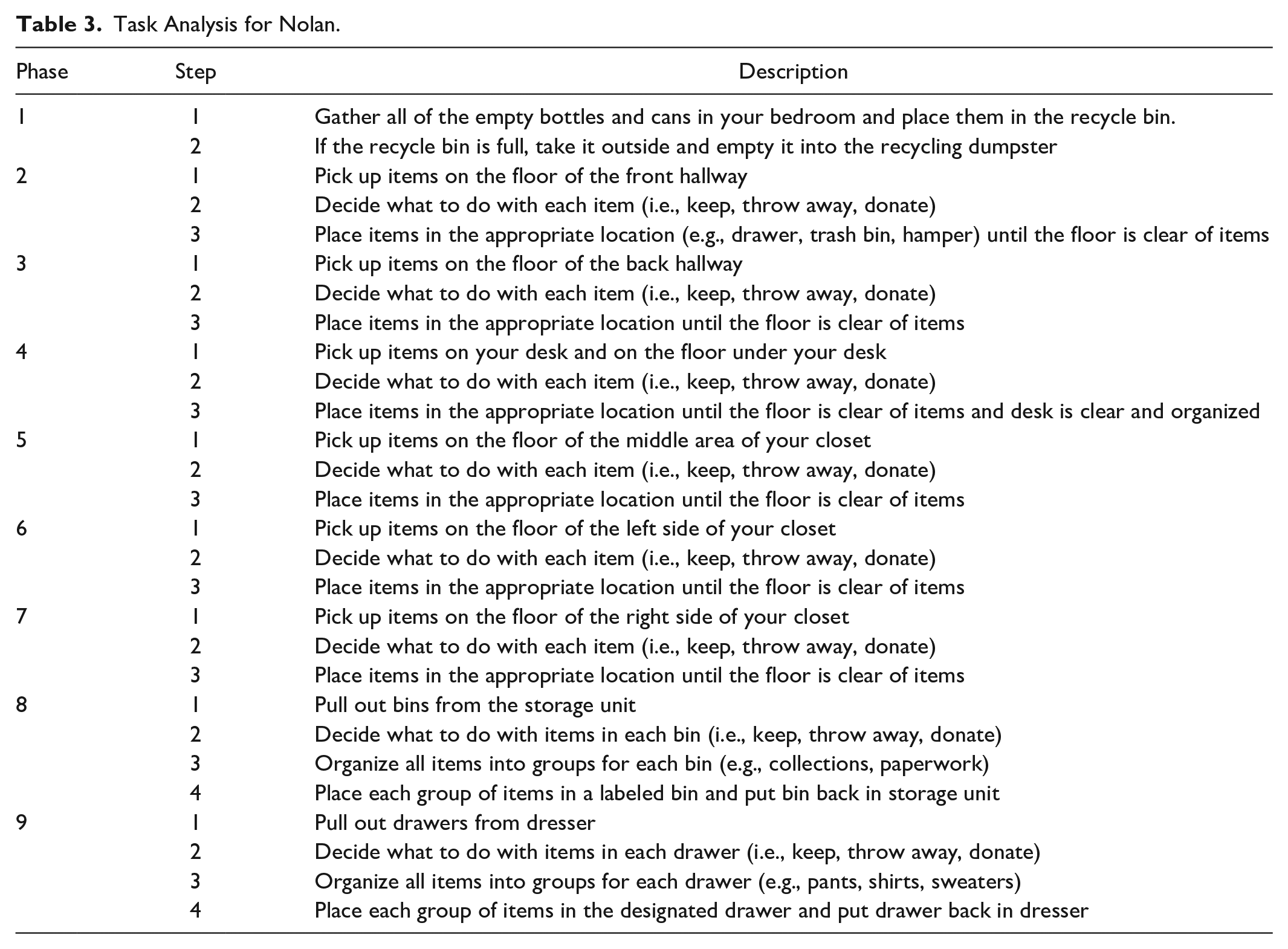
Target DLS were chosen from the Instrumental Activities of Daily Living (IADL), which includes behaviors such as cleaning, cooking, shopping, and managing finances (Roley et al., 2008). The clinician designed a preliminary hierarchy of behaviors (see Table 2) according to the estimated difficulty of each behavior, based on input from parents and support staff, baseline data, and an initial interview with each participant. Total task chaining procedures (Wolery & Gast, 1984) were embedded across treatment phases within each behavior hierarchy. Task analysis (Smith & Belcher, 1985) and shaping (Bensberg et al., 1965) strategies were used to assist each participant’s acquisition of the target behavior (see Tables 3–5).
Treatment Targets.

Task Analysis for Nolan.
Task Analysis for Max.

Task Analysis for Peter.

Nolan’s target behavior included bedroom cleaning and organizing. A nine-step hierarchy was designed according to his baseline hoarding behavior and self-reported anxiety regarding “open” bedroom space, beginning with the easiest areas to clean (i.e., floor space) and gradually moving toward areas that required more sorting and organization (see Table 3). Max’s target behaviors included oven-cleaning and cooking. A task analysis was created for each treatment phase within his hierarchy, designed according to baseline behavior, parent-reported, and self-reported anxiety regarding the stove, oven, and re-connected kitchen smoke detector (see Table 4). (Phase 1 included cleaning a cold oven so that it would be less likely to set off the smoke detector in Phase 2. Max also bought long rubber hot mitts that covered his hands and wrists to help him feel more comfortable while cooking. Phases 2 and 3 included the use of an oven to prepare two recipes, because Max reported being less afraid of using the oven compared with the stove, while Phase 4 included use of a stove to prepare a third recipe. Due to the length of the recipe and time required for meal preparation in Phase 4, individual meal components could be completed over two consecutive intervention sessions; therefore, four sessions with 100% of steps completed without prompting were required to meet criterion [see triangle data points in Figure 1]. Max completed a food preference assessment at baseline to guide recipe selection. Each recipe included at least two favorite foods and did not include any disliked foods. Recipes were found online and modified as needed [e.g., not requiring use of a sharp knife, omitting “spicy” black pepper]. One item that Max had never tried [i.e., olives] was added to the recipe in Phase 2.) Peter’s target behaviors included laundry and ironing. A task analysis was created for each treatment phase within his hierarchy (see Table 5). As Peter did not report any anxiety regarding or aversion to the washer, dryer, or iron, treatment phases were designed using total task chaining to reduce the difficulty of the behavior (i.e., sorting, washing, drying, folding, and ironing clothes from both housing locations).

Number of sessions required to complete changing criterion hierarchy.
Dependent measures
Dependent measures varied slightly for each participant according to their target behaviors (see Table 2). For Nolan, behavioral measures included the number of items picked up during each session, with criterion met by having zero items out of place in the targeted area for at least two consecutive intervention sessions. For Max and Peter, behavioral measures included the number of steps completed independently during each session, with criterion met by performing all steps of the task analysis without prompting for two consecutive sessions. Optionally, participants could complete the tasks before the scheduled intervention session and provide evidence that they independently completed the target skill (e.g., showing the targeted area during the VC session, sending a video of a baked pizza cooling on the rack).
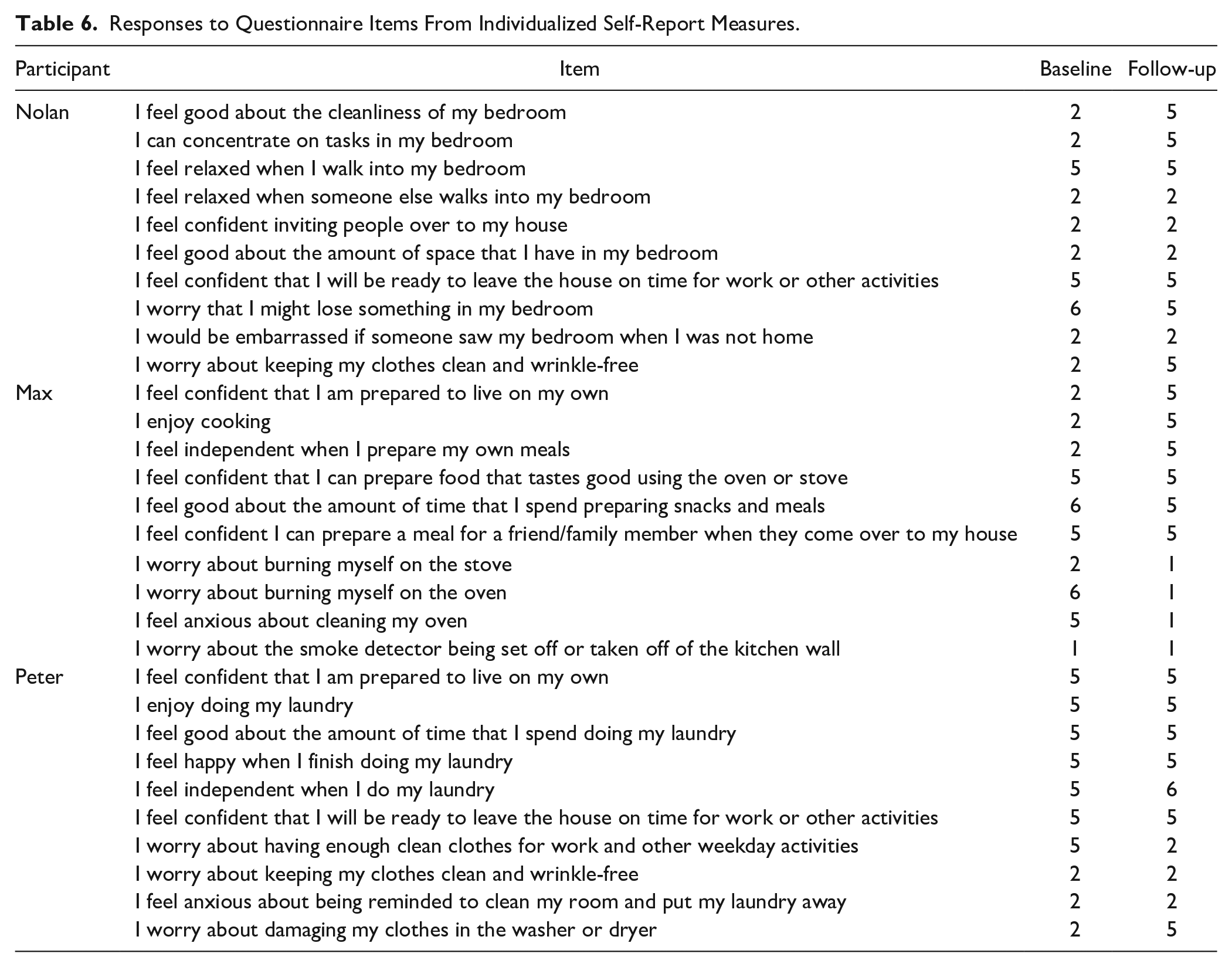
Participants completed multiple self-report measures, including a satisfaction survey and a researcher-developed individualized questionnaire examining the level of confidence regarding the target DLS at baseline and follow-up (see Table 6). Individualized questionnaires included six or seven positively framed statements (e.g., “I feel confident that I am prepared to live on my own”) using a 6-point Likert-type scale (1 = strongly disagree, 6 = strongly agree), and three or four negatively framed statements (e.g., “I worry about having enough clean clothes for work and other weekday activities”) where numbers were reversed (6 = strongly disagree, 1 = strongly agree). Negatively and positively framed statements were interspersed on the questionnaires, but regrouped in the table to facilitate comparison of results (see Table 6). Two out of three caregivers responded to requests to complete a parent satisfaction survey (see section “Results”).
Responses to Questionnaire Items From Individualized Self-Report Measures.
Procedures
Baseline
During the baseline condition, participants engaged in the target tasks as they normally would without prompts or other intervention. Completion of the target tasks was video-recorded or photographed by a parent (for Nolan and Peter) or by a support staff member (for Max). Participants completed the self-report questionnaires that were administered through SurveyMonkey. Videos were shared through Box, coded, and stored on an encrypted hard drive in a locked clinic room.
Intervention
VC intervention sessions were scheduled 1 to 2 times per week for approximately 15 to 60 min. Intervention sessions gradually decreased in length as participants began to master the steps. For the treatment phases that included down time between steps (i.e., waiting for laundry load to wash), the participant and clinician scheduled a second VC call at the approximate time when the previous step would have been completed.
The VC intervention consisted of four components: (a) rapport-building, or a brief friendly conversation at the beginning of the session without priming, teaching, or instructions; (b) prompting the target skill/steps using a system of least prompts procedure; (c) providing specific contingent praise throughout the session; and (d) refraining from negative comments about the participant or his performance of the target skill. Participants placed their computer, tablet, or phone near where they were working and described anything that the clinician could not see well (e.g., a specific item picked up off the floor, setting options for the oven or washer) as an assurance that data would be accurate, because no on-site assistance was provided. The clinician took data on unprompted occurrences of the target behavior. Descriptive praise was used throughout the session (e.g., “Wow, the oven is looking really good!” “You’ve picked up a lot so far!” “Cool! That’s a great idea.”). Positive feedback was given at the end of each session, including a summary of progress and comments about the progress and effort given during the session. The clinician video-recorded the entire session and downloaded videos onto an encrypted external hard drive stored in a locked office.
Also, because a reinforcer assessment showed that all three participants were motivated by social activities, social reinforcers were provided for all of the participants. Nolan and Peter celebrated completion of each treatment phase by attending a social lunch with the clinician, and Max picked out a new Lego set from a store and worked on it with his support staff member.
Follow-up
Maintenance probes were video-recorded by a parent or support staff member in the same manner as in the baseline condition. Nolan and Peter completed the tasks from all treatment phases, whereas Max completed the tasks from Phase 1 and alternated between the tasks from Phases 2 to 4 (i.e., preparing different recipes) at follow-up. Three follow-up probes were taken for Nolan, 7, 10, and 14 days after fading intervention. Two follow-up probes were taken for Max and Peter at 6 and 10 to 11 weeks after fading intervention.
Interobserver Agreement
Using an interval scoring system, a graduate researcher and an undergraduate research assistant, who was blind to the experimental conditions, independently recorded data for at least 20% of sessions across all conditions. Data were scored on a standardized observation sheet in 1-min intervals for videos presented in random order. Interobserver agreement (IOA) was calculated for two dependent variables, including (a) whether or not the participant met the criterion for the current treatment phase and (b) a frequency count of the individualized target behavior (i.e., number of items picked up or task analysis steps completed independently during the session), by dividing the number of agreements by the total number of agreements plus disagreements and multiplying by 100. An agreement was defined as both observers rating the behavior identically, and a disagreement was defined as any discrepancy between the two recordings. For reaching criterion, mean IOA across participants was 100% for both occurrences and nonoccurrences during intervention sessions. For the frequency count, mean IOA across participants was 90%. Mean agreement was 94% for occurrences and 71% for nonoccurrences of the target behavior (i.e., number of items picked up or steps completed) during intervention sessions.
Fidelity of Implementation
Fidelity of implementation for treatment delivery was measured for 26% of all sessions using an interval scoring system. Data were scored on a standardized observation sheet in 1-min intervals for videos presented in random order. Fidelity was calculated by dividing the number of agreements by the total number of agreements plus disagreements and multiplying by 100 for the occurrence of four VC intervention model components: (a) rapport-building, (b) assisting performance of the target skill, (c) providing praise, and (d) refraining from negative comments. An agreement was defined as both observers rating the behavior identically, and a disagreement was defined as any discrepancy between the two recordings. Mean observer agreement across participants was above 80% for each component (100%, 96%, 92%, and 100%, respectively).
Results
Baseline measures for all three adults indicated that none of the participants could engage in the targeted DLS prior to the start of intervention. Nolan, Max, and Peter respectively completed the treatment phases for all target behaviors after a total of 107, 28, and 22 intervention sessions over a period of approximately 54, 14, and 22 weeks (see Figure 1). As shown in Figure 1, all three participants increased the number of steps completed without prompting across intervention sessions for each treatment target beginning immediately after the first session, and reaching the criteria (i.e., all items picked up or all steps completed independently across two consecutive sessions) within two to 23 (M = 8.7) sessions for each treatment phase. Specifically, due to extensive hoarding behavior, Nolan required seven to 23 (M = 11.9) sessions to complete each treatment phase, compared with Max (range = 5–9, M = 7.0) and Peter (range = 2–6, M = 4.4). Nolan picked up a total of 2,881 items to meet criterion for Phases 1 to 9. The number of items picked up in each bedroom area ranged from 171 to 172 items for Phases 6 and 7 (i.e., left and right side of the closet floor) to 777 items for Phase 2 (i.e., front walkway). Thus, the greatest number of items were out of place in the area closest to the doorway, while the fewest number of items were out of place in areas that were difficult or impossible for Nolan to access prior to intervention. The participants also maintained their newly learned target behaviors across follow-up probes. Nolan maintained bedroom cleaning and organizing behaviors across three follow-up probes, while Max and Peter maintained oven-cleaning/cooking and laundry/ironing behaviors across two follow-up probes (see Figure 1). For Max, generalization of cooking behavior occurred during two follow-up probes: support staff members reported that Max independently prepared two new meals, including meatloaf and calamari with vegetables, and that the smoke alarm was not set off when he used the oven.
Supplemental Social Validation Measures
Each participant completed an individualized questionnaire at pre- and postintervention (see Table 6) assessing level of confidence regarding target DLS. Across participants, average level of confidence increased from baseline (M = 3.6) to follow-up (M = 3.8). Confidence scores increased from baseline to follow-up for Nolan (M = 3.0 and M = 3.8) and Peter (M = 4.1 and M = 4.2, respectively). Max’s score decreased slightly from baseline to follow-up (M = 3.6 and M = 3.4, respectively). Interestingly, changes in confidence scores differed according to the framing of response items. Scores for individual response items were considered to remain stable if pre- and post-intervention scores differed by 0 to 1 points. From baseline to follow-up, confidence scores increased (19%) or remained stable (81%) for positively framed items. In contrast, confidence scores for negatively framed items increased (15%), remained stable (62%), or decreased (23%) from baseline to follow-up.
Following the intervention, caregivers and participants filled out a four-item satisfaction survey using a 6-point Likert-type scale (1 = strongly disagree, 6 = strongly agree). Nolan and Peter’s mothers responded that the intervention was helpful for their family (M = 5.5), they noticed a difference in their child’s performance of the target living skill during intervention (M = 5.5) and after ending intervention (M = 5.5), and they would recommend the intervention to others (M = 6). Peter’s mother commented, “Laundry is now very appropriately a part of Peter’s routine. He does a good job and seems to find satisfaction in this increase in self-sufficiency.”
Nolan, Max, and Peter reported that they enjoyed participating in the intervention (M = 5), the intervention was helpful for them (M = 5.67), and they would recommend such intervention to others (M = 5). They did not report feeling stressed while participating in the intervention (M = 2.33). Peter commented on his survey that his clinician “was very fun to work with.”
Discussion
It is evident that all three participants in this study performed the target DLS independently (i.e., completing all steps from their individualized hierarchy without prompting) and reached the criteria. Such results suggest that a VC intervention program with systematic acquisition of target behaviors could be successful in teaching DLS to young adults with ASD. This study also suggests that the effects of several face-to-face interventions for individuals with ASD can also be achieved through VC (cf. Bensberg et al., 1965; Cullen & Alber-Morgan, 2015; Hume et al., 2009; R. L. Koegel et al., 2004; Mechling et al., 2009; Smith & Belcher, 1985). In addition, VC interventions appear to be effective in overcoming maintenance barriers of DLS due to its implementation in the natural setting. Such types of VC interventions may also decrease the individual’s dependence on in-person support and minimize potential impropriety or embarrassment of constantly having a clinician in the adult’s personal living space. Furthermore, VC interventions eliminate transportation issues (e.g., travel time for the clinician and adults with ASD).
Results from the satisfaction survey indicated that this intervention was positively received by all participants and helpful for their everyday life. Moreover, results from the individualized questionnaires allowed us to examine how each participant’s confidence in the specific DLS increased following the intervention. From baseline to follow-up, participants’ confidence increased from a response of “disagree” to “agree” for several positively framed items, such as confidence about bedroom cleanliness, being able to concentrate on tasks, being prepared to live on one’s own, enjoying cooking, and feeling independent when preparing meals (see Table 6). In addition, participants’ confidence increased from a response of “agree” to “disagree” for a number of negatively framed items, including worrying about keeping clothes clean/wrinkle-free and damaging clothes in the washer or dryer. Following the intervention, Max was able to incorporate more “favorite” items from the food preference assessment into his meal repertoire. For example, while Max had never eaten calamari at baseline, he prepared a calamari recipe and added it to his list of favorite food items at follow-up. Nonetheless, as shown in Table 6, all three participants continued to experience self-reported lack of confidence or anxiety related to the target behaviors at follow-up. Participants reported increased anxiety in response to several negatively framed questionnaire items, all of which related to acquisition of the target DLS, possibly because this meant that a caregiver would no longer be providing this service (i.e., being in charge of keeping the oven/laundry clean or preparing foods in the oven). However, it may as well be the case that, along with the improvements in confidence, some level of anxiety may increase when more responsibility is placed upon an adult. In addition, the individualized questionnaires used in this study could also be improved with the addition of an “N/A” response option, as some participants reported high levels of confidence for items that did not apply at baseline (e.g., enjoying doing laundry). Future interventions may need to address ways in which DLS may become more enjoyable.
Limitations of this study also manifest in the way of conducting maintenance probes, especially regarding participants’ availability for follow-up. Specifically, due to a remodeling at Nolan’s parents’ home, data could not be collected on maintenance or opportunities for generalization to other bedroom areas for more than 2 weeks following the intervention. However, it was encouraging that Max and Peter continued to demonstrate the appropriate DLS for at least 11 to 12 weeks following the intervention.
Another area of interest relates to caregivers. Caregivers in this study reported a high satisfaction with the newly learned skills of their adult child. Creating situations where individuals with ASD contribute to family functioning, such as completing DLS, may decrease parent stress (Iadarola et al., 2019). Future studies might benefit from having each participant’s parents and caregivers (including any support staff members that provide in-home support) complete satisfaction surveys. Caregiver observations about behavioral change postintervention and additional items on the follow-up questionnaire could potentially help us determine how VC interventions can help reduce caregiver stress and improve relationships between caregivers and young adults with ASD (Taylor & Seltzer, 2011).
Also, continuing research is needed to explore how VC interventions can be used with additional target behaviors for adults with ASD. Many interventions typically delivered in a clinic setting might also be implemented effectively through VC, such as structured social planning, mock interviews, and interventions using self-management or video-feedback to target various social communication skills (Ashbaugh et al., 2017; B. L. Koegel, 2015; L. K. Koegel, Ashbaugh, et al., 2016; L. K. Koegel, Navab, et al., 2016; Strickland et al., 2013). Finally, further research may be helpful for understanding how both DLS and VC interventions might be used with younger individuals with ASD. Early DLS interventions potentially may help children and adolescents with ASD to develop critical living skills before the transition to adulthood, when many of these skills will be required for success in employment, higher education, and independent living. Likewise, early intervention may help prevent development of symptoms of comorbid disorders that reduce adaptive functioning, such as hoarding behavior or anxiety surrounding performance of a specific DLS (Kraper et al., 2017). In conclusion, this study is the first to explore the effective use of VC to deliver direct interventions for DLS to individuals with ASD from a remote location. Given the shortage of clinicians available to provide applied behavior analysis (ABA) services for individuals with ASD of all ages (Granpeesheh et al., 2010), VC interventions are a promising alternative that may enable clinicians to work with a greater number of clients and families, including those who may otherwise be unable to access services due to the required travel cost or distance.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.