
Abstract

Introduction
Cell-based therapy is an exciting, emergent treatment frontier for cardiovascular repair that has seen a remarkable evolution over the last decade. Clinical studies have been published using different types of adult cells to treat the problems of acute and established myocardial infarction (MI), refractory coronary ischemia and both ischemic and non-ischemic cardiomyopathy. In this review, we will initially address the key issue of cell delivery to the myocardium, followed by an overview of past and present clinical experience in this field.
Cell Delivery
The goal of any delivery approach is to transplant enough cells into the cardiac territory of interest, to maximize initial retention of cells within that area and achieve adequate local engraftment and function at this site. This is heavily influenced both by the type of cell being transplanted and the myocardial microenvironment. There are three basic strategies for directing cells to the heart: systemic therapy, focused coronary vascular infusion and direct myocardial injection.
Systemic Therapy
Systemic administration of cell therapy can be accomplished either by (1) using growth factors to mobilize progenitor cells from bone marrow to the heart or (2) infusing cells into a peripheral vein.
In the early stages of MI healing, local and systemic chemoattractants and cell adhesion molecules are upregulated, including granulocyte-colony stimulating factor (G-CSF), stromal cell-derived factor 1 (SDF-1) and stem cell factor (SCF) (Lee et al. 2000; Askari et al. 2003; Ma et al. 2005). These cyto-kines encourage the mobilization of stem cells from tissues such as bone marrow and facilitate their migration to the damaged myocardium. This has also been observed to a lesser degree in ischemic cardiomyopathy (Askari et al. 2003). Usually, endogenous migration of circulating cells to the heart is not sufficient to impact greatly on myocardial healing or to prevent deleterious ventricular remodeling (Shintani et al. 2001). However, researchers have attempted to artificially induce this process by the use of supra-physiologic doses of exogenous growth factors like GSC-F. G-CSF therapy may therefore provide indirect cardiovascular effects by mobilizing bone marrow cells (BMCs) and endothelial progenitor cells (EPCs) to sites of myocardial injury where they promote and participate in neovascularization. In addition, direct actions on the heart and vascular system have also been demonstrated following growth factor therapy in acute MI, chronic ischemia and cardiomyopathy. These include inflammatory and scar-modifying effects, pro-angiogenic stimulation of endothelial and smooth muscle cells and anti-apoptotic protection of cardiomyocytes (Kovacic et al. 2007; Hu et al. 2007a). To date, functional outcomes have been encouraging, especially at a preclinical level, although there is evidence that efficacy may be superior when growth factor treatment is combined with actual cell transplantation (Kondoh et al. 2007). Several small-scale clinical studies applying G-CSF therapy alone or in combination with cellular therapy, have been performed in patients with chronic myocardial ischemia and acute MI, but are notable for the heterogeneity of their design and their results. Furthermore, safety concerns of increased coronary restenosis and acute coronary thrombosis have been raised (Kang et al. 2004).
Peripheral venous administration of cells has been used in animal models of MI (Bittira et al. 2003; Barbash et al. 2003; Ma et al. 2005; Price et al. 2006). Despite limited retention of transplanted cells within the myocardium, these studies provided evidence of modest cardiac improvement. Non-cardiac entrapment of cells is of particular concern with this approach, as highlighted by imaging studies that have made use of tracer molecule-labeled cells and SPECT, CT or MRI to track their engraftment (Gao et al. 2001; Chin et al. 2003; Barbash et al. 2003; Kraitchman et al. 2005). This may be especially problematic with adherent cell types such as mesenchymal stem cells (MSCs) (Aicher et al. 2003). Currently, a multi-center clinical trial in the United States is investigating the effectiveness and safety of intravenous MSC therapy in acute MI (Schuleri et al. 2007). In non-acute cardiac disease, intravenous delivery remains untested, although in this setting the lower expression of myocardial and systemic chemo-attractants is likely to hinder adequate cardiac engraftment of cells delivered peripherally.
Intracoronary Infusion
Selective intracoronary administration of cell therapy achieves higher first-pass delivery of cells to the site of myocardial injury, than is the case with systemic therapy. Unfractionated BMCs, MSCs and peripheral blood cells have all been delivered by coronary infusion in clinical trials of acute MI (Strauer et al. 2002; Assmus et al. 2002; Wollertet al. 2004; Chen etal. 2004; Bartuneket al. 2005), old MI (Assmus et al. 2006), ischemic cardiomy-opathy (Boyle et al. 2006) and non-ischemic cardiomyopathy (Seth et al. 2006). Typically, cells are injected through the central lumen of an over-the-wire balloon catheter during transient balloon inflations, which stop coronary blood flow, to prevent antegrade washout of cells and provide adequate exposure time to the microcirculation of the infarct-related vessel. In the context of recent MI where the culprit artery has been reperfused, this strategy is believed to enable cells to permeate across the damaged microvascular bed and distribute into the infarct territory and the adjacent peri-infarct tissue. Peri-infarct cardiomyocytes are an important target of treatment as they are vulnerable to “demand” ischemia, hypertrophic change and apoptosis as part of the post-infarction remodeling process. The suitability of intracoronary cell delivery is not established for patients with chronic myocardial ischemia and non-ischemic cardiac disease. It is also contentious as to whether this approach is safe for the administration of large, adherent cell types (e.g. MSCs and SkMs), with MSC infusion reportedly causing microvascular obstruction and increased myocardial ischemia in two separate large animal studies (Vulliet et al. 2004; Freyman et al. 2006).
Intra-myocardial injection
Unlike intravascular infusion, direct intramyocardial injection targets specific regions of myocardium without relying on the upregulation of inflammatory signals to assist transvascular cell migration and tissue invasion. Non-cardiac entrapment of the transplanted cells may also be reduced. This delivery approach appears suited to chronic myocardial disease, such as chronic ischemia or scarred myocardium from old infarction, and also to the administration of MSCs and SkMs. Non-ischemic CMP may be another possible niche. While the safety of direct injection in recent MI awaits clinical evaluation, complications such as myocardial perforation have not been reported in animal studies (Amado et al. 2005; Freyman et al. 2006).
Direct injection can be achieved (1) transepicardially during open chest surgery or via the coronary venous system or (2) transendocardially by percutaneous catheter-based techniques. Although these two injection strategies are likely comparable in their ability to disperse cells throughout the myocardial wall, relative comparisons have been limited and the long-term safety of direct cell injection requires evaluation (Gavira et al. 2006).
Transepicardial injection has been the commonest route used in animal studies, where surgical exposure of the heart provides direct visualization for localizing injection sites and then tagging them for later histological analysis. Its invasiveness has restricted its clinical use to patients undergoing sternotomy for other cardiac surgery, such as in the early trials of autologous skeletal myoblast and bone marrow therapy in patients having concurrent coronary artery bypass surgery (Menasche et al. 2001b; Stamm et al. 2003).
The less invasive alternative for direct cell injection is percutaneous, catheter-based delivery. A variety of systems are now in use, sharing a multi-component catheter design that consists of a core needle for cell delivery and a support catheter for directing the needle to the target sites for injection. The catheter is passed retrogradely across the aortic valve into the left ventricle, where intramyocardial injection takes place transendocardially. Adjunctive imaging is usually coupled to the catheter system to help select target sites for injection along the walls of the left ventricle. One such imaging modality is electromechanical mapping (NOGA™, Biologics Delivery Systems) which has been incorporated into the Myostar™ delivery system [Biologics Delivery Systems, Diamond Bar, CA, U.S.A.]. Electromechanical mapping is used to create a color-coded map capable of characterizing areas of myocardium into normal, ischemic but viable or scarred and non-viable. It has been validated against non-invasive imaging techniques, such as echocardiography, PET, SPECT and MRI and enables the identification of myocardial segments that are suitable for cell therapy, usually those that are poorly contractile but still viable (Kornowski et al. 1998; Botker et al. 2001; Keck et al. 2002; Perin et al. 2002). Electromechanical mapping has now been used in preclinical and clinical studies of gene and cell therapy and has been especially useful in chronic ischemic cardiomyopathy (Vale et al. 2000; Perin et al. 2003; Tse et al. 2003; Fuchs et al. 2003; Perin et al. 2004; Sherman et al. 2006; Tse et al. 2006). Serial mapping has been performed to demonstrate improvements in local contractility of hibernating myocardium following BMC transplantation (Perin et al. 2003). Other imaging modalities that have been used to guide catheter-based endomyocardial injection include conventional x-ray fluoroscopy and real-time magnetic resonance imaging (Lederman et al. 2002; Dick et al. 2003; Barbash et al. 2004; Corti et al. 2005). MRI is also capable of serial assessment of cardiac dimension and function, and advances are being made to enable its use for tracking the in vivo fate of stem cells that have been pre-labeled with ferromagnetic molecules (e.g. iron fluorophores).
Another emerging strategy for direct delivery is transcoronary venous injection. Cells can be infused retrogradely into the coronary veins during balloon occlusion (Hou et al. 2005), or directly injected into the myocardium, transepicardially from a catheter placed inside a coronary vein (Thompson et al. 2003). The latter has been achieved using the TransAccess Delivery System™ (Medtronic Vascular, Santa Rosa, CA, U.S.A.) which incorporates an intravascular ultrasound probe to locate structures. This system was trialed in a study of BMC injection in normal swine and a pilot study of SkM therapy in patients with ischemic cardiomyopathy (Thompson et al. 2003; Siminiak et al. 2005). This system may provide more direct access to the myocardium than coronary artery infusion, particularly in the presence of occlusive coronary artery disease. Compared to transendocardial systems, transvenous injection needles probably have superior stability due to their parallel plane of approach to the myocardium, which allows them to deposit cells more deeply into the myocardium than is possible with the perpendicular plane of transendocardial injection (Thompson et al. 2003). Hence the needle tip is less likely to be dislodged by cardiac movement and by high pressure injections. The main limitation of transvenous injection relates to potentially difficult engagement in tortuous and distal coronary veins, although newer generation catheters have greater flexibility to reduce this problem.
Determining the optimal delivery technique
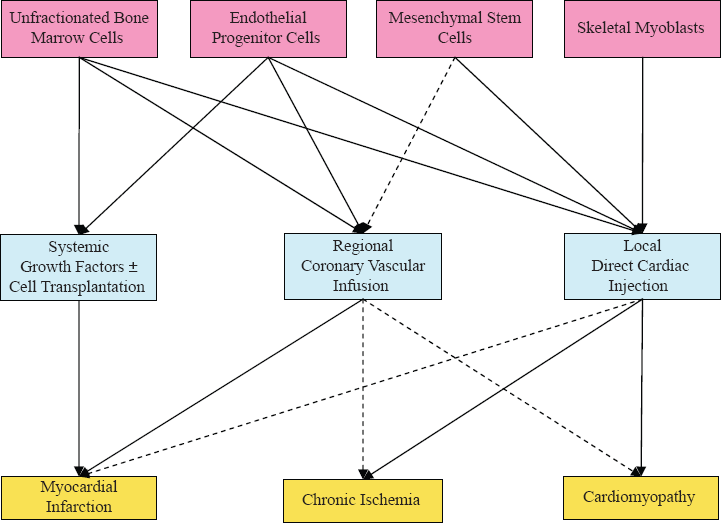
The choice of delivery route is largely dependent on both the disease process requiring treatment and the type of cell to be transplanted (Fig. 1). Myocardial retention of cells is currently disappointing with both vascular and direct routes of administration, although some cell types (e.g. EPCs) may be more effectively retained than others (e.g. BMMNCs) (Wollert and Drexler, 2006). It remains difficult to establish which delivery system will fulfill most of the intended need as studies comparing the different systems are presently lacking. In a porcine study of MI-reperfusion, radionuclide-labeled PB-derived MNCs were delivered by three different routes six days after induction of disease (Hou et al. 2005). Intramyocardial injection outperformed intracoronary and retrograde coronary venous infusion in terms of myocardial retention (11%, 2.6% and 3.2% respectively) and pulmonary entrapment (26%, 47%, 43% respectively) of cells, one hour after treatment. However, this was partly offset by inconsistency in efficacy following treatment by direct injection. A separate study investigated MSC transplantation in the early stages of MI by intracoronary infusion, peripheral venous infusion and transendocardial injection (Freyman et al. 2006). While intracoronary administration achieved the highest levels of cell engraftment two weeks after treatment, it was also associated with high rates of coronary flow obstruction during MSC delivery and a considerable incidence of pulmonary entrapment of cells, compared to direct myocardial injection. Further comparative studies are required in the future, as delivery techniques evolve and become more sophisticated.
Tailoring Cell Type to Delivery Technique and Disease Process.
Clinical Trial Experience
The first clinical trials of cell-based therapy in cardiac disease were published in 2001. Since then, the majority of trials have been phase I/II safety and feasibility studies utilizing either skeletal muscle cells or cells from bone marrow or blood in patients with MI, chronic coronary ischemia or cardiomyopathy.
Myocardial Infarction
Cell therapy aims to attenuate infarct size and prevent significant left ventricular remodeling after MI through the replacement of “lost” cardiomyo-cytes and by protecting vulnerable cardiomyocytes in peri-infarct tissue. Much of this latter effect may be mediated by improving local tissue perfusion through neovascularization.
Numerous groups have investigated the safety and feasibility of intracoronary cell infusion, 4-7 days after initial primary percutaneous revascular-ization for MI (Assmus et al. 2002; Janssens et al. 2006). Most commonly, the pragmatic strategies of using autologous unfractionated BMCs or peripheral blood cells (PBCs) have been adopted, avoiding the need for time-consuming ex vivo preparation of cells prior to treatment. A few groups have trialed more selective cell populations, including CD34+ EPCs and plastic-adhered, ex-vivo expanded MSCs.
Unfractionated bone marrow and blood-derived cells
Early studies demonstrated the safety and feasibility of intracoronary delivery of BMCs after MI (Strauer et al. 2002; Assmus et al. 2002; Britten et al. 2003; Fernandez-Aviles et al. 2004). Major complications, such as aggravated myocardial ischemia or systemic inflammatory reaction were not observed in the short-term, nor were longer-term problems such as arrhythmia, intramyocardial calcification, tumor formation or coronary reste-nosis. Although not primarily designed to assess the effectiveness of BMC transplantation, there were some indications that treatment enhanced regional wall motion in the area of infarct and global left ventricular ejection fraction (LVEF). Of these initial studies, TOPCARE-AMI compared BMCs with PBCs (Assmus et al. 2002; Schachinger et al. 2004). LVEF improved in both groups by 8%-9% from baseline to follow-up at four months and one year.
Randomized clinical trials of BM therapy in acute MI are summarized in Table 1. In the BOOST trial, 60 patients were randomized after successful primary intervention, to either coronary infusion of BMMNCs or non-placebo control (Wollert et al. 2004). Recipients of cell therapy had a 6.7% improvement in LVEF, as determined by MRI, from post-MI baseline, compared to a 0.7% increase in controls. This improvement occurred in the context of full conventional medication therapy and notably was superior to the 3°/o—1°% improvements in LVEF attributed to primary percutaneous reperfusion in the ADMIRAL and CADILLAC trials. Cell therapy did not result in significant reductions in infarct size and left ventricular end-diastolic volume. By 18 months of follow-up, mean LVEF had caught up in the control group, indicating that BMMNC treatment had probably accelerated the recovery of cardiac function post-MI, that otherwise occurred more gradually with conventional treatment (Meyer et al. 2006).
Key randomized clinical trials using intracoronary infusion of autologous bone marrow (BM) cells after myocardial infarction (MI).

In a study of similar size to the BOOST Trial, benefits of BMC therapy were restricted to infarct size, regional wall contractility and oxidative metabolism of severely infarcted territories (Janssens et al. 2006). Differences were not seen in follow-up LVEF or left ventricular volumes between recipients of cell therapy and placebo control. This may have been due to patients in this trial receiving earlier primary reperfusion after MI (3.7-4.1 hours compared to 8-9.8 hours in BOOST). Ejection fractions were well preserved at the time of enrolment (mean of approximately 50%) and such patients had less scope for additional benefit from adjuvant post-MI therapy than patients with more severe cardiac compromise.
The ASTAMI trial recruited patients with large anterior MI and reduced LVEF (mean 42%) (Lunde et al. 2006). One hundred patients were randomized to either BMC treatment given about 6 days after MI, or non-placebo control. Cell therapy neither improved LVEF nor reduced left ventricular end-diastolic volume at six months, compared to the control group. In contrast the larger-sized REPAIR-AMI trial reported positive results with BMMNC therapy resulting in more LVEF improvement than placebo (5.5% vs 3%), especially in individuals with lower baseline LVEF (<49%) and in those who received cell therapy at least five days afer MI (Schachinger et al. 2006a; Schachinger et al. 2006b). This trial was also the first to demonstrate clinical endpoint improvements, with cell therapy resulting in lower composite incidence of major cardiac events and mortality at twelve months, in patients already receiving optimal conventional treatment (Schachinger et al. 2006b).
The inconsistent results from trials of autologous BMC therapy reflect inherent problems with this treatment strategy. In the first instance, cardiac retention of BMCs is only modest (<3%) after coronary delivery and may be higher and more extensive with transfer of selected cell populations, such as EPCs (Hofmann et al. 2005). In addition unfractionated BM preparations contain a low frequency of truly multipotent endothelial and mesenchymal progenitors and this limitation is accentuated in elderly patients and in those suffering from significant illness and cardiovascular risk factors. It is unclear whether the large number of mature inflammatory cells accompanying BM infusion has a positive or deleterious effect on MI healing. Although the relationship between progenitor cell content (dose) and efficacy of therapy is not clearly defined, it is notable that compared to the negative ASTAMI trial, patients in the REPAIR-AMI study received 3-3.5-fold higher content of BMMNCs and CD34+ cells. This is despite the use of identical volumes of BM aspirate (50 mL) between the trials and reflects the observation that differences in the technique for BM collection and preparation may have a profound effect on the ultimate stem cell recovery (Seeger et al. 2007).
Selected Cell Populations
Fewer published trials have selectively used EPCs or MSCs for post-MI therapy (Chen et al. 2004; Bartunek et al. 2005; Boyle et al. 2005; Katritsis et al. 2005). CD34+ and CD133+ EPCs have been shown to possess a superior capacity for myocar-dial homing and retention after intracoronary infusion than unfractionated BMMNCs (Hofmann et al. 2005). However, the cardiac reparative potential of these cells may be negatively influenced by adverse cardiac risk factors, such as smoking and diabetes, that compromise their clonogenic and differentiation potency (Numaguchi et al. 2006; Wojakowski et al. 2007).
In a control-matched study of 35 patients, autologous CD133+ EPCs were obtained from high volume (>300 mL) BM aspirates and transplanted without ex vivo expansion, almost 12 days after MI (Bartunek et al. 2005). Treatment resulted in improvements in myocardial function, perfusion and viability, but was associated with higher rates of coronary in-stent reocclusion and restenosis.
Autologous MSC therapy has been applied post-MI in two published clinical trials, although the time required for in vitro preparation of these cells is obviously an obstacle to early infusion (Chen et al. 2004; Katritsis et al. 2005). This limitation will be overcome if clinical safety and efficacy can be shown for allogeneic MSC transplantation.
Chen et al. infused very high doses of autologous MSCs (48-60 × 109 cells) by coronary route 18 days after primary intervention for MI (Chen et al. 2004). Six month follow-up results were favorable with a marked absolute increase in mean LVEF from 49% to 67% in the MSC group, compared to 53% in the placebo group. Unfortunately detailed analysis of safety outcomes was not provided, despite the concerns that have arisen from preclinical studies showing complications from coronary infusion of this cell type. The study also failed to describe how such high numbers of MSCs were achieved in the relatively short period of time used to expand this population ex vivo.
It is noteworthy that in this study, the improvements from MSC treatment occurred in spite of the 2-3 week delay before cell delivery. Most other experience, particularly with unfractionated BMC therapy, has indicated that cell delivery is most effective between 4 and 7 days after MI (Janssens et al. 2006; Schachinger et al. 2006a; Hu et al. 2007b). Earlier infusion of cells may cause excessive obstruction and dysfunction of the microvascular bed, while longer delays to therapy allow more cardiomyocytes to be lost through apoptosis and a greater time for scar development. Delayed intra-coronary administration of a low-dose preparation of BM-derived MSCs and EPCs failed to achieve significant myocardial benefit in a small study of “old” anteroseptal MI (Katritsis et al. 2005). The ideal therapeutic window for cell delivery after MI may indeed differ between the various cell therapies currently available and remains an important issue requiring further clinical evaluation.
Growth Factor Therapy
The use of G-CSF therapy for acute and chronic ischemic syndromes, with or without accompanying coronary infusion of PBCs, is discussed in detail elsewhere (Kovacic et al. 2007). An early study from Kang et al. enrolled 27 patients who presented with MI too late for primary PCI. In this study patients only received coronary reperfusion, with bare metal stenting, once G-CSF therapy had been given for four days. Recipients of both G-CSF therapy and PBC infusion, but not G-CSF alone, exhibited improvements in exercise capacity, myocardial perfusion and systolic function after six months (Kang et al. 2004). However, both groups receiving G-CSF had unexpectedly high rates of in-stent coronary restenosis at culprit lesion site, causing the trial to be terminated early. G-CSF therapy was also associated with adverse coronary outcome in a study of chronic ischemia, where acute thrombus formation and MI were observed (Hill et al. 2005).
More recently, The MAGIC Cell-3-DES trial demonstrated a 5% absolute improvement in LVEF, six months after G-CSF mobilization and intracoronary delivery of PBCs in patients with recent MI (Kang et al. 2006). The lack of treatment response in a second group of patients with older MI, indicates that this therapy has pro-vasculogenic effects that are no longer beneficial once myocardial scarring is established. Patients in this study received drug-eluting stents and had no increase in restenosis as a complication of G-CSF.
Chronic Coronary Ischemia
The pro-angiogenic potential of BM-derived cells has led to their evaluation in several small-scale trials of patients suffering from refractory angina with no option for coronary revascularization. The goal of therapy in this scenario is to achieve improvement in myocardial perfusion and angina symptoms. Where myocardial hibernation has occurred with resultant cardiac dysfunction, cell-derived neovascularization may also provide restoration of regional and global contractility.
In chronic coronary ischemia, there is thought to be a lack of the necessary local and systemic homing signals needed to entice cells to the myocardium from the vascular route. Consequently, direct myocardial injection of cells has typically been favored over intracoronary administration, especially in patients with occlusive, diffuse coronary disease not amenable to revascularization.
In a non-randomized trial of ischemic patients with marked reduction of LVEF (mean 20%), NOGA-guided transendocardial delivery of BMMNCs was performed safely and resulted in substantial improvements in reversible perfusion defects, regional and global myocardial function, including a 9% improvement in mean LVEF after four months (Perin et al. 2003). Clinical angina scores and physiological parameters of myocardial performance on exercise testing also improved. Symptomatic benefits were sustained at twelve months, as was myocardial perfusion; however, the improvements in ejection fraction were no longer significant (Perin et al. 2004). In a smaller cohort of heart transplant candidates, cell therapy increased myocardial oxygen consumption to such an extent, that four out of five patients no longer were eligible for transplantation (Silva et al. 2004). Arrhythmias were not observed as an adverse outcome in these trials, nor were there histological changes associated with abnormal cell growth or tissue lesions (Dohmann et al. 2005).
Comparable observations have been observed in similarly designed trials performed by other groups (Beeres et al. 2006; Fuchs et al. 2006). The non-randomized nature of these trials prohibits firm conclusions to be made about the efficacy of BMMNC injection in these patients. One important observation has been the great diversity in the functional properties of BMCs taken from different patients (Fuchs et al. 2006). This is a well-known phenomenon that emphasizes the limitations of autologous BMC therapy, especially in elderly patients and those with severe, chronic illness (Heeschen et al. 2004).
Recent trials of PBCs in chronic coronary disease have also demonstrated promise even when these cells were administered by coronary infusion (Ozbaran et al. 2004; Erbs et al. 2005; Boyle et al. 2006). Therapy with G-CSF-mobilized circulating progenitor cells enhanced coronary flow reserve, reduced infarct size and improved myocardial hibernation, in patients who had received recanalization of chronic total occlusions ten days earlier (Erbs et al. 2005). Mean LVEF increased from 51.7% to 58.9%, largely due to augmented wall contractility in the target region. These benefits may have been mediated by a combination of neovascularization, improved coronary endothelial function, paracrine stimulation of endogenous cardiac stem cells and digestion of scar tissue by the release of proteases from the transplanted cells.
Post-MI cardiomyopathy
Patients with cardiac dysfunction who have late stage heart failure, represent a challenging group for clinicians. The limited donor supply of cadaveric hearts for transplantation has left a substantial need for the development of novel treatments that are capable of replacing the cardiac cell mass that is lost during ventricular remodeling. The replacement of non-viable, scarred myocardium with functional, contractile heart tissue is a difficult objective especially as current adult cell therapies appear to be limited by poor engraftment after transplantation and inadequate regeneration of the damaged cellular components. Nevertheless, results from preliminary clinical trials have provided some evidence for cardiac repair from transplantation of SkMs or BM-derived cells in these patients. As discussed below, these small studies have been dogged by inconsistent results, making it difficult to confidently draw conclusions regarding the efficacy of these different cell types in post-MI cardiomyopathy.
Skeletal Muscle Cells
Skeletal myoblasts are attractive for repair of scarred myocardium because of their resistance to ischemia and fatigue and their contractile properties. Positive preclinical experience has been translated to the bedside by applying these myogenic precursors to patients with chronic cardiac dysfunction associated with ischemia and non-viable scar (Menasche et al. 2001a; Menasche, 2002; Pagani et al. 2003; Siminiak et al. 2004; Dib et al. 2005; Hagege et al. 2006). In these studies, SkMs were delivered either by direct transepicardial injection, via sternotomy or the coronary venous route, or by percutaneous transendocardial injection (Smits et al. 2003). Initial results from non-randomized studies indicated promising augmentation of contractile function, although a common confounder was the presence of concurrent bypass surgery (Menasche et al. 2003; Smits et al. 2003; Herreros et al. 2003; Steendijk et al. 2006). Mechanistically, it has been shown that although engrafted myoblasts do not adopt a cardiac phenotype, they do retain their contractile properties in vivo and may upregulate their expression of slow-twitch myofibers, which potentially imparts fatigue resistance (Pagani et al. 2003; Hagege et al. 2003). A possible safety issue related to the use of SkM's is arrhythmogenesis, as highlighted by the variable incidence of sustained ventricular tachycardia after therapy (Smits et al. 2003; Herreros et al. 2003). Causative mechanisms for this adverse outcome include the use of non-human serum during myoblast culture (Chachques et al. 2004), failure of myoblasts to electrically couple with host cardiomyocytes, resulting in inhomogeneities in action potential conduction, and the possible creation of re-entry pathways by injection-related disruption of myocardial anatomy.
The MAGIC trial (presented at American Heart Association 2006 Scientific Sessions, Chicago, Illinois) intended to recruit 300 patients with ischemic cardiomyopathy to assess the safety and efficacy of two doses of autologous skeletal myoblasts, as compared to placebo. The study was terminated after enrolment of 97 patients because of slow recruitment and concerns about the study's ability to meet efficacy endpoints. The preliminary results indicated no difference among the three groups regarding major adverse events and ventricular arrhythmias, providing reassurance about the safety of intramyocardial myoblast injection. Primary efficacy endpoints pertaining to improvement in cardiac contraction were not met, although cautious optimism was drawn from secondary endpoint analysis which demonstrated reduction in left ventricular end-diastolic and end-systolic volumes with high dose cell therapy but not placebo.
Bone marrow and blood-derived cells
Autologous CD133+ and CD34+ cells have been injected in separate small series of patients with ischemic cardiomyopathy treated by concurrent CABG (Stamm et al. 2003; Patel et al. 2005). While global LVEF was enhanced in the majority of patients, it was likely that much of this effect was due to surgical revascularization, as there was not improvement in regional contractile function of the cell-treated scars. This reinforces that these cells are unlikely to achieve myocardial repair in regions of non-viable tissue, where there is little scope for benefit from vasculogenesis.
Other studies utilizing unfractionated BMMNCs have yielded more encouraging results, possibly due to the myogenic potential of the small number of mesenchymal precursors present in these populations. The non-randomized, controlled ICAT study enrolled 36 patients with chronic MI of at least nine months duration, and administered BMMNCs via intracoronary injection (Strauer et al. 2005). At three month follow-up, cell therapy resulted in significant improvements in global LVEF, infarct size, myocardial viability and patient exercise capacity, to a much greater extent than observed in the control patients. Another randomized, controlled study of intramyocardial injection of BMMNCs demonstrated improvement in systolic thickening in cell-implanted scars but not untreated scars (Hendrikx et al. 2006). Six out of nine treated patients had inducible ventricular arrhythmia during electrophysiological testing at follow-up. While this is an isolated observation with BMMNC transplantation, it highlights the need for all clinical studies to perform rigorous safety analyses and report on longer-term adverse outcomes.
Non-ischemic cardiomyopathy
The playing field and challenges for cell-based therapy are quite different in non-ischemic cardiomyopathy, due mainly to differences in etiology, pathogenic mechanisms, and because of unique cellular and cytokine responses involved in the disease process. One example of this is a lack of upregulation of cardiac gene expression for several important stem cell homing factors in idiopathic dilated cardiomyopathy (Theiss et al. 2007). This may account for the observation that patients with non-ischemic cardiomyopathy may have higher levels of CD34+ EPCs in peripheral blood, as in the absence of cardiac homing signals these cells fail to migrate and incorporate into the myocardium to assist with endogenous repair. Preclinical data in non-ischemic cardiomyopathy has focused on small animal models of toxic (doxorubicin-induced) or genetic cardiomyopathy, with promising results demonstrated for both SkMs and BM-derived cells (Agbulut et al. 2003; Kondoh et al. 2007; Ohnishi et al. 2007). Recently, myoblast transplantation also achieved functional benefit in an ovine model of cardiomyopathy, induced by intracoronary doxorubicin (Borenstein et al. 2007).
Clinical application of cell treatment in non-ischemic cardiomyopathy has lagged behind isch-emic syndromes, although this is being addressed by trials such as the First-in-Man ABCD Trial (Seth et al. 2006) and TOPCARE-DCM. In the First-in-Man ABCD trial, 44 patients with dilated non-ischemic cardiomyopathy (LVEF ≤ 35%) were randomized to either non-placebo control or intra-coronary administration of unfractionated BMMNCs. Six month results included improvement in the functional class of heart failure and in mean LVEF by 5.4% (20 to 25%) in the treatment group, which was not observed in the control patients. Mechanistic uncertainty remains however, as endomyocardial biopsy specimens did not have evidence for persistence of the injected cells, presence of new immature cardiomyocytes, or increased inflammation, infarction or neovascularization.
Conclusion
The field of cardiovascular cell-based therapy has undergone remarkable growth over the last decade. On the basis of exciting preclinical discoveries, extension to clinical trials has been rapid. Unfortunately many questions still remain unanswered—questions that must be addressed if clinical application of cell transplantation is to become widely accepted and safely practiced. To date the great majority of clinical studies have involved the transfer of autologous unfractionated BMCs to the heart. While strengths of this strategy lie in its relative simplicity and therefore its scope for wide practice, it should be noted that it represents a “blanket” approach to cell therapy that does not enrich for the critical stem cell components of the bone marrow. A crucial step for future studies is to determine which cell product(s) are most efficacious and safe at achieving myocardial repair in different patient groups. Follow-on questions such as optimal cell dose, method of delivery and timing of delivery also need resolution.
Much is still to be determined about stem cell biology and the mechanisms by which cardiac repair can be achieved and new strategies will no doubt seek to maximize the ability of cells to engraft, survive and function in vivo. By necessity there is still ground to cover through basic scientific and animal-based experiments. However, there is a considerable amount to be learned from well-conducted, randomized clinical studies, in which appropriate subject groups and meaningful endpoints are chosen. Efficacy of cell transplantation must be demonstrated by improvement in clinical endpoints, in patients who are “at-need” for adjuvant therapy because of refractoriness to conventional treatment. These endpoints should include assessment of quality of life, readmission rates, adverse cardiac events and mortality. In addition, the long-term safety profiles of different cell types also need to be clarified for specific disease cohorts. The performance and results of such carefully designed future studies will determine what role cell-based therapy may play in the future clinical management of patients with cardiovascular disease.