
Abstract
Objectives
The aim of the present study was to identify differences in fecal analytes (ie, microbiota, fatty acids [FAs]) in cats with exocrine pancreatic insufficiency (EPI) compared with healthy controls, and describe clinical signs at baseline and short-term follow-up.
Methods
A cross-sectional, observational study was conducted of 55 client-owned cats with EPI and 37 healthy client-owned blood donor control cats. Eligible cases had a feline trypsin-like immunoreactivity (fTLI) consistent with EPI. Fecal samples were analyzed for fecal microbiota dysbiosis index (DI) and FAs. Serum and fecal analytes from controls were compared with EPI cats using parametric and non-parametric methods including general linear models to adjust for potential confounding by signalment differences. Clinical signs were described for cats with EPI at enrollment and for one short-term follow-up time point.
Results
Fecal DI and FAs were abnormal in EPI cases compared with controls. Cats with EPI had a higher median DI (1.5 [range −2.6 to 3.8]), total FAs (74.1 µg/g [range 4.7–162]), arachidonic acid (2.54 µg/g [range 0.03–17.0]) and nervonic acid (0.37 µg/g [range 0.02–1.5]) than controls (–3 [range −4.4 to −0.6], 19.7 µg/g [range 9.4–75.2], 0.57 µg/g [range 0.32–1.51] and 0.17 µg/g [range 0.09–0.54], respectively), and a lower median Peptacetobacter hiranonis (4.8 log DNA [range 0.1–6.1]) compared with controls (5.9 log DNA [range 3.2–6.8]). The most common clinical signs were weight loss and appetite disturbances.
Conclusions and relevance
Cats with EPI have alterations in fecal microbiota and FA, and clinical signs in this population of cats were similar to those previously reported.
Keywords
Introduction
Exocrine pancreatic insufficiency (EPI) is characterized by insufficient production or secretion of pancreatic enzymes, causing malabsorption.1 –3 Diagnosis of feline EPI has risen since the development of the serum feline trypsin-like immunoreactivity (fTLI) assay and concurrent increased awareness of clinical signs, which differ in cats (eg, larger proportion of hyporexia to anorexia and less diarrhea) compared with those reported in dogs.1,3
Dogs with both treated and untreated EPI have shown altered fecal microbiota profiles (ie, reduced species richness and diversity) compared with healthy dogs. 4 A subset of these dogs achieve normalization of dysbiosis when treated with pancreatic enzyme replacement therapy (PERT). Dogs with EPI have also shown increases in their fecal microbiota dysbiosis index (DI) and lactate, along with decreased secondary bile acids (BAs), compared with healthy controls. 5 These findings highlight potential pathways to address in the therapeutic management of EPI dogs with persistent clinical signs despite standard PERT.2,5 Cats with EPI have been noted to have differences in their serum metabolome compared with healthy controls, suggesting enteric dysbiosis in cats with EPI. 6 Despite this, the fecal microbiota and fecal fatty acid (FA) profiles in cats with EPI have not been investigated. 2 If abnormalities in the microbiota or fecal FAs are found in cats with treated and untreated EPI, these changes might represent an avenue for prognostic or therapeutic intervention.
The primary aim of our study was to identify differences in the fecal DI and FA profiles, specifically alterations in Peptacetobacter hiranonis (formerly Clostridium hiranonis) and key FAs (ie, arachidonic and nervonic acids), of newly diagnosed EPI cats compared with healthy controls. A secondary aim was to describe clinical signs and short-term clinical outcomes in diseased cats. We hypothesized that cats with EPI were more likely to have abnormal fecal DI and FA profiles compared with healthy controls, and clinical signs in cats with EPI would resemble those reported in the previous literature.
Materials and methods
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)-Vet statement 7 checklist was consulted when preparing this manuscript, and the location in the text of where each criterion is addressed can be found in Figure S2 in the supplementary material.
Study animals
Client-owned cats were eligible for enrollment as EPI cases based on a serum fTLI less than or equal to 8.0 μg/l, the currently accepted range for diagnosis, through the Gastrointestinal Laboratory at Texas A&M University between April 2024 and February 2025. Cases were excluded if a fecal sample was not provided within 4 weeks after the enrollment fTLI, a primary comorbidity that explained the gastrointestinal (GI) clinical signs (eg, neoplasia or confirmed chronic enteropathy [CE]) and/or resulted in euthanasia before a follow-up time point was identified, or medical records were insufficient.
Healthy controls comprised blood donor cats enrolled between November and December 2023 (IACUC 2023-0166). Although all blood analyte outcome measures have well-established population-based reference intervals (RIs),8 –10 this control group was included for interpretation of fecal assays, some of which lack population-based RIs. Control cases were deemed healthy based on normal physical examination findings, unremarkable complete blood count and chemistry, no current GI signs and no antibiotic, steroid or proton pump inhibitor use within 6 months.
Design and medical records
This was a cross-sectional, observational study. A case was identified based on an eligible fTLI result, and the submitting veterinarian then contacted for enrollment and owner consent. Medical records were reviewed by a single investigator (AH) at enrollment and for short-term follow-up, and the following information recorded: breed, age, sex, neuter status, weight, body condition score (BCS), clinical signs, diet, medications and concurrent morbidities. Initial weights were recorded if obtained within 1 week of the initial serum sample submission. Cobalamin, folate and feline pancreatic lipase immunoreactivity (fPLI) were recorded if quantified at enrollment, and feces obtained within 4 weeks after inclusion. Updated medical records were requested starting at approximately 6–8 weeks after initial fTLI results and until follow-up records were obtained. Veterinarian and owner follow-up, via phone or email, were also performed if updated medical records were unavailable or insufficient for the 6–8-week mark.
Blood samples
All serum assays were performed at the Gastrointestinal Laboratory, with samples for all cats submitted by the attending clinics. Healthy control serum was collected over three dates in November and December 2023. Samples were stored at 4°C immediately after collection and then moved to −80°C within 12 h of collection until sample analysis within 1 week’s time. Serum cobalamin and folate concentrations were measured using an automated competitive binding chemiluminescence immunoassay system (IMMULITE 2000 XPi; Siemens) as previously described, 8 with lower and upper detection limits of 150 and 1000 ng/l, respectively. Serum fTLI concentrations were measured using an analytically validated radioimmunoassay (RIA) with an RI of 12–82 μg/l. 9 Serum fPLI concentrations were measured using an analytically validated RIA. 10 Population-based RIs have been established for all analytes (ie, cobalamin, folate, trypsin-like immunoreactivity, 9 pancreatic lipase immunoreactivity 11 and DI 12 ) except fecal FAs. All individuals performing serum assays were blinded to whether samples were from an EPI or healthy control subject.
Fecal samples
Acceptable fecal samples had to have been collected and received for analysis within 4 weeks of the enrollment fTLI. Naturally voided, healthy control feces (stored at 4°C) collected within 24 h of blood drives were stored at −20°C until batch processing for the DI. For EPI cats, storage conditions were at the discretion of the submitting veterinarian, recommended to be in accordance with current guidelines (eg, 4°C for up to 48 h, then −20°C until analysis). The fecal samples were shipped to the Gastrointestinal Laboratory on ice and stored at −20°C until batch processing. Remaining feces were stored and frozen at −80°C for DI and FA batch processing in January and April 2025 for healthy and EPI cats, respectively.
Microbiota DNA was extracted and DI calculated as previously described. 12 Fecal FAs (arachidonic acid, nervonic acid, total measured FAs) were processed as previously described. 13 All individuals performing fecal assays were blinded to whether samples were from an EPI or healthy control subject.
Clinical signs
Select clinical signs for EPI cats were obtained both at the time of enrollment and during a short-term follow-up period, including vomiting, diarrhea, abnormal appetite (increased or decreased), lethargy and weight loss. These parameters were selected based on a large retrospective of cats diagnosed with EPI. 3 Medical records obtained at the time of enrollment were reviewed by one of the investigators (AH). Short-term follow-up clinical data, including euthanasia, were obtained for all cats at the latest point possible before enrollment closed. If a clinical parameter was not mentioned, it was scored as absent.
Statistical analysis
Categorical data were described using frequencies and percentages. Quantitative data were assessed for normality by calculating descriptive statistics, plotting histograms and performing the Anderson–Darling test in commercial software (MINITAB Statistical Software, Release 13.32; Minitab). Quantitative data were described using the median and range as normality was violated for the majority of variables. Data distributions that violated the normality assumption were transformed using a natural logarithm or rank transformation. Data were compared between EPI and blood donor cats using Mann–Whitney U-tests or Student t-tests for non-normal and normally distributed data, respectively. Biomarkers were compared between blood donor and EPI cats using general linear models including cat population (EPI vs blood donor), age, weight, BCS and breed as fixed effects to investigate the potential for confounding. The same analysis was performed excluding cats receiving prior or current medical therapy at the time of enrollment to ensure significant findings were not influenced by treatments. Breed was categorized as domestic shorthair, purebred or mixed for analysis. Unless stated otherwise, all analyses were performed in available software (SPSS Statistics Version 30; IBM) with significance set as P <0.05. GraphPad Prism version 10.0.0 for Windows (GraphPad Software) was used to create all figures.
Results
EPI cases
Figure 1 illustrates the reasons cats were excluded from the originally screened population (n = 487) to end up with the final subjects for inclusion (n = 55), including non-survivors.

Flow diagram outlining reasons for exclusion of cats from the original screened to the final study population
Of the enrolled EPI cases, 36/55 (65.5%) were domestic shorthairs, 14/55 (25.5%) were purebred and 5/55 (9%) were crossbred cats (including domestic longhairs). Purebreds included Maine Coon (n = 7) and one each of British Blue, Snowshoe, Siberian, Rag Doll, Japanese Bobtail, Bengal and Himalayan. There were 33 spayed females and 21 castrated males. Two (3.6%) cases were already diagnosed with EPI at the time of initial serum sample submission. Table 1 summarizes diet, medications and comorbidities of the EPI cases at the initial time point. Figure 2 shows sampling timelines between blood and fecal samples for all EPI cases.
Summary of suspect comorbidities, medications (within the past month) and diets (within the month) for exocrine pancreatic insufficiency (EPI) cases at the time of case enrollment (feline trypsin-like immunoreactivity [fTLI] submission) (if cases received more than one diet in the last month or at same time, all diets were recorded)

Data are n (%)
Active or diagnosed within the past month; based on submitting veterinarian’s diagnosis list or comments in medical records, imaging or blood work results provided on medical records from within the month of the fTLI submission
Suspected hepatopathy or cholangiopathy based on blood work (elevated liver values), ultrasound imaging changes and/or submitting veterinarians’ diagnosis list
Cardiomyopathy due to echocardiogram or history of elevated proBNP
Potential chronic enteropathy based on submitting veterinarian listing inflammatory bowel disease on differential list or on medical record as comorbidity, mention of intestinal thickening (on palpation or imaging) or via intestinal biopsies (n = 1)
Potential pancreatitis based on submitting veterinarian listing pancreatitis on differential list or on medical records as comorbidity, mention of pancreatic changes on ultrasound
Antibiotics included pradofloxacin, metronidazole, cefovecin, amoxicillin-clavulanate and tylosin
CKD = chronic kidney disease; FIP = feline infectious peritonitis; GI = gastrointestinal; HP = hydrolyzed protein; PERT = pancreatic enzyme replacement therapy; PO = per os

Days between initial feline trypsin-like immunoreactivity and fecal sample collection for exocrine pancreatic insufficiency (EPI) cats. The x-axis represents the number of days in between the two samples, with the number of EPI cases on the y-axis
Healthy controls
A total of 37 healthy cats were enrolled as controls. Of the healthy controls, 20/37 (54%) were domestic shorthairs, 8/37 (21.7%) were purebreds and 9/37 (24.3%) were crossbred cats. Purebreds included Siamese (n = 2), American Shorthair (n = 3), Norwegian Forest Cat (n = 2) and Snowshoe (n = 1). There were 22 spayed females and 15 castrated males. Healthy control cats did not receive antibiotics within 6 months of sample collection, except for one case that received doxycycline for an upper respiratory tract infection 4 weeks before inclusion.
Serum and fecal analytes
Table 2 shows a comparison of serum and fecal variables between the cats with EPI and healthy controls. Results of the separate analysis excluding the EPI cats receiving various treatments (see Table S1 in the supplementary material) identified no differences in results compared with the original analysis. Therefore, all 55 cats remained in the study. Table 3 shows how many cats in each population fell within, below or above the previously established population-based RIs for each blood and fecal outcome measure. Figures 3 and 4 represent the raw, untransformed data for all outcome variables for all cats. Figure S1 in the supplementary material shows raw data for all non-statistically analyzed components of the DI.
Descriptive statistics and comparison of variables between 55 cats diagnosed with exocrine pancreatic insufficiency (EPI) enrolled between April 2024 and February 2025, from 54 veterinary hospitals, and 37 apparently healthy blood donor cats enrolled from a single referral veterinary hospital (TAMU Veterinary Hospital) between November and December 2023

Based on Student’s t-tests or Mann-Whitney U tests for normally distributed and non-normally distributed data, respectively
Based on general linear models on ranks of the variable (‡), natural logarithm transformed data (¶) or untransformed data (§) for the cat population (EPI yes/no) as a fixed effect while adjusting for age, breed, weight and BCS as potential confounders
Mann–Whitney U-tests
Student’s t-test on untransformed data
Student’s t-test on natural logarithm transformed data
BCS = body condition score; NA = not applicable; PLI = pancreatic lipase immunoreactivity; TLI = trypsin-like immunoreactivity
Proportions of cats in each population which fell below, within and above the population-based reference interval (RI) for analytes that have had a previously established RI

Data are n (%)
DI = dysbiosis index; EPI = exocrine pancreatic insufficiency; PLI = pancreatic lipase immunoreactivity; TLI = trypsin-like immunoreactivity
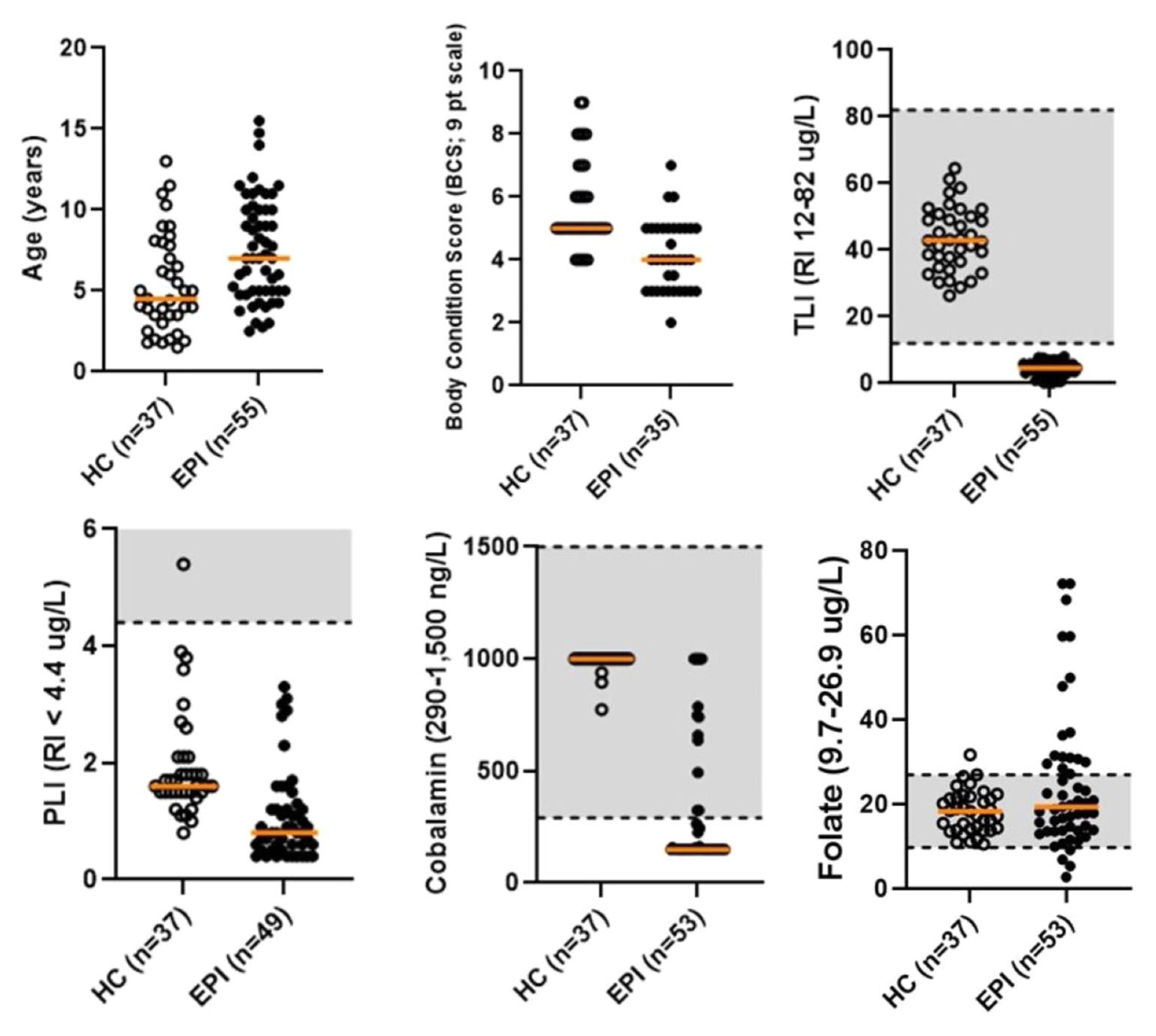
Raw data for all blood analytes for exocrine pancreatic insufficiency (EPI) and healthy control (HC) cats before model transformed values. The horizontal orange lines represent the median for each data set, while horizontal dashed lines and shaded gray areas denote the upper and lower reference intervals (RIs) for each analyte. PLI = pancreatic lipase immunoreactivity; TLI = trypsin-like immunoreactivity

Raw data for all fecal analytes statistically analyzed for exocrine pancreatic insufficiency (EPI) and healthy control (HC) cats, prior to model transformed values. The horizontal orange lines represent the median for each data set, while horizontal dashed lines and shaded gray areas denote the upper and lower reference intervals (RIs) for each analyte with an established population-based RI. DI = dysbiosis index; FAs = fatty acids
Clinical signs at enrollment and follow-up (EPI cases)
Short-term follow-up clinical signs for the EPI cases were recorded within a 10-month period after enrollment (range 2 weeks–10 months), with 8/55 (14.5%) cases being within 4 weeks. Table 4 shows descriptive data for the five clinical signs documented and proportion of cats with clinical signs present at follow-up compared with baseline.
Clinical signs for the exocrine pancreatic insufficiency cases at the time of case enrollment (feline trypsin-like immunoreactivity submission) and during patient follow-up*

Data are n (%) unless otherwise indicated
Cases that were euthanized (n = 5) at time of follow-up medical record request were excluded in the follow-up evaluation. Percentage reduction in clinical signs is reflective of the decrease in the overall percentage of the population affected at follow-up, compared with baseline
Appetite for baseline: 18 (32.7%) with ravenous appetite, 13 (23.6%) with decreased appetite
Appetite for follow-up: 5 (10%) with ravenous appetite; 3 (6%) with decreased appetite
Medications initiated between enrollment and follow-up (EPI cases)
After enrollment, treatments initiated in the EPI cats included the following: PERT (48/55, 87.2%), cobalamin (44/55, 80%), steroids (15/55, 27.3%), anti-nauseas (11/55, 20%), antibiotics (10/55, 18.2%), probiotics (9/55, 16.4%), mirtazapine (7/55, 12.7%) and (1/55, 1.8%) each for cyclosporine, chlorambucil, cisapride and capromorelin. Antibiotics recorded included ampicillin-sulbactam, amoxicillin, doxycycline, enrofloxacin, marbofloxacin, metronidazole, pradofloxacin and tylosin. Although doses for PERT were not reliably recorded, owners of 12 (21.8%) cats reported difficulty with administering PERT.
Discussion
To the authors’ knowledge, this is the first study to show that cats with EPI have an abnormal microbiota and altered FA profiles compared with healthy controls.
Over 50% of this population of EPI cats had significant dysbiosis. This finding was true for comparisons with control cats of all ages, weights and BCS based on our adjusted analysis. This suggests that changes in outcome measures are likely not attributable to differences in patient demographics between groups. A significant decrease in P hiranonis was found in this population of EPI cats, contributing greatly to the abnormal DI. This bacteria is a major contributor of conversion of primary to secondary BA in the intestinal tract of dogs and cats.5,13 BAs are known to play a large role in GI homeostasis and do influence local microbial populations, with certain secondary BAs associated with carcinogenesis in people. 14 A limitation of this study is that fecal BAs were not measured, making it difficult to interpret the clinical significance of the reduced P hiranonis finding. Nevertheless, we suspect cats with lower P hiranonis likely had secondary BA dysregulation, as shown previously. 15 Dogs with EPI have been reported to have higher fecal Bifidobacterium species compared with healthy dogs, 4 although this was not appreciated in this population of EPI cats.
Prospective clinical trials are necessary to know whether the dysbiotic states of the EPI cats in this study contributed to persistent clinical signs at follow-up. Of note, subsets of PERT-treated EPI dogs have been found to be dysbiotic, especially those cases with persistent clinical signs.4,5 Although this theory has yet to be investigated prospectively, this might suggest that intestinal dysbiosis could be a contributing factor in persistent or unresolved clinical signs in PERT refractory dogs. In a retrospective paper of 150 cats with EPI, although 60% of cats had a good treatment response, 27% and 13% of cats had partial or poor to no response, respectively. 3 Although most cats in our study had improvements in weight loss (79%), appetite disturbances (74%) and lethargy (88%), vomiting and diarrhea were persistent in 65% and 54% of cats compared with baseline, respectively. Comorbidities such as CE were not an exclusion criterion, with up to 45% of cases suspected to have concurrent CE. It cannot be determined from this study whether the dysbiosis in these cats is due to a primary malabsorptive state, underlying or concurrent CE, or a combination of both. Regardless, this finding underscores a need for improvement in the treatment and management of EPI in cats that are unresponsive to PERT therapy alone.
Cats with EPI in this study also displayed higher fecal FAs, particularly arachidonic acid and nervonic acid. This finding is similar to the FA abnormalities in cats with CE. 13 Long chain FAs have a wide effect on gene expression that influences inflammation and immune responses. 16 In people, fecal arachidonic and nervonic acid have been shown to be higher in cases of inflammatory bowel disease, serving as potential biomarkers of disease.17,18 It is thought that fecal arachidonic acid is mainly derived from injured epithelial cells. 17 Nervonic acid is an integral part of sphingomyelin and ceramide structure, which is a critical component for normal cell signaling function and also important for epithelial cell structure. The serum metabolome of dogs with EPI has shown elevations in metabolites consistent with intestinal inflammation, but it is still unknown if this is a cause, consequence or representative of a separate intestinal comorbidity. 19 There are several possible explanations for why cats with EPI in our study have higher fecal FAs. These include the following: (1) changes in lipid metabolism secondary to lack of pancreatic enzymes or dysbiosis; (2) damaged intestinal epithelium from pancreatic enzyme deficiency or dysbiosis; or (3) a high prevalence of concurrent inflammatory CE. It is difficult to distinguish whether the elevated fecal FAs is a consequence, cause or both of the underlying disease pathology. Approximately 45% of the EPI cases in this study were noted to have suspect concurrent intestinal disease, such as thickened bowel loops on palpation or via abdominal imaging and one case via biopsies. Our results highlight the need to evaluate cats with EPI for concurrent CE, whether it is sequelae of the EPI or a comorbidity, especially in cases not responding to PERT.
A secondary aim was to describe the clinical presentation and short-term follow-up outcome in cats newly diagnosed with EPI. Weight loss was the most common clinical sign in the largest retrospective feline EPI study 3 to date, with diarrhea uncommon compared with what is reported with canine EPI. Our study results mirror that weight loss was the most common clinical sign in the EPI cases, with 80% of cases reporting weight loss at enrollment. Conversely, diarrhea was only reported in 40% of the cases. The median age of EPI cats in this study was 7 years, also reflecting that of Xenoulis et al. 3 Follow-up data in our population of EPI cats showed that although there was overall improvement in the initial weight loss, appetite disturbances and lethargy, vomiting and diarrhea persisted in a large number of cats. Xenoulis et al found that up to 20% of 150 EPI cats were thought to have concurrent CE. Similar to our study, a subset of cats failed to respond to PERT therapy; 3 it is unknown if this was due to comorbidities or other differences within that EPI population. These repeatable findings reiterate the need for larger scale studies looking at comorbidities, therapies in addition to PERT and long-term follow-up in feline EPI.
There are several limitations to this study. As it aimed to look at differences in a select population of cats diagnosed with EPI over a set time frame, no sample size calculation was performed. Despite this, several significant differences were identified between EPI and control animals. This was a strictly observational study; therefore, standardization of treatments, diets and diagnostics performed was lacking. Medications (including antibiotics) and diets could have been changed from the time between serum and fecal collection without documentation, as over half of the cats in this study had more than 1 week between samples. Fecal samples were batch processed per group, and although they were stored at recommended conditions we cannot say if this impacted quantitative fecal outcome variables between groups. Clinical sign data were based on medical records from veterinarians and owners rather than cases seen primarily by the authors, which might have inconsistences, be missing important information and be subject to recall bias. The follow-up timeline was also not controlled, with a range of a few weeks to approximately 10 months from baseline to follow-up time points. Although this time range could all be considered short-term follow-up relative to the entirety of a cat’s life, there might be significant differences in clinical sign outcome parameters within even a few months of therapy. Two cases had been previously diagnosed with EPI at the time of enrollment. However, as seen with two studies in dogs with EPI, those that were treated or untreated with PERT both still showed a significant difference with fecal microbiota compared with healthy controls.4,5 Despite these limitations, many differences were still found between cats with EPI and healthy controls, and believed by the authors to be reflective of cases seen in practice.
Conclusions
Cats with EPI were more likely to have a higher fecal DI, decreased P hiranonis and increased fecal FAs compared with healthy controls. Clinical signs at diagnosis were similar to those reported previously for cats and differ from those reported most commonly in dogs. Controlled studies should further investigate the fecal microbiota, FAs and BAs in PERT responsive and unresponsive EPI cats to determine if targeted therapeutics for the microbiota (eg, probiotics, fecal microbiota transplantation) would improve clinical outcomes.
Supplemental Material
Figure S1
Raw data for non-statistically analyzed components of the dysbiosis index.
Supplemental Material
Figure S2
The STROBE-Vet statement checklist.
Supplemental Material
Table S1
Descriptive statistics and comparison of variables between 37 cats diagnosed with exocrine pancreatic insufficiency enrolled from April 2024 to February 2025.
Footnotes
Acknowledgements
The authors would like to acknowledge the genetics and metabolomics employees within the Gastrointestinal Laboratory for acquisition of outcome measure data.
Correction (June 2026):
This paper has been updated to correct fTLI in Figure 1.
Supplementary material
The following files are available as supplementary material:
Figure S1: Raw data for non-statistically analyzed components of the dysbiosis index.
Figure S2: The STROBE-Vet statement checklist.
Table S1: Descriptive statistics and comparison of variables between 37 cats diagnosed with exocrine pancreatic insufficiency enrolled from April 2024 to February 2025.
Conflict of interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: three of the authors (EG, CHC, JS) are employed by the Gastrointestinal Laboratory at Texas A&M University, which offered the assays in this article on a fee-for-service basis.
Funding
This study was in part supported by the Purina Petcare Research Fund.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.