
Abstract
This research investigates whether Indigenous Populations are disproportionately vulnerable to COVID-19 infection and deaths in Chile. To answer this question, we use a regression model to analyze data from the Chilean government. Our analysis indicates that municipalities with a higher proportion of Indigenous people evinced higher rates of infection and deaths to COVID-19. Indigenous groups were not only highly affected at the beginning of the coronavirus outbreak; their rate of infection and mortality has increased as the virus has spread to the general population. We argue that the COVID-19 pandemic can have devastating effects on Indigenous communities, mainly because it increases the historically accumulated inequalities and structural racism linked to colonization, neoliberalism, and neo-extractivism in Chile.
Introduction and research problem
The Coronavirus pandemic is having a disproportionate effect on particular communities, exacerbating social, gender, and racial/ethnic inequalities (Comisión Económica Para América Latina y el Caribe [CEPAL], 2020). Various community leaders, human rights organizations, and researchers have maintained that Indigenous populations are among the most vulnerable groups to the pandemic and that COVID-19 could have catastrophic effects on their life systems (Ferrante & Fearnside, 2020; Fondo para el Desarrollo de los Pueblos Indígenas de América Latina y El Caribe, 2020; Laurencin & McClinton, 2020; Raifman & Raifman, 2020). This outcome is plausible, fundamentally because Indigenous peoples are facing the pandemic under conditions of racism and structural violence, poverty, inequality, and precariousness accumulated because of the history of colonization (The Anti-Racist Research and Action Network, 2020).
During the last decades, the effects of neoliberal and neo-extractivist logics have increased the vulnerability of Indigenous people in general (Veltmeyer & Petras, 2015), particularly in Chile (CEPAL & Alianza Territorial Mapuche, 2012; Toledo Llancaqueo, 2006). On the one hand, neoliberalism has limited the role of the state as a guarantor of social rights while commodifying them and increasing ethnic/racial inequalities in access to health care (Harvey, 2007; Meneses-Navarro et al., 2020). On the other hand, neo-extractivism has hindered indigenous territorial self-determination through the dispossession and exploitation of natural resources, as well as by undermining the conditions that sustain their communal living (Coordinadora Arauco Malleco, 2019; Melin et al., 2017; Svampa, 2019). To mitigate the impact of these conditions, among other initiatives, Latin American governments have implemented intercultural health models (Organización Panamericana de la Salud, 2008). However, various studies illustrate that the historical situation of impoverishment and structural racism undermines the intended effect of these health policies: Indigenous peoples continue to be vulnerable in the contexts of health care and disease prevention (Sacchi et al., 2007). It has also been demonstrated that intercultural health initiatives act as homogenizing and destabilizing forces against traditional indigenous health systems in Latin America (Navarro et al., 2017; Ramírez Hita, 2014) and Chile (Cuyul, 2012). Other studies further expose the persisting inequalities in access to health care between Indigenous people and the rest of the population, mainly due to linguistic-cultural discrimination (Amoroz, 2011).
In the context of COVID-19 and the systemic vulnerabil-ities of Indigenous populations explained above, this study aims to answer the following research question: Do municipalities with a higher proportion of Indigenous people experience a higher rate of cases and deaths of COVID-19? To address this question, we use a multiple regression model to analyze data from the Chilean government.
Data and methods
The Chilean data stems from two sources. The first dataset comes from the Ministry of Health of Chile (Ministerio de Salud, 2020), and it provides information about the number of cases and deaths due to COVID-19 at the municipal level. To control for the population of each municipality, we used the numbers of cases and deaths of COVID-19 per 100,000 people. The second source comes from the Census of Population and Housing (Instituto Nacional de Estadísticas, 2017). We collapsed the individual data at the municipal level to extract the following variables (by percentage): Indigenous population, gender, employment status, the population living in rural areas, age (eight categories), adult population with higher education, and average years of schooling.
We used two regression models to determine whether municipalities with larger Indigenous populations see more cases and deaths of COVID-19 than the municipalities with smaller Indigenous populations. The dependent variables are the number of COVID-19 cases and number of deaths due to COVID-19 per 100,000 people in each municipality. The independent variables were the percentage of Indigenous population, men, rural population, age group (eight categories), unemployment, population with higher education, and years of schooling. To control for geographic differences, the models use a dummy variable to identify the region where municipalities are located. Municipalities are then compared to each other within each region.
Results
In this section, we present the evolution of infection and mortality rates of COVID-19 over the five-month period following the first reported case in Chile (March 03). Table 1 illustrates that the rate of contagion among municipalities with a high concentration of Indigenous citizens has increased as the virus has spread to the general population. For instance, an increase of 1% of the Indigenous population per municipality implied an increase of 5.1 cases of COVID-19 per 100,000 people at month 3 of the pandemic, 12.5 and 17.5 cases at months 4 and 5, respectively. All the coefficients are statistically significant (p < .05).
Regression model using the total number of individuals infected with COVID-19 per 100,000 people at the municipality level in Chile.
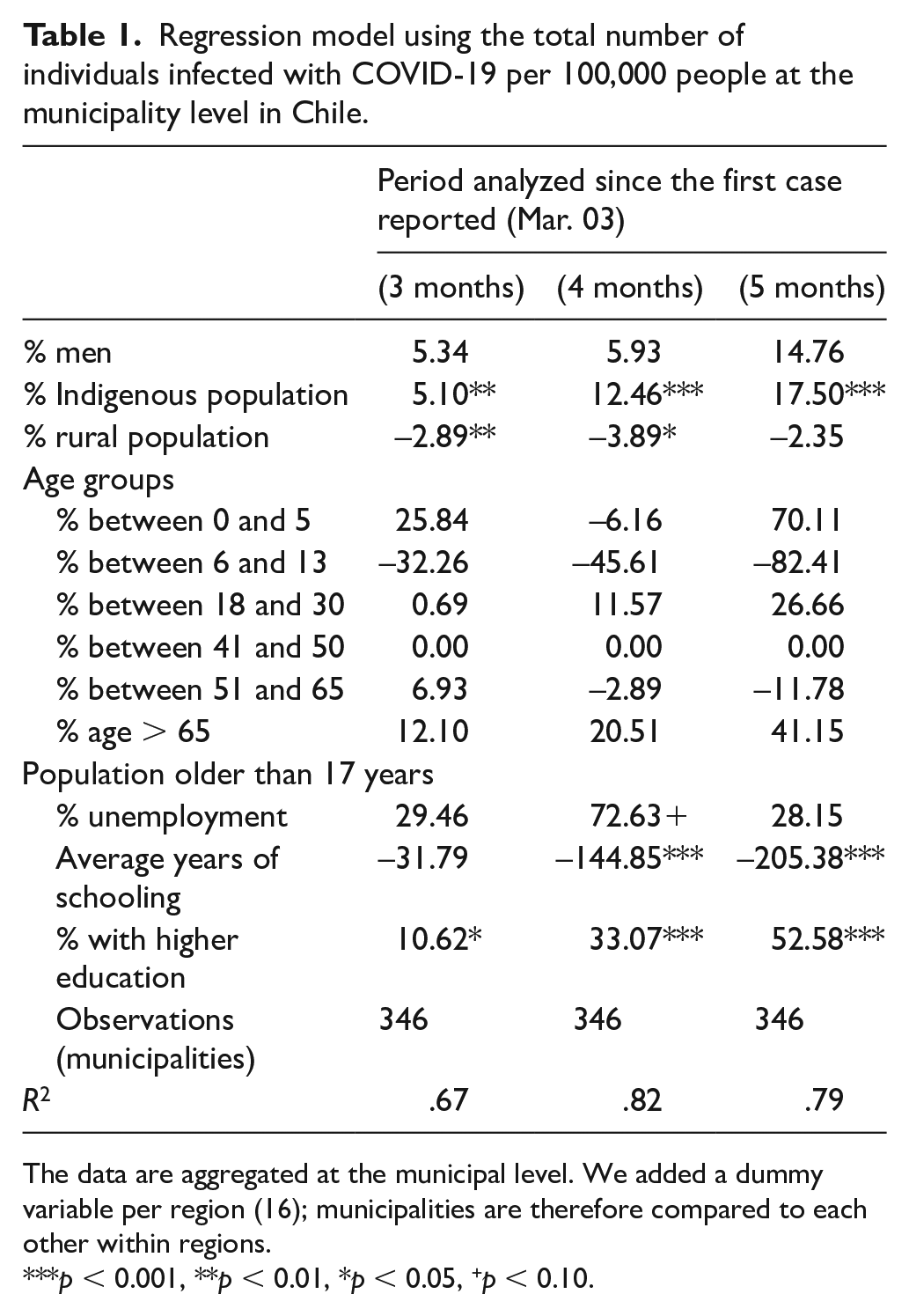
The data are aggregated at the municipal level. We added a dummy variable per region (16); municipalities are therefore compared to each other within regions.
p < 0.001, **p < 0.01, *p < 0.05, +p < 0.10.
Table 2 also shows an upward trend: as COVID-19 has spread across the country, the mortality rate linked to the Indigenous population has risen. For example, an increase of 1% of the Indigenous population per municipality implied an increase of 0.22 deaths per 100,000 people month 3 of the pandemic, 0.39 and 0.50 deaths at 4 and 5 months, respectively. All the coefficients are statistically significant (p < .05).
Regression model using the total number of deaths of COVID-19 per 100,000 people at the municipality level in Chile.

The data are aggregated at the municipal level. We added a dummy variable per region (16); municipalities are therefore compared to each other within regions.
p < 0.001, **p < 0.01, *p < 0.05, +p < 0.10.
Discussion and conclusion
In this study, we have sought to determine whether the Indigenous population in Chile is more vulnerable to COVID-19 than the rest of the population. Our analysis confirms that municipalities with a higher proportion of Indigenous people are not only more susceptible to the virus, but also evince more deaths to COVID-19.
These results point to the devastating effects that COVID-19 is poised to have on the Indigenous population. First, the pandemic may exacerbate the precariousness, vulnerability, and poor living conditions that Indigenous people have been subjected to because of the history of colonization, neoliberalism, and neo-extractivism in Chile. Extractivism is manifest mainly in forestry (radiata pine and eucalyptus) and hydroelectric projects, which have been strongly questioned by Mapuche communities through social mobilization in recent decades (Mella Seguel, 2007). Second, the pandemic has revealed underlying inequalities in hegemonic health care systems, including intercultural models that were already inadequate before COVID-19. In the face of this adversity, Mapuche communities in Southern Chile have not remained passive; instead, they have activated diverse community responses to confront the pandemic based on their strong tradition of organizing. These responses include cordons sanitaires, food support networks, strengthening their own health care systems, or forms of mutual support, such as epu imple kelluwun (mutual collaboration in the Mapuche language).
In sum, our analysis illustrates that the municipalities with a higher percentage of Indigenous peoples present a higher rate of infection and mortality to COVID-19. These findings are consistent with previous studies demonstrating that Indigenous Peoples are more vulnerable to infection and deaths of COVID-19. One of the main limitations of this study is the unit of analysis. The Chilean government data is aggregated at the municipality level, which may obscure relevant information for estimating the impact of COVID-19 on Indigenous populations. However, aggregated data are widely used in social sciences and researchers are proof that the results obtained between individual and aggregated data may be almost identical (Bloom et al., 2007; Jacob et al., 2014). Future studies should consider these limitations, as well as how Indigenous communities have responded to COVID-19, and how these responses are part of the exercising autonomy and self-determination in a context of crisis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of the FONDECYT Project No. 11170193.