
Abstract
Officers in law enforcement agencies (LEAs) experience long-term health morbidity and mortality at rates exceeding other occupations and the general population. The purpose of this study was to pilot a survey of officer safety and wellness to demonstrate feasibility, assess the need for further research, and lay the groundwork for policies and additional support for officer wellbeing. A random sample of 184 officers from 11 participating LEAs responded to a survey regarding physical activity patterns, job characteristics, substance use, critical incidents, job-related stress, personal health, and health-care usage. Officers reported physical health outcomes at rates similar to the general population but screened positive for elevated rates of posttraumatic stress disorder, common mental disorders, and alcohol misuse. These data support the need for research at the regional and national levels to inform LEA policies and programs.
Background
Law enforcement officers face multiple threats to their safety and wellbeing. The occupational fatality rate of police officers is nearly three times that of the average U.S. worker (Maguire, Hunting, Smith, & Levick, 2002). Moreover, officers have morbidity and mortality for long-term health outcomes at rates exceeding the general population (Anderson, Litzenberger, & Plecas, 2002; Franke, Collins, & Hinz, 1998; J. M. Violanti, Vena, & Petralia, 1998). In addition to assaults (Brandl & Stroshine, 2012; National Law Enforcement Officers Memorial Fund, 2013b); traffic injuries (Ashton, 2012; National Highway Traffic Safety Administration, 2000); and biological, particulate, and chemical hazards (Chen & Jenkins, 2007a, 2007b; Cooper, Rice, Wilburn, Horton, & Rossiter, 2005; Fent, 2010; Riediker, 2007; Sonder et al., 2005; Witter, Martyny, Mueller, Gottschall, & Newman, 2007), officers experience posttraumatic stress disorder (PTSD) at high levels (Carlier, Lamberts, & Gersons, 1997; Neylan et al., 2005; Shucard et al., 2012). At the same time, police officers face occupational, organizational, and personal stressors (Abdollahi, 2002; Beehr, Johnson, & Nieva, 1995; Hart & Wearing, 1995). Such stressors may manifest themselves as risky behavioral choices, such as alcohol use (Chopko, Palmieri, & Adams, 2013). Twelve percent of officer deaths over the period 2003 to 2012 involved alcohol or drug use (National Law Enforcement Officers Memorial Fund, 2013a).
While there is growing attention to key stressors that officers experience (Abdollahi, 2002; Auerbach, Quick, & Pegg, 2003; Beehr et al., 1995; McCreary & Thompson, 2006) as well as interventions to mitigate these risk factors (Chae & Boyle, 2013; LeBlanc, Regehr, Jelley, & Barath, 2008; Salmon, 2001), most research has been compartmentalized with respect to risk factors and specific health outcomes (e.g., Hartley, Burchfiel, Fekedulegn, Andrew, & Violanti, 2011). While this body of literature, particularly the longitudinal work, is critical to establishing associations and causal relationships, it is inherently based on more limited models of the safety and wellness needs of law enforcement officers.
Our conceptual model of officer safety and wellness (see Figure 1) reflects the occupational, organizational, and personal stressors serving as risk factors for officers’ health and wellness outcomes (Chae & Boyle, 2013; Regehr & LeBlanc, 2011; Shane, 2010). Job characteristics specific to police work are termed occupational stressors, such as the experience of traumatic events (Shucard et al., 2012), shift work, and on-the-job injuries (J. M. Violanti et al., 2012). Further, the nature of an officer’s assignment is relevant to occupational stressors. For example, compared to an officer with a desk assignment, an officer assigned to patrol duty who drives extensively is at greater risk of traffic collisions, with concomitant potential for physical injury as well as anxiety and other mental health outcomes. Likewise, officers assigned to day shifts experience different exposures than those working rotating shifts. Personal stressors represent individual response and vulnerabilities, in the context of personal demographics, psychosocial factors such as coping mechanisms, and health histories. Despite the easily recognized occupational risks associated with police work, a growing body of research suggests that organizational factors—such as bureaucratic red tape, administrative interactions, and constraints on career mobility experienced by officers—are critical to officer stress and health outcomes. Research in employee outcomes has been informed by extensive research over the past 30 years regarding workplace psychosocial wellbeing. For example, the demand-control-support model predicts that a combination of high demands, low decision latitude, and low social support leads to a state of job strain, carrying the highest risk for illnesses and negative health outcomes (Johnson & Hall, 1988; Karasek, 1979). Thus, understanding the interplay of different types of stressors, personal coping strategies, and social support is essential to serving the overall safety and wellness of law enforcement officers through support services, health services, and policy. An initial step is the collection of a broad profile of stressors, health behaviors, and outcomes for officers in different settings, different assignments, and different personal characteristics, as documented in this pilot study.
Conceptual model of police officer safety and wellness.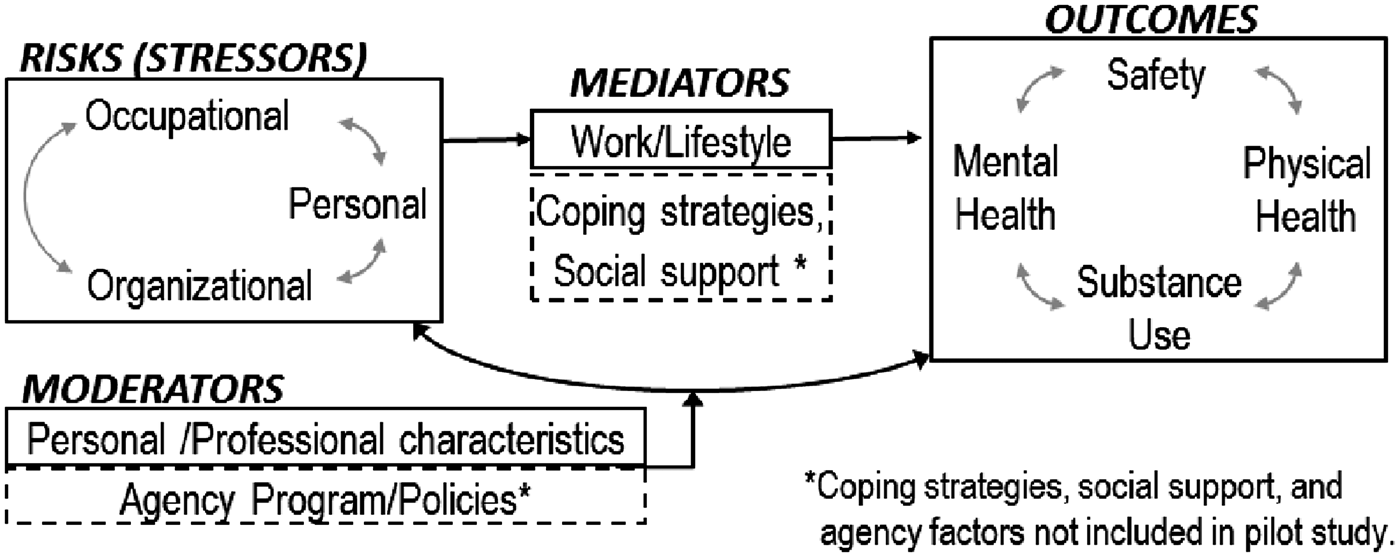
Methods
Design and Sample
Our team selected a convenience sample of 15 law enforcement agencies (LEAs) from the mid-Atlantic region for participation in the pilot study. This initial sample of 15 agencies was expanded to include four more LEAs that expressed interest in the study.11 After the initial contact with each LEA, once agency participation was confirmed, the officer roster of each agency was requested. For the few very small LEAs, all officers on the roster were surveyed. For the remaining LEAs in the study, we drew a random sample of officers instead of conducting a census, following a multistage methodology (Weisburd, Lum, & Petrosino, 2001). The final sample included 184 respondents from 11 agencies. Our overall response rate was 69.4%. The study protocol was approved by the authors’ Institutional Review Boards, covering the written informed consent received from each respondent prior to survey completion.
Measures
The measures were developed based on a focus group discussion our team held with 12 representatives of 11 LEAs—ranging from medium suburban agencies to large urban departments, including both local to state agencies—from Washington, DC, Maryland, and Virginia (July 2011). The authors prepared a draft survey instrument for review and discussion at this meeting. The project team also presented background data at the focus group regarding morbidity and mortality and reviewed research studies examining exposure rates and outcomes for these topic areas. Meeting participants also reflected on the value of collecting longitudinal data capturing, for example, the physical fitness and stress levels of recruits in their first 5 years of service, and officers’ health trajectories postretirement. The agency representatives felt it would be valuable to request survey respondents’ personal contact information to allow the research team to reapproach willing respondents for longitudinal data collection.
Constructs included in the draft instrument included officer physical activity patterns, job-related stress, personal demographics and health information, health-care usage, job training and available equipment, and exposure to environmental hazards (e.g., environmental pollution, blood-borne pathogens, and radiation).22 Following a detailed discussion, the sense of the group confirmed that the primary topics of interest to these agency representatives were the perceived insufficient data on physical activity and related health conditions for officers, clinical markers of health problems (high blood pressure, cholesterol), stressful working conditions (assumed to be as much or more a result of bureaucratic/political challenges as the stress of fieldwork), and exposure to transdermal or other transmissions of biopathogens. The former categories (physical and mental health) were of greatest interest to meeting participants because of the perceived prevalence of the problems; meeting participants felt that based on anecdotal evidence these conditions are widespread among agency personnel and are acknowledged to impact performance readiness and long-term health concerns.
An additional topic of particular concern to the meeting participants was the current and expected increase in former military personnel entering law enforcement. Meeting participants discussed the reality that agencies will be hiring personnel with potential health conditions (e.g., PTSD, head injuries) that the individuals may not have divulged to the military prior to separation (in order to facilitate a hasty separation and return home).
After the focus group meeting, our research team made some modifications to the draft instrument. The final pilot instrument was next reviewed via e-mail by members of the focus group and covered the multiple constructs described later.
Demographics and employment history
Based on a previous officer safety survey (Taylor et al., 2009), the instrument included background demographic items (age, gender, race/ethnicity, and marital status) as well as items describing military experience, duration of law enforcement employment, current rank and duty assignment, and experience working rotating shifts.
Physical activity and diet
The instrument assessed a healthy diet using a reliable two-item measure of fruit and vegetable consumption on a typical day, items that are correlated with 3-day extensive food record data (Prochaska & Sallis, 2004). Two items queried the number of sedentary hours on typical workdays and nonworkdays (coded 0 for less than an hour, 1 = 1–3 hr, 2 = 4–6 hr, 3 = 7–9 hr, 4 = more than 9 hr per day). Further, drawing on the young adult instrumentation of a national longitudinal survey (Harris, 2009), we included measurement of vigorous physical exertion, modified to quantify the number of days in the past week (range 0–7).
Job-related stress, environmental, and critical incident exposures
The survey incorporated 10 operational (α = .842) and 10 organizational items (α = .905) from the widely used Police Stress Questionnaire (PSQ) inclusive of Occupational (PSQ-Op) and Organizational (PSQ-Org) stress scales (1 = no stress at all, 4 = moderate stress, 7 = a lot of stress; Donnelly, Chonody, & Campbell, 2014; McCreary & Thompson, 2006). Higher values on each of these scales represent greater reported stress by the respondent.
Further, the instrument incorporated the Critical Incident Exposure index, designed to measure the trauma officers are exposed to in relation to their years of service on the force (Weiss et al., 2010). Items were modified in presentation of categories of incidents that had happened to a colleague, another person, or to the respondent, and incidents for which the respondent was responsible. To code critical incident histories, we followed Weiss et al. (2010) in creating a 4-point scale (0 = 0, 1–9 = 1, 10–20 = 2, and both 21+ = 3), although Weiss et al. also investigated other treatment of the scale and made no recommendation for a single coding schemata.
Substance use behavior
Prescription drug use (under nonprescribed purposes, quantity, or duration) was assessed with a single indicator for ever use, drawn from the young adult instrumentation of a national longitudinal survey (Harris, 2009). Tobacco use history and current smoking or smokeless tobacco use, as well as time to first cigarette upon waking (a measure of dependence and health risks) are from the Tobacco Use Supplement to the Current Population Survey (Fagan et al., 2007). The instrument also incorporated a three-item screen for alcohol misuse, the AUDIT-C, validated in veteran and general populations (Bradley et al., 2007). Each item is scored on a 4-point scale, with a total score of ≥4 for males and ≥3 for females indicating alcohol misuse.
Physical and mental health information
Respondent’s perception of their general health is screened with as a single 5-point item (1 = excellent, very good, good, fair, 5 = poor) from the Medical Outcomes Study Short Form-36 (Ware & Sherbourne, 1992), also used in the Census and for other ongoing national surveys. Global self-rated health has consistently been a strong predictor of health outcomes and mortality (Idler & Benyamini, 1997).
Self-reports of height (without shoes) and weight (without clothes or shoes; prior to pregnancy if relevant) were collected with measures from the PhenX toolkit (Hamilton et al., 2011). Further, respondents were asked if they had ever been diagnosed with high blood pressure/hypertension (with an exception for pregnancy) or, separately, high blood cholesterol. For both conditions, officers responding in the affirmative were asked about their age at diagnosis, and if the respondent had ever took medication for the condition. These items were also drawn from the PhenX toolkit. A single indicator assessed experience of back pain in the past 12 months (Waxman, Tennant, & Helliwell, 2000).
The two-item screener for major depression (Patient Health Questionnaire depression module; PHQ-2) assesses anhedonia and depressed mood over the past 2 weeks on a 4-point scale (0 = not at all, 1 = several days, 2 = more than half, 3 = nearly every day). A score of 3 or more has a high sensitivity for identifying major depression (Kroenke, Spitzer, & Williams, 2003). The study instrument also included the ninth item from the longer PHQ-9 (analyzed separately), assessing suicidal ideation on the same scale (Kroenke et al., 2003). Further screening on depression and anxiety relied on the Mental Health Index (MHI-5; Friedman, Heisel, & Delavan, 2005), with a “common mental disorder” (CMD) coded 1, reflecting a score ≤76 on the MHI scale, consistent with definitions of a case using the General Health Questionnaire (GHW-12; Kelly et al., 2008). The instrument also incorporated the brief four-item Primary Care-PTSD scale, which was developed for the general population but has also been used to detect PTSD in military veterans (Prins et al., 2004). Scores on the primary care-PTSD range from 0 to 4, and respondents with a score of 3 or greater screened positive for PTSD.
Health-care use
Two items asked about health-care usage covering physical or mental health needs other than for treatment for alcohol/substance abuse or smoking cessation. These items are drawn from the National Survey of America’s Families (Abi-Habib, Safir, Triplett, & Cunningham, 2004). Based on the input of the LEA representatives, the instrument additionally queried flu shot receipt in the past 12 months and, in the past 2 years, whether the officer had received a complete physical (whether standard for all sworn employees, upon entry/exit, or for a specialty unit) as required or offered by the agency.
Results
Sample Description and Health Behaviors.

Note. PSQ = Police Stress Questionnaire.
Categories collapsed due to low cell count.
Stressors
The average operational-PSQ in this sample was 34.3 (SD 11.1); organizational-PSQ scores averaged 38.0 (SD 14.0). Both scores fall just under the scaled value of moderate stress. The average reported CIH score was 22.4 (SD 12.4), indicating that on average across the 35 item scale, officers had experienced each incident somewhere between 0 and 10 times in their careers.
Health Behaviors
On a typical workday, most respondents (88%) reported seated inactivity in excess of 4 hr (30% for more than 7 hr a day), compared to only 33% seated 4 hr or more on a nonworking day. Nearly two thirds (63%) of officers report vigorous exercise on at least 3 days per week, but one in four report only a day or two of vigorous exercise and 12% report that they get none on a weekly basis.
Less than 4% of respondents reported current smoking behavior, and 11% reported use of smokeless tobacco. While 86% reported alcohol consumption, 57% typically consumed only one or two drinks on a given occasion. However, 65% reporting current binge drinking and one in five respondents reported binge drinking on at least a monthly basis. Over half of both male and female respondents meet the criteria for alcohol misuse.
Reports of misuse of prescription drugs were rare. One in five officers elected not to respond to the question about mental health care received in the past year, but of those who did respond, 8.3% reported at least one visit for mental health services. About half of the sample reported receiving physicals in the past year. Likewise, half of the sample received a flu shot in the past year.
Health Outcomes
Health Outcomes and Health Service Usage.
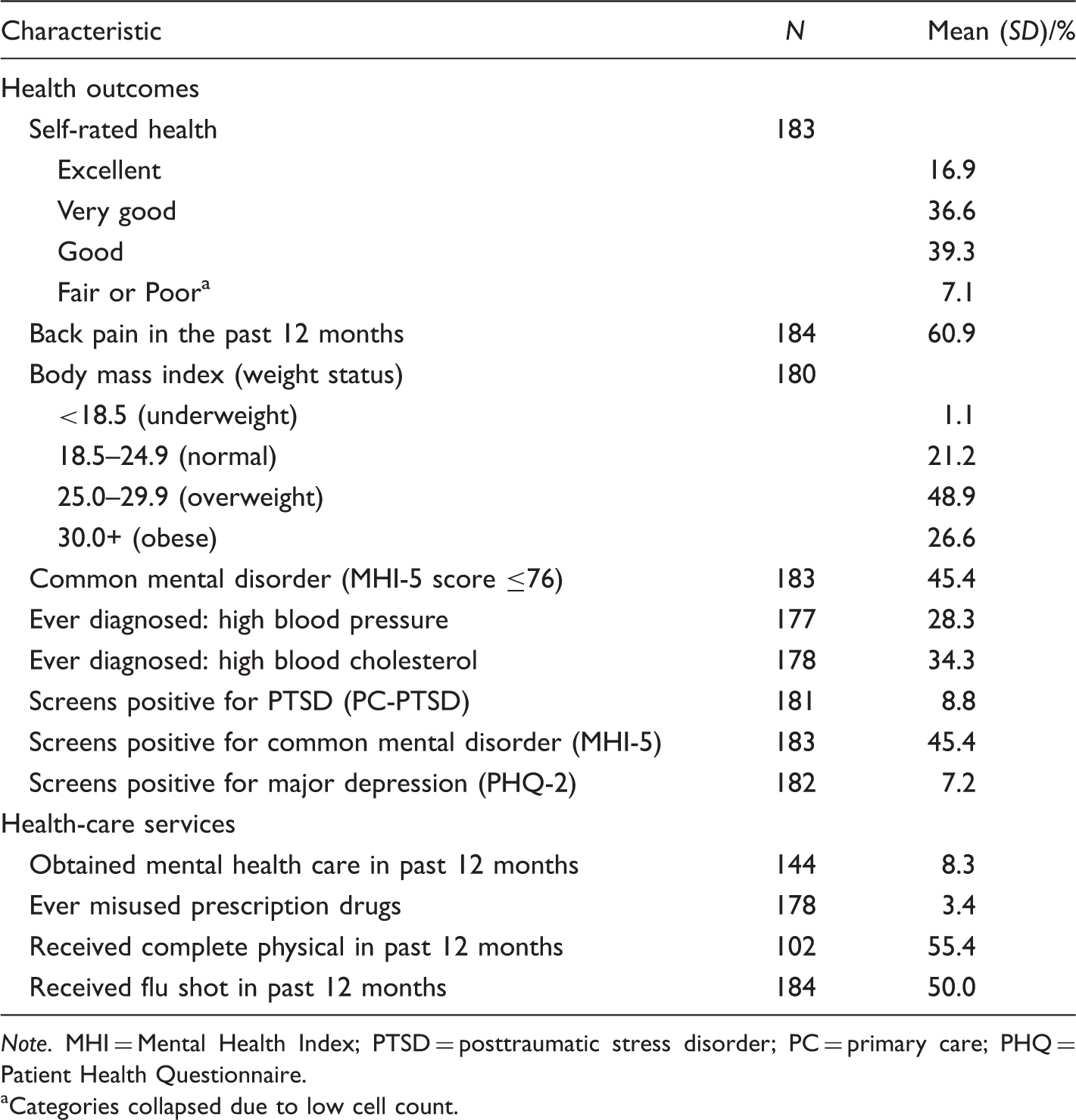
Note. MHI = Mental Health Index; PTSD = posttraumatic stress disorder; PC = primary care; PHQ = Patient Health Questionnaire.
Categories collapsed due to low cell count.
Nearly half of the respondents (45%) screened positive for a CMD (related to anxiety or depression), 9% screened positive for PTSD, and 7% screened positive for major depression.
Correlations
Correlation Matrix of Risk Factors and Health Status.
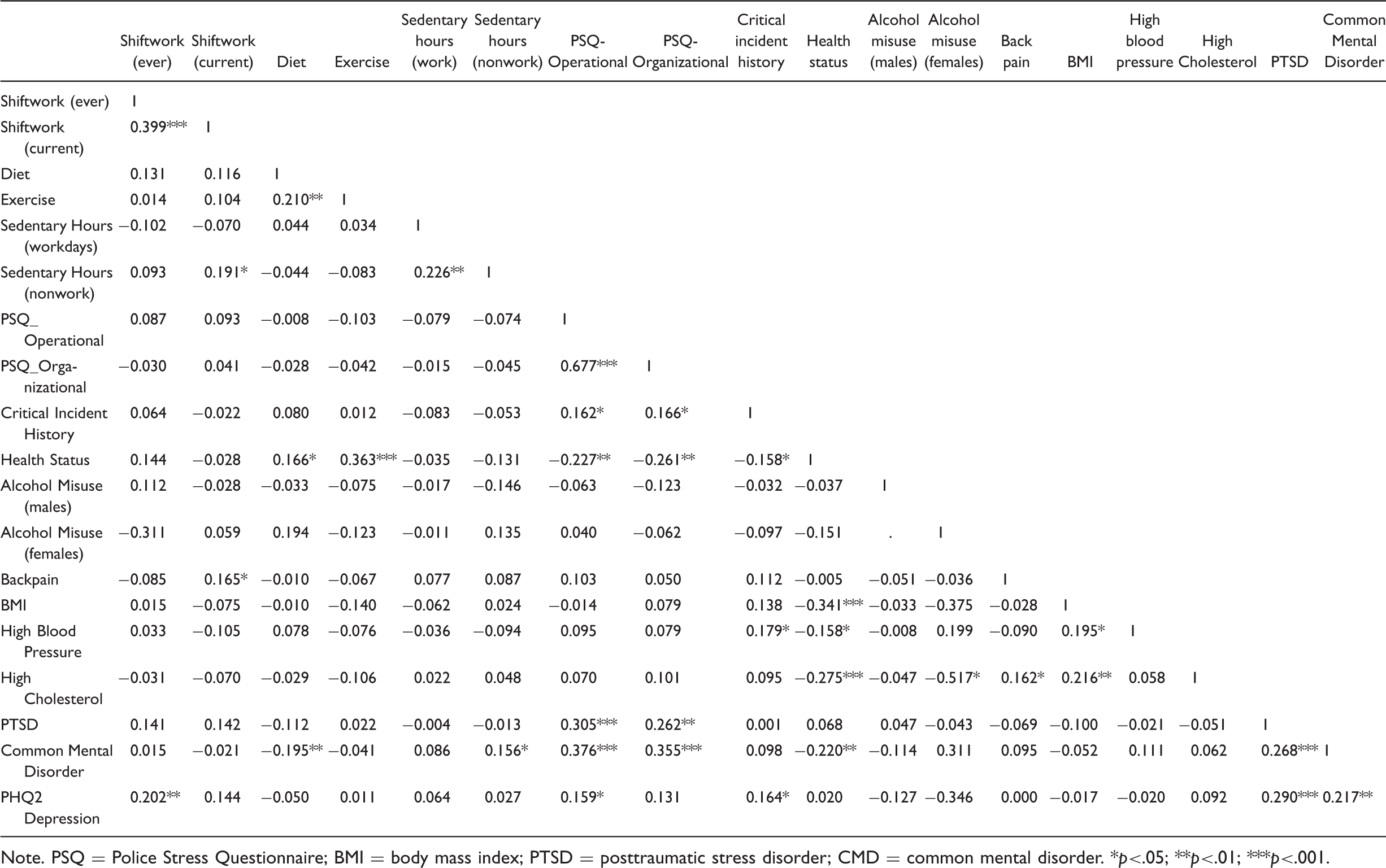
Note. PSQ = Police Stress Questionnaire; BMI = body mass index; PTSD = posttraumatic stress disorder; CMD = common mental disorder. *p<.05; **p<.01; ***p<.001.
Subgroup Analyses
Preliminary analyses (results available from authors) include examination of key outcomes by gender, rank, and age as well as years of service. With some exceptions, poorer physical health, CMDs, PTSD, and critical incident scores were positively associated with age. However, officers who had served 6 to 10 years reported higher stress and were more likely to screen positive for a CMD and PTSD than those with fewer or more years on the force. Gender differences were observed for operational and organizational stress (females reporting more) and BMI (significantly higher BMI for males), but not for diet, exercise, critical incidents, PTSD, CMDs, major depression, or general health status.
Discussion
We examined the estimated rates of stressors and health outcomes results from this pilot study in comparison with general population studies. Physical activity among officers exceeded that of the general population, in which only half of adults (compared to two thirds of sampled officers) meet aerobic guidelines (Harris et al., 2013). Respondents’ reported tobacco use was far less than that of the general population (19.3%; Agaku, King, & Dube, 2012). However, the monthly binge drinking rate in this sample of officers (22.4%) slightly exceeded that of the general population (17.1%; Kanny, Liu, Brewer, Garvin, & Balluz, 2012). Further, in terms of alcohol misuse, while in a primary care population one in three males and one in four females screened at risk (Bradley et al., 2007), over half of both male and female officers screened positive for alcohol misuse although alcohol use is a maladaptive coping strategy in response to stressors (J. Violanti, Marshall, & Howe, 1983). The average PSQ score in our sample was consistent with other police research (McCreary & Thompson, 2006) as was the frequency of exposure to traumatic incidents (Weiss et al., 2010). Operational and organizational stress in this sample of officers appears no higher than workplace stress in the general population (41%; American Psychological Association, 2009), although the measurement on which these estimates are based differ. While environmental factors may increase the stress levels of police officers, it is notable that organizational factors may moderate the relative perceived stress (Dollard, Osborne, & Manning, 2013) and in some cases may be a greater source of stress than occupational factors (Shane, 2010).
In an examination of several risk factors for cardiovascular disease (CVD) comparing officers from Buffalo, NY with the general population, police officers’ risks were uniformly higher (Hartley et al., 2011). By contrast in our sample, the rate of hypertension (high blood pressure) in the sample (28.3%) was similar to the general population rate (30.9%; Gillespie, Kuklina, Briss, Blair, & Hong, 2011), as was the rate of hypercholesterolemia (33.5%) in the general population (Kuklina, 2011). Sample prevalence of obesity (26.6%) was lower than that of the general population (34.9%; Ogden, Carroll, Kit, & Flegal, 2013). However, while most officers (92.9%) reported at least good health in the past year, compared with 89.7% of the general population, half as many officers reported excellent health (16.9%) as did members of the general population (32.7%; O’Hara & Caswell, 2012). Self-reported health as a continuous measure predicts morbidity and mortality outcomes (Idler & Benyamini, 1997), and distinctions in status between officers and the general population are perhaps signaling the documented long-term differences in morbidity and mortality outcomes (Anderson et al., 2002; Franke et al., 1998; J. M. Violanti et al., 1998).
Poorer health status and outcomes may be attributable to differences in mental health. Using the MHI-5, officers in this sample screened positive for anxiety and depression (CMDs) at nearly twice the rate of the general population (Kessler, Chiu, Demler, & Walters, 2005). However, the difference may be largely in anxiety disorders, as 7.2% of the sample screened positive for major depression (using the PHQ-2) compared with 6.7% diagnosed with major depression (Diagnostic and Statistical Manual of Mental Disorders, 4th ed., DSM-IV) in the general population (Kessler et al., 2005). Among anxiety disorders, PTSD may constitute a considerable part of the problem among officers, who screened positive (8.8%) at a rate more than twice that of the general population (3.5%; Kessler et al., 2005). The extent to which this rate is a result of on-the-job exposures versus prior experiences is unknown. Half of LEAs actively recruit new personnel with military experience (Reaves, 2012). As discussed in the initial design meeting (for this pilot study) with LEA representatives, the concern is whether the population of LEA officers is being replenished with veterans already suffering from PTSD. With consideration of these rates and the potential impact on physical health outcomes going forward (Joseph et al., 2010; Pacella, Hruska, & Delahanty, 2013; J. M. Violanti et al., 2006), further investigation of the prevalence and correlates of officers’ PTSD is warranted, as well as services to address the condition.
While this pilot study was not designed to investigate longitudinal relationships, the incidence of stressors and health risk behaviors in this sample are of concern. For example, that 20% of the respondent population reported binge drinking at least monthly is of particular concern for multiple health outcomes such as coronary heart disease and metabolic syndrome (Fan et al., 2008; O’Keefe, Bybee, & Lavie, 2007; Rehm, Sempos, & Trevisan, 2003). In other research, male officers’ longer work hours have been directly related to waist circumference and BMI (Gu et al., 2012). Further, while individual experiences rather than frequency of exposure to critical incidents were related to PTSD symptoms in nurses and ambulance staff (Declercq, Meganck, Deheegher, & Van Hoorde, 2011), among police officers, frequency of exposure has been related to both PTSD symptoms and brain structure as measured by magnetic resonance imaging (Shucard et al., 2012).
In these pilot data, we see a compelling network of correlated risk factors and health outcomes, largely consistent with the literature but instructive regarding the design of a more inclusive health study for law enforcement officers to better understand main effects, moderation, and mediation. For example, research has linked negative life events but not traumatic policy incidents to officers’ depression (Hartley, Violanti, Fekedulegn, Andrew, & Burchfiel, 2007), highlighting the important cross-fertilization of personal and professional lives. Research investigating these pathways in longitudinal designs is essential to understanding the relative contribution of different risk factors. In turn, this information will be instructive for policy and training design and prioritizing the allocation of agency resources.
Further, this pilot study demonstrated the feasibility of gathering personal health and safety information from a random sample of police officers. Our team was successful in recruiting LEAs to participate through the provision of officer rosters for the random selection of officer respondents. However, the study was not designed to be representative of U.S. law enforcement officers from all regions of the country nor did it represent officers in sufficient numbers to investigate the theoretical relationships between stressors and selected health outcomes for men and women serving law enforcement. Pursuing this research with a national sample would allow for investigation of national and regional estimates of officer wellness. In addition to providing national and regional estimates that are unavailable elsewhere, expansion of this research to understand the role of occupational and organizational stressors in health and safety outcomes will inform the design of more effective interventions and services to support officer safety and wellness.
Limitations to this pilot study have been carefully examined to inform expansion to the national level. The pilot instrument as fielded covered multiple constructs of concern as identified by the literature and from input from multiple LEA representatives. As the pilot study unfolded and in subsequent research, it became apparent that additional constructs are relevant to the conceptual model of officer safety and welfare. For example, more than half of officers do not maintain healthy sleep patterns, 90% are routinely fatigued on the job (National Law Enforcement and Corrections Technology Ctr, 2008), and more than 40% have a sleep disorder (Pearsall, 2012; Rajaratnam Sw & et al., 2011). Sleep deprivation is associated with the onset of health disorders (depression, CVD, and metabolic syndrome; Esquirol et al., 2009; McEwen, 2006; Wolk & Somers, 2007; Yoo, Gujar, Hu, Jolesz, & Walker, 2007) that officers are prone to develop (Ma et al., 2013; Mccanlies et al., 2012; Pearsall, 2012; Rajaratnam Sw & et al., 2011; J. M. Violanti et al., 2009). Additionally, theory and empirical studies point to the importance of styles of coping with traumatic situations to attenuate negative impact on officer wellness (Anshel, 2000; Chae & Boyle, 2013; LeBlanc et al., 2008; Patterson, 2003). The range of personal coping strategies, the availability of agency support to develop effective coping strategies, and the extent to which officers are implementing coping strategies are critical components in a conceptual model understanding the relationship between stressors and health outcomes. Moreover, further investigation in officer personality constructs to understand and mitigate health outcomes from occupational and organizational stressors is warranted (Salters-Pedneault, Ruef, & Orr, 2010). While not intended to diminish attention to these constructs, our model as currently designed does not include attention to several risk factors of interest such as sleep quality (Slaven et al., 2011), or outcomes such as domestic violence, although this behavioral outcome is of concern in the context of stressors and maladaptive coping strategies (Johnson, Todd, & Subramanian, 2005).
Operational and Policy Implications
While the results of this study will help inform a national study on officer safety and wellness, our findings do identify some areas of immediate concern. This article highlights the scarcity of information about the availability and specific components of LEA wellness programs (Church, 1993; Church & Robertson, 1999), and while management and operations standards are commonly evaluated among police agencies seeking certification (Commission on Accreditation for Law Enforcement Agencies, n.d.) and standards exist for equipment related to various immediate threats officer face (e.g., body armor for firearms and reflective vests for car accidents), neither corollary national environmental hazard safety standards nor standards for employee wellness programs for law enforcement exist. Further, when officers require long-term disability leave, there are multiple barriers (e.g., mental health, physical job demands) to their returning to the job (Board & Brown, 2011). As in public health, prevention is the first tier of effort to avoid poor health outcomes and associated costs. Despite the general dearth of information on officer health, some promising developments are emerging to improve the communication of officer health concerns to the field. For example, the BJA VALOR program, which has previously focused on officer safety, is expanding to include officer health and resilience (see http://www.valorforblue.org/Home/VALOR-Resources/Health).
Should officer stress and associated physical and behavioral health outcomes be further identified as a significant cost to LEAs, the policy implications for LEAs are clearly in line with other organizations investing in organizational wellness programs (Claxton et al., 2008). Based on the results of this pilot study, such wellness programs will likely need to offer a comprehensive array of support services, including alcohol abuse treatment, whole life wellness training, and mental health services that may be extended to families of officers. In addition to policy attention to shift length and schedules, agencies may consider addressing sedentary time policy attention to promoting preventative care for officers to avoid subsequent tertiary costs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NORC at the University of Chicago in collaboration with Police Executive Research Forum provided support for this study.