
Abstract
Objectives
The aim of this study was to evaluate the accuracy of cone-beam CT (CBCT) for predicting implant position relative to the vertebral canal in the feline thoracolumbar vertebral column.
Methods
This in vitro imaging and anatomical study included 22 feline cadavers. A realistic surgical approach was performed at three thoracolumbar locations. Four smooth 1.2 mm Kirschner wires were inserted per location using the recommended insertion points. Perforation of the spinal canal was not avoided. Images from end-on fluoroscopy (eoF), multi-slice CT (MSCT) and CBCT using a C-arm were obtained. The images were randomised, and the implant position was assessed by four evaluators who classified implant position and recorded their subjective certainty. Sensitivity, specificity and accuracy were calculated using anatomical dissection as the reference standard. Interrater agreement was assessed using Fleiss’ kappa (κ). Duration of image acquisition was compared across modalities using a mixed-effects linear model.
Results
For eoF, the sensitivity and specificity were 81.9% and 80.7%, respectively, with a balanced accuracy of 81.3% (95% confidence interval [CI] 0.79–0.84) and good κ agreement (0.63). For MSCT, sensitivity was 80.2% and specificity was 83.1%. Balanced accuracy was 81.7% (95% CI 0.79–0.84) and κ was good (0.63). CBCT showed a sensitivity of 88.5% and specificity of 83.4%, with a balanced accuracy of 85.9% (95% CI 0.84–0.88) and good κ agreement (0.72). Interrater reliability showed overall κ values of 0.38 for eoF, 0.54 for MSCT and 0.58 for CBCT. Interrater reliability was higher for completely perforating and non-perforating implants and lower for partially perforating implants. CBCT and eoF were performed faster than MSCT (P <0.01).
Conclusions and relevance
Intraoperative C-arm-based CBCT is an accurate and fast method for assessing pin position in relation to the thoracolumbar spinal canal in cadaveric cats.
Keywords
Introduction
Vertebral fractures and luxations in cats often result from trauma, such as falls from a great height or motor vehicle accidents, and occur with a prevalence of 3.5% of all fractures. 1 The thoracolumbar spine, including the T3–L3 spinal segment, is most frequently affected in cats, followed by L4–L7.2–4 Choice of conservative or surgical treatment depends on the neurological status and the biomechanical stability of the fracture.5–8 Various stabilisation techniques have been described, but pins and polymethylmethacrylate are often used in cats because of the small size of the vertebral bodies and proven stability. 5 To avoid injury to the spinal cord and other sensitive structures by perforation of implants into the spinal canal, anatomical insertion points and angles have been defined.9–11 The most common way of implant placement is the freehand technique.12,13 To ensure the correct position of the implants, intra- or postoperative imaging is required. Standard radiographs have low sensitivity for detecting spinal canal perforation, with only 51% of cases identified in a study on dogs. 14 CT has a reported accuracy of 93% to detect perforation of the spinal canal and is therefore considered the gold standard. 14 Multi-slice CT (MSCT) has the disadvantage that imaging can be performed only postoperatively in most cases. 15 Intraoperatively, end-on fluoroscopy (eoF), with a sensitivity of 98.8% and specificity of 98.0% according to one study, can be performed using a C-arm. 15 Multiple studies in human surgery over the past years have shown that three-dimensional imaging is advantageous and offers better intraoperative control. 16 Cone-beam CT (CBCT) is a newer imaging technique 17 that uses x-ray beams and a flat panel detector rotating around the patient. 18 Differences between MSCT and CBCT include mechanical components such as detector type, image acquisition mode and image characteristics, including a smaller field of view, lower soft tissue contrast resolution and higher spatial resolution for CBCT compared with MSCT. 19 With CBCT, CT can be performed intraoperatively, enabling immediate multiplanar evaluation after implant placement. 20 Studies in dental, maxillofacial and orthopaedic surgery have demonstrated that CBCT reduces metal artefacts and improves image quality.18,21,22 In veterinary medicine, CBCT has been reported to be a superior modality for visualising oral structures, particularly dentoalveolar anatomy.23,24 To the authors’ knowledge, however, few studies have investigated the vertebral spine of companion animals using CBCT.
The aim of this study was to compare intraoperative CBCT with conventional MSCT and eoF for accurate assessment of implant position relative to the vertebral canal in feline cadaveric vertebral spines. The first hypothesis was that both CT modalities would demonstrate similar accuracy. The second hypothesis, considering only intraoperative imaging modalities, was that CBCT would be a more accurate and faster technique than eoF for assessing implant position.
Materials and methods
Adult feline cadavers (n = 22), euthanased for reasons unrelated to this study, were collected and frozen (–20°C). Ethical approval by an institutional entity was granted (AZ 402-27-05-2024). The cadavers were thawed for 24 h before evaluation. Orthogonal radiographs of the spines were obtained to exclude skeletal pathologies. The exclusion criteria consisted of pathologies of the thoracolumbar vertebral spine and skeletal immaturity.
Three locations (T12–T13, L2–L3 and L5–L6) were chosen. One vertebral segment was left free between each simulated fracture to minimise metal artefacts during diagnostic imaging. The paraspinal musculature was preserved to simulate realistic conditions for evaluation of the imaging techniques. The cadavers were positioned in sternal recumbency and placed on a radiolucent acrylic glass table for eoF and CBCT to avoid artefacts. A dorsal approach was used to access each of the three locations. For simulated fracture stabilisation, smooth 1.2 mm Kirschner wires (K-wires) (Mede Technik) were inserted bicortically into the thoracolumbar vertebral columns by a board-certified surgeon (MK). At each location, four K-wires were inserted using recommended insertion points; however, insertion angles were varied, and perforation of the spinal canal was not avoided.
To obtain eoF and CBCT images, a mobile C-arm was used (Cios Spin; Siemens Healthineers) (Table 1, Figure 1). 25 To obtain an end-on view of each pin, the C-arm was adjusted so that the fluoroscopic beam was precisely aligned with each pin. The CBCT was acquired using the same device after aligning the beam to the region of interest based on orthogonal radiographs. Reconstruction was generated by the system in three planes; detailed hardware specifications are not publicly disclosed (Table 1). The system software automatically applies a set of predefined correction algorithms, including metal artefact reduction, scatter correction, iterative edge-preserving reconstruction and motion correction. These processing steps are intended to reduce metal-induced streak artefacts, ring artefacts, scatter-related contrast degradation and motion-related blurring. 25 Optional advanced reconstruction protocols are available but were not utilised in the present study as such options were not available for MSCT. MSCT was performed with a 64-line multi-slice device (SOMATOM Definition AS 64; Siemens) (Table 1, Figure 1). Subsequently, reconstruction in three planes was performed. No additional metal suppression or enhanced CT mode was applied.
Imaging acquisition and reconstruction parameters of multi-slice CT (MSCT) and cone-beam CT (CBCT) according to Guidelines for Reporting Image Acquisition Technical Parameters, revised by the Veterinary Radiology & Ultrasound Editorial Board 26
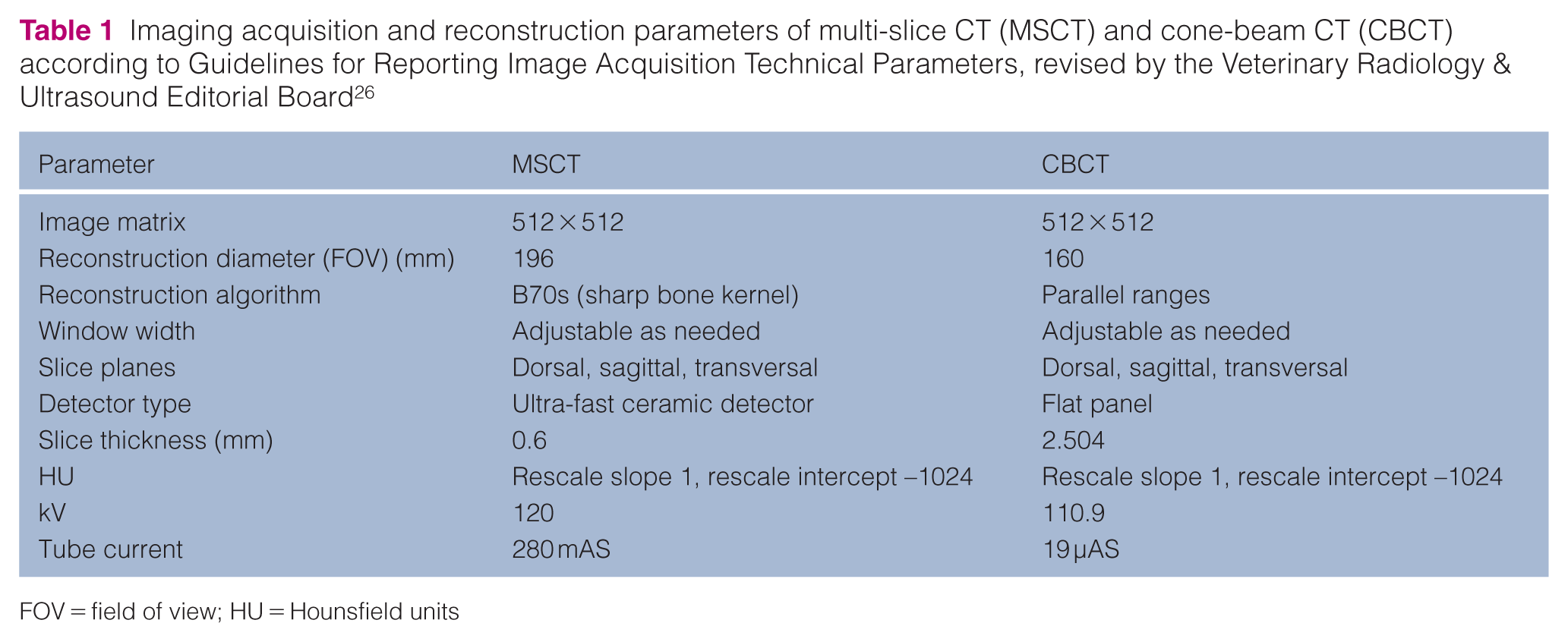
FOV = field of view; HU = Hounsfield units
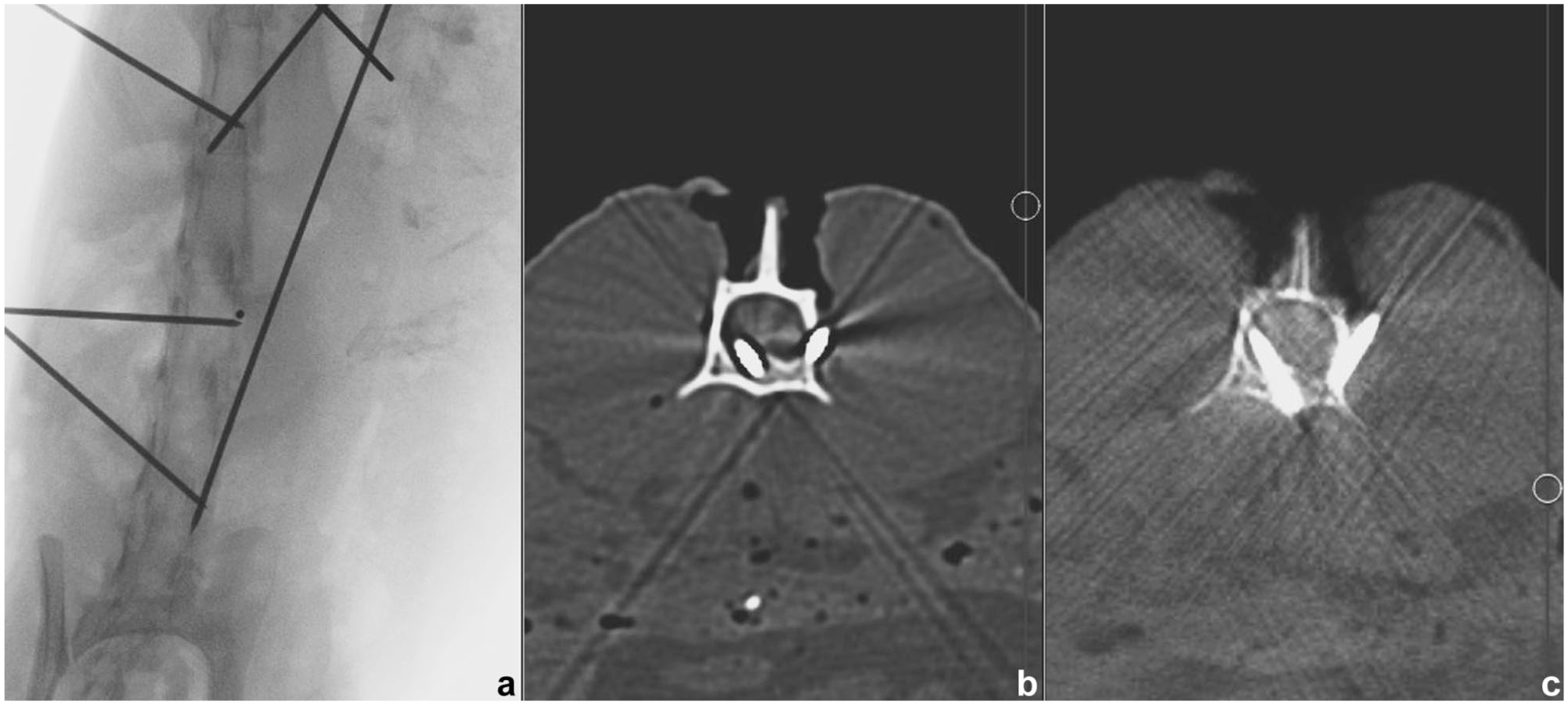
Exemplary images of the fifth lumbar vertebra with the same right-sided pin not perforating the spinal canal according to the gold standard in the three modalities investigated: (a) end-on fluoroscopy (pin visible as a circle), (b) multi-slice CT and (c) cone-beam CT
The duration of the image generation and reconstruction of each location (four K-wires) was documented. For evaluation, a standardised numeration of the K-wires was applied. Anatomical preparation of the spines was used for verification of pin position in relation to the spinal canal and defined as the gold standard. The K-wires were graded as completely, partially or not perforating the vertebral canal. The cadavers and respective images were randomised, and the implant position was assessed by four evaluators (two Diplomates of the European College of Veterinary Surgeons [ECVS] [MK, JS], one Resident of the ECVS [CK] and one Diplomate of the European College of Veterinary Diagnostic Imaging [JK]). Evaluation was performed at least 2 weeks after implant placement to minimise evaluator bias. The evaluators were allowed to use a DICOM viewer and adjust window settings as needed. They determined whether the vertebral canal had been perforated. Perforating implants were further classified as either partially or completely perforating the vertebral canal. Finally, the evaluators’ subjective confidence in the assessment of each implant was documented as either certain or uncertain.
All statistical analyses were performed using R version 4.4.1 software. 27 The diagnostic performance of each imaging modality was assessed using confusion matrix analysis. Sensitivity, specificity, balanced accuracy, positive predictive value (PPV) and negative predictive value (NPV) were calculated with anatomical preparation findings serving as the reference standard. Implants were categorised into three groups – non-perforating, partially perforating and completely perforating – and results were compared across these categories. As a result of repeated measurements, mixed-effects logistic regression was used to predict results. Imaging modality was included as a fixed effect. The outcome variable was the presence or absence of vertebral canal perforation, with ‘no vertebral canal perforation’ defined as the reference category. The random-effects structure included crossed random intercepts for cadaver number, implant position and evaluator. In addition, a mixed-effects logistic regression model was used to estimate the probability of certainty. The model included an interaction term between the result category (non-perforating, partially perforating, completely perforating) and the imaging modality (CBCT, eoF, MSCT), while maintaining a similar random-effects structure. Inter-observer agreement among the four observers was calculated using Fleiss’ kappa (κ). The following qualitative classifications for κ coefficients were used: excellent (0.81–1.00), good (0.61–0.80), moderate (0.41–0.60), borderline (0.21–0.40), poor (0.00–0.20) and bad (<0.0). 28 Statistical significance was set at P <0.05. The duration of the imaging modalities was compared using a robust mixed-effects linear model.
Results
For this study, 22 cadavers (13 female, nine male) of domestic shorthair cats, with a mean weight of 3.0 kg (range 1.9–4.7), were used. None of the vertebral columns had radiographic evidence of bony lesions. A total of 264 smooth 1.2 mm K-wires were inserted; however, 263 pins were evaluated because one was lost in anatomical preparation. According to the gold standard, 141 K-wires did not perforate the vertebral canal, 70 K-wires partially perforated the vertebral canal and 52 K-wires completely perforated the vertebral canal. The numbers of the cadavers and location of the K-wires were randomised for evaluation.
Diagnostic performance
All modalities demonstrated high overall diagnostic accuracy relative to the reference standard. Accuracy was highest for CBCT (balanced accuracy = 85.9%), followed by MSCT (balanced accuracy = 81.7%) and lowest for eoF (balanced accuracy = 81.3%) (Table 2). Across all modalities, accuracy was consistently lowest for partially perforating implants compared with non-perforating and completely perforating implants (Table 2).
Comparison of balanced accuracy, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) across three imaging modalities (end-on fluoroscopy [eoF], multi-slice CT [MSCT] and cone-beam CT [CBCT])

Results are stratified into non-perforating, partially perforating and completely perforating implants
Agreement between eoF-, MSCT- and CBCT-based classifications and the reference standard was assessed (Table 3). Classifications from each imaging modality were compared with the reference standard using Fleiss’ κ. Agreement was moderate for eoF, MSCT and CBCT. Across all modalities, agreement was higher for non-perforating and completely perforating implants and lower for partially perforating implants.
Agreement between end-on fluoroscopy (eoF)-, multi-slice CT (MSCT)- and cone-beam CT (CBCT)-based classifications and the reference standard

Classification of Fleiss’ kappa (κ): excellent (0.81–1.00), good (0.61–0.80), moderate (0.41–0.60), borderline (0.21–0.40), poor (0.00–0.20) and bad (<0.0)
Comparison of the odds of success between modalities showed that there were no significant differences between eoF and MSCT (odds ratio [OR] 0.89, SEM 0.09; P = 0.55) as well as between eoF and CBCT (OR 0.867, SEM 0.09; P = 0.36). Between MSCT and CBCT, there was a statistically significant difference (OR 0.78, SEM 0.08; P = 0.04). These results provide evidence of differences between imaging modalities with respect to the outcome, favouring the performance of CBCT.
Reliability and certainty of evaluators
Interrater reliability among four evaluators demonstrated that, for MSCT and CBCT, Fleiss’ κ values indicated moderate agreement (>0.6) for classifications of non-perforating and completely perforating implants, whereas agreement was borderline (<0.4) for partially perforating implants (Table 4). For eoF, overall interrater reliability was lower, with the lowest level of agreement observed for classification of partially perforating implants (Table 4). Furthermore, diagnostic accuracy declined as the number of evaluators increased. In comparison, analyses involving three evaluators yielded overall κ coefficients of 0.62 for EoF, 0.65 for MSCT and 0.66 for CBCT.
Interrater reliability of four raters for evaluation of end-on fluoroscopy (eoF), multi-slice CT (MSCT) and cone-beam CT (CBCT) images, highlighting the differences between the classification groups by Fleiss’ kappa (κ) coefficient
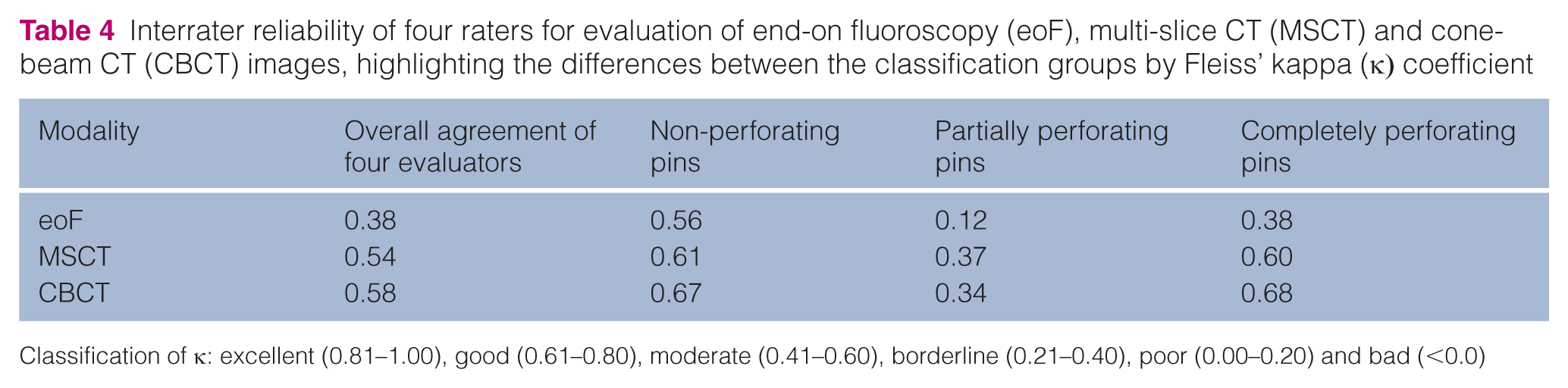
Classification of κ: excellent (0.81–1.00), good (0.61–0.80), moderate (0.41–0.60), borderline (0.21–0.40), poor (0.00–0.20) and bad (<0.0)
All evaluators rated their subjective certainty in assessing the implant position as either certain or uncertain. Across all modalities, the probability of certainty (43.9%, 95% CI 2.84–6.07) was lower than the probability of uncertainty (55.7%, 95% CI 3.86–7.15). The odds of uncertainty were significantly higher (OR 0.62, SEM 0.13; P <0.01). Comparison of evaluators’ certainty across all modalities showed that eoF demonstrated the greatest separation between perforation categories. In contrast, CBCT and MSCT yielded comparable results, with no significant differences between them, whereas both differed significantly from eoF. This indicates a modality-dependent effect, with cross-sectional imaging (MSCT and CBCT) demonstrating more consistent performance than eoF (Figure 2). Certainty for partially perforating implants was significantly lower than for non-perforating and completely perforating implants, whereas no difference was observed between non-perforating and completely perforating implants for MSCT and CBCT (Table 5).
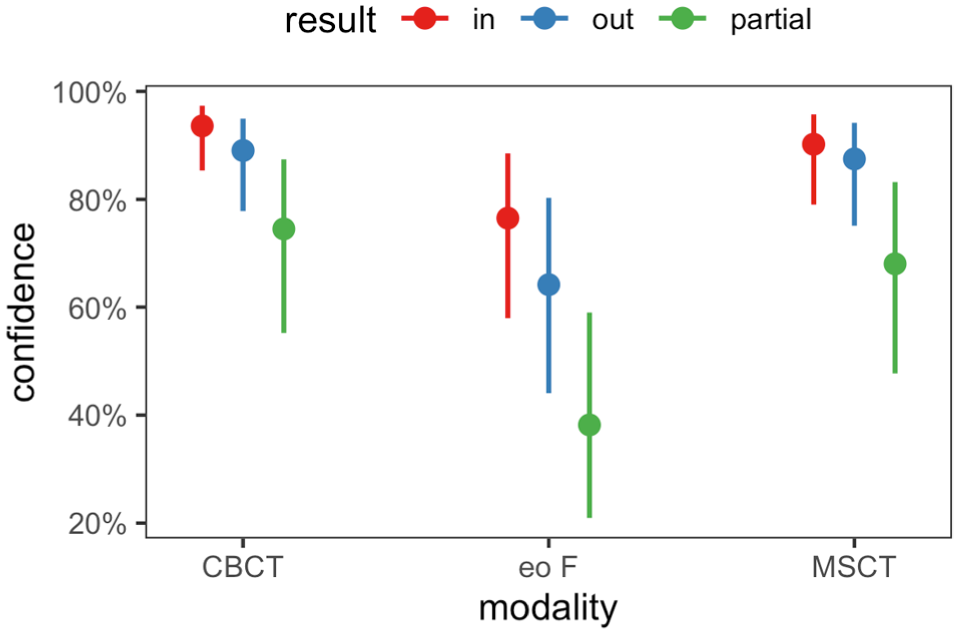
Probability of evaluator certainty for three imaging modalities with different degrees of implant perforation of the spinal canal. CBCT = cone-beam CT; eoF = end-on fluoroscopy; MSCT = multi-slice CT
Pairwise odds ratio (OR) comparisons of evaluator certainty among end-on fluoroscopy (eoF), multi-slice CT (MSCT) and cone-beam CT (CBCT) across varying degrees of implant perforation
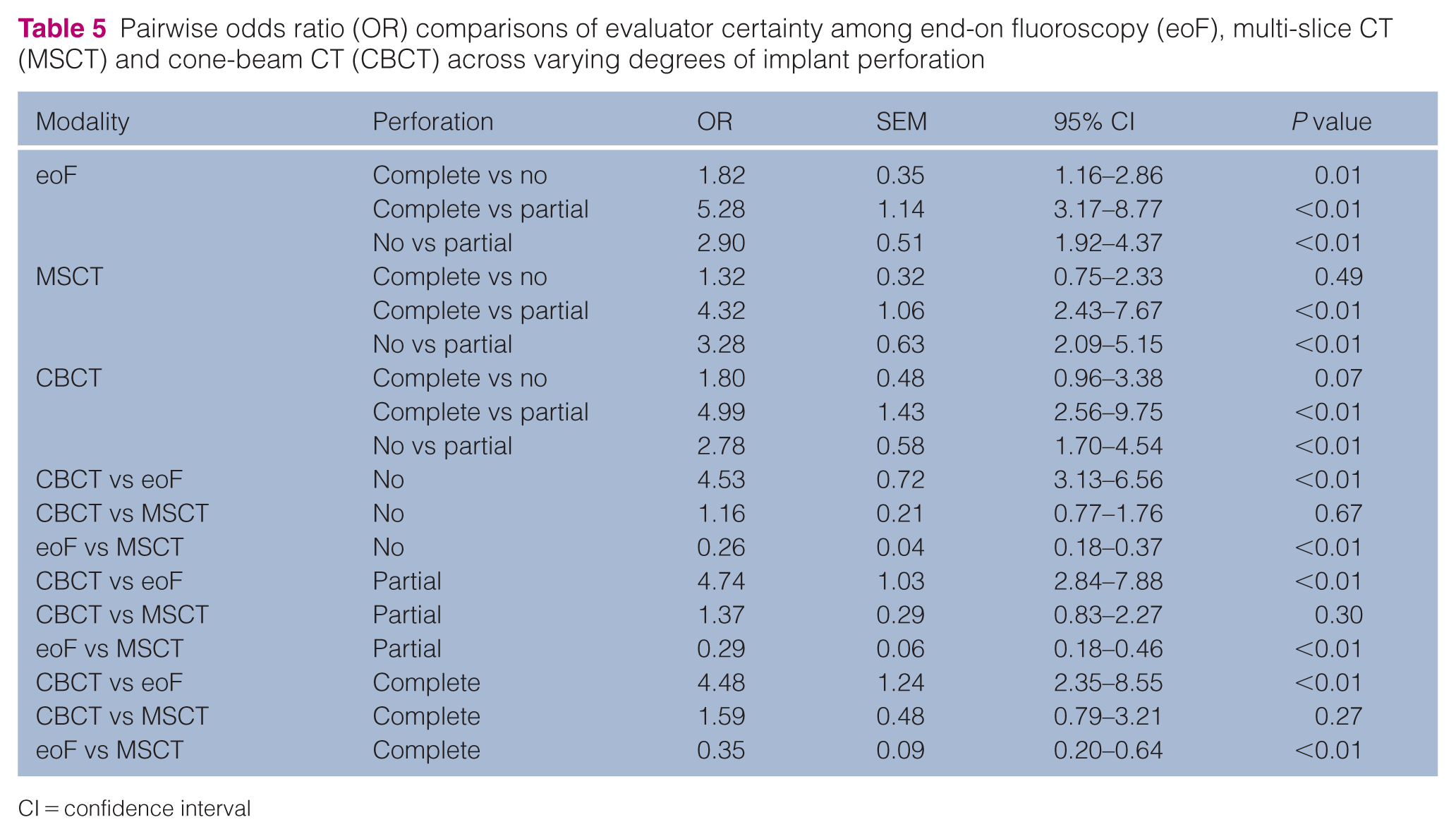
CI = confidence interval
Duration
The duration of all modalities was documented and compared (Table 6). CBCT and eoF were significantly faster to perform than MSCT (P <0.01). No statistically significant difference was detected between eoF and CBCT (P = 0.58).
Median duration of image acquisition of one location compared across modalities
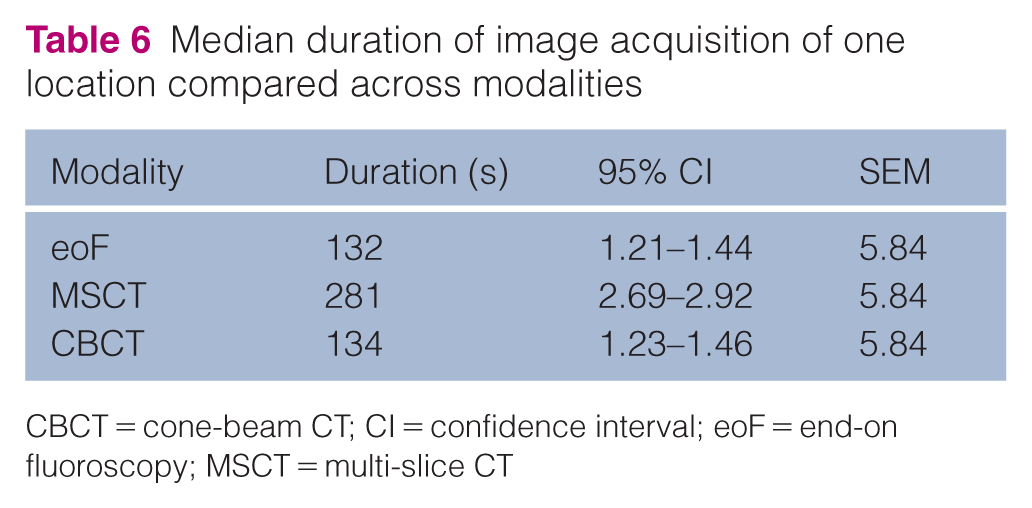
CBCT = cone-beam CT; CI = confidence interval; eoF = end-on fluoroscopy; MSCT = multi-slice CT
Discussion
In this cadaveric study, three imaging modalities were evaluated for their ability to accurately determine the position of K-wires inserted into the feline vertebral spine. The results provide the first evidence that intraoperative C-arm CBCT is an accurate technique for the evaluation of implant position in the feline thoracolumbar vertebral spine. CBCT provided the highest accuracy (balanced accuracy = 85.9%), followed by MSCT (balanced accuracy = 81.7%) and eoF (balanced accuracy = 81.3%). Although CBCT showed numerically higher accuracy, the difference compared with MSCT was small, indicating that both modalities provide comparable accuracy and thereby supporting the first hypothesis. No significant difference was observed in image acquisition time between CBCT and eoF. Therefore, the second hypothesis is not supported.
Image quality is influenced by various artefacts arising from motion, metallic objects or reconstruction inaccuracies.29,30 In CT imaging, these include noise, beam hardening, scatter, pseudo-enhancement, motion, cone beam, helical, ring and metal artefacts. 31 Metal artefacts are of significant interest in implant evaluation, manifesting as beam hardening and high-density edge gradients that produce bright and dark streaks, as well as distortions within the image. 32 The impact of metal artefacts differs between MSCT and CBCT. MSCT uses a fan-beam geometry that, often together with iterative reconstruction algorithms, enables correction of metal artefacts to a certain point. 31 CBCT works with a cone-beam geometry in which an entire volume is captured in a single rotation. This leads to scattering artefacts, 33 particularly the blooming effect, increased scattering and overshoot artefacts. 34 In this study, CBCT image acquisition and reconstruction were performed using predefined manufacturer protocols that include a non-adjustable level of artefact reduction. The use of additional implant mark-up or metal suppression mode could potentially improve image quality. As these features were not available for the MSCT device, they were not evaluated. Device-dependent differences in reconstruction methods between MSCT and CBCT may influence evaluation. A number of studies have compared CBCT with other imaging modalities and found advantages of the modality,24,35 which could explain the greater accuracy and interrater agreement for CBCT images in this study. Iikubo et al 35 compared radiographs, MSCT and CBCT following induction of horizontal fractures in canine incisors. CBCT provided a smaller slice thickness than MSCT and showed significantly greater sensitivity and diagnostic accuracy for detecting fracture lines compared with both radiography and MSCT. Similarly, Soukup et al 24 compared CBCT with a 64-slice MSCT unit for imaging canine maxillary dentoalveolar structures and found CBCT images to be superior in all evaluated image quality categories.
The least accurate modality was eoF. Compared with MSCT and CBCT, eoF is a two-dimensional imaging technique. Concerns regarding the use of intraoperative fluoroscopy compared with CT include the potential for wrong-level surgery, as image projections can be technique-dependent and require extensive anatomical knowledge and experience. 36 Further, retention of the soft tissues may have contributed to greater superimposition on eoF images, as discussed by Goffart et al. 15
Across all analysed modalities, non-perforating and completely perforating K-wires were identified correctly more often than partially perforating K-wires. Partially perforating K-wires appeared more difficult to evaluate, which may be attributable to artefacts or limited image resolution, particularly given the small vertebral bodies in cats. Differences and limitations among imaging modalities may also have contributed to the observed variation. As perforation of the spinal canal was not avoided, an artificially increased prevalence of spinal canal perforation occurred. The PPV and NPV reflect the diagnostic performance of the investigated modalities under controlled conditions. Given the dependence of PPV and NPV on disease prevalence, this likely influenced the reported values. In a clinical setting, spinal canal perforation occurs less frequently, and the PPV would therefore be expected to decrease because of a higher proportion of false-positive findings, whereas the NPV would likely increase.
As previous studies have demonstrated, imaging artefacts can impair accurate image interpretation. In particular, the blooming effect may contribute to false-positive diagnoses of spinal canal perforation by causing implants to appear artificially enlarged. 37 This phenomenon is likely to be more pronounced in cases of partial perforation, where the spatial proximity between the implant margins and the spinal canal reduces the distinguishability of their boundaries. Such effects may account for the reduced diagnostic accuracy observed in partially perforating implants. Further, it may have an impact if the evaluator knows the size of the implant during evaluation to estimate the extent of the artefact. Greater contrast and sharper delineation of the bony margins can be achieved if soft tissue surrounds bony structures. 38 Consequently, soft tissues were retained in this study.
The precise degree of implant perforation into the vertebral canal that leads to neurological deficits is not consistently defined in cats and dogs. In humans and dogs, classifications based on the percentage of screw diameter outside the pedicle have been applied.39,40 However, a study of feline spinal surgery reported that any implant perforating the vertebral canal increases the risk of neurological deficits. 41 Therefore, any violation of the spinal canal should be avoided through careful implant positioning.
Interrater agreement increased from eoF to MSCT and was highest for CBCT, consistent with the diagnostic accuracy found for the modalities. The individual accuracy of the four raters was considered similar despite differences in their specialisation and level of experience. Accuracy decreased as the number of evaluators increased, an effect expected with lower agreement across larger groups of observers. One possible explanation for the converging interrater reliability among modalities may be variation in familiarity with the modalities, particularly eoF. A higher level of evaluator confidence did not correlate with correct assessment. The probability of being uncertain (κ = 0.56) was higher than that of being certain (κ = 0.44). Published data regarding evaluator confidence are inconsistent. High confidence levels have been reported to be unrelated to accuracy in one study 14 but associated with correct assessment in another. 15 The reason for this remains unclear, although individual evaluator differences have been suggested. 15 Whether difficulties were related to three-dimensional visualisation, as proposed by Hettlich et al, 14 is unknown. For future studies, the authors suggest that classification may be facilitated by more detailed specification of certainty levels. A grading system such as ‘certainly no perforation’, ‘possible perforation’ and ‘certain perforation’ may be applicable.
The duration of CBCT and eoF procedures is significantly shorter than that of MSCT. As CBCT is both more accurate than MSCT and faster to perform, its use may also reduce overall anaesthesia time by eliminating the need for postoperative imaging. In contrast, MSCT requires transfer of the patient out of the operating room, thereby prolonging anaesthesia and potentially increasing the risk of infection. 42 In addition, surgical revision is necessary if implants perforate the spinal canal, 42 further supporting the use of CBCT.
This study has several limitations. First, the random angulation of the pins and the high number of pins inserted per cadaver do not accurately reflect a realistic clinical scenario. These factors may have introduced confusion during evaluation and potential evaluator bias, as surgeons generally aim to avoid perforation of the vertebral canal. In a realistic setting, end-threaded positive-profile pins would typically be used because they provide greater pull-out resistance and reduce the incidence of pin displacement and implant failure.42,43 Whether the use of end-threaded pins could introduce artefacts, and thereby affect the accuracy of evaluation results, requires further investigation. The field of view and reconstruction algorithms used for CBCT and MSCT were similar but not identical, which may have affected the evaluation. Fluoroscopy is typically performed as a dynamic imaging process using multiple images (cine loops); however, in this study, only a single image per K-wire was assessed, which may have influenced the interpretation. True fluoroscopy may therefore have improved the results. Finally, as this was a cadaveric study, the findings cannot fully replicate clinical conditions and should be validated in future in vivo investigations.
Conclusions
According to the results of this study, CBCT is an accurate modality for evaluating implant position in cadaveric feline vertebral spines and may represent an alternative intraoperative modality with reduced surgical duration. The modality carries the potential to reduce the incidence of revision procedures. Further investigations are warranted to support this assumption in clinical cases.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.