
Abstract
Background/objectives
Staphylococcus aureus (S. aureus) can cause life-threatening infections, with colonization often preceding infection. Understanding the determinants of S. aureus carriage may improve infection prevention. While smoking has been associated with S. aureus carriage, studies on smokeless tobacco products remain scarce. This study aimed to investigate whether the use of snuff (Swedish snus), a smokeless tobacco product, is associated with S. aureus carriage in adolescents.
Design
We used data from Fit Futures 1, a population-based cross-sectional study including 1,038 participants (93% attendance).
Methods
A total of 457 boys and 443 girls had data on snuff use and two nasal and throat swab cultures for S. aureus carriage assessment. Snuff use was defined as occasional or daily use. Logistic regression analysis was used to examine the association between snuff use and S. aureus carriage, with odds ratios (ORs) adjusted for known risk factors.
Results
Snuff use was associated with a 64% higher odds of nasal carriage (95% CI = 1.18-2.26; carriage defined as one or two positive nasal cultures) compared to non-use. In sex-stratified analyses, this association was observed only among girls, with an adjusted OR of 1.62 (95% CI = 1.03-2.55; carriage defined as two positive nasal cultures) and an adjusted OR of 1.99 (95% CI = 1.25-3.16; carriage defined as one or two positive nasal cultures). Among girls using snuff, the adjusted OR for S. aureus throat carriage was 1.66 (95% CI 1.06-2.59; carriage defined as two positive throat cultures) compared to non-users.
Conclusion
We identified an association between snuff use and S. aureus nasal and throat carriage among adolescent girls. Girls who used snuff had higher odds of S. aureus nasal (62%) and throat (66%) carriage compared to female non-users. Futures longitudinal studies are needed to clarify whether the observed associations reflect casual relationships.
Introduction
Staphylococcus aureus (S. aureus) is one of the most potent human bacterial pathogens and can cause life-threatening infections. 1 However, 20-30% of the general adult population carry S. aureus in the anterior nares as part of their normal flora, with higher carriage rates observed among men and younger age groups.2-6 Studies among various patient populations have shown that nasal carriers have an increased risk of S. aureus infections and are frequently autoinfected with their own bacterial strain. 7 Because colonization precedes infection, and S. aureus infections are associated with substantial morbidity and mortality, carriage represents a major public health concern.8,9
To reduce the risk of infections, hospitals have implemented measures to eradicate or at least suppress nasal carriage prior to surgery and invasive procedures. 10 S. aureus also colonizes other anatomical sites including the throat, though the role of this reservoir in transmission and infection remains less well understood. 11 Nasal decolonization is typically followed by subsequent decolonization of the perineum, pharynx, and axillae, reinforcing the assumption that the nose serves as the primary site of S. aureus colonization. 11
Prevention of S. aureus infections and death is a major clinical and public health challenge. Identifying modifiable determinants of S. aureus carriage is therefore essential, as effective prevention strategies rely on understanding factors that may be amenable to intervention. Colonization likely results from an interplay between host and microbe. For instance, multiple adaptive bacterial mutations associated with S. aureus colonization have been demonstrated. 12 Cross-sectional studies have found that high serum glucose levels and low serum vitamin D levels are associated with a higher prevalence of S. aureus nasal carriage.4,5 Furthermore, young women using combination hormonal contraceptives have been found to have higher nasal carriage rates than non-users, and carriage has also been linked to circulating testosterone in women.13,14
Cigarette smoking has been negatively associated with S. aureus nasal carriage in some observational studies, 5 while other studies have reported a positive association between smoking and nasal carriage, 15 or as having no association. 16 It has been hypothesized that a link with cigarette smoking may be due to effects on both microbe and host. Lacoma et al showed that cigarette smoke exposure induces strain-specific growth inhibition of S. aureus, while also enhancing biofilm formation, as well as increased invasion and persistence in bronchial alveolar epithelial cells. 17 In an in-vitro study investigating the nicotine component of cigarette smoke, Shi et al found that nicotine treatment enhanced S. aureus adherence and biofilm formation but inhibited bacterial virulence. 18 Cigarette smoking affects both innate and adaptive immune responses, thereby increasing the risk of infections. 19 Cole et al reported that healthy smokers had higher nasal S. aureus loads than healthy non-smokers and that smoking cessation improved innate host immune responses and increased the clearance rate of S. aureus. 20 However, it remains unclear whether direct exposure to cigarette smoke or indirect exposure to tobacco-derived chemicals through systemic uptake plays a more significant role in S. aureus nasal carriage. Notably, studies examining the impact of smokeless tobacco products on S. aureus carriage are largely lacking.
In Norway, the use of the smokeless tobacco product “Swedish snus,” a moist snuff placed under the lip, has a long tradition and is legally available to individuals aged 18 years and older. 21 According to Statistics Norway, use of snuff has increased over the past decade, with the proportion of daily users aged 16-24 years rising from 18% in 2011 to 21% in 2024. 22 Its speculated that this increase in use is due to availability and the perception of low risk with use. 23 Compared to smoking, research on the potential health effects of smokeless tobacco remains limited. To the best of our knowledge, no studies have investigated a possible association between snuff use and S. aureus carriage. Given that snuff components are absorbed through the oral mucosa and enter systemic circulation, it is plausible that snuff use may be a determinant for S. aureus carriage both in the nasal cavity and oropharynx. The aim of this study was to investigate the potential association between snuff use and nasal and throat carriage of S. aureus in a general adolescent population in Northern Norway.
Material and Methods
Population and Study Design
The study population consisted of participants from the Fit Futures 1 study (FF1). 24 Conducted in 2010-2011, FF1 invited all first-year upper-secondary school students from the municipalities of Tromsø and Balsfjord in Northern Norway to participate in a health and lifestyle examination. A total of 1,038 students attended (508 girls and 530 boys), corresponding to a 93% attendance rate. FF1 participants attended a half-day visit at the Clinical Research Unit, University Hospital of North Norway. During this visit, they provided information on alcohol use, snuff use, smoking, atopic eczema, physical activity and hormonal contraceptives through a self-administered an self-reported electronic questionnaire. Additionally, trained nurses conducted interviews about medications, chronic disease, social network and menstruation/pregnancy. As well as preforming microbiological sampling, blood sampling, and general clinical examinations, including height and weight measurements for body mass index (BMI) calculation (kg/m2). 25
We excluded 36 participants due to an age > 19 years, in accordance with the World Health Organization’s definition of adolescents as individuals aged 10-19 years.
26
Additionally, 19 participants were excluded due to antibiotic intake within the 24 hours preceding nasal and throat swabbing. Furthermore, 83 participants were excluded due to missing data on snuff use and/or nasal and throat swab samples (Figure 1). Excluded participants did not differ in terms of age, BMI, glycated hemoglobin (HbA1c), atopic eczema, smoking, alcohol use or physical activity compared to study participants. The study population. Fit Futures 1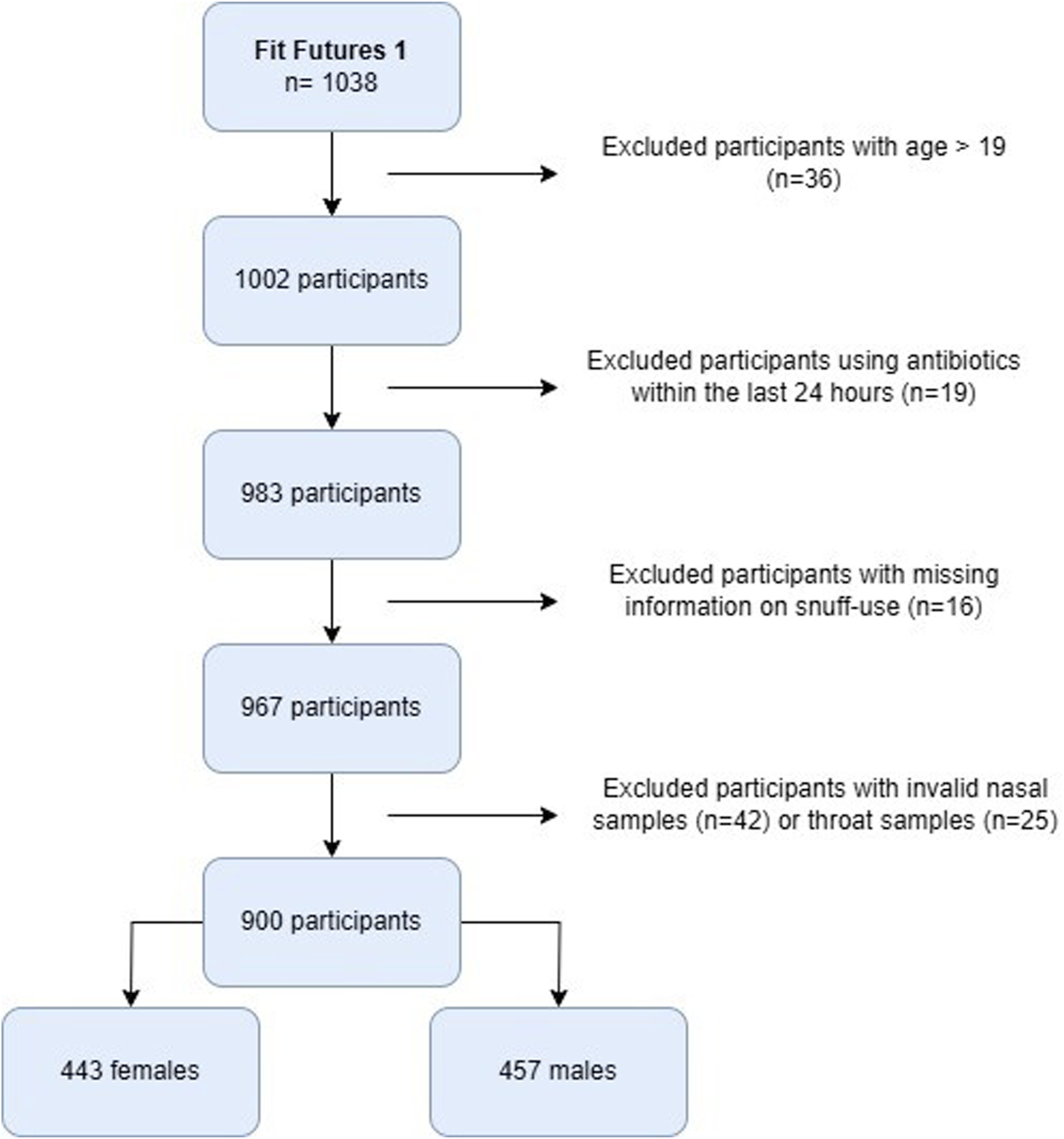
Detection of S. aureus Colonization and Carriage
To detect S. aureus carriage, samples were collected during the half-day hospital visit and repeated approximately one week later at the school, both times by trained health personnel. Swabs were taken from the anterior nares and the surface of both tonsils with NaCl-moistened sterile swabs. The swabs were enriched in Bacto Staphylococcus medium broth (Difco laboratories, Sparks, MD, USA) and incubated for 18-24 hour at 37 °C. One drop of enrichment broth was streaked on blood agar, chromID S. aureus and chromID™ MRSA agars (bioMérieux, Marcy l’Etoile, France) and incubated for 48 hours at 35°C. Colony morphology on the agar plates served as the basis for further S. aureus identification. Suspected positive colonies were confirmed as S. aureus using the Staphaurex Plus agglutination test (Murex Diagnostic Ltd, Dartford, UK). No methicillin-resistantStaphylococcus aureus (MRSA) isolates were detected. Based on the culturing results, S. aureus carriage was classified into three categories: non-carriers (two negative swabs), intermittent carriers (one positive swab), and persistent carriers (two positive swabs). In the logistic regression models, we used a dichotomous S. aureus outcome variable; “Persistent carriers” versus “Others” (including non- and intermittent carriers), representing a modified application of the S. aureus carriage classification proposed by van Belkum et al. 27 Additionally, we applied an alternative dichotomization, categorizing participants as “Carriers” (at least one positive swab) and “Non-carriers” (two consecutive negative swabs).
Smokeless Tobacco Use Assessment
Smokeless tobacco use was assessed through an electronic questionnaire, which included the question: “Do you use snuff?” with response options “No, never”, “Yes, sometimes”, “Yes, daily”. For the statistical analysis, snuff use was recoded into a dichotomous variable with the categories “No snuff use/non-user” and “Snuff use/user”.
Statistical Analysis
To investigate the association between snuff use and nasal and throat carriage of S. aureus, we used descriptive analyses and logistic regression models. Differences in S. aureus carriage prevalence between snuff users and non-users were assessed using chi-square test. Logistic regression analysis was conducted to estimate the odds ratio (OR) for S. aureus nasal and throat carriage among snuff users compared to non-users adjusting for potential confounding factors. Model selection was performed using DAGitty software (Figure 2).
28
Because the prevalence of S. aureus is well known to differ between women and men, and because the pattern of S. aureus carriage in relation to snuff use also varied by sex in our dataset, we chose to stratify the analyses by sex, in addition to presenting results for the total population, despite the test for interaction not reaching statistical significance. Missing data was excluded from the analysis. Hosmers-Lemeshow goodness of fit is reported for all statistical models. All statistical analyses were done using Stata/MP 18.5 for Macintosh, and statistical significance was set at p < 0.05. Directed acyclic graph for the association between snuff-use and Staphylococcus aureus carriage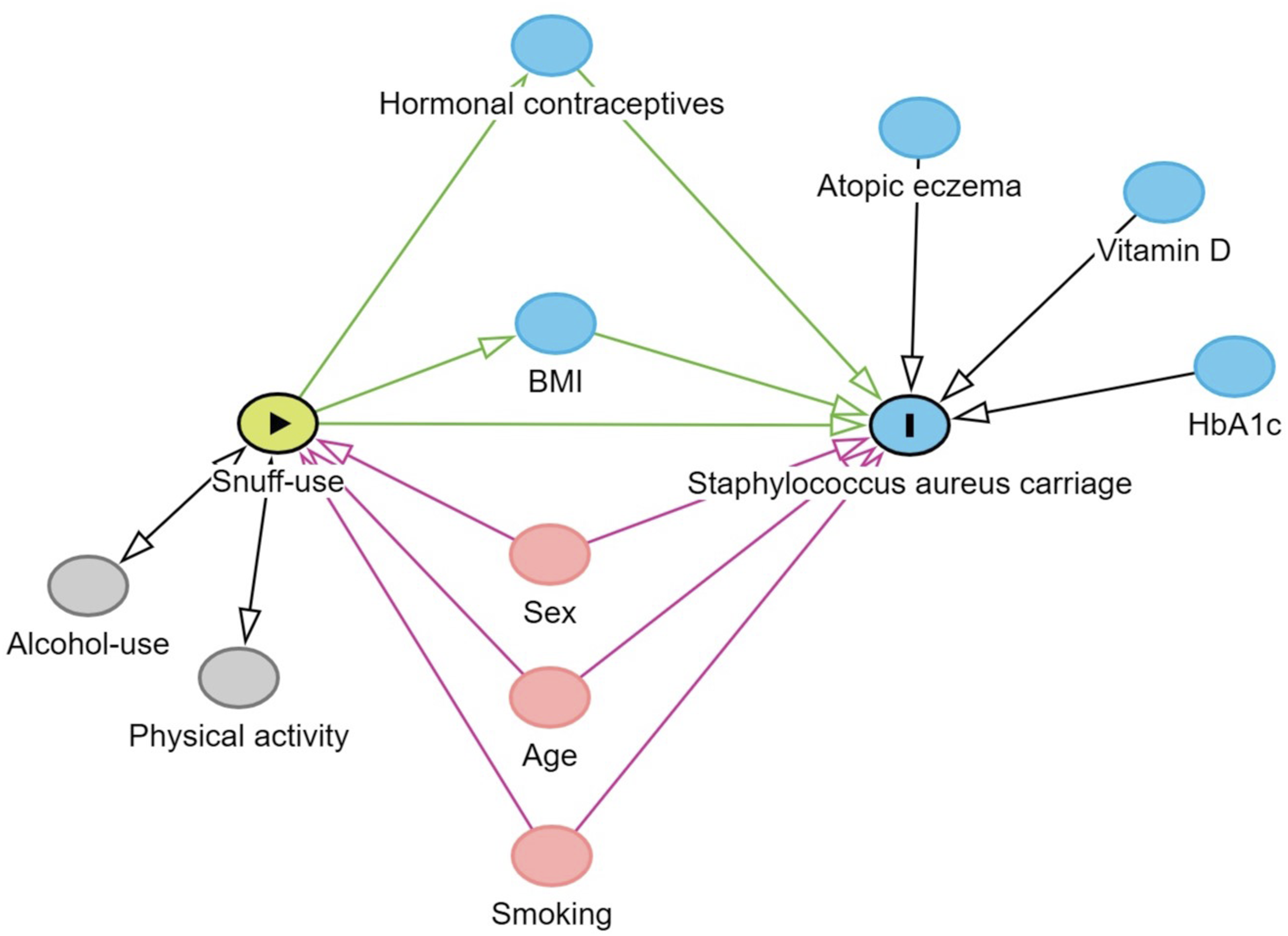
Results
Characteristics of the Study Population in the Fit Futures 1 Study. Figures are Means (Standard Deviations) and Numbers (Percent). Numbers May Vary due to Missing Values
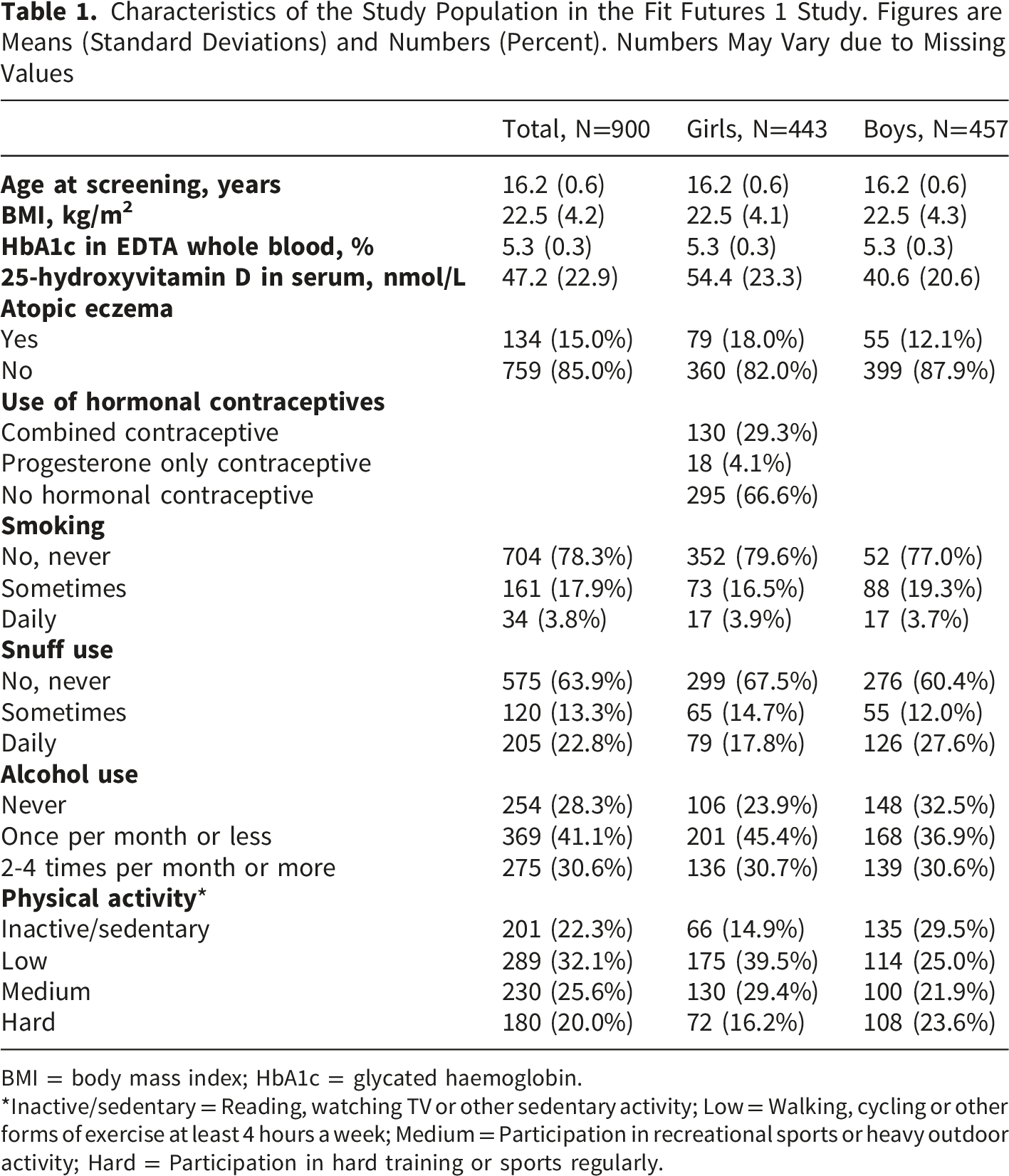
BMI = body mass index; HbA1c = glycated haemoglobin.
*Inactive/sedentary = Reading, watching TV or other sedentary activity; Low = Walking, cycling or other forms of exercise at least 4 hours a week; Medium = Participation in recreational sports or heavy outdoor activity; Hard = Participation in hard training or sports regularly.
Repeated Nasal Swab Samples. Staphylococcus aureus Culturing Results and Carrier Status by Snuff Use (N and Percent in Brackets). The Fit Futures 1 Study
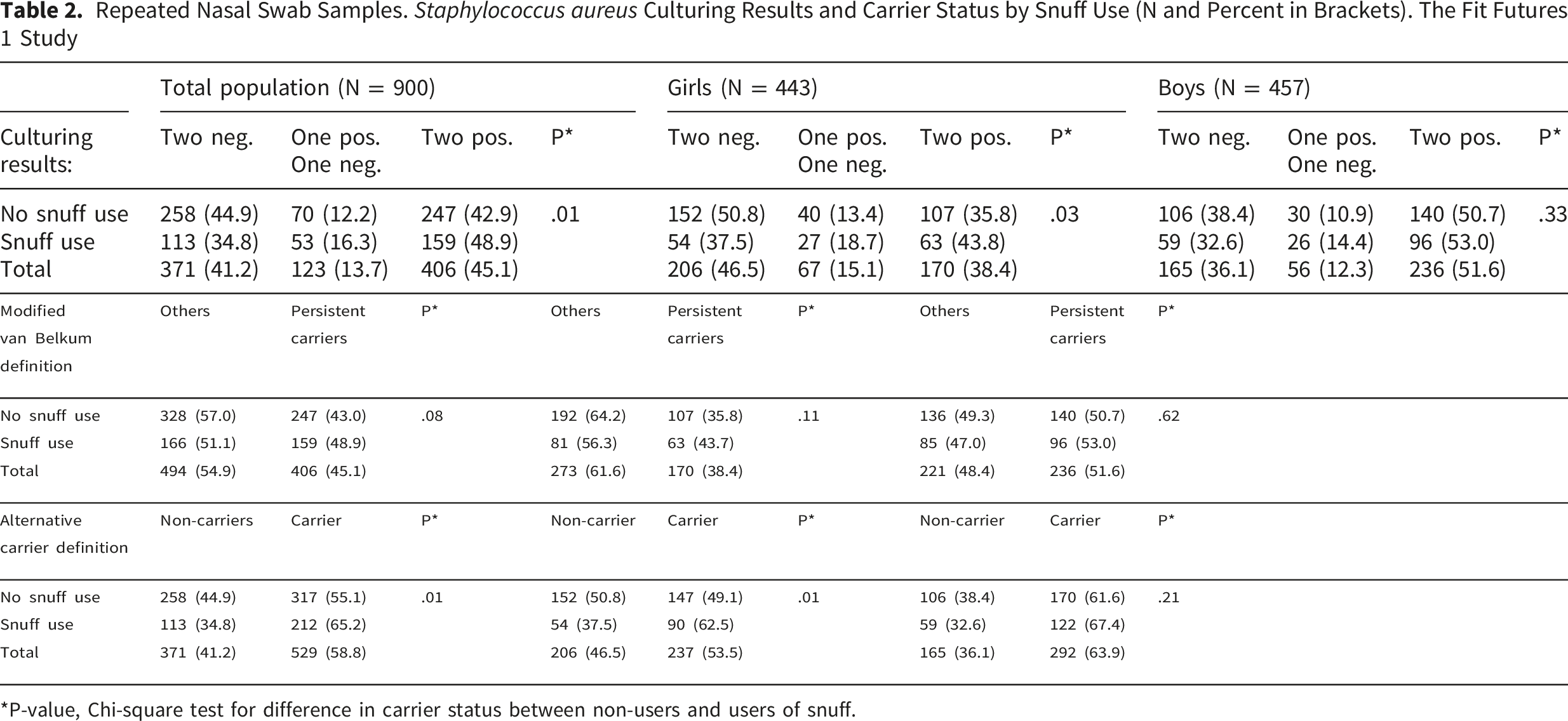
*P-value, Chi-square test for difference in carrier status between non-users and users of snuff.
Repeated Throat Swab Samples. Staphylococcus aureus Culturing Results and Carrier Status by Snuff Use (N and Percent in Brackets). The Fit Futures 1 Study
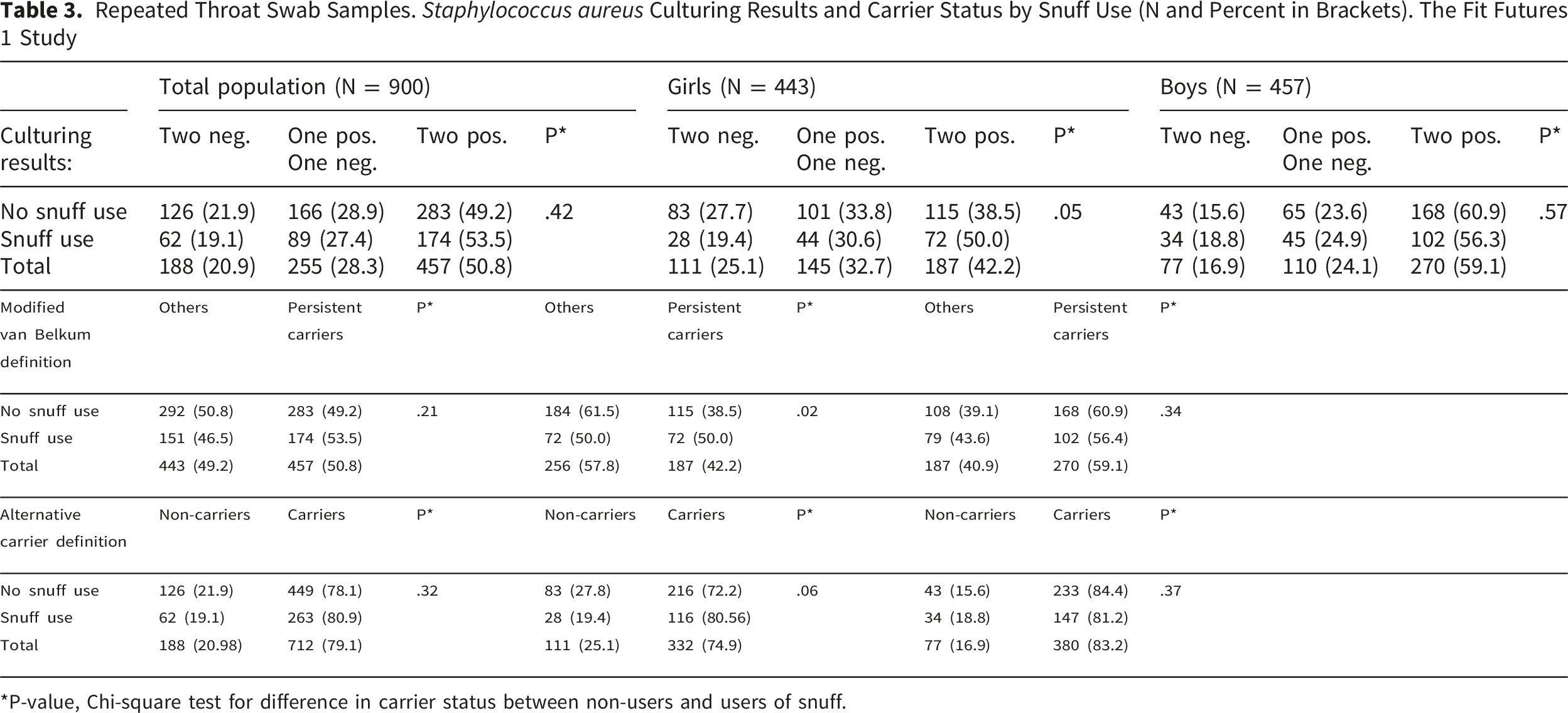
*P-value, Chi-square test for difference in carrier status between non-users and users of snuff.
Associations Between Snuff Use and Staphylococcus aureus Nasal Carrier State; Odds Ratios (OR) and 95% Confidence Intervals (95% CI) From Multivariable Logistic Regression Analysis. The Fit Futures 1 Study
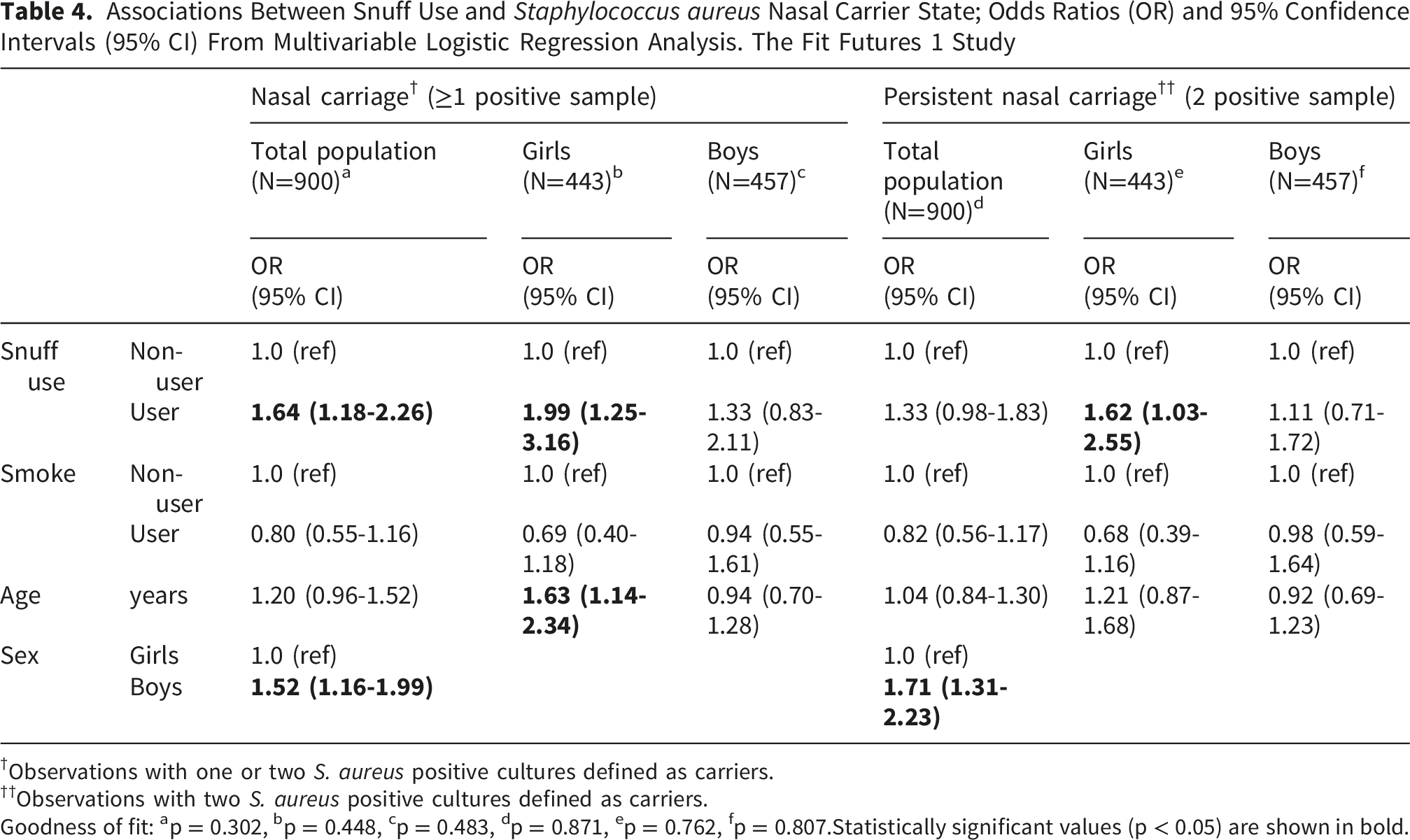
†Observations with one or two S. aureus positive cultures defined as carriers.
††Observations with two S. aureus positive cultures defined as carriers.
Goodness of fit: ap = 0.302, bp = 0.448, cp = 0.483, dp = 0.871, ep = 0.762, fp = 0.807.
Statistically significant values (p < 0.05) are shown in bold.
Associations Between Snuff Use and Staphylococcus aureus Throat Carrier State; Odds Ratios (OR) and 95% Confidence Intervals (95% CI) From Multivariable Logistic Regression Analysis. The Fit Futures 1 Study
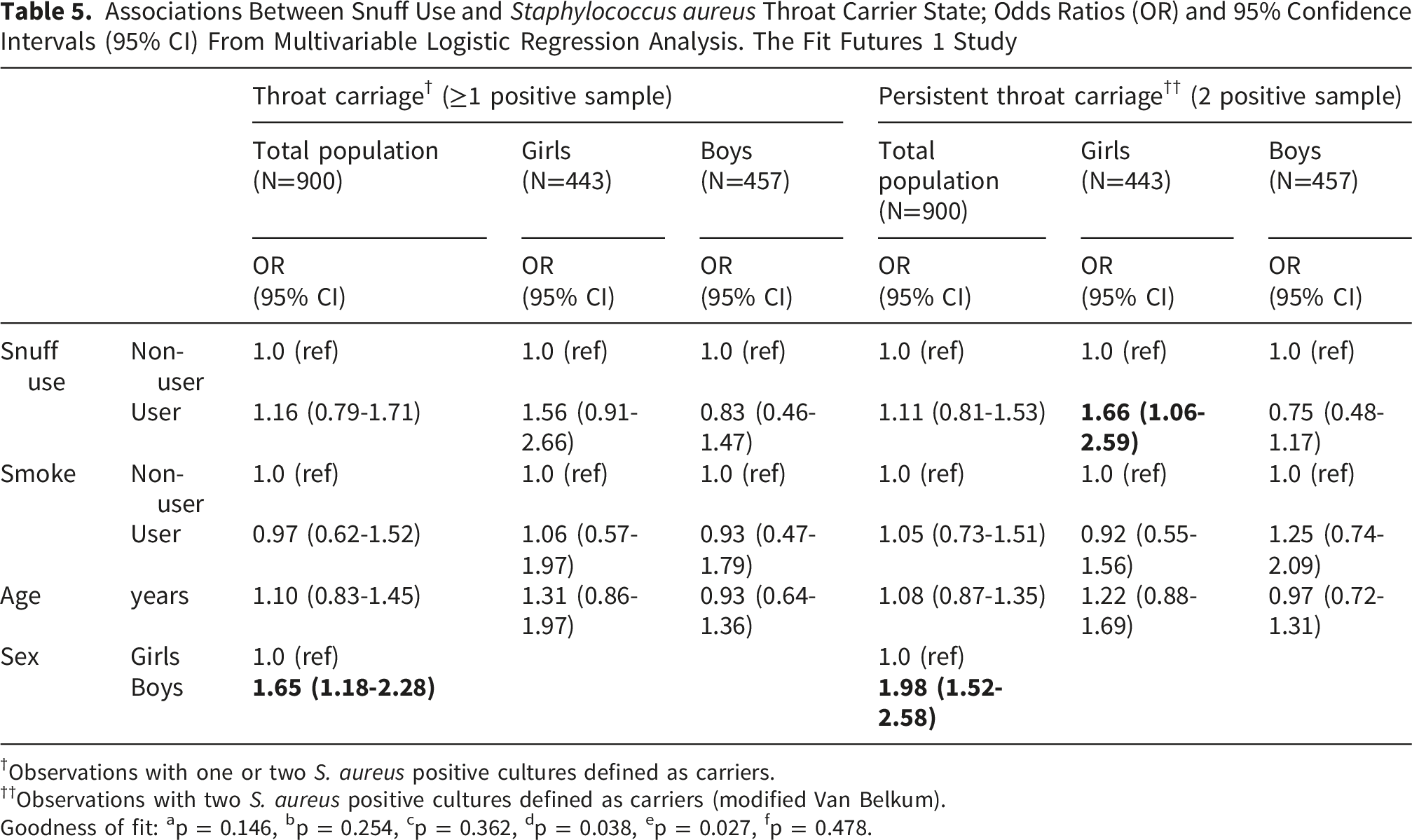
†Observations with one or two S. aureus positive cultures defined as carriers.
††Observations with two S. aureus positive cultures defined as carriers (modified Van Belkum).
Goodness of fit: ap = 0.146, bp = 0.254, cp = 0.362, dp = 0.038, ep = 0.027, fp = 0.478.
A sensitivity analysis including snuff-use only, smoking only and dual-use (participants reporting smoking and snuff use) showed an increased odds of nasal carriage for the snuff-only group. Participants reporting only smoking had lower odds of nasal carriage compared to non-users, though not statistically significant. Dual-use was not statistically significantly associated with nasal carriage, representing the conflicting effects of smoking and snuff-use (Supplementary table 1). No similar association was shown for the sensitivity analysis for throat carriage (Supplementary table 2).
Discussion
In this population-based cross-sectional study, we identified an association between snuff use and S. aureus carriage among adolescent girls. Our findings indicate that girls who used snuff either occasionally or daily had 99% increased odds of nasal carriage of S. aureus compared to non-users. Additionally, they exhibited a 62% higher odds of persistent nasal carriage and a 66% higher odds of S. aureus throat carriage.
In our study, the association between snuff use and S. aureus carriage was observed only among girls, while no similar association was found in boys. The reason for this discrepancy remains speculative. Male sex is a well-established risk factor for S. aureus nasal carriage, as demonstrated in several epidemiological studies, including the Fit futures cohort. 13 Additionally, sex steroid hormones are known to regulate immune responses, 29 and circulating sex-steroid levels have been identified as determinants for S. aureus carriage.5,14 Studies have shown that smoking is associated with lower estrogen levels and higher testosterone levels in females.30,31 If smokeless tobacco exerts a similar effect on sex steroid hormones, this could be a plausible explanation for why the association between snuff use and S. aureus carriage was observed only in females. However, it remains unclear whether the increased prevalence of S. aureus nasal and throat carriage among snuff users is directly caused by tobacco exposure or by other factors associated with snuff use, such as shared behavioral or environmental exposures. The use of snuff involves frequent hand-to-mouth contact and sharing of snuff containers, which may facilitate S. aureus transmission. This theory is strengthened by the conflicting results between snuff-use and smoking, also demonstrated in other studies. 5 A 2016 study found that some smokeless tobacco products contained S. aureus, 32 supporting the hypothesis that snuff use may be a risk factor for S. aureus carriage. Nevertheless, further research, including larger population-based prospective studies, is needed to establish a causal relationship.
To the best of our knowledge, no previous studies have investigated the association between smokeless tobacco use and S. aureus nasal or throat carriage. One study demonstrated that smokeless tobacco extract (STE) at low concentrations enhanced the production of cytokines. 33 However, findings from Hasseus et al suggest that water-soluble extracts from Swedish moist snuff significantly inhibited T-cell proliferation induced by accessory cells from rats, 34 indicating an immunosuppressive effect. Shi et al reported that nicotine treatment enhances S. aureus biofilm formation by promoting initial attachment and extracellular DNA release, while simultaneously inhibiting S. aureus virulence. 18 The existing research presents conflicting evidence, making it difficult to draw definitive conclusions regarding the effects of smokeless tobacco on the immune response. Given our findings of an association between smokeless tobacco use and a higher prevalence of S. aureus colonization, it is plausible that smokeless tobacco may inhibit the innate immune response or promote bacterial adherence and growth.
This study has several important strengths, but also limitations that should be considered when interpreting the findings. Strengths of this study include the high response rate (93% attendance), which likely reduces selection bias. The prevalence of the main predictor snuff-use is similar compared to the national prevalence. 22 We therefore believe the findings to be generalizable to adolescents with similar sosioeconomic backgrounds in comparable societies where smokeless tobacco is available.
The use of two repeated nasal and throat cultures collected approximately one week apart represents a methodological strength. This repeated sampling design improves the reliability of carriage classification compared with single-sample studies. Participants with two culture-positive samples from a single site can be classified with greater confidence as persistent or S. aureus–dominant carriers27,35 Our finding of an association between snuff use and any S. aureus positive culture from one site may indicate that snuff users have a higher likelihood of both persistent and transient colonization. Alternatively, limited sampling, particularly at school, may have led to some misclassification of persistent carriers.
The high prevalence of S. aureus carriage observed in our study is partly attributable to the use of enrichment methods and should be considered when comparing our results with other studies. 13 Access to a large dataset with a wide range of variables allowed adjustment for several known risk factors for S. aureus nasal and throat carriage. As a population-based study, the findings are largely representative of the general adolescent population.
Nevertheless, some limitations must be acknowledged. The study was conducted within a narrow age range, and the results cannot be directly generalized to other age groups without further research. Another limitation is that snuff use was self-reported. Since the sale of snuff and tobacco products to individuals under 18 years of age is illegal in Norway, underreporting of snuff use is possible. However, any misclassification of snuff use is likely to be non-differential, meaning that it would affect both carriers and non-carriers of S. aureus equally, potentially attenuating the observed associations. Furthermore, we did not collect data on the average number of snuff portions consumed per week among users, which precluded assessment of a potential dose-response relationship. In addition, the questionnaire was not a previously validated instrument, and no formal pilot study with predefined testing procedures was conducted. However, previous research among adolescents in similar age groups has demonstrated high sensitivity and specificity of self-reported snus use, suggesting that such measures are generally reliable. 36 Nonetheless, the lack of formal validation should be considered when interpreting the findings.
The logistic regression analysis was adjusted for known risk factors for S. aureus carriage, including sex, age and smoking. However, residual confounding due to unmeasured variables cannot be ruled out, including social network. 37 A formal power calculation was not performed because the analyses were based on the entire Fit Futures cohort rather than on a sample drawn from a larger source population. The sample size was therefore fixed and not determined by an a priori design consideration. In this setting, statistical precision is more appropriately evaluated through the reported effect estimates and their 95% confidence intervals. Post hoc power calculations would not provide additional meaningful information beyond these measures.
Conclusion
Our findings indicate a higher risk of S. aureus colonization among girls who use snuff. This supports the hypothesis that smokeless tobacco use may have negative health effects that are not yet fully understood. These findings are relevant for public health education, highlighting the potential risks associated with smokeless tobacco use. Additionally, our study contributes to the understanding of possible determinants of S. aureus carriage. This knowledge is valuable, as it may offer new perspectives on controlling the S. aureus reservoir and preventing S. aureus-related diseases in the population. However, future studies are needed to determine whether a causal relationship exists between smokeless tobacco use and S. aureus carriage.
Supplemental Material
Supplemental Material -Sex-Specific Associations Between Smokeless Tobacco Use and Staphylococcus aureus Carriage in Norwegian Adolescents
Supplemental Material for Sex-Specific Associations Between Smokeless Tobacco Use and Staphylococcus aureus Carriage in Norwegian Adolescents by Dina B. Stensen, Anna Karlsen, Gunnar Skov Simonsen, and Anne-Sofie Furberg in Tobacco Use Insights.
Footnotes
Acknowledgement
We thank the participants of The Fit Futures 1 study for their contribution. We also express our gratitude to the Clinical Research Department at the University Hospital of North Norway, Tromsø, for their assistance with data collection. Lastly, we extend our appreciation to the Department of Medical Microbiology and the Department of Community Medicine at the Faculty of Health Sciences for their support.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The data collection in FF1 was approved by the Regional Committee for Medical and Health Research Ethics, REK North (REF NR 16773, date: 01.09.10), and the Norwegian Data Inspectorate. The present study received approval from REK North (REF NR 23432), date: 01.10.11.
Consent to Participate
All participants provided written informed consent upon arrival at the study site. For participants younger than 16 years of age, written informed consent was obtained from parents, legal guardians or legally authorized representatives.
Author Contributions
ASF and GSS conceptualized the study and contributed in revision and editing. DBS and AK analyzed the data and wrote the first draft of the manuscript. All authors made agreed on the final version of the manuscript for publishing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Fit Futures 1 was funded by Troms county municipality, Northern Norway Regional Health Authority, Odd Berg Medical Research Foundation, and “Sparebankens gavefond” UiT.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the Fit Futures study, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available upon request from the Fit Futures study,
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.