
Abstract
Background
Despite the recognised importance of communication in healthcare delivery, limited research has examined how communication interacts with other service quality (SERVQUAL) dimensions to shape patient satisfaction in Ghanaian hospital settings. This study aimed to assess communication and SERVQUAL dimensions as determinants of satisfaction among patients accessing outpatient services at a university hospital in Ghana.
Methods
This cross-sectional study collected data from 366 patients who accessed outpatient services from November 1, 2025, to December 20, 2025. A structured questionnaire incorporating socio-demographic characteristics, communication, SERVQUAL model, and satisfaction was used to collect study data. Structural equation modelling was used to examine the relationship between the SERVQUAL dimensions, communication, and satisfaction. A mediation analysis was conducted to test whether communication mediated the relationship between the SERVQUAL dimensions and satisfaction.
Results
The median satisfaction and communication scores were 75.0 [58.3–91.7] and 75.0 [50.0–90.0], respectively. Among the SERVQUAL domains, tangibility (median: 75.0 [62.5–87.5]) was the highest-rated, whereas reliability (median: 68.8 [50.0–81.2]) was the lowest-rated. Communication (β = 0.400, p = 0.002) and empathy (β = 0.434, p = 0.043) were identified as determinants of patient satisfaction. Communication did not significantly mediate the association between the SERVQUAL dimensions and patient satisfaction.
Conclusion
This study highlights the critical role of communication and empathy in shaping patient satisfaction in outpatient services at the university hospital. Prioritising patient-centred communication and compassionate care should therefore be an integral part of healthcare quality improvement strategies aimed at strengthening health systems and advancing progress towards universal health coverage.
Introduction
Patient satisfaction is widely recognised as an important indicator of healthcare quality and a key measure of how well health systems respond to patients’ needs.1,2 When patients feel satisfied with the care they receive, they are more likely to trust healthcare providers, follow treatment instructions, and return to the same facility when they need care.3,4 In contrast, dissatisfaction with healthcare services can reduce healthcare utilisation and negatively affect health outcomes. 5 For this reason, patient satisfaction has become a central component of healthcare quality improvement initiatives worldwide. In recent years, health systems, particularly in low- and middle-income countries (LMICs), have increasingly emphasised patient-centred care as a strategy to improve service delivery and strengthen trust between healthcare providers and patients.6,7 Understanding the factors that influence patient satisfaction is therefore essential for improving the effectiveness and responsiveness of healthcare services.
In many LMICs, including Ghana, health systems continue to face challenges such as high patient loads, limited resources, and shortages of healthcare personnel.8-10 These constraints can affect the quality of services provided and influence patients’ experiences during healthcare encounters. Although Ghana has made significant progress in expanding access to healthcare through initiatives such as the National Health Insurance Scheme, ensuring the quality of care remains a priority for policymakers and healthcare managers. 11 Studies conducted in Ghana and other African countries have shown that patients’ perceptions of healthcare quality depend not only on the availability of services but also on how care is delivered, with factors such as healthcare workers’ behaviour, waiting times, communication, and the physical environment all contributing to overall patient satisfaction.12-17
One widely used framework for assessing service quality in healthcare is the service quality (SERVQUAL) model. 18 This model evaluates service quality across five key dimensions: tangibility, reliability, responsiveness, assurance, and empathy. Tangibility refers to the physical environment and equipment available in healthcare facilities; reliability relates to the ability of healthcare providers to deliver services accurately and consistently; responsiveness concerns the willingness of staff to provide prompt assistance; assurance reflects the competence and professionalism of healthcare providers; and empathy relates to the extent to which healthcare workers provide caring and individualised attention to patients. 18 Previous studies conducted in Ghana have demonstrated that these dimensions play an important role in shaping patients’ perceptions of healthcare quality and satisfaction.19-21 However, the relative influence of these dimensions may vary depending on the healthcare setting and the nature of interactions between patients and healthcare providers.
Among the different factors that shape patient satisfaction, communication between healthcare providers and patients has been identified as particularly important.22,23 Effective communication helps patients understand their health conditions, treatment options, and care procedures, while also allowing healthcare providers to better understand patients’ concerns and expectations. When communication is clear, respectful, and empathetic, patients are more likely to feel valued and involved in decisions regarding their care. Poor communication, on the other hand, can lead to confusion, anxiety, and dissatisfaction with healthcare services.22,24 Despite the recognised importance of communication in healthcare delivery, limited research has examined how communication interacts with other SERVQUAL dimensions to influence patient satisfaction in Ghanaian hospital settings.
Improving patient satisfaction through effective patient-centred communication and high-quality service delivery is an important step towards achieving universal health coverage (UHC). Aside from access to healthcare services, UHC also highlight the significance of providing high-quality, equitable and patient-centred care that meets the expectations and needs of users. 25 Given this, the SERVQUAL dimensions and effective patient-centred communication between healthcare professionals and service users are essential for improving healthcare quality. Improving these aspects of care is relevant to achieving UHC by enhancing patient experiences and building trust in the health system. 26
Therefore, this study aimed to assess communication and SERVQUAL dimensions as determinants of satisfaction among patients accessing outpatient services at the University Hospital of Kwame Nkrumah University of Science and Technology (KNUST) in Kumasi, Ghana, using a structural equation modelling approach. This study generates evidence on experiential quality and patient satisfaction as key quality dimensions within Ghana’s progress towards UHC.
Methods
Study Design and Setting
This study employed a cross-sectional design to examine the influence of communication and SERVQUAL dimensions on patient satisfaction in the outpatient departments of the University Hospital, KNUST, Kumasi, Ghana, from November 1, 2025, to December 20, 2025. The University Hospital is a 135-bed capacity district-level healthcare facility that provides primary healthcare services to the university staff and their dependents, students, and private patients. 27 The hospital has four outpatient service points, including the main outpatient department, the Students’ Clinic, and the two Staff Clinics. The hospital operates a 24-hour service and employs over 400 multidisciplinary healthcare professionals, including physicians, nurses, pharmacists, laboratory scientists, and allied health personnel. On average, the hospital records approximately 350 outpatient visits every day.
Study Population and Eligibility Criteria
The study population comprised adults attending all outpatient departments for medical care. All patients who accessed outpatient services during the study period and provided informed consent were eligible, regardless of the number of prior hospital visits. Patients had to agree and either sign or thumbprint an informed consent form before being recruited into the study. Patients who were critically ill and required admission were excluded from the study.
Sample Size Estimation and Sampling Technique
The sample size was estimated using the Cochran formula (
A consecutive sampling technique was employed to select study participants. Each day, all patients who attended the outpatient departments were approached by the research team and assessed for eligibility. The purpose of the study was explained to the eligible patients, and those who agreed to participate provided written informed consent before recruitment. This process was repeated every day until the required sample size was achieved. The consecutive sampling technique was considered feasible for this study because outpatient visits vary throughout the day and allowed the recruitment of participants immediately after they had accessed care, thereby providing timely feedback on the quality of services received. Participants were recruited at the pharmacy units of all outpatient service points. The Pharmacy Unit was selected because it represents the final service point in the care process, ensuring that patients have completed all service encounters before providing feedback.
Data Collection Tool and Techniques
Data were collected using an interviewer-administered structured questionnaire (see Supplemental File 1). The questionnaire consisted of four sections. The first section included eight demographic variables: age, gender, marital status, educational level, employment status, type of patient, having National Health Insurance Scheme, and type of visit. The second part assessed service quality using 13 items adapted from the SERVQUAL model. 18 The SERVQUAL model is an internationally validated tool that has been widely utilised to measure service quality in healthcare settings worldwide.12,18,30,31 The items assessed the five dimensions of SERVQUAL: tangibility (2 items), empathy (2 items), responsiveness (2 items), reliability (4 items), and assurance (3 items). The items were adapted to reflect the outpatient context in Ghana while retaining their original conceptual meanings, and responses were recorded on a 5-point Likert scale. The third section assessed patient-provider communication using 5 items adapted from the Communication Assessment Tool, 32 while the final section measured overall satisfaction using 3 items. All the items were rated on a 5-point Likert Scale ranging from 1 (strongly disagree) to 5 (strongly agree), with 3 representing a neutral response. A higher total score per construct indicated higher perceived quality, better communication, or higher patient satisfaction. The Communication Assessment Tool is a validated scale used to examine patient-provider communication in healthcare settings. 32
The questionnaire was administered by four research assistants who underwent three days of training on the informed consent procedure, the administration of the data collection instrument, and the translation of the questionnaire into the local Twi language. The training was done to enhance the consistency in the data collected. All interviews were conducted in English or Twi (a commonly spoken local language), where appropriate. Prior to use, the questionnaire was pretested among 20 participants who accessed outpatient services at a different facility, and all necessary corrections were made.
Statistical Analysis
Data analysis was conducted using R Programming Language version 4.4.2 (R Core Team, 2024). Participants’ characteristics were described using medians and interquartile ranges for continuous, non-normally distributed data, and as frequencies and percentages for categorical data. The overall scores for all the SERVQUAL dimensions, communication, and satisfaction were computed and scaled to a percentage of the maximum possible score (0-100%). These domains were summarised and presented using medians and interquartile ranges. The internal consistency and reliability of each item were assessed using Cronbach’s alpha.
Structural equation modelling (SEM) was used to examine the relationship between the SERVQUAL dimensions, communication, and satisfaction, with satisfaction treated as the outcome. Separate latent variables were specified for each SERVQUAL dimension, communication, and satisfaction based on their respective item sets, and path coefficients were estimated to quantify the associations between these constructs. The raw scores were used for all the constructs for the Structural equation modelling. Model fit was evaluated using Chi-square (Chisq), degrees of freedom (DF), comparative fit index (CFI), Tucker-Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA), and Standardised Root Mean Square Residual (SRMR).
A mediation analysis was conducted to test whether communication mediated the relationship between the SERVQUAL dimensions and satisfaction. In this model, SERVQUAL dimensions were specified as independent variables, communication as the mediator, and satisfaction as the dependent variable. The model tested the direct, indirect, and total effects of communication on the relationship between the SERVQUAL dimensions and satisfaction, and indirect effects were evaluated using non-parametric bootstrapping with 5,000 resamples to obtain bias-corrected 95% confidence intervals.
Ethics Approval
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval to conduct the study was obtained from the Committee on Human Research, Publications and Ethics, School of Medical Sciences, KNUST, Kumasi, Ghana (reference number: CHRPE/AP/1131/25) on 31st October 2025. Administrative approval was sought from the hospital management, and all study participants provided written informed consent before participation. No Legally Authorised Representative (LAR) was required for this study, as all participants were able and provided written informed consent. Therefore, informed consent from LAR was not applicable in this study.
Results
Demographic Characteristics of Study Participants
Socio-Demographic Characteristics of Respondents
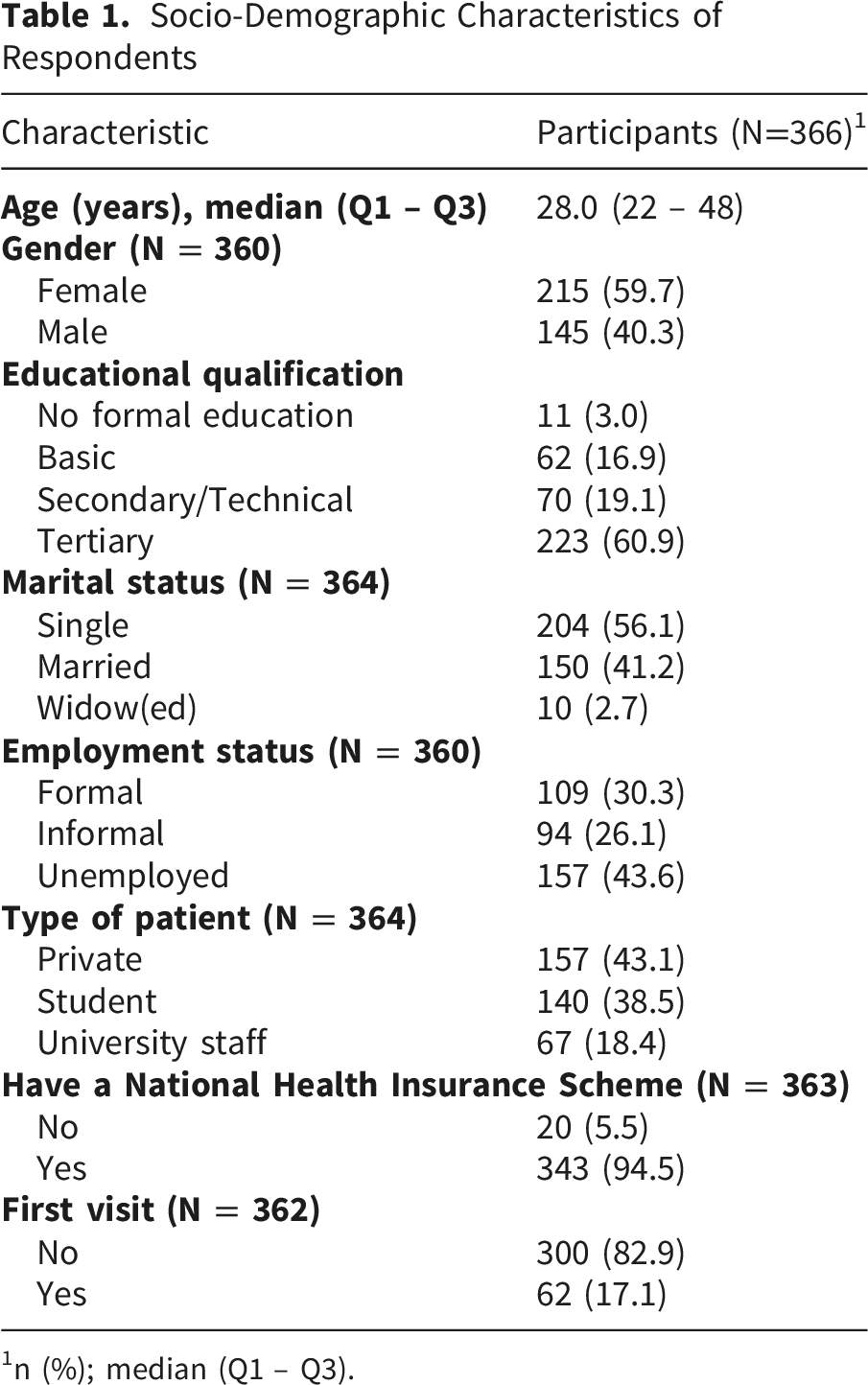
1n (%); median (Q1 – Q3).
Summary of Satisfaction and SERVQUAL Domains Among Study Participants
Summary of Satisfaction and SERVQUAL Domains

SD: Standard deviation; IQR: Interquartile range.
Structural Equation Modelling and Mediation Analyses for Patient Satisfaction
SEM Regression Weights for Patient Satisfaction

Note: Chisq = 478.16; DF = 168.00; p-value = <0.001; CFI = 0.96; TLI = 0.954; RMSEA = 0.071; SRMR: 0.030. Bold means significant predictors (p < 0.05)
In the mediation analysis, communication did not significantly mediate the association between the SERVQUAL dimensions and patient satisfaction, as the indirect effects were not significant. However, communication remained directly associated with satisfaction (β = 0.404, p = 0.017), and empathy was significantly associated with communication (β = 0.499, p = 0.011) (Supplemental Table 1).
Discussion
This study aimed to assess communication and SERVQUAL dimensions as determinants of patient satisfaction among outpatient attendees at a public university hospital in Ghana using the SERVQUAL framework and structural equation modelling. Overall, patient satisfaction was moderately high, with a median score of 75%. Most SERVQUAL domains and communication scores had median scores of 75%, suggesting a generally positive perception of service quality. The relatively high satisfaction observed in this study is consistent with previous research conducted in Ghana and LMICs, where patients reported favorable perceptions of healthcare services despite structural challenges such as long waiting times, resource constraints, and staff shortages. For example, studies conducted in Ghanaian public hospitals have reported satisfaction levels ranging between 70% and 90%, often attributed to improvements in hospital infrastructure and respectful provider-patient interactions.4,33 Similar findings have been reported in Ethiopia, Nigeria and Iraq, where patients reported higher satisfaction when healthcare providers treated them with respect, ensured privacy, and communicated effectively during clinical encounters.31,34,35
Tangibility, the highest-rated SERVQUAL domain in this study, reflects patients’ satisfaction with the hospital’s physical environment, staff appearance, and equipment availability, which are usually used as visible indicators for service quality.36-38 In Nigeria, a study found that tangible elements of healthcare services strongly influence patients’ initial perceptions of service quality. 31 In contrast, reliability received the lowest rating by the study participants. Reliability refers to healthcare providers’ ability to deliver services consistently, accurately, and as promised. 39 Lower reliability scores may indicate perceived gaps in service processes such as delays in receiving care, inconsistencies in service delivery, or challenges in obtaining follow-up services. Similar concerns have been reported in several studies across sub-Saharan Africa, where patients identified waiting times and service delays as key factors affecting satisfaction.40-42 These findings highlight the need for healthcare facilities to strengthen service processes and improve operational efficiency to ensure that infrastructure improvements are matched by reliable, consistent service delivery.
In the present study, the structural equation modelling results indicated that communication and empathy were the only variables associated with patient satisfaction, with both showing similar magnitudes of association. Given the cross-sectional design of this study, these associations should not be interpreted as evidence of causal effects but rather as patterns that warrant further investigation. These findings highlight the importance of interpersonal aspects of healthcare delivery in shaping patient satisfaction. Effective communication helps patients understand their care, trust healthcare providers, and feel confident about treatment decisions.
The association between communication and satisfaction observed in this study aligns with growing evidence from healthcare quality research demonstrating that communication is one of the most important determinants of patient satisfaction. Studies across healthcare settings have shown that effective provider-patient communication improves understanding, adherence to treatment, and trust in healthcare systems.43-45 Similarly, research on patient-centred care has shown that communication plays a central role in improving the patient experience by ensuring that healthcare services are responsive to patients’ needs and expectations. 46 In many healthcare environments, communication serves as the key link between clinical competence and patient perception of care.47,48
Empathy, which focuses on the ability of healthcare providers to understand patients’ concerns, respond to their emotional needs, and provide compassionate care49,50 was also identified as associated with patient satisfaction. Empathetic interactions are essential for building trust and creating supportive healthcare environments. A previous study by Keshtkar et al (2024) found that patients who perceive healthcare providers as empathetic were more likely to report greater satisfaction, improved psychological well-being, and stronger adherence to medical advice. 51 Empathy also contributes to stronger therapeutic relationships between patients and healthcare providers, thereby improving healthcare outcomes. 52 However, while these studies and the present findings suggest important links between empathy and patient-reported outcomes, causal pathways cannot be confirmed without longitudinal or experimental designs.
We tested whether communication mediated the relationship between SERVQUAL dimensions and patient satisfaction. The study found that communication did not significantly mediate the relationship between the SERVQUAL dimensions and patient satisfaction, as the indirect effects of these constructs were not significant. This pattern suggests that, within the limits of our data, improvements in SERVQUAL dimensions may not necessarily translate into higher patient satisfaction through changes in communication alone. Communication remained an independent determinant of patient satisfaction, suggesting a direct association rather than acting as a mechanism through which other SERVQUAL dimensions affect satisfaction. While a study conducted by Yanti et al (2025) in Indonesia reported mediation effects in which patient experience or communication explains the relationship between service quality and satisfaction, 53 the absence of mediation in this study may reflect the specific context of outpatient services, where communication plays an immediate and direct role in shaping patient perceptions.
Empathy emerged as a significant determinant of communication. This finding suggests that empathy shown by healthcare professionals may improve the quality of communication during encounters. Although the indirect effect was not statistically significant, the positive association between empathy and communication highlights the key role of empathetic care in improving patient experiences by facilitating more effective provider-patient communication. Our finding is consistent with previous studies demonstrating that patient perception of empathetic care is associated with the quality of provider-to-patient communication.54-56 These findings, therefore, highlight the central role of interpersonal care in determining patient satisfaction in outpatient healthcare services. While improvements in infrastructure and service processes remain important, strengthening communication and empathy among healthcare providers may produce more immediate improvements in patient satisfaction. Healthcare providers who communicate clearly and demonstrate empathy can significantly enhance patient experiences, even in resource-limited environments.
Our sample was relatively young, predominantly female and highly educated. The relatively young population may be partly due to the study being conducted in a university hospital, with students also sampled from the Students’ Clinic, one of the outpatient service points. 57 The Students’ Clinic serves a predominantly younger student population. 57 Similarly, the high proportion of highly educated participants may also be due to the two staff clinics, which are part of the hospital’s outpatient service points and are heavily dominated by faculty members. Additionally, the dominance of females in our sample aligns with the literature, suggesting that women exhibit better health-seeking behaviour than men. 58 These characteristics may influence participants’ perceptions of communication and service quality. For instance, younger, highly educated participants may have greater experience with healthcare delivery and may be better able to perceive and articulate their experiences of communication, empathy, and service quality. Similarly, females may be more concerned about the interpersonal dimensions of care, including provider responsiveness and empathy. As a result, our findings should be interpreted with caution, and their generalizability may be limited, as older or less-educated populations may yield different results.
Implication of Empathy and Communication for UHC
The observed influence of communication and empathy on patient satisfaction in this study has important implications for UHC. 59 Achieving UHC requires not only expanding access to healthcare but also improving the quality and responsiveness of healthcare services. Patient satisfaction is a key component in this process because individuals are more likely to use health services and follow treatment recommendations when they trust the healthcare system and perceive the care they receive as respectful, responsive, and effective. The observed association also highlights the need to strengthen patient-centred care within health systems. These findings provide evidence that interpersonal dimensions of care are significant aspect of quality healthcare within the broader goal of UHC. In Ghana and many other LMICs, health reforms have largely focused on expanding insurance coverage and improving infrastructure; however, these findings suggest that equal attention should be given to improving the interpersonal aspects of care.
Our findings suggest that improving the interpersonal component of care is relevant to increasing access to services in achieving UHC goals in Ghana. Training healthcare workers in effective communication, shared decision-making, and compassionate care can significantly enhance patient experiences and strengthen public trust in health services. Additionally, integrating communication and empathy training into health professional education and continuous professional development programs can strengthen patient-provider relationships and improve health outcomes. Healthcare institutions may also benefit from implementing routine patient satisfaction monitoring tools, such as SERVQUAL-based assessments, to track service quality and identify areas for improvement.
Strengths and Limitations of the Study
This study has several strengths. The study utilised a validated SERVQUAL-based instrument with high internal consistency across all constructs, ensuring reliable measurement of service quality and patient satisfaction. The use of structural equation modelling allowed the simultaneous examination of complex relationships among multiple SERVQUAL dimensions and patient satisfaction while accounting for measurement error.
Despite these strengths, several limitations should be considered when interpreting the results. The cross-sectional design limits the ability to establish causal relationships between SERVQUAL dimensions and patient satisfaction. The study was conducted in a single university hospital, which may limit the generalizability of the findings to other healthcare facilities with different resource levels.
Our findings provide useful evidence for future studies to build on by addressing the contextual and methodological limitations. Future research may adopt a longitudinal and multi-site design with a more diverse population to enhance causal inference and improve the generalisability of findings on communication, empathy and patient satisfaction. Additionally, a qualitative approach is needed to provide a more nuanced understanding of how communication and empathy are linked to patient satisfaction.
Conclusion
The findings revealed generally high levels of patient satisfaction, particularly regarding the hospital’s physical environment and staff professionalism, although reliability was perceived as the weakest dimension of SERVQUAL. The structural equation modelling results identified communication and empathy as the key determinants of patient satisfaction in this study. These findings reflect the critical role of interpersonal care in shaping patient experiences in this study. Effective communication and empathetic interactions between healthcare professionals and patients can significantly enhance patient satisfaction and strengthen trust in healthcare services. Prioritising patient-centred communication and compassionate care should therefore be an integral part of healthcare quality improvement strategies aimed at strengthening health systems and advancing progress towards UHC. Future research could adopt a mixed-methods approach to further explore these relationships and better understand how communication and empathy influence patient satisfaction in different healthcare settings.
Supplemental Material
Supplemental Material - Determinants of Patient Satisfaction in a Public University Hospital in Ghana: A Structural Equation Modelling Approach
Supplemental Material for Determinants of Patient Satisfaction in a Public University Hospital in Ghana: A Structural Equation Modelling Approach by Bhavana Singh, Kwame Tieku Asaaseasa, Julius Kwabena Karikari, Douglas Aninng Opoku, Irene Ohene-Manu1, Richmond Darko, Ricky Antwi Boasiako, Alfred Matthew Owusu, Akwasi Ohene Adjei, Edward Osei-Boateng, Emmanuel Konadu, Eric Kojo Nsa Oduro and Nana Kwame Ayisi-Boateng Health Services Insights.
Supplemental Material
Supplemental Material - Determinants of Patient Satisfaction in a Public University Hospital in Ghana: A Structural Equation Modelling Approach
Supplemental Material for Determinants of Patient Satisfaction in a Public University Hospital in Ghana: A Structural Equation Modelling Approach by Bhavana Singh, Kwame Tieku Asaaseasa, Julius Kwabena Karikari, Douglas Aninng Opoku, Irene Ohene-Manu1, Richmond Darko, Ricky Antwi Boasiako, Alfred Matthew Owusu, Akwasi Ohene Adjei, Edward Osei-Boateng, Emmanuel Konadu, Eric Kojo Nsa Oduro and Nana Kwame Ayisi-Boateng Health Services Insights.
Footnotes
Acknowledgements
We are grateful to the management and staff of the University Hospital, KNUST, for their support in conducting this study. We also appreciate the support of the research assistants who facilitated the data collection and other research activities.
Ethical Considerations
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval to conduct the study was obtained from the Committee on Human Research, Publications and Ethics, School of Medical Sciences, KNUST, Kumasi, Ghana (reference number: CHRPE/AP/1131/25) on 31st October 2025.
Consent to Participate
All study participants provided written informed consent before participation. No Legally Authorized Representative (LAR) was required for this study, as all participants were able and provided informed consent. Therefore, informed consent from LAR was not applicable in this study. Participants were briefed on the study, including its background, objective, potential risks, and benefits of participation. They were also made aware that participation was voluntary and that their decision to either accept or reject would not affect their welfare or care at the hospital.
Author Contributions
BS, RD, IOM, RAB, AOA, EO-B, and NKAB contributed to the conceptualisation of the idea, study protocol development, supervision, and manuscript review. EK, JKK, and DAO also contributed to the conceptualisation, data curation, statistical analysis, writing the original draft, and manuscript review. KTA and EKNO were involved in data collection and curation, writing the original draft, and reviewing the manuscript. All authors read and approved the manuscript for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.