
Abstract
Background:
Safe water and sanitation are basic human needs and human rights. Lack of access to safe water and sanitation has been a major problem for the health and well-being of the people. In developing countries like Ethiopia, the proportion of people with access to improved sanitation is low. Information on household access to improved sanitation in some rural districts of Ethiopia is scarce.
Objective:
To assess access to basic sanitation services and associated factors in South Achefer district, Northwest Ethiopia 2023.
Methodology:
This study was conducted among the population of the South Achefer District, Northwest Ethiopia, using a cross-sectional study design. The study was conducted among 691 households selected using multistage and systematic random sampling. The data were entered into EpiData version 3.1 and analyzed using SPSS version 23. Binary logistic regression analysis was conducted to identify the factors associated with access to basic sanitation services. Statistical significance was declared at a 95% confidence interval and a P-value <.05.
Result:
Only 19 households (2.7%; 95%CI: 1.6-4.1) were accessing basic sanitation services. The significant factors associated with access to basic sanitation services were smaller family size (AOR = 3.06; 95%CI: 1.04-8.98), merchant occupation (AOR = 3.18; 95%CI: 1.19-8.50), better knowledge about sanitation services (AOR = 3.07; 95%CI: 1.17-8.09), and positive attitude about sanitation services (AOR = 3.83; 95%CI: 1.46-10.00).
Conclusion:
The access rate to basic sanitation services in South Achefer District is extremely low compared to national and international standards. Family size, occupation, knowledge, and attitude about sanitation services were significant predictors of access to basic sanitation services.
Introduction
Basic sanitation services are the availability and use of improved sanitation facilities that hygienically separate human excreta from human contact. Improved sanitation facilities include flush toilets, pour-flush toilets, sewer systems, septic tanks, pit latrines with slabs, pit latrines, ventilated improved pit latrines, and composting toilets. 1
Inadequate access to basic sanitation services is a critical health concern in the world today. Inadequate access to basic sanitation services allows for the fecal-oral transmission of infectious diseases like diarrhea, cholera, and intestinal infections. These diseases are common among children aged 5 years and below, with serious health implications, including stunted growth, cognitive development, and productivity in the future. 2 Inadequate access to basic sanitation services was also cited as a contributing factor to environmental degradation, healthcare costs, and health inequalities in low- and middle-income countries. 3
Globally, the access level to safely managed services in terms of sanitation is still far from the international goals set. According to recent estimates, there are still more than 1.4 billion people living in the rural areas without access to basic sanitation services, showing that the efforts made so far are still inadequate in achieving the Sustainable Development Goal (SDG) target 6.2, which focuses on ensuring access to adequate and equitable sanitation and hygiene in all by the year 2030. 3 The situation in the sub-Saharan region is alarming, with more than 779 million people living in the region without access to basic sanitation services. 4 The population growth rate, poverty, lack of adequate infrastructure, and poor sanitation services are the factors hindering the improvement of the situation in the region. 5
In Ethiopia, the access rate to improved sanitation services is very low, especially in the rural areas. According to the national reports, the access rate to basic sanitation services in the country is only about 7%, while in the rural areas, the access rate is as low as 4%.5,6 The poor access to improved sanitation services is one of the factors contributing to the burden of communicable diseases, especially diarrhea and parasitic diseases, in the country. In addition, several studies carried out in different parts of Ethiopia have indicated that the access rate to improved sanitation services is low, with several factors, including socioeconomic factors, education level, family size, knowledge, and attitudes, playing a role in the low access rate.7,8
To mitigate these challenges, the Ethiopian Federal Ministry of Health has included the improvement of sanitation in the Health Sector Transformation Plan. The aim is to increase the proportion of people using basic sanitation facilities from 20% in 2019 to 60% in 2025 through market-oriented and community-centered approaches.9,10 One of the approaches adopted to improve sanitation is the implementation of Community-Led Total Sanitation and Hygiene (CLTSH), which seeks to change behavior and encourage communities to stop practicing open defecation. 11 However, studies have shown that most latrines developed through this program are not improved sanitation facilities and are prone to failure shortly after completion. 12 Recent studies have also indicated that latrine ownership is not the only factor to be considered in sanitation improvements but also the socioeconomic, behavioral, and environmental determinants that affect sanitation access. 13
Despite the ongoing national and international initiatives aimed at increasing the coverage of sanitation services in the country, there is still limited access to basic sanitation services in most rural areas in Ethiopia. Moreover, there is limited information about the level of access to basic sanitation services and the factors that affect this level in specific rural districts in Ethiopia, such as the South Achefer District in Northwest Ethiopia.
Thus, this study aimed to assess the level of access to basic sanitation services and the factors that affect this level among rural households in the South Achefer District in Northwest Ethiopia. The findings of this study will be useful in providing evidence for local and regional health authorities in planning effective sanitation programs in the region and in monitoring the progress toward the achievement of SDG target 6.2 in the national context.
Methods
Study Design and Setting
A community based cross-sectional study was conducted from March 01 to 30/2023. The study was conducted in the rural communities of South Achefer District, West Gojjam Zone, Amhara Region, northwest Ethiopia, in 2023. The district, located about 113 km northwest of Bahir Dar and 552 km from Addis Ababa.
South Achefer District is 1 of the 20 districts of the West Gojjam Zone. The total geographical area of the district is 118 288 ha. The topography of the district is flat, with 72% of the total geographical area, whereas 12% of the land is undulating, 10% mountainous, and 6% valley. The altitude of the district varies from 1500 to 2300 m above sea level. In terms of climatic zones, the district can be classified as Woina Dega, covering 87% of the total geographical area, whereas the remaining 13% of the land is classified as Kola. 14
In terms of administrative structure, the total administrative units of the district include 22 rural kebeles, 4 urban kebeles, 1 primary hospital, 8 health centers, 22 health posts, and an estimated total population of 172 812. In the district, approximately 27% of the total population practices open defecation. 15
Population
Source Population
All rural households of the South Achefer District were the source population of the study.
Study Population
All households of the 6 selected rural kebeles of south Achefer district were the study population.
Study Unit
All selected households’ heads from whom data was actually collected were the study unit.
Inclusion and Exclusion Criteria
Inclusion Criteria
All selected house hold heads that permanently live above 6 months in the Kebele and had sanitation services were included in the study.
Exclusion Criteria
The households were excluded if the head or eligible adult was unable to provide reliable information because of serious illness, or if no eligible adult was available after at least 2 visits.
Variables
Dependent Variables
Access to basic sanitation services (Yes/No).
Independent Variables
Operational Definition
● Good Knowledge > overall mean
● Poor knowledge < overall mean
● Positive attitude > mean
● Negative attitude < mean
Sample Size Determination
Sample size was calculated for both objectives and the larger sample size was selected for the study and it was calculated as follows.
The sample size was determined by using a single population proportion formula considering the following assumptions of proportion of access to basic sanitation service of 16%, 17 95%CI, level of significance to be 5%.
Where: n = sample size
Z = standard value for 95%CI, z = 1.96
p = proportion of household’s access to basic sanitation = 16%
D = marginal error = 0.05 (5%)



There for: n = (1.96)2 × (0.16) × (0.84)/(0.05)2 n = 207
For design effect it was multiplied by 2; Then the sample size became 414.
For non-response rate 10% of sample size was added which was equals to 414 × 10/100 = 41
Finally, the total sample size of the study was n plus non-response rate
N = n + non-response rate
N = 414 + 41 = 455
Total sample size for objective 1 of the study was = 455
●
Sample Size for the second objective:
The study used epi info7 statcalc for cohort and cross sectional study software to calculate sample size for all significant variables in the reference study conducted Gurage Zone, SouthernEthiopia 18 and sample size was calculated for Educational status, family size, presence of school children and from those variables using the literature the study uses 95%CI, power (80%),ratio, 1 % of outcome in unexposed group (77% ), Odds ratio (2.53) finally Statcalc provides 314 “sample size which was the largest sample size from all calculated values are presented in Table 1. ”
Table Showing Statcalc Sample Size Calculated Values Summary Result.

Thus, sample size of second objective was stat calc result × 2 for design effect = 314 × 2 = 628
For non-response rate the study added 10% which was equal to 628 + (628 × 10/100) = 691
Finally, when comparing sample size of the first and second objective the second was larger than the first which was selected as the sample size of the study.
Total sample size for objective 2 of the study was 691.
Finally, the sample size for the study was the larger from the 2 which was 691.
Sampling Method
There were 20 rural kebeles in the district and from the total, rural kebeles, as a rule of thumb, 30% 19 or 6 kebeles were selected using a stratified multistage sampling technique to ensure the geographic and demographic diversity of the district. The total sample size of 691 households was proportionally distributed over the selected kebeles based on the size of the population.
For each selected kebele, households were selected using a systematic random sampling technique. The sampling interval, denoted by K, was calculated by dividing the total number of households in the selected kebeles by the total sample size. The value of K was 13. The first household was randomly selected, and every 13th household was selected until the desired sample size was achieved.
Figure 1. Schematic presentation of the sampling procedure for selecting study units from the study population in rural kebeles of South Achefer District, Ethiopia, 2023.
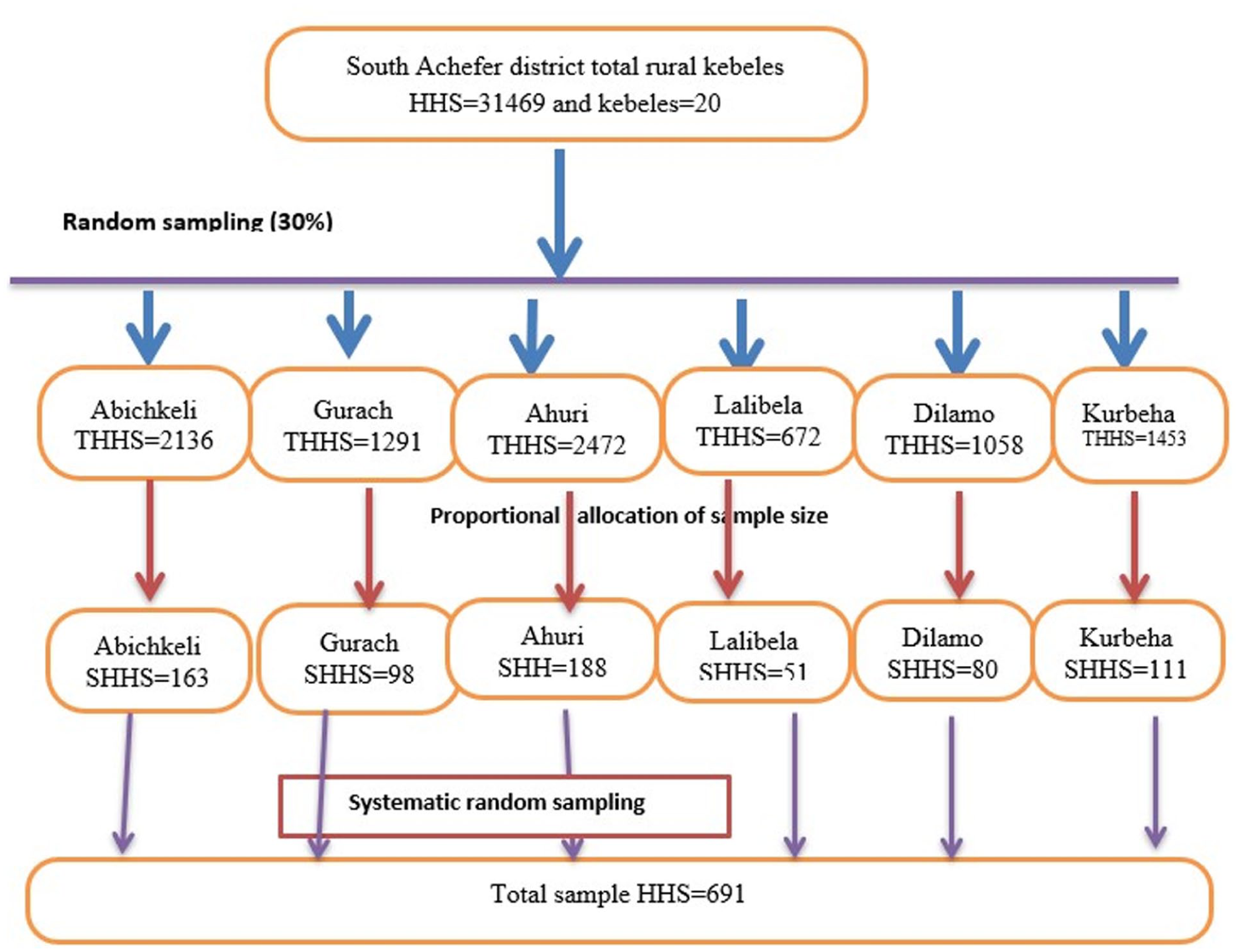
Schematic presentation of sampling procedure for selecting study units from the study population in rural kebeles of South Achefer district, 2023.
Data Collection Method and Procedures
The data were collected using a structured questioner and observational checklist adapted from WHO/UNICEF joint monitoring program for WASH management and monitoring assessment
Data Quality Control
The questionnaire was first developed in English, then translated into Amharic, and finally back-translated into English by language experts. To avoid any bias, a standard questionnaire was used. In addition, the data collectors were chosen from the list of health professionals working in the area. A training was given to the data collectors and supervisors for a day on the objectives of the study, the method of data collection, and the contents of the questionnaire. Pre-testing of the tool was conducted on 5% of the total sample households in a non-selected kebele a week prior to the actual data collection period. Modifications were made accordingly. During the data collection, the supervisors and the principal investigators monitored the activities daily.
Data Processing and Analysis
The data was checked for completeness and consistency, and it was cleaned, coded and entered into Epi data version 3.1 and was exported into SPSS for Windows version 23 for analysis. Descriptive statistics were computed to describe the frequency, percentage, mean and standard deviation of the variables. Binary logistic regressions were done to predict the association between independent and dependent variables. Bivariate analysis was done to identify candidate variables with P-value <.25. Multivariate analysis was done to identify significant associated factors between dependent variables and independent variables. In the final model, the confidence interval (95%) and a P-value <.05 were considered as statistically significant.
Result
Socio Demographic and Economic Characteristics
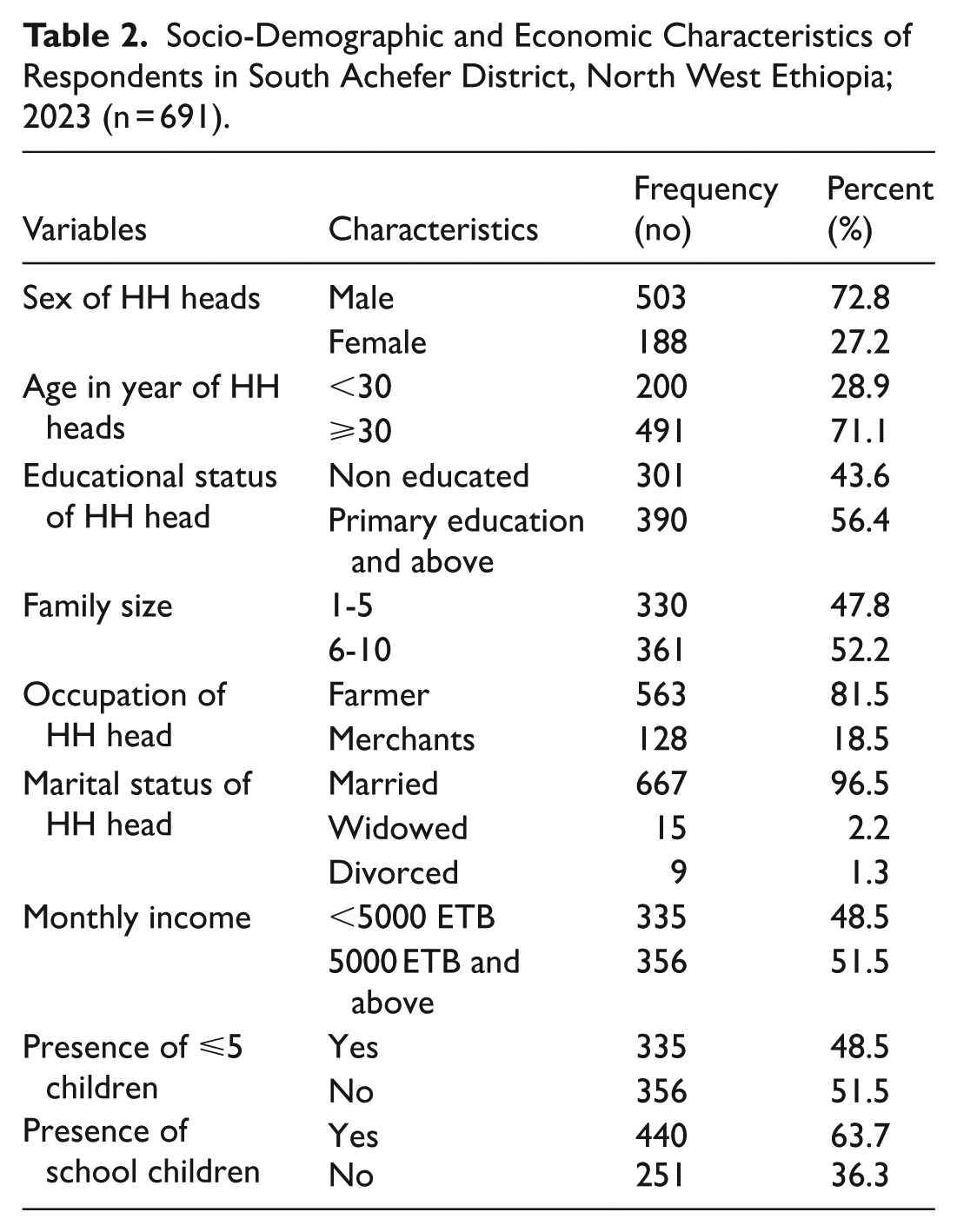
A total of 691 study participants took part in the study with a 100% response rate. Most of the participants were male-headed households, accounting for 503 (72.8%), while the majority of the participants were farmers, 563 (81.5%). Regarding the participants’ marital status, the majority of the participants were married, 667 (96.5%). The findings indicate that the study participants were mostly male-headed, married, and involved in farming activities.
Socio-Demographic and Economic Characteristics of Respondents in South Achefer District, North West Ethiopia; 2023 (n = 691).
Environmental Related Factors
The location of latrines can greatly impact their use and effectiveness. Ideally, latrines should be located away from water sources, to avoid contamination of these sources. In a study area, all latrines are located in their own yard/plot (100%).
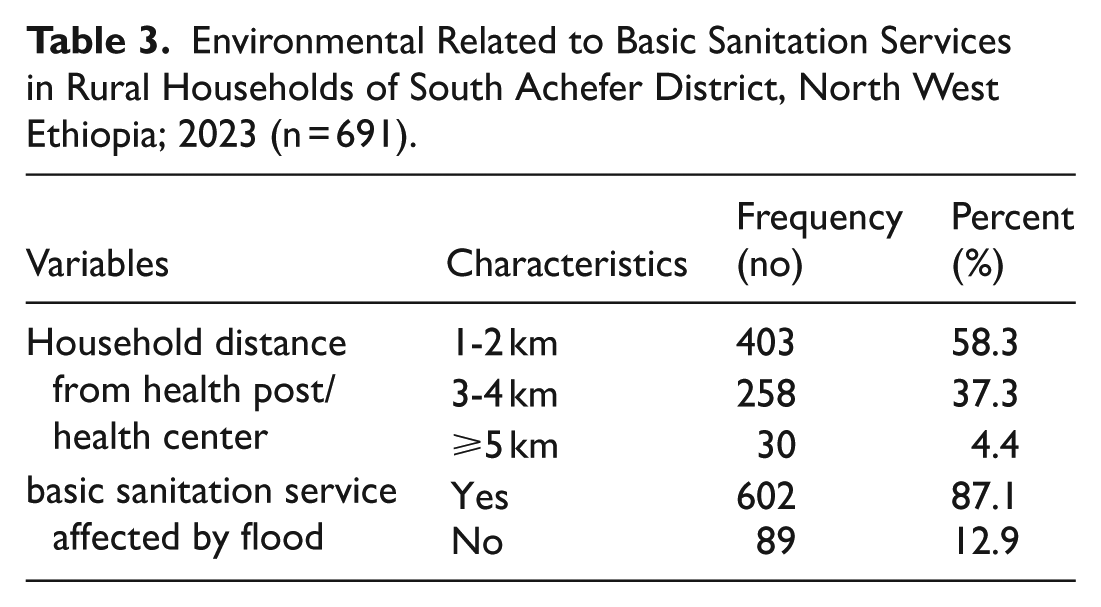
In a study area, the attitude of respondents indicates flood affects basic sanitation services was 87.1% of households. Floods can damage sanitation infrastructure and increase the risk of disease transmission through contaminated water sources. In areas where flooding is common, it is important to design sanitation facilities that are resistant to flood damage and place them in high ground locations that are less likely to be affected by flooding.
In the study area, the distance from the household to the health facility far from 1 to 2 km 58.3%, 3 to 4 km 37.3% and 5 km and above 4.4%. The distance between sanitation services and health care centers can impact the spread of diseases that are related to poor sanitation. When facilities are located far from health posts, it may be difficult for people to access basic sanitation services.
Environmental Related to Basic Sanitation Services in Rural Households of South Achefer District, North West Ethiopia; 2023 (n = 691).
Knowledge Related to Basic Sanitation Services
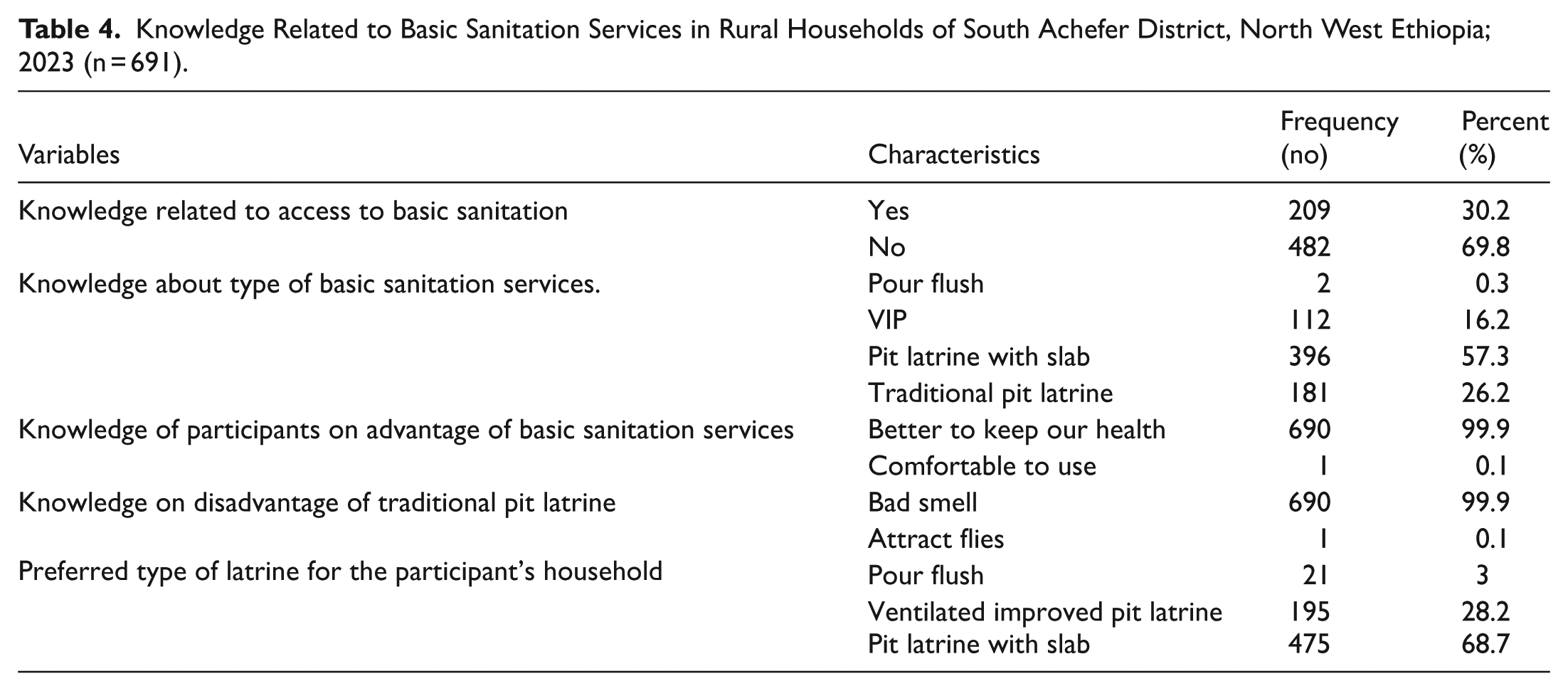
The study findings show that 209 (30.2%) of the respondents have knowledge regarding the issue of access to basic sanitation facilities, whereas 482 (69.8%) of the respondents have no knowledge. In terms of types of sanitation facilities, the most known facility was pit latrine with slab, known by 396 (57.3%) of the respondents, whereas traditional pit latrine was known by 181 (26.2%), VIP latrine by 112 (16.2%), and pour flush by 2 (0.3%).
In terms of the advantages of basic sanitation facilities, nearly all respondents, 690 (99.9%), identified the improvement of health as the major advantage of basic sanitation facilities, whereas only 1 (0.1%) identified the comfort of the facilities. Similarly, nearly all respondents, 690 (99.9%), identified the bad smell of the traditional facilities as the major disadvantage of traditional pit latrines, whereas only 1 (0.1%) identified the fly attraction of traditional facilities.
In terms of preference, most participants preferred pit latrine with slab 475 (68.7%), followed by VIP latrine 195 (28.2%), while few preferred pour flush latrine 21 (3.0%).
Knowledge Related to Basic Sanitation Services in Rural Households of South Achefer District, North West Ethiopia; 2023 (n = 691).
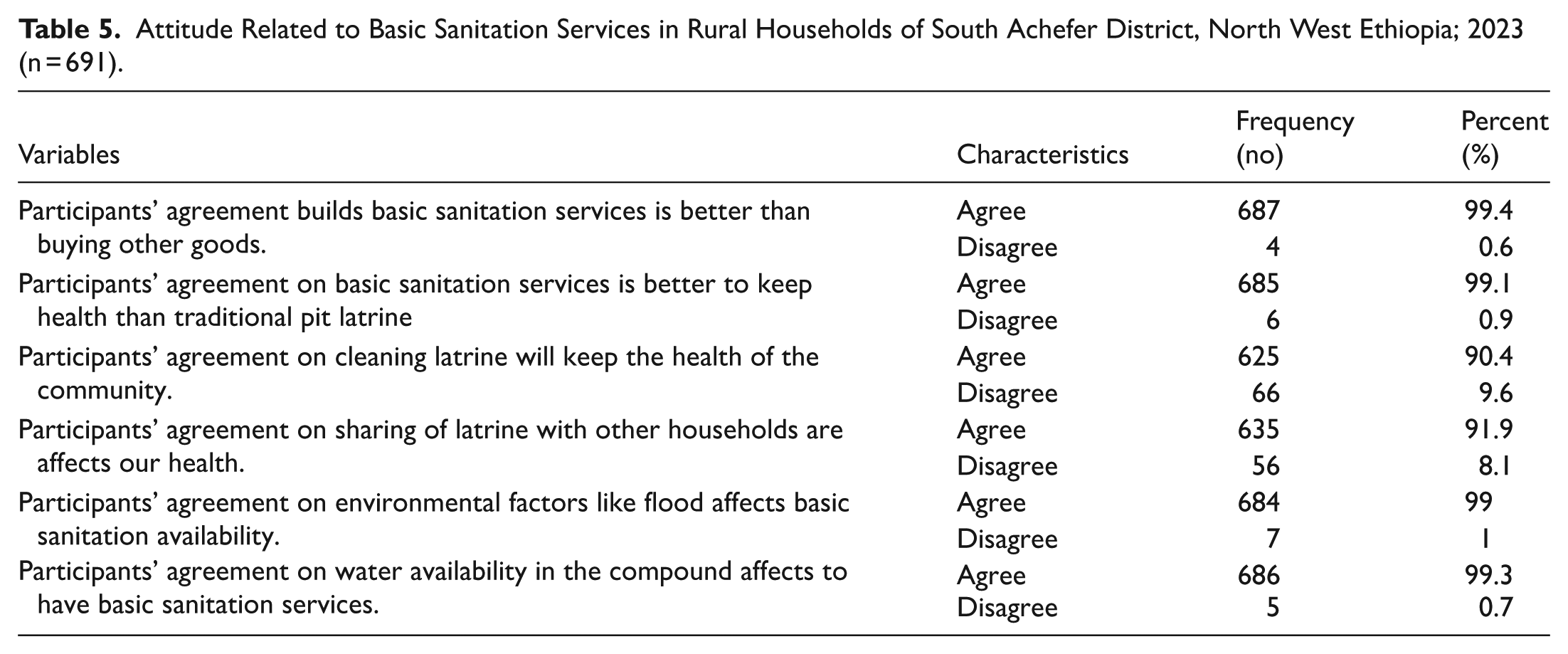
Attitude Toward Basic Sanitation Services
The findings reveal that the majority, 687 (99.4%), agreed that investing in basic sanitation services is better than investing in other goods, and 685 (99.1%) agreed that basic sanitation services are better for health than traditional pit latrines. Moreover, 625 (90.4%) agreed that cleaning latrines improves health within the community, and 635 (91.9%) agreed that sharing the latrine with other households negatively impacts health. In addition, the majority, 684 (99.0%), agreed that environmental factors, such as flooding, impact the availability of sanitation services, and 686 (99.3%) agreed that the availability of water within the compound impacts the availability of basic sanitation services.
Attitude Related to Basic Sanitation Services in Rural Households of South Achefer District, North West Ethiopia; 2023 (n = 691).
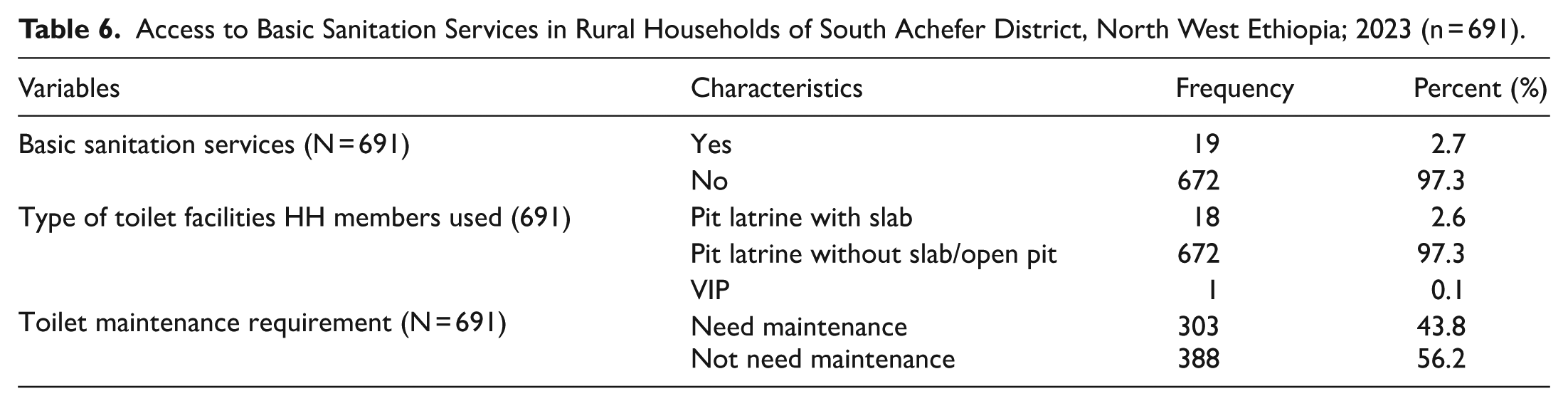
Access to Basic Sanitation Services
The findings reveal that only 19 (2.7%) households had access to basic sanitation services, while the majority, 672 (97.3%), did not. In terms of the type of toilet facilities used, the majority, 672 (97.3%), used pit latrines without slab/open pits, while 18 (2.6%) used pit latrines with slab, and only 1 (0.1%) used VIP latrines. In addition, 303 (43.8%) of the households reported that their toilets needed maintenance, while 388 (56.2%) reported that there was no need for maintenance.
Access to Basic Sanitation Services in Rural Households of South Achefer District, North West Ethiopia; 2023 (n = 691).
Factors Associated With Basic Sanitation Services
During the bivariate analysis, age, family size, occupation, <5 children, knowledge and attitude of the households were variable that have significant associated with the basic sanitation services at a significant level of P < .25.
Results of the multiple binary logistic regression analysis showed family size, occupation of household head, knowledge of household head on basic sanitation services and attitude of household heads toward basic sanitation services were significantly associated with access to basic sanitation services with P-values <.05.
Therefore, the odds of households with a family size of 1 to 5 were 3 times higher to have basic sanitation services than the odd of households with a family size 6 to 10 (AOR: 3.06, 95%CI = 1.04, 8.98). The odd of households who had merchants was 3.2 times higher for having basic sanitation services than the odds of the household who had farmers (AOR = 3.18, 95%CI = 1.19, 8.5). similarly, the odds of the households who had good knowledge was 3 times higher to have basic sanitation services than the odds of the households who had poor knowledge (AOR = 3.07 95%CI = 1.17, 8.09) Similarly the odd of the households who had positive attitude 3.8 times higher to have basic sanitation services than the odd of the households who negative attitude (AOR = 3.83, 95%CI = 1.46, 10).
Factors Associated with Basic Sanitation Services in Rural Households of South Achefer District, North West Ethiopia; 2023 (n = 691).
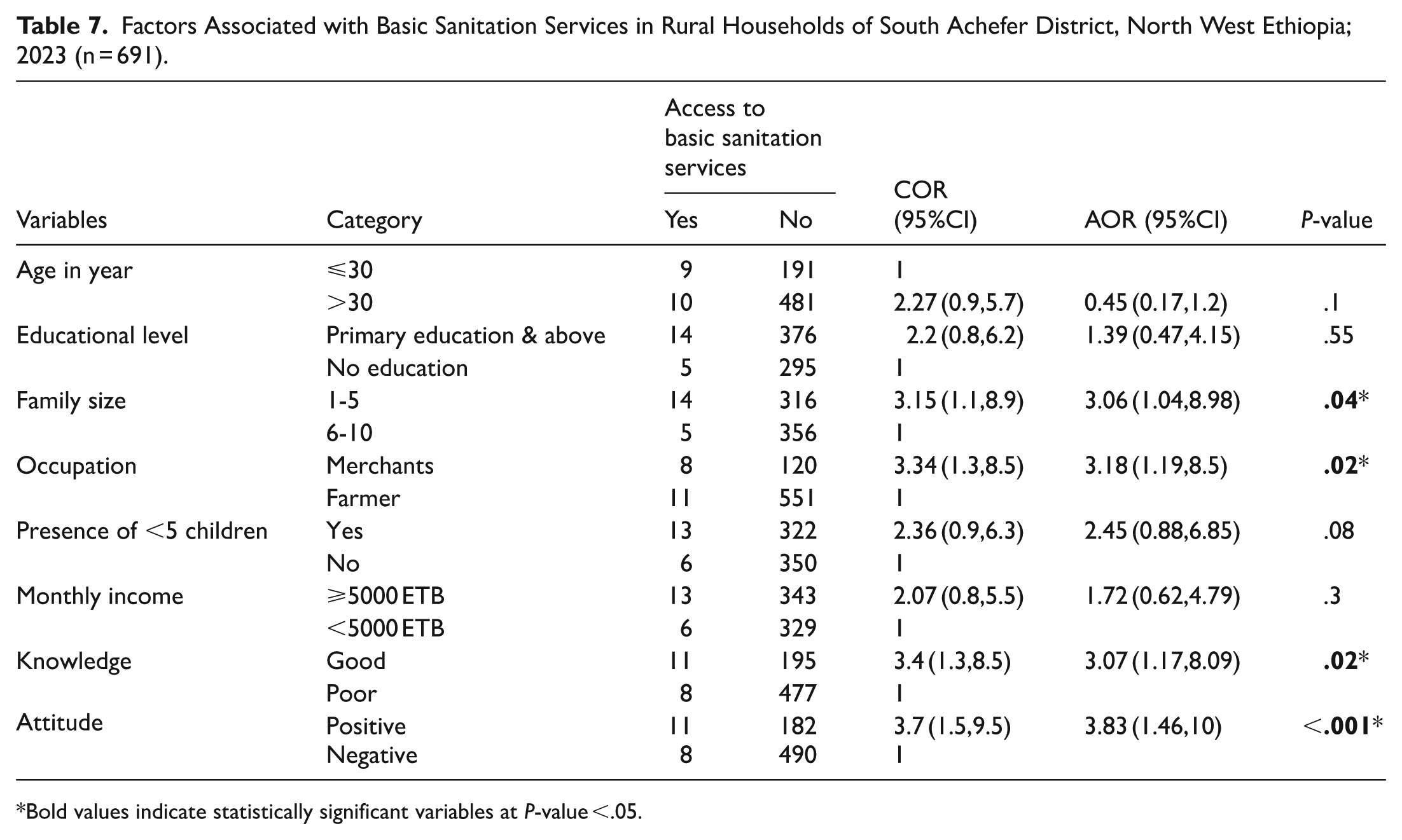
Bold values indicate statistically significant variables at P-value <.05.
Discussion
This study assessed the level of access to basic sanitation services and its determinants among households in South Achefer District. The results show that only 19 households (2.7%, 95%CI: 1.6-4.1) had access to basic sanitation services. The quantitative approach was used in this study. The findings show that access to basic sanitation services is extremely low. The results of this study indicate that access to basic sanitation services is far below national and international standards.
This level of access to basic sanitation services is lower than the WHO/UNICEF JMP 2021 estimates of access to basic sanitation services in rural Ethiopia. 22 The level of access to basic sanitation services is also lower than that of other rural sub-Saharan African countries such as Chad (3.6%), Eritrea (5.6%), Central African Republic (5.9%), South Sudan (9.3%), Liberia (6.4%), Niger (7.4%), Congo Republic (6.3%), and Ethiopia (5.5%). 23 The level of access to basic sanitation services is also lower than the average access to basic sanitation services in other sub-Saharan African countries (6%) and least developed countries (4%). 24 The difference may be attributed to differences in socio-economic and socio-demographic factors such as education levels, occupation types, income levels, and awareness levels.
Moreover, the findings of this study further revealed that family size, occupation of household heads, knowledge level, and attitude were significantly associated with access to basic sanitation services. It was revealed that households with fewer than 5 family members were more likely to have access to basic sanitation facilities. This finding is supported by studies conducted in Jimma town and Amhara Region.25,26 It might be due to the fact that households with fewer members are likely to plan better for household resources. In addition to this, similar findings were revealed in Enderta District in Tigray Region, in which family size was significantly associated with access to basic sanitation services. 27
Moreover, the occupation of household heads was significantly associated with access to basic sanitation services. Merchant households were 3.34 times more likely to have access to basic sanitation services than households of farming heads. This finding is supported by studies conducted in Wolaita Sodo town and Southern Ethiopia.28,29 It might be due to the fact that households of merchant heads are likely to have more diversified and stable sources of income to construct improved sanitation facilities. In contrast, households of farming heads might depend on seasonal agricultural income.
In addition, knowledge level was a strong predictor of access. Households with a good knowledge were 3.07 times more likely to have access to basic sanitation facilities compared to those with poor knowledge. These findings were consistent with studies conducted in rural Bangladesh and Northwest Ethiopia.30,31 Improved knowledge may lead to awareness of sanitation-related diseases such as diarrhea and parasitic infections, thus encouraging improved sanitation practices.
Attitude toward sanitation facilities was also a significant predictor of access. Households with good attitude toward sanitation facilities were 3.83 times more likely to have access to improved sanitation facilities compared to those with a poor attitude. These findings were consistent with studies conducted in rural Ethiopia, Arsi Negele town, and southeastern Ethiopia.32,33 Good attitudes may be associated with the benefits of improved sanitation facilities, whereas poor attitudes may discourage households from investing in sanitation facilities.
From the comparative analysis point of view, although different approaches were employed in the analysis (descriptive and inferential analysis), the regression analysis was more useful in identifying the key determinants of access to sanitation. The descriptive analysis provided information on the general extremely low level of access to sanitation.
The implications of this study for public health practice and policy are immense. The extremely low level of access to sanitation implies that existing interventions have been inadequate to achieve the targets set in the Sustainable Development Goal (SDG) 6 to attain universal access to sanitation services by 2030. 34 The existing interventions need to focus on enhancing income opportunities for households, improving health education, and enhancing behavioral change communication approaches. In addition, farming households and large families need to be targeted because they have lower access to improved sanitation. The significance of this study lies in its contribution to identifying context-specific determinants of sanitation access in rural Ethiopia. The findings provide evidence-based insights for policymakers, district health offices, and development partners to design more targeted and effective sanitation programs. Moreover, the study highlights key successes in quantifying sanitation coverage and identifying major behavioral and socio-economic barriers, which can guide future interventions aimed at improving rural public health outcomes.
Overall, the study demonstrates that access to basic sanitation services in South Achefer District is critically low and shaped by multiple interrelated factors. Addressing these determinants through integrated public health and socio-economic interventions is essential to improve sanitation coverage and reduce the burden of sanitation-related diseases.
Limitation of the Study
A major limitation of the present study was that the cross-sectional design of the study restricts the capacity to identify cause-and-effect relationships. Moreover, the self-reporting method used in the current study has the potential for recall bias and social desirability bias, which might impact the results of the study. Further, the lack of qualitative studies has restricted the comprehensive comprehension of the context and behavioral determinants.
Conclusion and Recommendation
This study is significant in demonstrating that access to basic sanitation facilities is still limited in rural Ethiopia, despite recent efforts. This study contributes to the body of knowledge in the area of sanitation access in Ethiopia. This study is significant in that it identified basic household determinants that affect access to sanitation. These determinants included family size, occupation, knowledge, and attitudes.
The findings of this study have significant public health implications, especially in the prevention of diseases and the achievement of the country and global sanitation targets. In this regard, health education in the community is essential in bringing about positive behavioral changes. Furthermore, the role of community leaders, including religious leaders, is crucial in bringing about positive changes in the community. In addition, support for vulnerable groups and monitoring and evaluation at the regional and zonal levels are essential in bringing about the achievement of the goals set in the sustainable development goals. Qualitative and intervention studies should be conducted in the future.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support of the Amhara Public Health Institution. We also thank the data collectors and study participants for their invaluable contributions to this study.
Abbreviations and Acronyms
HH: household, JMP: joint monitoring program, MDG: millennium development goals, MOH: ministry of health, SDG: sustainable development goal, SHH: sample households, THHS: total households, UN: united nations, UNICEF: united nations international children’s emergency fund, VIP: ventilated improve pit, WASH: water, sanitation and hygiene, WHO: world health organization.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board of the College of Medicine and Health Sciences at Bahir Dar University. Support letters were also obtained from the Amhara Public Health Institute and the South Achefer Health Office. Participant confidentiality was maintained by assigning study identification codes to each household. All collected data were securely stored in locked cabinets and password-protected computers. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Consent to Participate
Oral informed consent was obtained from all study participants before the commencement of data collection.
Authors’ Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request*.