
Abstract
Cardiovascular diseases remain the leading cause of global mortality, necessitating precise strategies for diagnosing and managing myocardial injury. This review critically synthesizes the current biomarker landscape and proposes an integrative framework to address the significant translational gaps between biomarker science and clinical practice. We conducted a comprehensive critical review, analyzing established and emerging biomarkers, including cardiac troponins, natriuretic peptides, and inflammatory and fibrotic markers, within the context of biological confounders, etiology-specific challenges, and clinical implementation barriers. Through thematic synthesis, we developed the novel C.A.L.I.B.R.A.T.E. framework to structure biomarker integration. While high-sensitivity assays have improved detection, they reveal chronic elevations in conditions like renal dysfunction, aging, and heart failure, reducing specificity and complicating acute diagnosis. Emerging biomarkers (eg, sST2, galectin-3) offer prognostic insight but lack therapeutic guidance and specificity. Etiology-specific puzzles (eg, myocarditis, COVID-19, MINOCA) highlight the limitations of isolated biomarker interpretation. The C.A.L.I.B.R.A.T.E. framework addresses these gaps by integrating Clinical context, Assay characteristics, Likelihood, Injury mechanism, Biomarker profiles, Rule-out/in thresholds, Adjunctive tests, Time kinetics, and Etiologies & comorbidities. The future of myocardial injury management depends on shifting from isolated biomarker measurement to integrated, algorithm-driven interpretation. The C.A.L.I.B.R.A.T.E. framework provides a structured pathway for personalized diagnostic reasoning, bridging the translational chasm and advancing precision cardiology through context-dependent, multi-modal data synthesis.
Plain Language Summary
Diagnosing heart injury using blood tests is complex because factors like age, kidney disease, and other illnesses can skew the results. This review shows that using single tests is often misleading. Instead, doctors should combine multiple test results, imaging scans, and the patient’s full medical story to make an accurate diagnosis. We introduce a new practical guide—the C.A.L.I.B.R.A.T.E. approach—to help clinicians integrate all this information, leading to more precise, personalized, and effective care for patients with heart injury.
Current management of myocardial injury relies on isolated biomarkers (eg, troponins, natriuretic peptides), but their interpretation is confounded by age, kidney function, and comorbidities, leading to diagnostic uncertainty. This review critiques these limitations and the poor specificity of emerging inflammatory/fibrotic markers. It argues that precision requires integrating multi-modal data—biomarkers, imaging, clinical context—rather than seeking new biomarkers alone. We propose the C.A.L.I.B.R.A.T.E. framework, a structured clinical reasoning tool that synthesizes Clinical context, Assay details, Likelihood, Injury mechanism, Biomarker profiles, Rule-out/in thresholds, Adjunctive tests, Time kinetics, and Etiologies & comorbidities to bridge the gap between biomarker science and personalized patient care.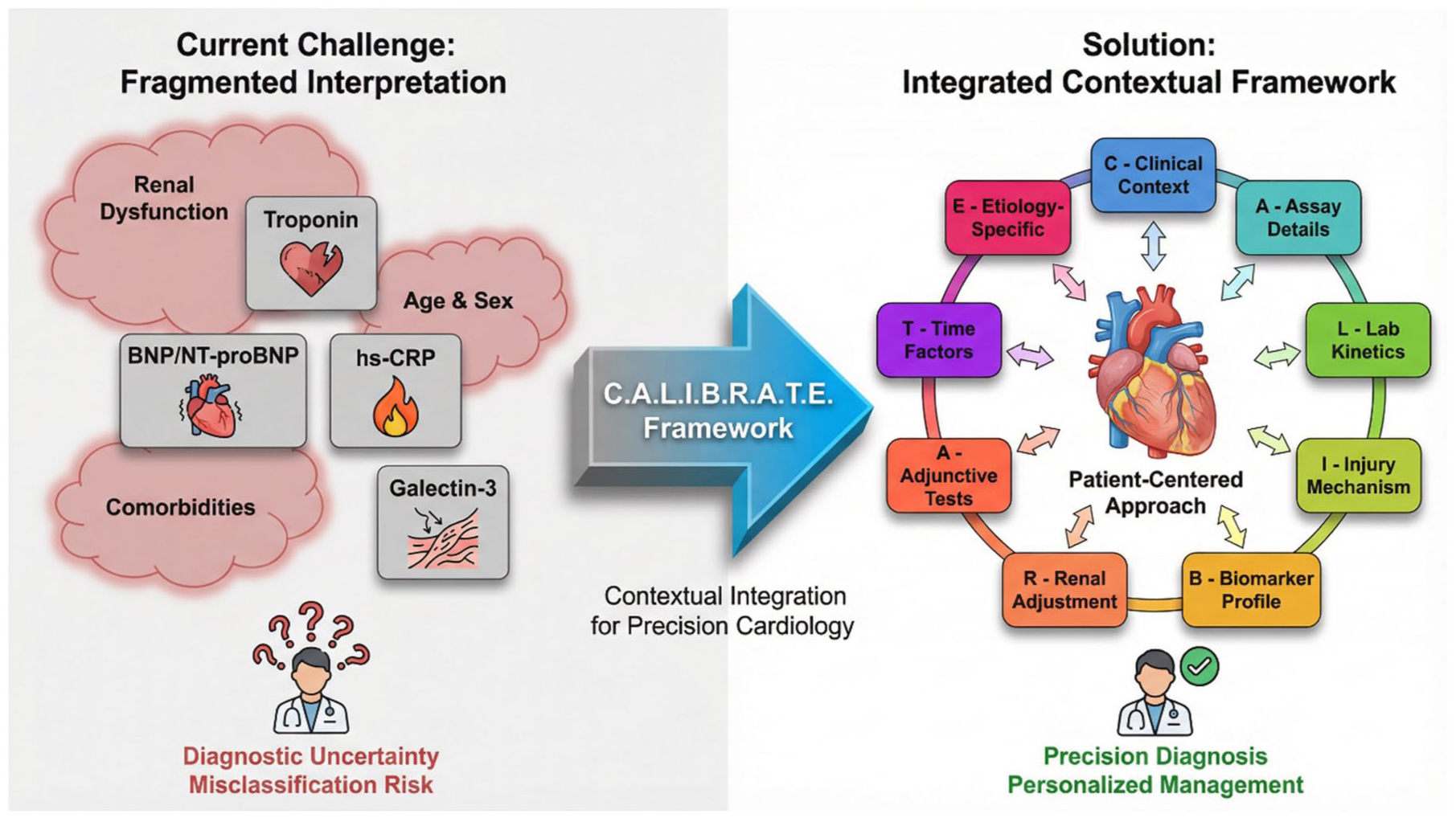
Keywords
Introduction
Cardiovascular diseases (CVDs) remain the leading cause of global mortality, a burden sustained despite transformative advancements in diagnostic technology. 1 At the core of acute coronary syndromes, heart failure, and myocarditis lies myocardial injury—a final common pathway of cardiomyocyte damage arising from ischemia, inflammation, or toxic insult. The Fourth Universal Definition of Myocardial Infarction enshrines cardiac troponins (cTnI/cTnT) as the biochemical gold standard for detecting necrosis, a classification that has streamlined diagnostic criteria globally. 2 Concurrently, the prognostic utility of natriuretic peptides (BNP/NT-proBNP) in heart failure and of inflammatory markers like high-sensitivity C-reactive protein (hs-CRP) is unequivocally established.3 -6 The advent of high-sensitivity assays has further refined our temporal resolution of injury, enabling the detection of subclinical damage and accelerating rule-out protocols.7,8
Yet, this proliferation of biomarkers and enhanced analytical sensitivity has precipitated a new set of clinical and interpretative complexities, revealing a significant translational gap between biomarker measurement and personalized therapeutic action. The current paradigm often treats biomarkers as isolated diagnostic silos—troponin for necrosis, BNP for volume stress, CRP for inflammation—rather than as interconnected components of a pathophysiological narrative. This fragmented approach falters in the face of real-world patient heterogeneity. For instance, the very sensitivity that makes high-sensitivity troponin (hs-cTn) a powerful tool also unveils chronic, low-grade elevations in patients with renal dysfunction, heart failure, or advanced age, blurring the line between acute injury and chronic disease states and challenging the specificity of a “positive” result.7 -9 Similarly, while novel biomarkers like galectin-3 and soluble ST2 offer insights into fibrotic remodeling, their independent prognostic value and optimal point of integration into existing heart failure management algorithms remain contentious.10 -13
This review posits that the next frontier in precision cardiology is not the discovery of novel biomarkers per se, but the development of contextual, integrative frameworks for their application. True precision requires moving beyond a reactive, biomarker-led diagnosis to a proactive, phenotype-informed biomarker interpretation. This necessitates a critical reckoning with fundamental confounders—renal function, age, sex, and comorbid conditions—that biologically modulate biomarker levels and can lead to diagnostic misclassification. 1 It demands a rigorous assessment of the economic and practical barriers to implementing multi-marker strategies in diverse healthcare settings. Furthermore, it calls for a synthesis of biomarker data with advanced multimodal imaging and clinical scoring systems to construct a coherent patient-specific narrative.14 -21
Here, we provide a critical synthesis of the current biomarker landscape for myocardial injury. We will not merely catalog established and emerging markers but will interrogate the evidence for their utility, expose the controversies and limitations that temper their clinical application, and analyze the persistent gap between their theoretical potential and real-world implementation. We will critically evaluate the mechanistic pathways of injury—from ionic dysregulation and oxidative stress to infection and genetic predisposition—to elucidate why biomarker profiles differ across etiologies.22 -41
Finally, we propose a novel integrative framework—the C.A.L.I.B.R.A.T.E. approach—designed to bridge the translational gap. Unlike existing guideline-based algorithms that provide diagnostic cut-offs or risk scores, the C.A.L.I.B.R.A.T.E. framework functions as a cognitive reasoning tool, structuring how clinicians synthesize multi-modal data—including biomarker profiles, imaging findings, and patient-specific confounders—to arrive at a personalized, mechanism-informed diagnosis. By shifting from isolated biomarker measurement to integrated, algorithm-driven interpretation, this framework aims to advance precision cardiology through context-dependent, multi-modal data synthesis.
Methodology
This review employed a systematic, multi-stage strategy for evidence identification and critical appraisal, designed to facilitate analytical synthesis rather than quantitative meta-analysis. The methodological approach prioritized thematic integration and critical evaluation of conflicting evidence to identify persistent knowledge gaps and interrogate the translational challenges inherent in applying myocardial injury biomarkers within precision medicine frameworks.
Literature Search Strategy and Source Identification
A comprehensive literature search was conducted across PubMed/MEDLINE, EMBASE, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials without initial date restrictions to capture foundational studies. The search combined Medical Subject Headings (MeSH) and free-text keywords spanning 4 conceptual domains: (1) Biomarker Domain (eg, “cardiac troponin,” “natriuretic peptide,” “galectin-3”); (2) Pathology Domain (eg, “myocardial infarction,” “heart failure,” “myocarditis”); (3) Mechanism Domain (eg, “oxidative stress,” “calcium overload”); and (4) Application Domain (eg, “diagnostic accuracy,” “high-sensitivity assay”). Primary emphasis was placed on literature from 2000 to 2025, particularly for advancements in high-sensitivity assays and novel biomarkers. The search was supplemented by hand-searching reference lists of key reviews and consulting current clinical practice guidelines from the ESC, ACC/AHA, and WHF.
Study Selection and Inclusion/Exclusion Criteria
Studies were selected based on relevance to myocardial injury biomarkers and their clinical application. Inclusion criteria encompassed: original research (basic, translational, observational cohorts, and randomized controlled trials), systematic reviews, meta-analyses, and authoritative guidelines. Human studies and relevant preclinical mechanistic studies were included. Outcomes of interest included diagnostic accuracy, prognostic value, correlation with imaging or histology, impact on clinical decision-making, and exploration of novel biomarkers. Studies were excluded if they were duplicate publications, abstracts without peer-reviewed full texts, or focused exclusively on non-cardiac biomarkers without clear correlation to myocardial injury. The selection process involved independent screening by at least 2 reviewers, with disagreements resolved through consensus.
Data Extraction and Thematic Synthesis
A standardized data extraction form captured study characteristics, biomarker details (assay method, timing), mechanistic insights, and data on clinical utility and confounding factors. Given the heterogeneity of the topic, a narrative synthesis approach was employed to enable contextual and critical analysis. The synthesis involved: (i) logical grouping and critical comparison of evidence by biomarker class, injury mechanism, and clinical context; (ii) identification of themes, controversies, and evidence gaps—for example, contrasting studies on copeptin’s early rule-out utility 42 with those highlighting limitations in specific comorbidities 43 ; (iii) mechanistic integration of basic science findings with clinical biomarker studies; and (iv) explicit addressing of conflicting evidence through exploration of assay generation differences, population characteristics, or study design variations.
Critical Quality Assessment
The risk of bias of included studies was appraised using design-specific tools: the Newcastle-Ottawa Scale for observational studies, the Cochrane Risk of Bias Tool (RoB 2) for randomized controlled trials, and AMSTAR 2 for systematic reviews. For basic and translational studies, focus was placed on methodological rigor, biological plausibility, and reproducibility. This appraisal informed the weight given to individual studies in the narrative synthesis.
Development of the C.A.L.I.B.R.A.T.E. Framework
The C.A.L.I.B.R.A.T.E. framework emerged from the critical integration of extracted data on biomarker strengths, weaknesses, confounders, and complementary diagnostic modalities. It was not derived from any single source but represents a novel conceptual synthesis aimed at providing a structured yet flexible schema for contextual biomarker application.
Limitations
The methodological approach has inherent limitations: (i) the broad interdisciplinary scope necessitated a narrative rather than meta-analytic synthesis; (ii) the rapidly evolving field means some very recent developments may not be fully captured; (iii) publication bias may underrepresent negative studies; and (iv) the synthesis prioritized evidence with direct clinical relevance, potentially foregrounding certain topics over exploratory basic science.
The Gold Standards & Their Discontents: A Critical Appraisal of Troponins and Natriuretic Peptides
The diagnostic and prognostic assessment of myocardial injury and heart failure rests firmly on 2 pillars: cardiac troponins (cTnI and cTnT) for the detection of myocyte necrosis, and natriuretic peptides (BNP and NT-proBNP) for the identification of hemodynamic cardiac stress. Their integration into universal definitions and clinical guidelines is a testament to their transformative impact.2,3 However, the very properties that confer their “gold standard” status—exquisite sensitivity and cardiac specificity—also unveil profound complexities in interpretation. This section critically evaluates the indispensable yet fraught role of these cornerstone biomarkers, moving beyond uncritical acceptance to analyze the evidence for their limitations, contextual pitfalls, and the ongoing debates that define their modern application.
Cardiac Troponins: The Double-Edged Sword of Sensitivity
The evolution from nonspecific enzymes to cardiac-specific troponins revolutionized the diagnosis of acute myocardial infarction (AMI). High-sensitivity (hs) assays represent the apotheosis of this progress, detecting troponin concentrations an order of magnitude lower than conventional tests. This sensitivity permits earlier rule-in of AMI and, through rapid serial sampling, highly efficient rule-out protocols, fundamentally changing emergency department practice.8,44
Critical Appraisal and Controversies
The central paradox of hs-cTn lies in its revelation of chronic, subclinical myocardial injury. Elevated hs-cTn is now a common finding in populations with stable coronary artery disease, chronic heart failure (HF), renal impairment, and even advanced age, independent of an acute ischemic event.7,9 This phenomenon critically challenges the binary “positive/negative” paradigm. For instance, in a patient with stage 4 chronic kidney disease presenting with dyspnea, a baseline elevated hs-cTnT may obscure the diagnosis of an acute Type 2 MI, as the absolute change (delta) required for diagnosis is poorly defined in this population. This directly impacts the specificity of the test, converting it from a precise indicator of acute plaque rupture to a sensitive but non-specific barometer of cumulative cardiac strain and clearance dysfunction.
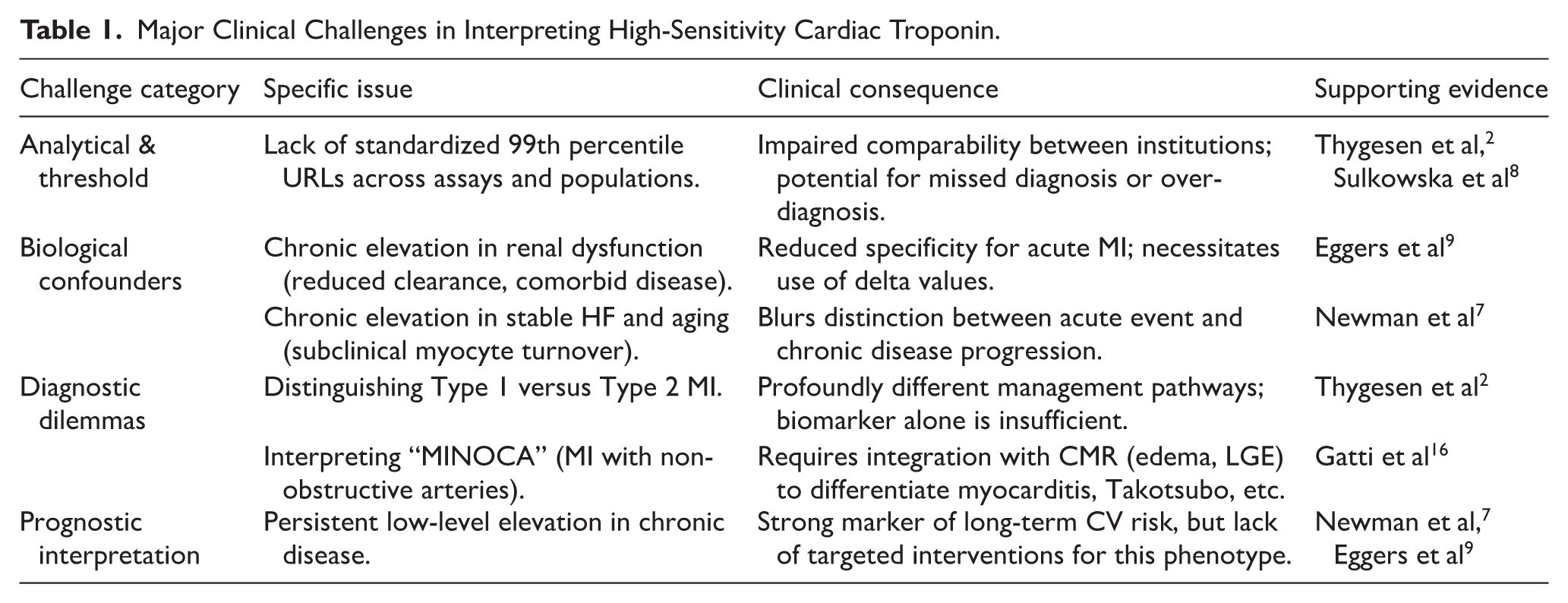
Furthermore, the Universal Definition’s classification of MI types hinges critically on troponin interpretation within a clinical context. 2 Distinguishing Type 1 MI (plaque rupture) from Type 2 MI (supply-demand mismatch) is a frequent and consequential clinical dilemma. While troponin confirms injury, it does not elucidate mechanism. A critically ill septic patient with hypoxia and tachycardia may have significant troponin elevation, meeting criteria for Type 2 MI. However, the therapeutic implication—focusing on sepsis management versus dual antiplatelet therapy and coronary angiography—diverges radically. Over-reliance on the biomarker without rigorous clinical correlation risks diagnostic misclassification and iatrogenic harm from inappropriate anticoagulation or invasive procedures. 7 The evidence underscores that troponin is a leak marker, not an etiology marker. Table 1 summarizes the principal analytical, biological, and diagnostic challenges that complicate hs-cTn interpretation in clinical practice.
Major Clinical Challenges in Interpreting High-Sensitivity Cardiac Troponin.
Natriuretic Peptides: Beyond Heart Failure Diagnosis
B-type natriuretic peptide (BNP) and its inactive N-terminal fragment (NT-proBNP) are secreted by ventricular cardiomyocytes in response to wall stress and volume overload. They are cornerstone biomarkers for diagnosing HF, discriminating cardiac from pulmonary causes of dyspnea with high accuracy, and providing powerful independent prognostic information across the spectrum of cardiovascular disease.3,45
Critical Appraisal and Controversies
Despite their utility, natriuretic peptides are subject to significant biological modulation that can confound interpretation. Obesity presents a well-documented paradox: patients with obesity-related HF often have lower than expected NP levels due to increased adipokine-mediated clearance, reduced synthesis, or receptor downregulation, potentially leading to under-diagnosis. 3 Conversely, renal impairment decreases clearance of NT-proBNP (more so than BNP), leading to disproportionately elevated levels that may overestimate the degree of cardiac stress, a critical factor in guiding diuretic therapy. 4
A major emerging application is the use of NPs to identify covert atrial fibrillation (AF) in post-stroke patients, given the association between atrial stretch and NP secretion. 4 While promising, this application highlights an interpretive gray zone: is an elevated NT-proBNP a marker of underlying hypertensive heart disease, systolic/diastolic dysfunction, or paroxysmal AF? This ambiguity limits its specificity as a standalone screening tool and necessitates confirmatory monitoring.
Furthermore, while NPs are excellent for diagnosis and prognosis, their role in guiding HF therapy has been contentious. The concept of “NP-guided therapy” aimed at titrating drugs to achieve a target NP level has yielded mixed results in clinical trials. This suggests that while NPs are robust markers of state, they may not be dynamic, responsive markers of therapeutic efficacy in all patients, underscoring the complexity of the underlying pathophysiology they reflect.
The Primacy of Cardiac-Specific Biomarkers
An essential principle underlying the interpretation of myocardial injury biomarkers—one that is frequently underappreciated in clinical practice—is the distinction between biomarkers that are truly cardiac-specific and those that are systemic markers with cardiac associations. Among the vast array of molecules proposed as cardiovascular biomarkers, only 2 families meet the stringent criterion of cardiac specificity: the cardiac natriuretic peptides (ANP, BNP, and their related peptides, including NT-proBNP) and the cardiac troponins (cTnI and cTnT). These biomarkers are either exclusively or predominantly produced by cardiomyocytes, whereas all other biomarkers discussed in this review—including hs-CRP, sST2, galectin-3, GDF-15, and copeptin—are systemic markers released from multiple tissue sources in response to various pathological stimuli. This fundamental distinction, recently emphasized in an international consensus document, 46 has profound implications for diagnostic reasoning, risk stratification, and the design of multi-marker strategies.
The clinical significance of this distinction extends beyond mere biological taxonomy. From a pathophysiological perspective, an elevated BNP or NT-proBNP concentration signals that the neuro-immuno-hormonal system has been activated in response to a pathological stressor—typically increased myocardial wall tension or volume overload—which has stimulated increased production and release of natriuretic peptides from ventricular cardiomyocytes. When a concentration of hs-cTnI or hs-cTnT above the 99th percentile upper reference limit is simultaneously detected, this indicates that the inciting stressor was sufficient to cause significant myocardial tissue damage with myocyte necrosis, thereby fulfilling the biochemical criteria for myocardial injury as defined by the Fourth Universal Definition of Myocardial Infarction. 2 The combined measurement of both cardiac-specific biomarker families therefore provides complementary and additive pathophysiological information: natriuretic peptides reflect hemodynamic stress and neurohormonal activation, while cardiac troponins directly quantify the extent of myocyte necrosis. Neither biomarker family alone can fully characterize the underlying disease state, and consensus guidelines now recommend their combined assessment in individuals suspected of cardiovascular disease. 46
The clinical importance of recognizing cardiac specificity also extends to the interpretation of novel biomarkers. Markers such as sST2, galectin-3, and GDF-15, while providing valuable prognostic information, are inherently non-specific to the heart. Their concentrations are influenced by pulmonary disease, renal dysfunction, hepatic fibrosis, systemic inflammation, and other extra-cardiac conditions. Consequently, isolated elevations in these markers cannot be attributed solely to cardiac pathology and must be interpreted within the broader clinical context and in conjunction with cardiac-specific biomarkers. Failure to appreciate this distinction risks diagnostic misattribution and inappropriate therapeutic decision-making. The C.A.L.I.B.R.A.T.E. framework explicitly addresses this challenge by requiring the integration of cardiac-specific biomarker data with clinical context and adjunctive testing before etiological conclusions are drawn.
Proposed Integrative Schematic: Contextualizing Biomarker Interpretation
The limitations of both troponins and NPs underscore that no biomarker operates in a diagnostic vacuum. Figure 1 proposes a schematic framework for integrating biomarker results with the essential clinical context. It illustrates how the pre-test probability of disease (eg, classic chest pain vs critical illness) and the presence of key confounders (renal function, age, BMI) must actively shape the interpretation of an elevated troponin or NP level, guiding the clinician toward the appropriate diagnostic pathway and avoiding mechanistic misattribution.
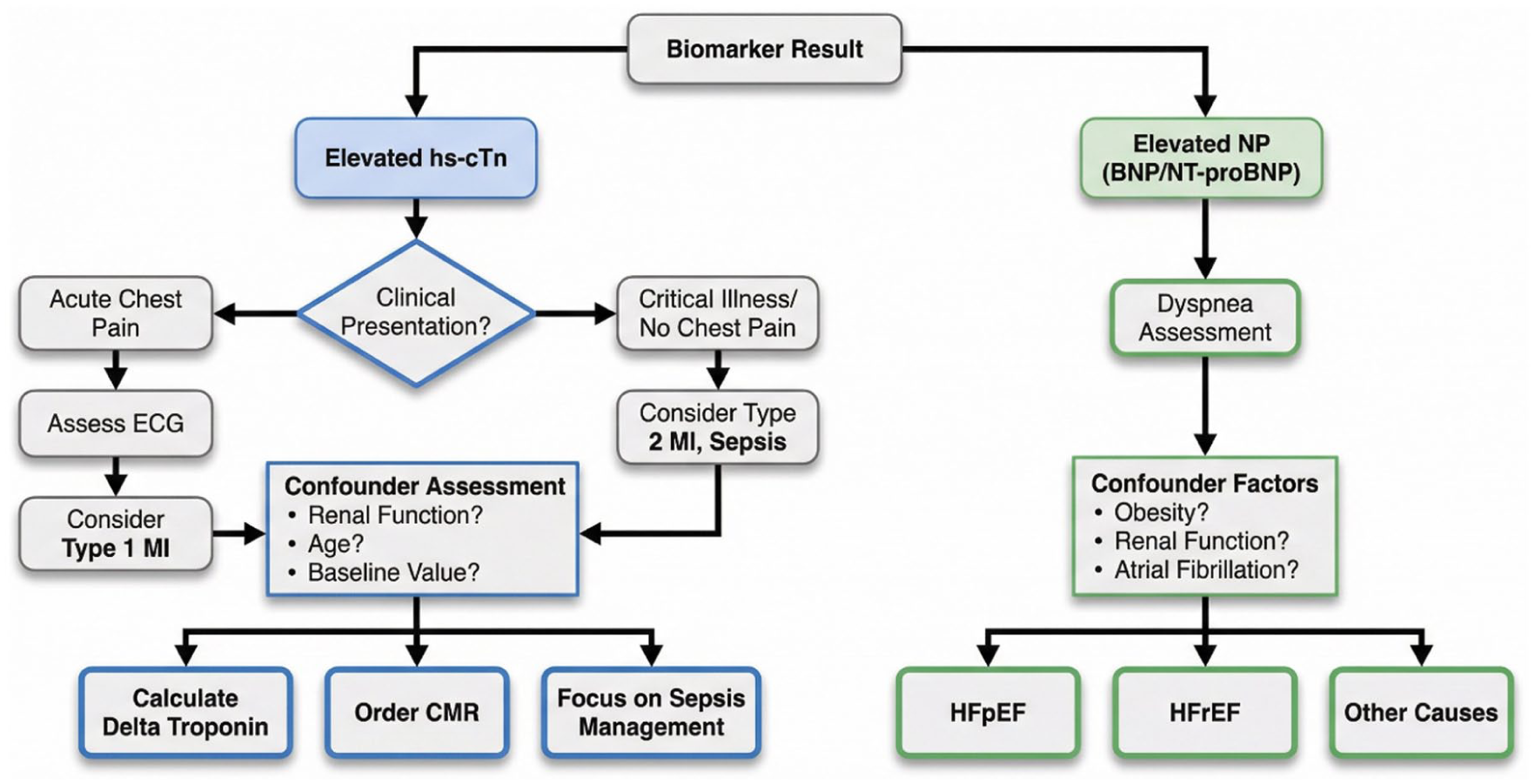
A framework for contextual interpretation of cardiac biomarkers.
Troponins and natriuretic peptides are irreplaceable tools in cardiovascular medicine. However, their advanced sensitivity has revealed a landscape of biological complexity that demands an equally sophisticated, critical, and integrative approach to interpretation. Recognizing their “discontents”—the confounders, the diagnostic ambiguities, and the gaps between biomarker elevation and therapeutic clarity—is not a repudiation of their value but a necessary evolution in their clinical application. This critical perspective forms the foundation upon which a truly precision-based approach to myocardial injury must be built, paving the way for the integration of additional biomarker and imaging modalities discussed in subsequent sections.
Beyond Necrosis: The Expanding Biomarker Universe—A Critical Appraisal of Inflammatory, Stress, and Fibrosis Markers
The diagnostic and prognostic assessment of myocardial injury has evolved from a singular focus on myocyte necrosis to a broader recognition of the contributory roles of inflammation, hemodynamic stress, and fibrotic remodeling. While troponins and natriuretic peptides address the “what” and “how much” of injury and stress, a new generation of biomarkers seeks to elucidate the “why” and “what next,” offering insights into underlying pathophysiology and long-term risk. However, the translational trajectory of these emerging biomarkers has been marked by a persistent gap between pathophysiological promise and clinical utility. Unlike troponins and natriuretic peptides—which are cardiac-specific and directly inform diagnostic and therapeutic decisions—the majority of inflammatory, stress, and fibrosis markers are systemic in origin, lack diagnostic specificity, and have failed to demonstrate that their measurement alters management or improves outcomes. This section critically evaluates these biomarkers, interrogating not only their proposed utility but, more importantly, the substantial evidence gaps, interpretative challenges, and controversies that currently limit their integration into routine precision care.
Inflammatory Mediators: Prognostic Signal or Actionable Target?
Systemic and vascular inflammation are central to the pathogenesis, progression, and destabilization of atherosclerotic disease and myocardial injury. High-sensitivity C-reactive protein (hs-CRP), an acute-phase reactant, is the most extensively studied inflammatory biomarker in cardiology. Elevated hs-CRP is a consistent, independent predictor of future cardiovascular events in both primary and secondary prevention settings, adding prognostic information beyond traditional risk factors.5,47 Myeloperoxidase (MPO), a leukocyte-derived enzyme that generates reactive oxidants, has been implicated in plaque vulnerability, endothelial dysfunction, and adverse outcomes in acute coronary syndromes.48,49
Critical Appraisal and Persistent Controversies
The primary limitation of hs-CRP is its profound lack of cardiovascular specificity. Elevated levels occur in any systemic inflammatory state—infection, autoimmune disease, trauma, or malignancy—rendering it diagnostically useless for acute cardiac events. Its role is overwhelmingly prognostic, not diagnostic. Furthermore, while epidemiologically robust, the clinical actionability of measuring hs-CRP remains contested. The JUPITER trial demonstrated that statin therapy reduced events in individuals with elevated hs-CRP but low LDL-C, suggesting a role in guiding primary prevention. 50 However, whether hs-CRP should be a routine therapeutic target beyond LDL lowering is unresolved. The CANTOS trial, which demonstrated that IL-1β inhibition with canakinumab reduced cardiovascular events, provided proof-of-principle that targeting inflammation improves outcomes. 51 Yet, the modest absolute benefit, high cost, and increased infection risk have precluded widespread adoption. Thus, hs-CRP remains a risk marker rather than a modifiable therapeutic target in routine practice.
MPO faces even greater barriers to clinical implementation. Beyond its non-specificity, MPO assays lack standardization across platforms, and no therapy has been shown to lower MPO levels with consequent improvement in hard clinical endpoints. The critical question for both hs-CRP and MPO is whether they represent modifiable risk pathways or merely epiphenomena of underlying disease. Emerging evidence from network pharmacology approaches suggests that inflammatory pathways are highly interconnected with oxidative stress, mitochondrial dysfunction, and cell death signaling in reperfusion injury. 52 Such systems-level analyses reveal that single-biomarker targeting may be insufficient; rather, multi-target therapeutic strategies—potentially guided by multi-marker panels—may be required to meaningfully modulate inflammation-driven myocardial injury. This insight underscores why isolated measurement of hs-CRP or MPO, without integration into a broader pathophysiological framework, yields limited clinical traction.
Markers of Myocardial Stress and Fibrotic Remodeling
In heart failure (HF), biomarkers reflecting mechanical stress and maladaptive fibrotic remodeling have emerged to complement natriuretic peptides. Soluble Suppression of Tumorigenicity 2 (sST2) is a member of the interleukin-1 receptor family released by cardiac myocytes and fibroblasts in response to mechanical strain. Galectin-3, a β-galactoside-binding lectin, is secreted by activated macrophages and is involved in tissue inflammation and fibrosis.10,12,13
Critical Appraisal: Why Has Therapeutic Translation Failed?
Both sST2 and galectin-3 provide strong prognostic information for mortality and HF hospitalization, often independent of natriuretic peptide levels.12,13 However, their clinical adoption has been hampered by several fundamental limitations that are emblematic of the broader challenges facing novel biomarkers.
First, neither biomarker is cardiac-specific. sST2 is elevated in pulmonary disease, autoimmune conditions, and severe infections, while galectin-3 is involved in fibrotic processes in the liver, kidneys, and lungs. 10 In multimorbid patients—the very population in whom refined risk stratification is most needed—elevations in sST2 or galectin-3 cannot be reliably attributed to cardiac pathology alone. This confounds both diagnostic and prognostic interpretation.
Second, and more critically, there is a paucity of evidence demonstrating that targeting therapies based on these biomarkers improves outcomes. Unlike natriuretic peptides, which reflect a treatable state of volume overload amenable to diuresis and guideline-directed medical therapy, it is unclear how a clinician should act upon an isolated elevation in galectin-3 or sST2. Should diuretics be intensified? Should novel anti-fibrotic agents be initiated? Currently, no therapy is proven to specifically lower these markers and subsequently improve hard endpoints. Consequently, sST2 and galectin-3 remain primarily risk stratifiers without a clear, evidence-based therapeutic imperative, raising legitimate questions about their cost-effectiveness in routine management.
Third, biological variability and assay characteristics complicate serial monitoring. The intra-individual biological variation of sST2 and galectin-3 is substantial, and the lack of standardized assays across manufacturers precludes the establishment of universal decision thresholds. This contrasts sharply with high-sensitivity troponins and natriuretic peptides, for which analytical harmonization efforts are more advanced.
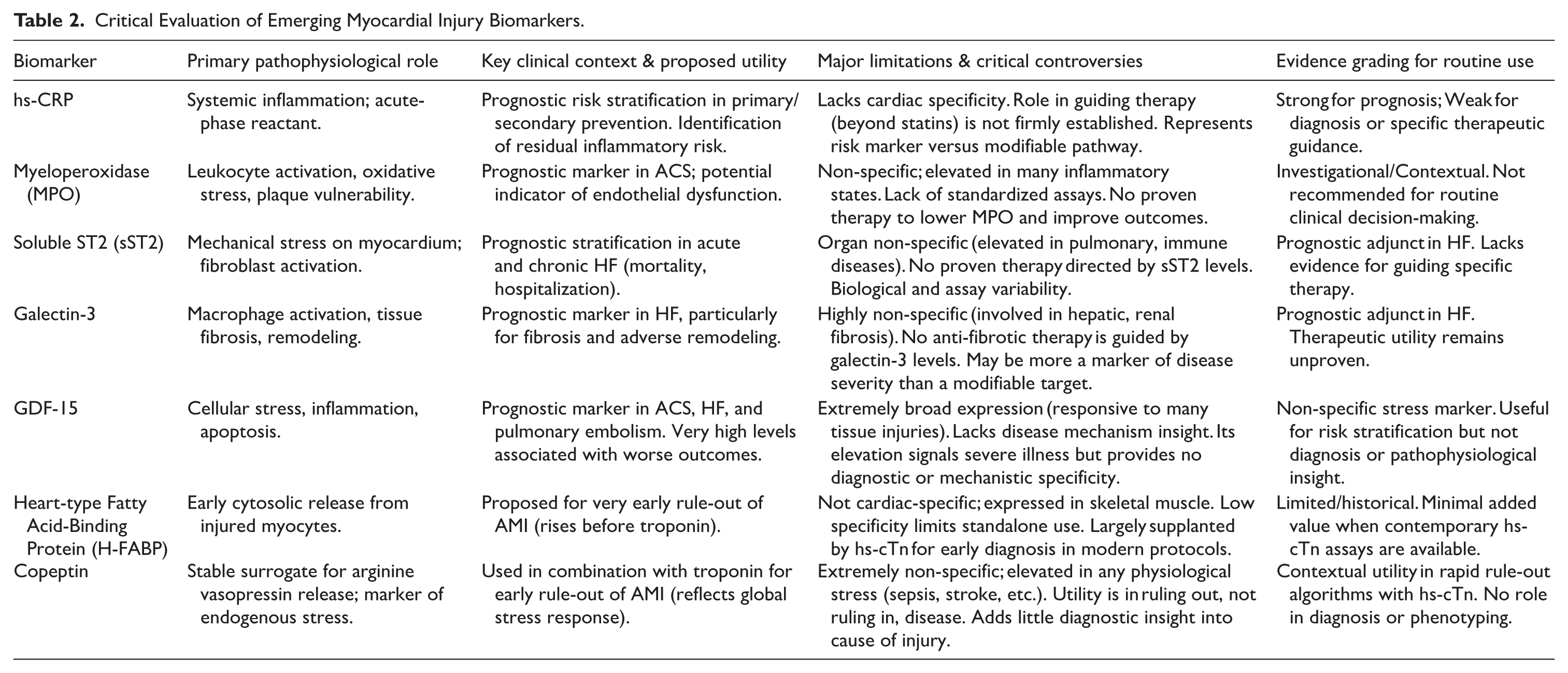
From a systems biology perspective, network pharmacology analyses have identified galectin-3 and related fibrotic pathways as central nodes within broader protein-protein interaction networks governing myocardial remodeling and inflammation. 52 Such analyses suggest that galectin-3 does not operate in isolation but rather participates in complex signaling cascades involving TGF-β, matrix metalloproteinases, and inflammatory cytokines. This interconnectivity may explain why single-marker targeting has yielded disappointing results and supports the rationale for multi-marker, multi-target therapeutic strategies that address the network rather than individual nodes. Table 2 provides a structured critical evaluation of the major emerging biomarkers, highlighting their pathophysiological roles, clinical contexts, key limitations, and the current level of evidence supporting routine clinical use.
Critical Evaluation of Emerging Myocardial Injury Biomarkers.
The Challenge of Specificity and the Quest for Clinical Utility
A universal theme across the expanding biomarker universe is the tension between pathophysiological insight and clinical specificity. Growth Differentiation Factor-15 (GDF-15), for example, is a distant member of the TGF-β family upregulated under conditions of cellular stress, inflammation, and apoptosis. It is a powerful prognostic marker across diverse conditions, including ACS, HF, and pulmonary embolism. However, its expression is induced in virtually all tissues following injury, making it an exquisitely sensitive but profoundly non-specific biomarker of overall illness severity rather than a tool for cardiac diagnosis (Table 2). This lack of specificity limits its utility in mechanistic phenotyping—a core objective of precision cardiology.
Similarly, markers promoted for early diagnosis, such as Heart-type Fatty Acid-Binding Protein (H-FABP) and copeptin, face significant hurdles. H-FABP, while released rapidly from injured myocytes, is also abundant in skeletal muscle, and its diagnostic performance is generally inferior to contemporary hs-cTn assays. Copeptin, a stable surrogate for arginine vasopressin, reflects endogenous stress and is useful in combination with troponin for accelerated rule-out of AMI due to its very high negative predictive value when low. However, it is elevated in any acute illness—sepsis, stroke, trauma—providing zero diagnostic specificity for the cause of myocardial injury.42,43 Its utility is purely in excluding disease rapidly, not in characterizing it.
The translational failure of many emerging biomarkers can be attributed, in part, to the reductionist paradigm that has dominated biomarker research: the search for a single, superior analyte that independently predicts risk or guides therapy. Network pharmacology offers a conceptual antidote to this reductionism by modeling the complex, multi-target interactions that underlie myocardial injury and repair. 52 By identifying hub genes and central pathways—such as those involved in inflammation, fibrosis, and metabolism—network-based approaches can inform the development of multi-marker panels and multi-target therapies that more faithfully reflect the underlying biology. This systems-level perspective reinforces the central thesis of this review: that precision in myocardial injury management will be achieved not through the discovery of isolated novel biomarkers, but through the intelligent, contextual integration of multiple data streams within a structured clinical reasoning framework.
Integrative Pathophysiological Mapping: From Injury to Biomarker Signature
The relationships between diverse injury mechanisms and their corresponding biomarker patterns are complex and overlapping. Figure 2 proposes a conceptual map to visualize these connections. This schematic illustrates how a primary insult (eg, plaque rupture, viral infection, or cytotoxic drug) activates core injury pathways—necrosis, inflammation, oxidative stress, and fibrosis. These pathways, often interconnected, lead to the release of specific biomarker clusters. The figure highlights, for instance, that while acute necrosis primarily elevates troponins and H-FABP, it also triggers a secondary inflammatory response (raising hs-CRP, MPO). A chronic hemodynamic stress state primarily elevates NPs and sST2, which over time drives a fibrotic response (elevating galectin-3). This visual model underscores that a patient’s biomarker profile is a composite signature reflecting the predominant active pathways, explaining why single biomarkers are often insufficient for mechanistic diagnosis and why multi-marker integration, as advocated in the C.A.L.I.B.R.A.T.E. framework, is essential.
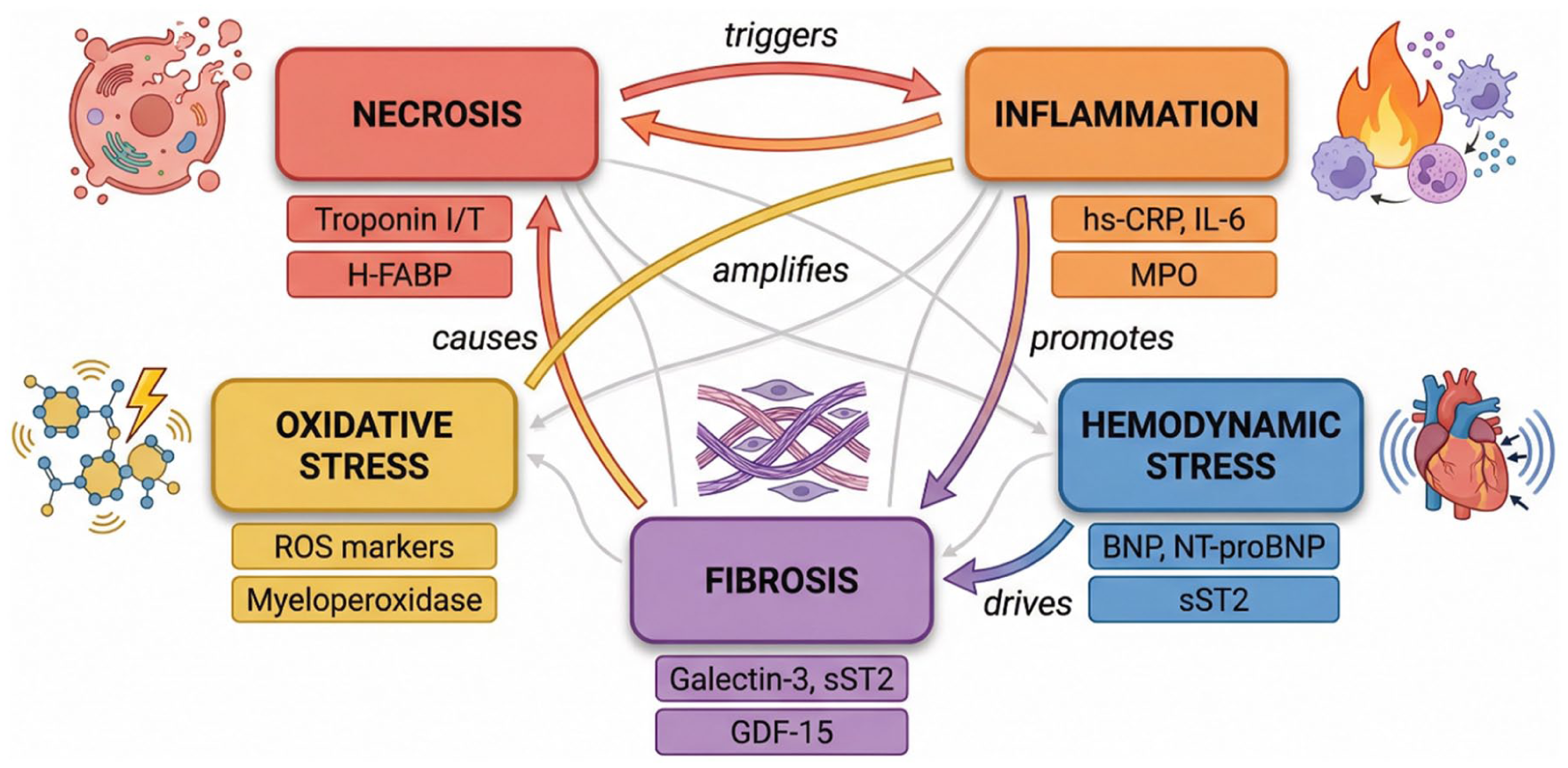
Pathophysiological pathways of myocardial injury and associated biomarker clusters.
The expansion of the biomarker universe beyond necrosis offers tantalizing potential for deeper phenotyping of myocardial injury and heart failure. However, a critical appraisal reveals significant barriers to their integration into precision medicine paradigms. Issues of organ specificity, a lack of evidence for therapy guidance, and the challenge of interpreting isolated elevations in multimorbid patients are pervasive. While these markers enrich prognostic assessment, their transition from risk markers to actionable therapeutic targets remains largely unfulfilled. Their greatest value may lie not in isolation, but as components of a multi-marker panel, interpreted within a rigorous clinical and pathophysiological framework as illustrated in Figure 2. This integrated approach is essential to avoid diagnostic distraction and to harness their potential for truly personalized management, a theme explored in the proposed C.A.L.I.B.R.A.T.E. framework in section 8.
Etiology-Specific Biomarker Puzzles: Navigating Diagnostic Dilemmas in Myocarditis, COVID-19, and Beyond
The interpretation of myocardial injury biomarkers reaches its zenith of complexity in specific etiologies where traditional diagnostic pathways are obscured. In conditions such as viral myocarditis, COVID-19-associated cardiac injury, myocardial infarction with non-obstructive coronary arteries (MINOCA), and Takotsubo cardiomyopathy, elevated troponin confirms injury but provides scant insight into its mechanism. This creates profound diagnostic dilemmas, as the management for an acute plaque rupture (Type 1 MI) diverges radically from that for viral-induced myocyte damage or catecholamine-mediated stunning. This section critically examines the distinctive yet overlapping biomarker puzzles presented by these conditions, focusing on the limitations of biomarkers in isolation and the imperative for a multi-modal diagnostic strategy. For brevity and clarity, we concentrate on 3 prototypical scenarios that illustrate the core challenges: acute myocarditis, COVID-19-associated myocardial injury, and the spectrum of MINOCA/Takotsubo.
Myocarditis: The Troponin-Positive Mimicker of Myocardial Infarction
Acute myocarditis, often viral in origin, is characterized by inflammatory infiltration of the myocardium leading to myocyte necrosis. Patients frequently present with chest pain, ECG changes (ST-elevation or depression), and elevated cardiac troponin, creating a clinical picture indistinguishable from acute Type 1 MI.53,54 This diagnostic overlap represents a critical challenge.
Critical Appraisal and Diagnostic Dilemmas
While troponin is nearly universally elevated in acute myocarditis and correlates with the extent of injury, its kinetic profile and peak magnitude are nonspecific and cannot reliably differentiate it from an ischemic cause. 55 Inflammatory markers like CRP and ESR are typically elevated but are also nonspecific. The diagnostic dilemma crystallizes when coronary angiography, performed to exclude obstructive coronary artery disease, reveals non-obstructive arteries. At this juncture, biomarkers alone provide no etiological clarity. The resolution depends on advanced cardiac imaging. Cardiac magnetic resonance (CMR) imaging, utilizing the Lake Louise Criteria (edema on T2-weighted imaging and late gadolinium enhancement in a non-ischemic pattern), has become the non-invasive gold standard for confirming myocarditis and distinguishing it from other MINOCA etiologies.16,56 This scenario perfectly illustrates that biomarkers signal a problem, but imaging defines its nature—a principle central to the “A” (Adjunctive Tests) component of the C.A.L.I.B.R.A.T.E. framework.
COVID-19-Associated Myocardial Injury: A Multifactorial Conundrum
The COVID-19 pandemic starkly revealed the multifaceted nature of myocardial injury. A significant proportion of hospitalized patients exhibited elevated troponin levels, which were strongly associated with increased mortality.55,57 However, the elevation of troponin in COVID-19 can stem from a bewildering array of mechanisms, rendering it a profound diagnostic and prognostic puzzle.
Critical Appraisal and Diagnostic Dilemmas
The injury pathways are heterogeneous and often concurrent: (1) direct viral cytotoxicity via ACE2 receptors; (2) cytokine storm leading to inflammatory cardiomyopathy; (3) microvascular thrombosis due to endothelialitis and a hypercoagulable state; (4) Type 2 MI from respiratory failure and hypoxia; and (5) stress cardiomyopathy (Takotsubo).58,59 A solitary troponin value cannot distinguish among these mechanisms. Consequently, biomarkers in COVID-19 serve more as integrated markers of illness severity and systemic dysregulation than specific cardiac diagnostic tools. Elevated D-dimer and inflammatory markers (IL-6, ferritin, CRP) often parallel troponin elevation, painting a picture of global thromboinflammation.60,61 The clinical challenge is determining the dominant, treatable injury mechanism in real-time—a task that mandates integration with echocardiography to assess ventricular function and, in selected cases, CMR to characterize tissue injury. 56
MINOCA and Takotsubo: The Spectrum of Non-atherosclerotic Injury
MINOCA and Takotsubo cardiomyopathy represent critical diagnoses of exclusion where biomarker interpretation is particularly nuanced. Both present with troponin elevation (often modest in Takotsubo) and absence of obstructive coronary disease on angiography.
Critical Appraisal and Diagnostic Dilemmas
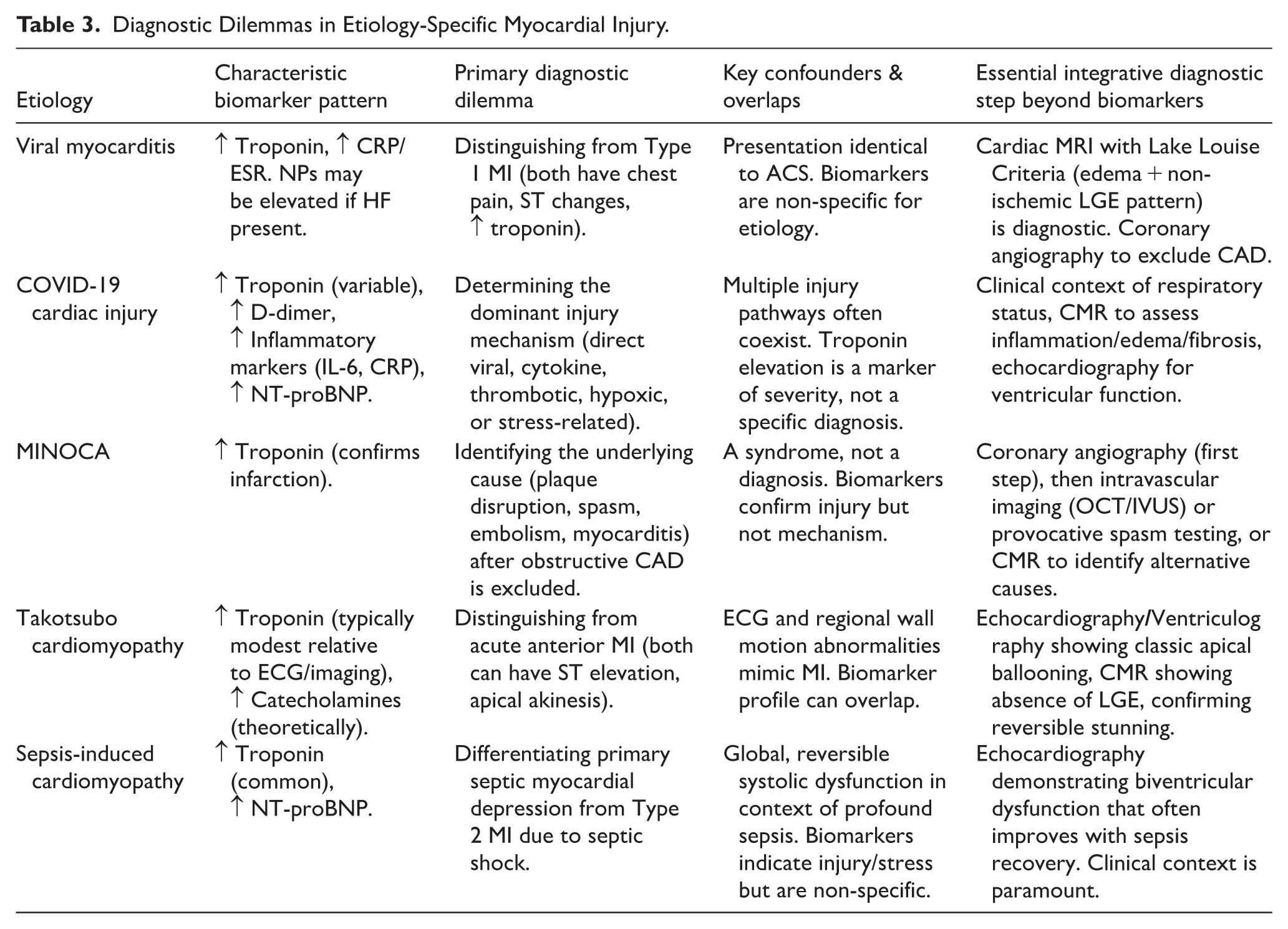
MINOCA is not a final diagnosis but a working description encompassing diverse pathologies: coronary plaque disruption, epicardial or microvascular spasm, coronary thromboembolism, and myocarditis. 16 Troponin confirms the infarction but not its cause. Definitive diagnosis requires dedicated investigations: intravascular imaging (OCT/IVUS) during angiography to identify plaque rupture or erosion, provocative testing for spasm, or CMR to identify myocardial inflammation or edema patterns. Takotsubo cardiomyopathy, characterized by transient regional wall motion abnormalities often triggered by emotional or physical stress, further complicates the picture. A key differentiating feature is the disproportionately elevated catecholamine levels relative to troponin elevation, though catecholamines are not routinely measured. The primary diagnostic tool remains imaging—ventriculography or echocardiography showing apical ballooning, with CMR confirming the absence of late gadolinium enhancement, supporting the diagnosis of transient stunning rather than necrosis. Table 3 summarizes the characteristic biomarker patterns, primary diagnostic dilemmas, and essential integrative diagnostic steps for the major etiology-specific myocardial injuries discussed in this section.
Diagnostic Dilemmas in Etiology-Specific Myocardial Injury.
The Integrative Diagnostic Imperative: A Schematic Approach
The consistent theme across these etiology-specific puzzles is the failure of biomarkers to provide a standalone diagnosis. Figure 3 proposes a diagnostic algorithm for the patient presenting with acute myocardial injury (elevated troponin) to navigate these dilemmas. The algorithm begins with the initial clinical presentation and ECG. The pivotal branch point is the result of coronary angiography. If obstructive disease is found, the pathway follows standard ACS management. If angiography is normal or shows non-obstructive disease (MINOCA), the algorithm branches based on the next most appropriate test: CMR to look for myocarditis or Takotsubo patterns, intravascular imaging to look for plaque pathology, or provocative testing for vasospasm. This visual schema reinforces that biomarkers are the starting alarm, not the final map, and that a structured, multi-modal investigative pathway—exemplified by the C.A.L.I.B.R.A.T.E. framework—is essential to arrive at an accurate etiological diagnosis.
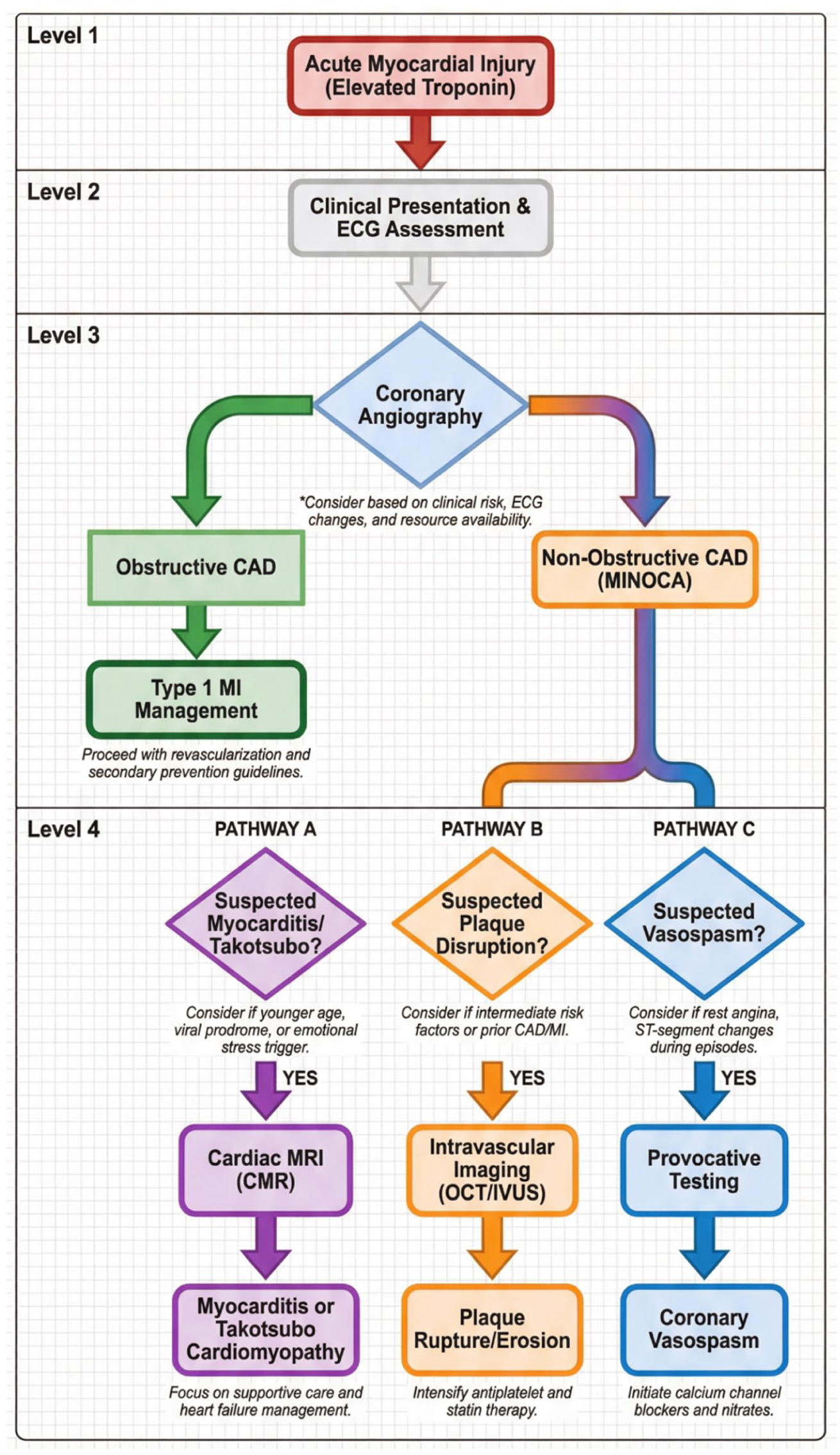
Integrative diagnostic pathway for troponin-positive patients with suspected non-atherosclerotic etiologies (diagnostic flowchart).
Etiology-specific cardiac injuries represent the frontier where conventional biomarker interpretation is most severely tested. In myocarditis, COVID-19, MINOCA, and Takotsubo, elevated troponin is a sensitive sentinel of injury but a blunt instrument for diagnosis. The critical lesson is that these conditions create biomarker overlap syndromes, where identical laboratory findings can stem from radically different causes. Resolving these puzzles demands a disciplined, sequential diagnostic approach that prioritizes anatomical and functional imaging (angiography, echocardiography, CMR) and integrates the full clinical context. This approach moves the clinician from the non-specific question of “Is there injury?” to the precise question of “What is the nature and cause of this injury?”—a fundamental shift necessary for delivering targeted, effective therapy and avoiding the mismanagement that can arise from an over-reliance on biomarkers alone.
The Confounders’ Veto: Biology Versus Test Result
The pursuit of diagnostic precision through biomarkers is perpetually challenged by human biological diversity. A biomarker level is not a pure, isolated signal of cardiac disease but a composite value filtered through the individual’s unique physiology. Renal function, age, sex, and comorbid conditions exert profound and predictable effects on the synthesis, release, metabolism, and clearance of every major cardiac biomarker. This biological “noise” can be of such magnitude that it effectively vetoes the standard interpretation of a test result, leading to diagnostic misclassification, inappropriate risk stratification, and potentially harmful therapeutic decisions. This section provides a critical, in-depth analysis of these fundamental confounders, arguing that their neglect represents one of the most significant barriers to achieving true precision in cardiovascular medicine.
Renal Dysfunction: The Paramount Confounder
Chronic kidney disease (CKD) presents the most complex and consequential challenge to biomarker interpretation. Its effects are bidirectional, multifaceted, and impact nearly all key cardiac biomarkers, often mimicking or masking true cardiac pathology.
Critical Analysis of Mechanisms and Impact
For cardiac troponin, renal impairment leads to chronically elevated baseline levels. The mechanisms are synergistic: (1) Reduced renal clearance of troponin fragments, particularly impactful for cTnT; (2) Heightened cardiac strain from associated hypertension, fluid overload, and left ventricular hypertrophy; and (3) Subclinical myocardial injury from uremic toxins, endothelial dysfunction, and accelerated atherosclerosis. 9 The clinical dilemma is acute: in a CKD patient presenting with chest pain, an elevated hs-cTn may represent an acute MI, chronic stable elevation, or an acute-on-chronic rise from another insult like sepsis. Reliance on a single value above the 99th percentile URL, derived from a healthy reference population, is therefore invalid. The diagnostic pivot must be to serial changes (deltas), yet optimal, CKD-stage-specific delta thresholds remain inadequately validated, creating a persistent evidence gap.
For natriuretic peptides, the effect is differential and critical. NT-proBNP is passively cleared by the kidneys, and its levels rise exponentially as glomerular filtration rate (GFR) declines, often disproportionate to the degree of cardiac filling pressure. 4 BNP is cleared more via receptor-mediated pathways and neutral endopeptidases, making it less dependent on renal function, though still affected. This has direct management implications: using a standard NT-proBNP cutoff for diagnosing acute HF in a patient with stage 4 CKD will yield frequent false positives, potentially leading to unnecessary diuresis. Conversely, the “obesity paradox”—where higher BMI blunts NP secretion—can compound interpretation in the growing population with both obesity and CKD.
Other biomarkers are similarly affected. Inflammatory markers like hs-CRP and cytokines may be elevated due to the chronic inflammatory state of CKD. Fibrosis markers like galectin-3 are also influenced by renal function, as galectin-3 is involved in renal fibrosis itself, confusing its interpretation as a purely cardiac risk marker. 10 This pervasive influence means that in renal impairment, the entire biomarker profile is shifted, demanding a radically contextualized interpretation.
Age and Sex: Non-modifiable Biological Determinants
Aging and biological sex are intrinsic determinants of cardiovascular physiology and biomarker biology that are frequently overlooked in the application of uniform cut-off values.
Age is associated with a progressive increase in baseline levels of both hs-cTn and NPs, even in the absence of clinically overt cardiovascular disease. This reflects age-related phenomena: myocardial senescence with low-grade myocyte turnover, increased myocardial stiffness, and reduced renal clearance.7,9 Using a single, young-adult-derived 99th percentile URL in an 85-year-old patient guarantees a high rate of “false positive” elevations for acute MI and over-diagnosis of HF. Age-stratified reference ranges, while recommended by assay manufacturers, are often not implemented in clinical practice algorithms or emergency department protocols, leading to diagnostic inaccuracy.
Sex differences are profound. Women, on average, have lower muscle mass and different myocardial remodeling patterns. Assay-specific 99th percentile URLs for hs-cTn are consistently lower in women than in men. Failure to use sex-specific cut-offs disproportionately disadvantages women, reducing the diagnostic sensitivity for MI in a population already prone to under-diagnosis due to atypical presentation. 44 Similarly, NP levels are generally higher in women than in men at any given age, partly due to differences in body composition and hormonal influences. A nuanced understanding of these baseline differences is not a minor detail but a fundamental requirement for equitable and accurate diagnosis.
Comorbidities: The Multimorbid Kaleidoscope
The real-world patient rarely presents with a single pathology. Comorbid conditions create a kaleidoscope of interacting effects on biomarker profiles.
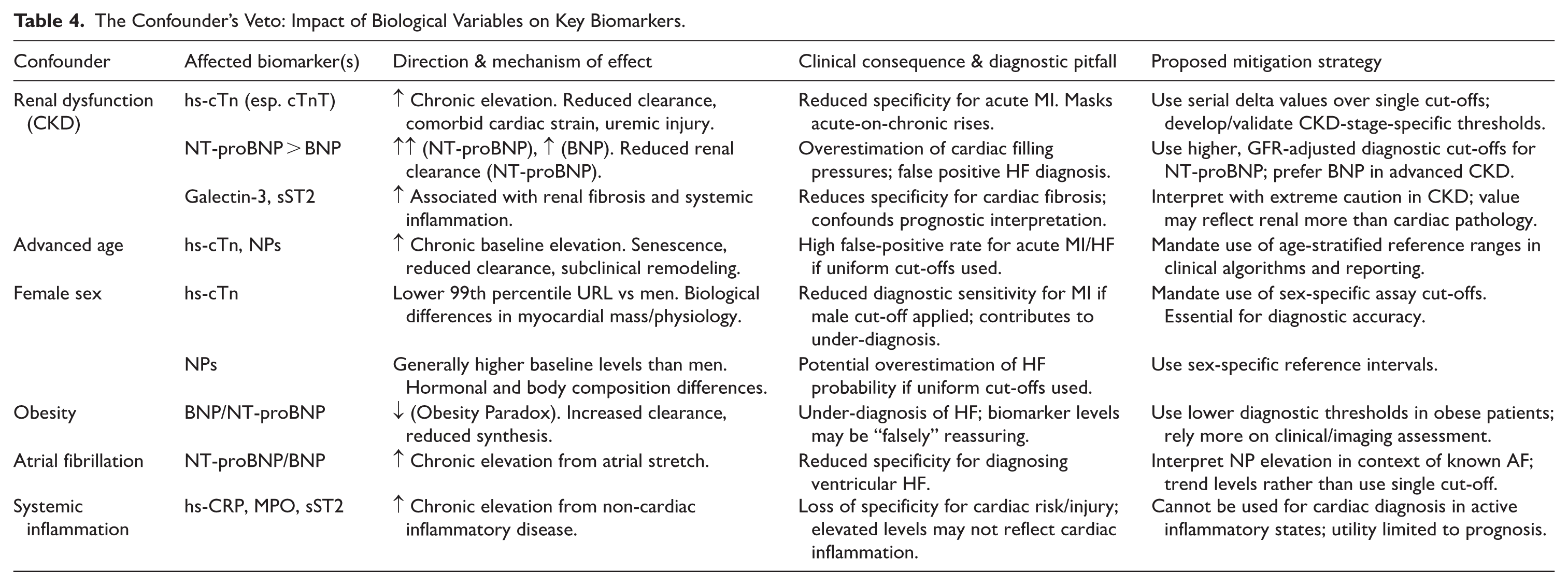
Obesity directly modulates NP biology through increased receptor clearance and possibly reduced synthesis, leading to lower circulating levels for any given degree of cardiac wall stress. 3 This can delay or obscure the diagnosis of HF in obese individuals. Atrial fibrillation causes chronic atrial stretch and elevated NPs independent of ventricular dysfunction, confounding their use in diagnosing HF. 4 Chronic inflammatory diseases (eg, rheumatoid arthritis, SLE) and pulmonary diseases (eg, COPD, pulmonary hypertension) chronically elevate hs-CRP, MPO, and sST2, stripping these biomarkers of their specificity for primary cardiac events. Diabetes accelerates atherosclerosis and causes microvascular dysfunction, leading to a higher prevalence of Type 2 MI and chronic troponin elevation. Furthermore, cancer and cardiotoxic therapies like anthracyclines can cause direct myocardial injury, elevating troponin and NPs in patterns that must be distinguished from ACS or primary HF. 62 Table 4 provides a comprehensive overview of how key biological confounders—renal dysfunction, advanced age, female sex, obesity, atrial fibrillation, and systemic inflammation—modulate the levels of major cardiac biomarkers and the clinical consequences of these effects.
The Confounder’s Veto: Impact of Biological Variables on Key Biomarkers.
Biological Variability: The Hidden Confounder
Beyond the well-recognized influences of renal function, age, sex, and comorbidities, an additional layer of complexity confounds the interpretation of serial biomarker measurements: intra-individual biological variation. While analytical imprecision and inter-individual differences are routinely acknowledged, the inherent fluctuation of biomarker concentrations within a single individual over time—independent of changes in disease state—is frequently overlooked. This biological “noise” has profound implications for distinguishing true clinical change from random variation, particularly when monitoring response to therapy or assessing disease progression.
The magnitude of intra-individual biological variation differs markedly between the 2 cornerstone families of cardiac biomarkers. For natriuretic peptides, the week-to-week intra-individual coefficient of variation (CV_i) is notably high, typically ranging from 30% to over 40% in both healthy subjects and clinically stable patients with chronic heart failure. 63 This substantial variability necessitates a large change in serial measurements—often exceeding 100%—to indicate a statistically significant alteration in clinical condition. Consequently, modest fluctuations in BNP or NT-proBNP levels during outpatient follow-up or hospitalization may reflect biological variation rather than meaningful deterioration or improvement. This insight tempers the enthusiasm for natriuretic peptide-guided therapy that relies on small, incremental changes in biomarker concentration. Clinicians should interpret NP trends with caution, reserving judgment for sustained and substantial directional changes that exceed the reference change value (RCV) specific to the assay and patient population. 64
In contrast, high-sensitivity cardiac troponins exhibit considerably lower intra-individual biological variation. Recent consensus guidance indicates that a variation exceeding approximately 30% between serial hs-cTnI or hs-cTnT measurements should be considered significant in both healthy individuals and patients with cardiac disease. 64 This lower biological noise floor enhances the utility of serial troponin measurements for detecting acute myocardial injury and monitoring disease activity. The higher signal-to-noise ratio of hs-cTn compared to natriuretic peptides partly explains why delta-based algorithms for acute MI diagnosis have achieved robust clinical validation, whereas analogous approaches for heart failure monitoring have yielded more variable results.
The clinical implications of biological variability extend to all components of the C.A.L.I.B.R.A.T.E. framework. In particular, the “T” (Time kinetics) and “R” (Rule-out/in thresholds) components must account for both analytical and biological variation when interpreting serial changes. A patient whose BNP decreases by 40% after diuresis may not have experienced a true biological response; this change falls within the expected intra-individual variation. Conversely, a hs-cTnI increase of 50% over 3 hours strongly suggests an acute process. Integrating knowledge of biological variability into clinical reasoning prevents both over-interpretation of random fluctuations and under-recognition of genuine pathophysiological signals. As precision cardiology advances, the development of personalized reference change values—accounting for individual baseline variability, comorbidities, and assay characteristics—represents a critical frontier for enhancing the accuracy of biomarker-guided care. 64
The Integrative Imperative: A Conceptual Model of Biological Noise
The cumulative effect of these confounders is to create a “biological noise floor” that varies substantially from patient to patient. Figure 4 conceptualizes this challenge. The figure would depict 2 vertical axes: one for the “True Cardiac Signal” (eg, acute necrosis, hemodynamic stress) and one for the “Measured Biomarker Level.” For a healthy young individual, the baseline “noise floor” is low, and a rise in the measured biomarker closely reflects the true cardiac signal. However, for a patient with multiple confounders (eg, an elderly woman with CKD and obesity), the baseline noise floor is markedly elevated due to the cumulative effects of age, renal impairment, and sex. An identical “true cardiac signal” from a small acute MI would now be superimposed on this high baseline, resulting in a measured biomarker level that may only slightly exceed a generic cut-off, making detection difficult. The figure would visually argue that precision requires estimating and adjusting for this individual-specific noise floor rather than comparing a result to a population average.
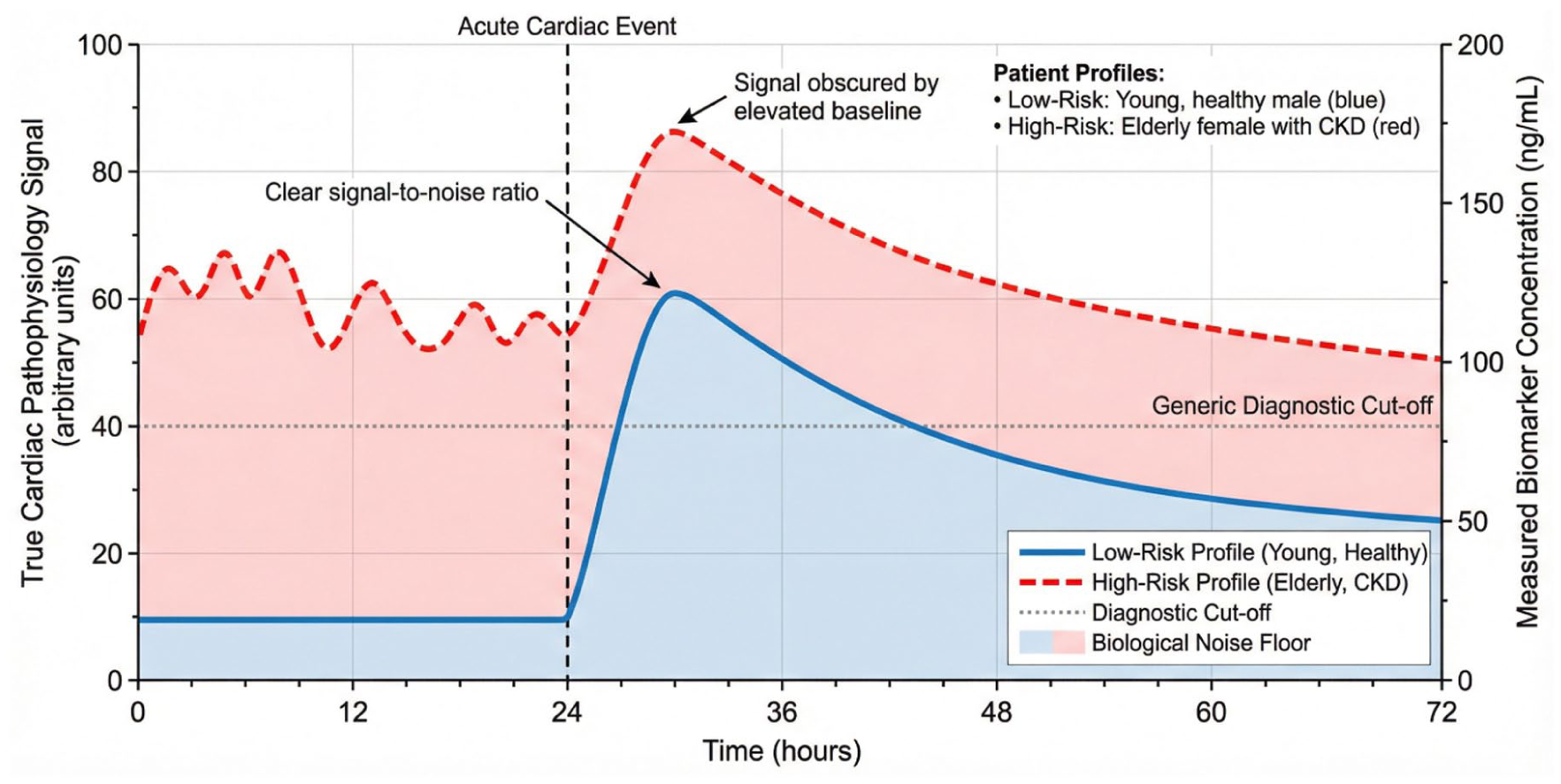
The confounder effect: elevated biological noise floor obscuring the cardiac signal.
The biological confounders of renal function, age, sex, and comorbidities do not merely introduce statistical error; they fundamentally alter the clinical meaning of biomarker results. Ignoring them leads to a rigid, flawed application of precision tools. Recognizing their veto power necessitates a paradigm shift from a one-cut-off-fits-all model to a personalized reference framework. This framework must incorporate adjusted thresholds, prioritize serial kinetic changes over single values, and demand the integration of biomarker data with a comprehensive understanding of the patient’s physiological landscape. The following section will explore the translational chasm between this ideal and current clinical practice, before proposing a concrete framework to bridge it.
From Bench to Bedside: The Translational Chasm—A Critical Analysis of Implementation Barriers
The preceding sections have outlined a compelling vision for precision cardiology: a future where multi-marker panels, interpreted through the lens of individual biology and integrated with advanced imaging, guide personalized diagnosis and therapy. However, a formidable chasm separates this theoretical potential from routine clinical practice. The translation of biomarker science into tangible improvements in patient care and outcomes is hindered by a complex array of economic, practical, educational, and systemic barriers. This section critically examines these implementation challenges, arguing that their neglect renders even the most promising biomarker innovation merely an academic exercise. Bridging this translational gap is not a secondary concern but the central challenge for the field.
Economic and Reimbursement Hurdles
The financial ecosystem of healthcare actively shapes which technologies are adopted. High-sensitivity and novel biomarker assays are frequently more expensive than their conventional counterparts. While evidence may support the cost-effectiveness of hs-cTn in accelerating emergency department discharge and improving outcomes, the immediate cost-impact on hospital laboratories and health systems can be a significant deterrent, particularly in resource-constrained settings. 65
The development and validation of multi-marker panels exacerbate this issue. A strategy combining troponin, NP, and a fibrosis marker like sST2 or galectin-3 for heart failure phenotyping multiplies reagent and processing costs. Without robust, prospective data demonstrating that such panels definitively improve hard clinical endpoints (eg, mortality, hospitalization) and reduce overall healthcare costs, payers are reluctant to provide adequate reimbursement. The current fee-for-service model often fails to reward the preventive risk stratification that these biomarkers enable, instead incentivizing procedural interventions for established disease. This misalignment creates a powerful economic disincentive for the adoption of comprehensive biomarker profiling.
Clinical Practice Integration and Interpretive Complexity
Beyond cost, the integration of new biomarkers into clinical workflows presents substantial operational and cognitive challenges. The emergency department physician managing a possible ACS or the general cardiologist managing heart failure already operates under significant time pressure and information overload.
Workflow Integration
Rapid, serial hs-cTn measurements require streamlined laboratory turn-around times and effective communication protocols. Point-of-care testing offers a solution but may involve trade-offs in analytical precision. Incorporating a novel biomarker result from a send-out lab that returns hours or days later disrupts clinical decision-making timelines, limiting its utility.
Interpretive Burden
Perhaps the most significant barrier is the cognitive load placed on clinicians. As detailed in Section 6.0, each biomarker comes with a list of confounders, specific cut-offs (which may vary by age, sex, and assay), and nuanced kinetic profiles. Expecting a busy clinician to accurately synthesize a troponin delta, an NT-proBNP level adjusted for renal function and obesity, and a galectin-3 result in the context of the patient’s comorbidity profile is often unrealistic. Without clear, protocol-driven guidance and clinical decision support (CDS) tools integrated into electronic health records (EHRs), the risk of misinterpretation is high. This complexity can lead to clinical inertia, where providers default to familiar, simpler patterns of practice, or to diagnostic confusion, where ambiguous biomarker results prompt unnecessary referrals and tests rather than providing clarity. The C.A.L.I.B.R.A.T.E. framework is specifically designed to mitigate this interpretive burden by providing a structured cognitive pathway for data synthesis.
Health System Infrastructure and Assay Standardization
The reliable implementation of precision biomarker medicine depends on foundational infrastructure that is often lacking.
Assay Standardization and Availability
A critical limitation is the lack of standardization across different manufacturer platforms for many biomarkers. While progress has been made with cardiac troponins, significant inter-assay variability persists for markers like sST2 and galectin-3.12,13 A patient’s result is therefore only interpretable in the context of the specific assay used, hindering the development of universal cut-offs and complicating care transitions between institutions. Furthermore, novel and specialized biomarkers are often unavailable in smaller community hospitals or in low- and middle-income countries, exacerbating healthcare disparities.
Data Integration and Interoperability
The promise of integrating biomarker data with ECG findings, imaging reports, and genetic information requires sophisticated health information technology. Many EHR systems are not designed to synthesize these disparate data streams into a unified patient dashboard. Without effective interoperability, the vision of a comprehensive, algorithm-driven diagnostic approach remains fragmented.
Ethical and Psychological Considerations
Increased biomarker sensitivity also introduces ethical dilemmas and potential psychological harms.
Overdiagnosis and Patient Anxiety
The detection of subclinical troponin elevation in an asymptomatic individual with stable CKD, for example, labels the patient with “myocardial injury” but offers no clear therapeutic pathway. This can generate significant patient anxiety, lead to a cascade of low-yield testing, and potentially result in overtreatment without proven benefit. The ethical principle of primum non nocere (first, do no harm) demands careful consideration of when not to test.
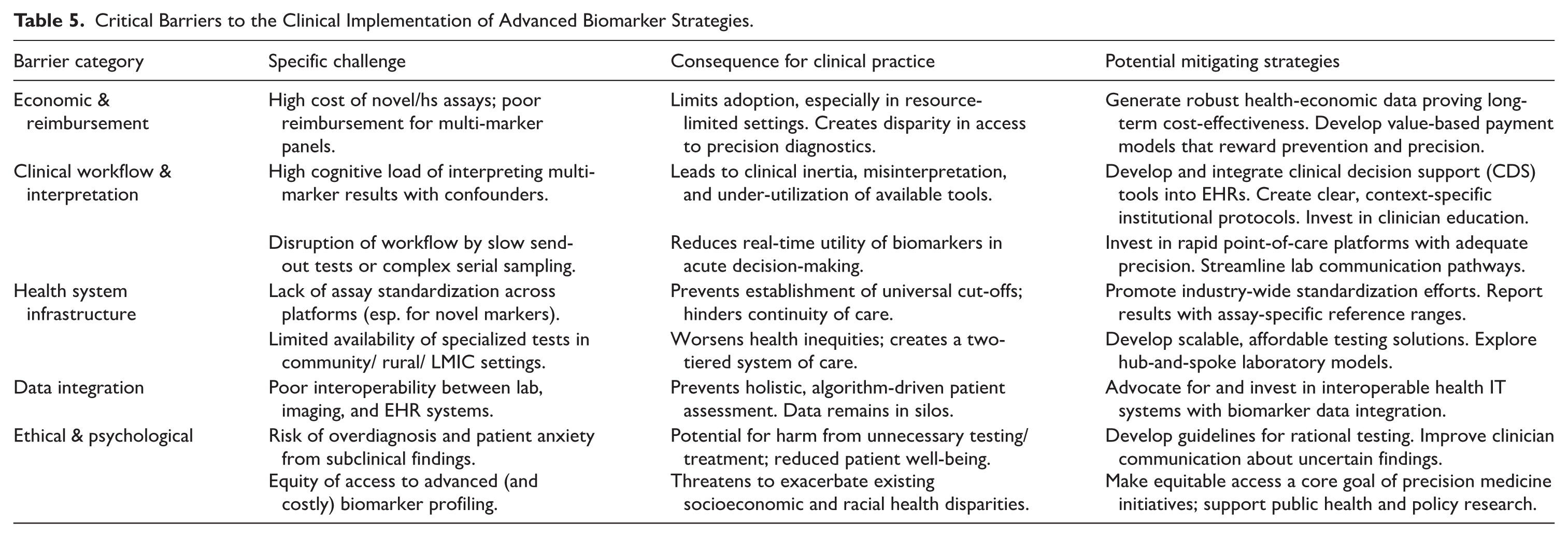
Equity of Access
As precision biomarker strategies evolve, there is a palpable risk that they will become the standard of care for affluent, well-insured populations in tertiary care centers, while remaining inaccessible to others. This would worsen existing cardiovascular health disparities rather than alleviate them. Table 5 categorizes the principal barriers to clinical implementation—economic, workflow-related, infrastructural, and ethical—along with their specific challenges, consequences for practice, and potential mitigating strategies.
Critical Barriers to the Clinical Implementation of Advanced Biomarker Strategies.
Visualizing the Translational Pipeline: A Leaky Pathway
The journey from biomarker discovery to routine clinical impact is a pipeline with multiple potential failure points. Figure 5 conceptualizes this “translational pipeline.” The diagram illustrates stages from Basic Discovery & Assay Development through Clinical Validation, Health Economic Assessment, Clinical Guideline Adoption, to final Clinical Implementation. At each stage, a “leak” or barrier—labeled with the challenges from Table 5 (eg, “Lack of Standardization,” “High Cognitive Load,” “Poor Reimbursement”)—drains potential innovations away from clinical practice. This visual model underscores that a failure at any single stage can halt translation, explaining why so few biomarker discoveries successfully navigate the entire path to become bedrock tools of patient care.
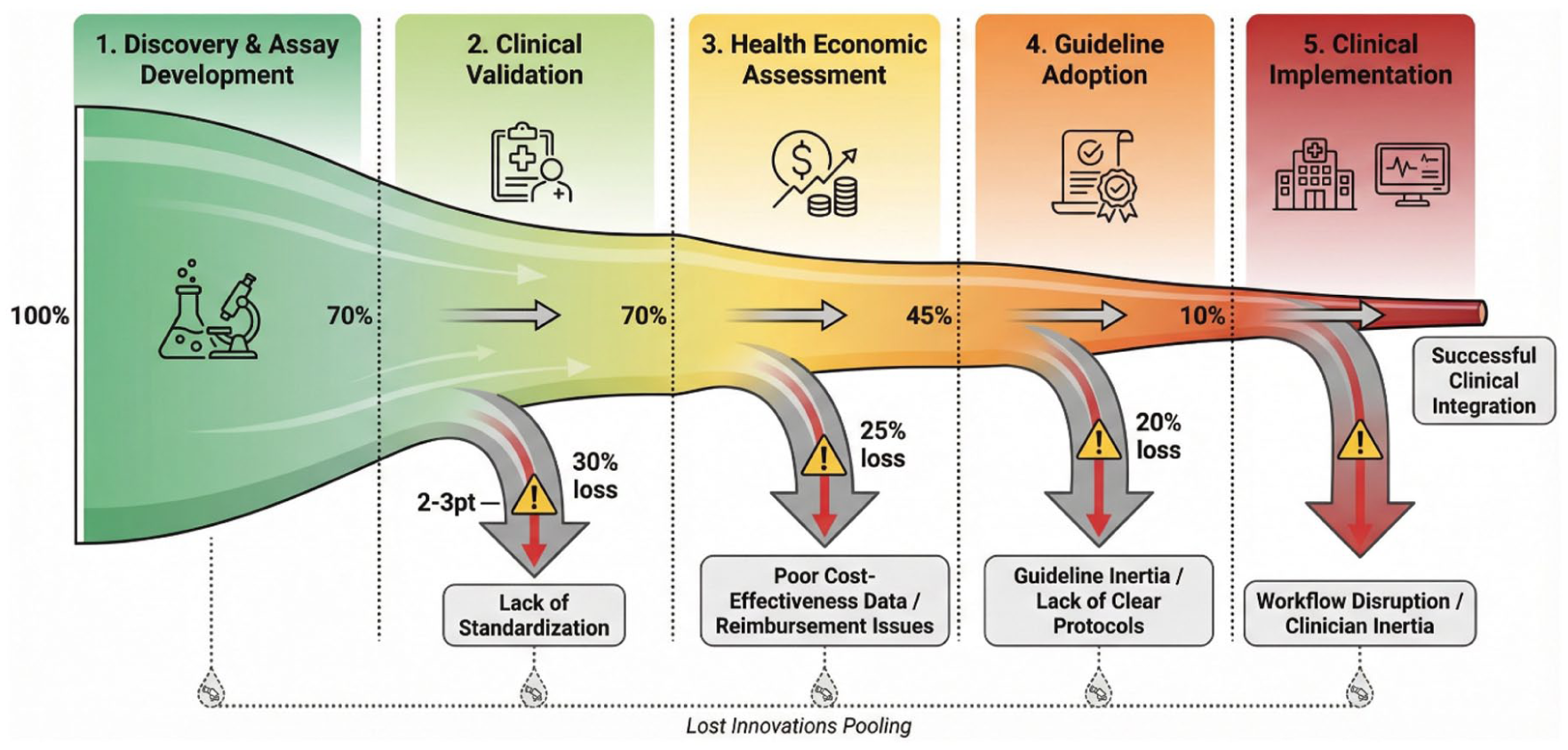
The translational pipeline for biomarker implementation: sites of attrition.
The sophisticated biomarker science detailed in this review exists within a fragile ecosystem. Economic constraints, clinical workflow realities, infrastructural limitations, and ethical considerations collectively form a “translational chasm” that is as consequential as any biological knowledge gap. Critically analyzing these barriers is not pessimistic but essential. It shifts the focus from purely technological advancement to the necessary concomitant advances in health economics, clinical informatics, education, and policy. The following section will synthesize the critical insights from both the biological and implementation domains to propose a pragmatic framework designed to bridge this chasm, offering a realistic pathway toward contextual, precise, and equitable biomarker application.
Proposed Framework for Contextual Biomarker Integration: The C.A.L.I.B.R.A.T.E. Approach
The critical analyses presented thus far converge on a central thesis: the future of precision in myocardial injury management lies not in the discovery of a single superior biomarker, but in the intelligent, context-dependent integration of available data. To address the translational chasm and provide a practical pathway for clinicians, we propose a novel integrative framework: The C.A.L.I.B.R.A.T.E. Approach. This model synthesizes the critical themes of this review—mechanistic understanding, biological confounders, multi-modal diagnostics, and clinical context—into a structured yet flexible schema for personalized biomarker interpretation and therapeutic decision-making.
The C.A.L.I.B.R.A.T.E. Framework: Core Components
C – Clinical Context
This is the foundational and non-negotiable first step. It involves a deliberate assessment of the gestalt: the patient’s symptoms (typical chest pain vs dyspnea at rest), hemodynamic status, and the clinical scenario (emergency department, post-operative, outpatient clinic). A troponin elevation in a 25-year-old with viral prodromes and pleuritic pain suggests a different pathway (myocarditis) than the same elevation in a 65-year-old with crushing substernal pressure (Type 1 MI). Context sets the pre-test probability and directs the entire diagnostic journey.
A – Assay Characteristics & Generation
The clinician must know the tool being used. Is it a contemporary or a high-sensitivity (hs) troponin assay? Which manufacturer (critical for interpreting specific cut-offs)? Is it NT-proBNP or BNP? Understanding the assay’s performance—its limit of detection, 99th percentile URL (and whether age/sex-specific values are applied), and known interferences—is essential to avoid misinterpreting a technically inadequate result or applying an inappropriate reference standard.
L – Likelihood (Pre-Test Probability)
Formally or informally, estimating the pre-test probability of disease (eg, using the HEART score for ACS) should guide the aggressiveness of the diagnostic pursuit and the interpretation of borderline results. A low pre-test probability patient with a minimally elevated hs-cTn may be managed conservatively with observation and repeat testing, while the same value in a high-probability patient warrants urgent intervention.
I – Injury Mechanism (Pathophysiological Phenotyping)
Upon confirming injury (elevated biomarker), the immediate next question must be “Why?” This step involves active consideration of the major mechanistic pathways: Type 1 MI (plaque rupture), Type 2 MI (supply-demand mismatch), Myocarditis, Direct Toxicity (eg, sepsis, chemotherapy), or Hemodynamic Stress (decompensated HF). The initial biomarker profile, combined with context, points toward the dominant mechanism and dictates subsequent steps.
B – Biomarker Profile (Multi-Marker Integration)
Move beyond a single biomarker. Integrate the results to create a pathophysiological profile (as illustrated in Figure 2):
Necrosis
Stress
Necrosis
R – Rule-out/In Thresholds (Dynamic & Personalized)
Apply diagnostic cut-offs not as rigid binaries, but as dynamic thresholds informed by steps C, A, and L. For hs-cTn, this means using serial delta changes personalized to the assay’s precision and the patient’s baseline (especially in CKD or elderly patients). For NPs, this means mentally adjusting the diagnostic threshold for obesity (lower threshold) or renal failure (higher threshold for NT-proBNP). This step acknowledges the “Confounder’s Veto” and moves toward individualized reference ranges.
A – Adjunctive Tests (Mandatory Integration)
Biomarkers are not standalone diagnostics. Their interpretation mandates integration with:
This step closes the diagnostic loop, confirming or refuting the mechanistic hypothesis generated from the biomarker profile.
T – Time (Kinetic Profile)
The dimension of time is critical. The timing of biomarker sampling relative to symptom onset, the observed rise-and-fall kinetic pattern (peak, doubling time), and the trend over hours, days, or weeks provide indispensable information. A rapidly rising and falling troponin suggests acute necrosis, while a stable, chronic low-level elevation suggests a non-acute process. Serial NP trends are more useful than single values in guiding HF therapy.
E – Etiology & Comorbidities (Final Synthesis)
This is the final, synthetic step that incorporates all confounders and comorbidities to arrive at the most accurate Integrated Diagnosis. It answers: “Given this clinical context (C), with these assay results (A, B, T), interpreted through personalized thresholds (R), and confirmed by adjunctive tests (A), what is the specific etiology of this patient’s myocardial injury, and how do their age, renal function, sex, and other diseases modify this diagnosis and its management?”
Figure 6 provides a visual synthesis of this framework, depicting it not as a linear checklist but as an integrated, iterative clinical reasoning cycle. The center of the figure is the Integrated Patient-Specific Diagnosis. Surrounding it are the nine C.A.L.I.B.R.A.T.E. components, interconnected by bidirectional arrows, illustrating how information flows between them during the diagnostic process. For instance, an initial Clinical Context triggers consideration of Injury Mechanism, which guides the selection of the initial Biomarker Profile. The results then cycle through Adjunctive Tests and Time to refine the hypothesis, continuously informed by Assay details and Comorbidities, until a coherent diagnosis is synthesized.
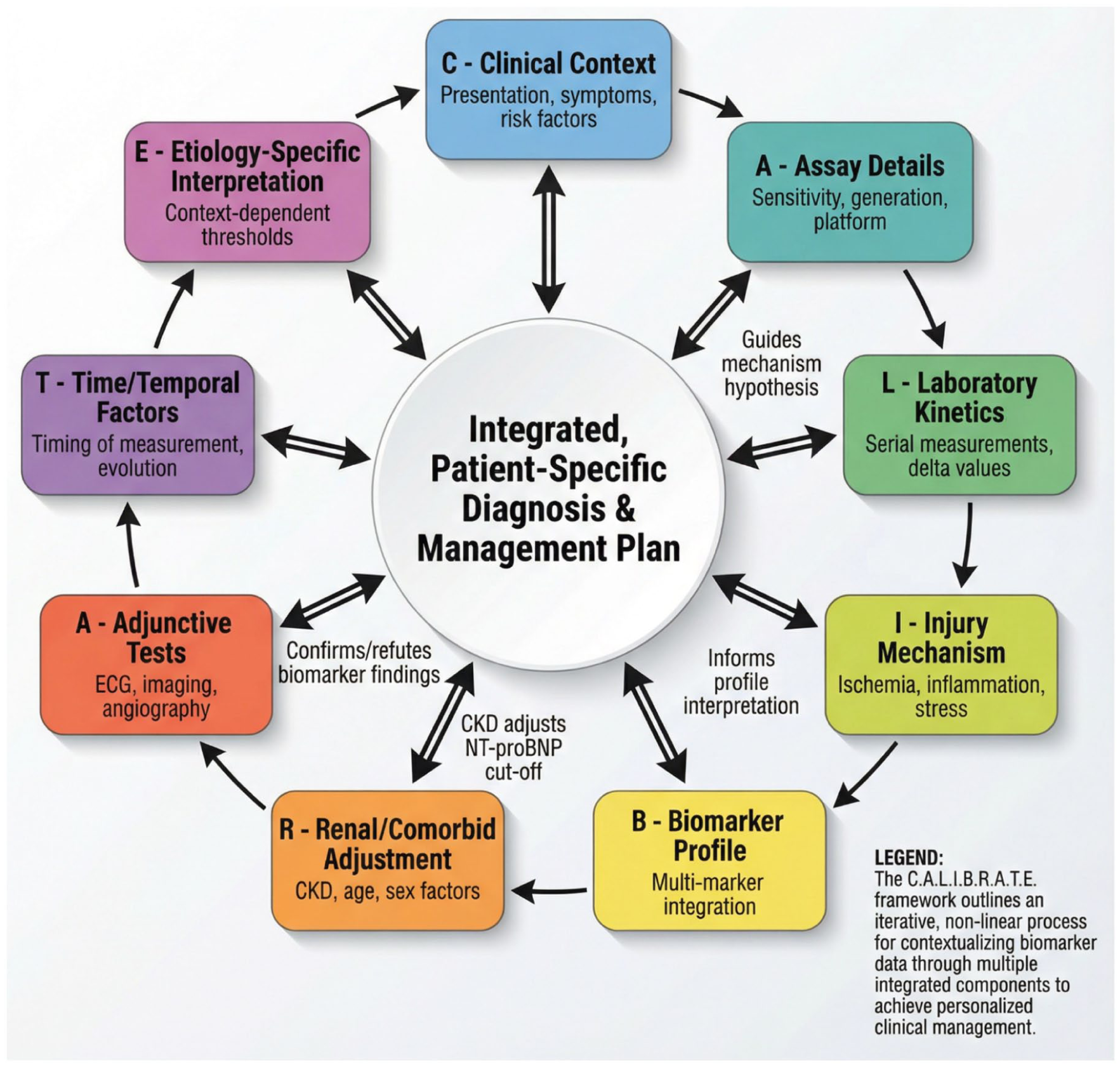
The C.A.L.I.B.R.A.T.E. framework for contextual biomarker integration.
Comparison with Existing Integrative Approaches
The C.A.L.I.B.R.A.T.E. framework does not exist in a conceptual vacuum. Several guideline-based algorithms, multi-marker panels, and clinical decision tools have been developed to address the challenges of biomarker interpretation in cardiovascular medicine. To clarify the unique contribution of the C.A.L.I.B.R.A.T.E. framework, a direct comparison with existing approaches is warranted (Table 6).
Comparison of C.A.L.I.B.R.A.T.E. Framework with Existing Integrative Approaches.
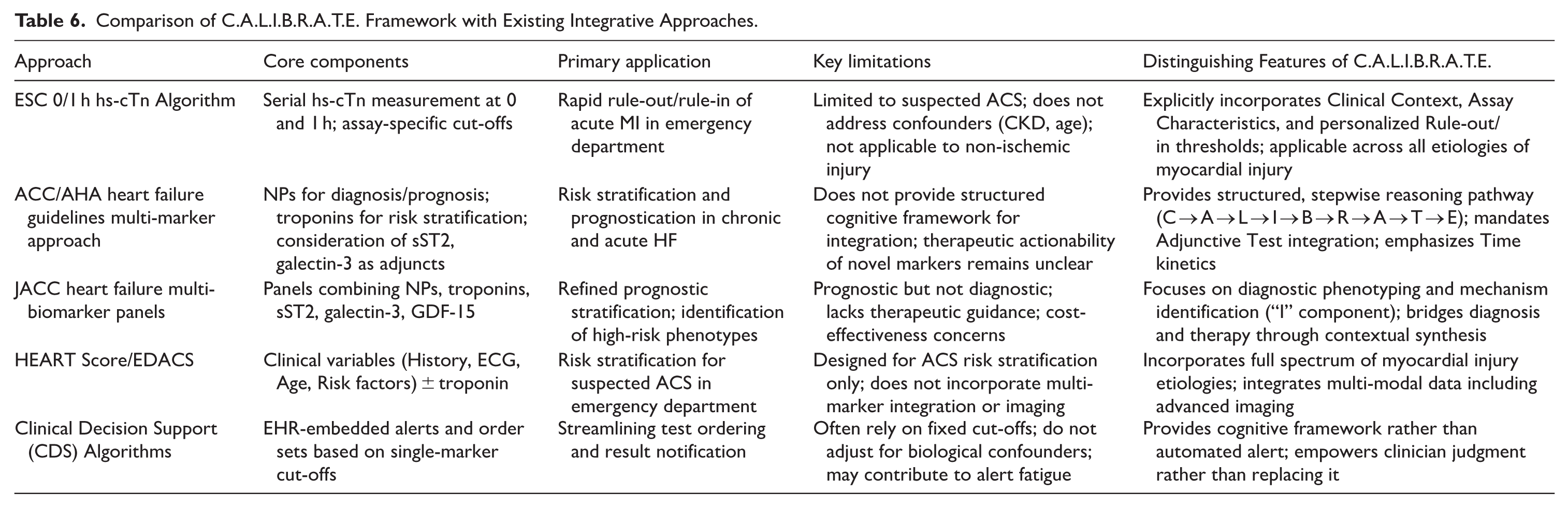
The fundamental distinction of the C.A.L.I.B.R.A.T.E. framework lies in its design as a cognitive reasoning tool rather than a diagnostic algorithm or risk calculator. Where existing approaches excel at specific, circumscribed tasks—rapid MI rule-out, HF risk stratification, or ACS probability estimation—the C.A.L.I.B.R.A.T.E. framework provides a universal scaffolding for clinical reasoning across the full spectrum of myocardial injury. It does not specify which tests to order or which cut-offs to apply; rather, it structures how clinicians should think about the results they obtain. This distinction is critical in an era of increasingly complex multi-marker panels and multi-modal imaging, where algorithmic decision-making may fail to account for patient-specific biological confounders and atypical presentations.
Moreover, the C.A.L.I.B.R.A.T.E. framework explicitly mandates the integration of adjunctive tests—particularly advanced imaging modalities such as echocardiography and cardiac MRI—as an essential component of diagnostic synthesis. Existing guideline-based algorithms often treat biomarkers and imaging as parallel or sequential investigative pathways rather than as complementary data streams to be synthesized simultaneously. By embedding the “A” (Adjunctive Tests) component within the core framework, C.A.L.I.B.R.A.T.E. ensures that biomarker interpretation is never performed in isolation from the broader clinical and imaging context.
Finally, the framework’s explicit attention to biological confounders—age, sex, renal function, and comorbidities—distinguishes it from population-derived cut-off-based approaches. The “R” (Rule-out/in thresholds) and “E” (Etiology & Comorbidities) components compel clinicians to personalize diagnostic thresholds rather than apply uniform reference limits. This addresses a persistent limitation of current guideline recommendations, which acknowledge the influence of confounders but rarely provide actionable guidance for adjusting interpretation accordingly.
Operationalizing the Framework: Clinical Vignettes
To illustrate the practical application of the C.A.L.I.B.R.A.T.E. framework, we present 3 clinical vignettes representing common yet challenging diagnostic scenarios in myocardial injury management. Each vignette demonstrates how structured, context-dependent biomarker interpretation alters clinical decision-making compared to conventional, siloed approaches.
Vignette 1: Elderly Patient with CKD and Elevated hs-cTn
•
•
•
•
•
•
•
•
•
Vignette 2: Obese Patient with Dyspnea and “Normal” BNP
•
•
•
•
•
•
•
•
•
Vignette 3: Post-COVID Patient with Persistent Troponin Elevation
•
•
•
•
•
•
•
•
•
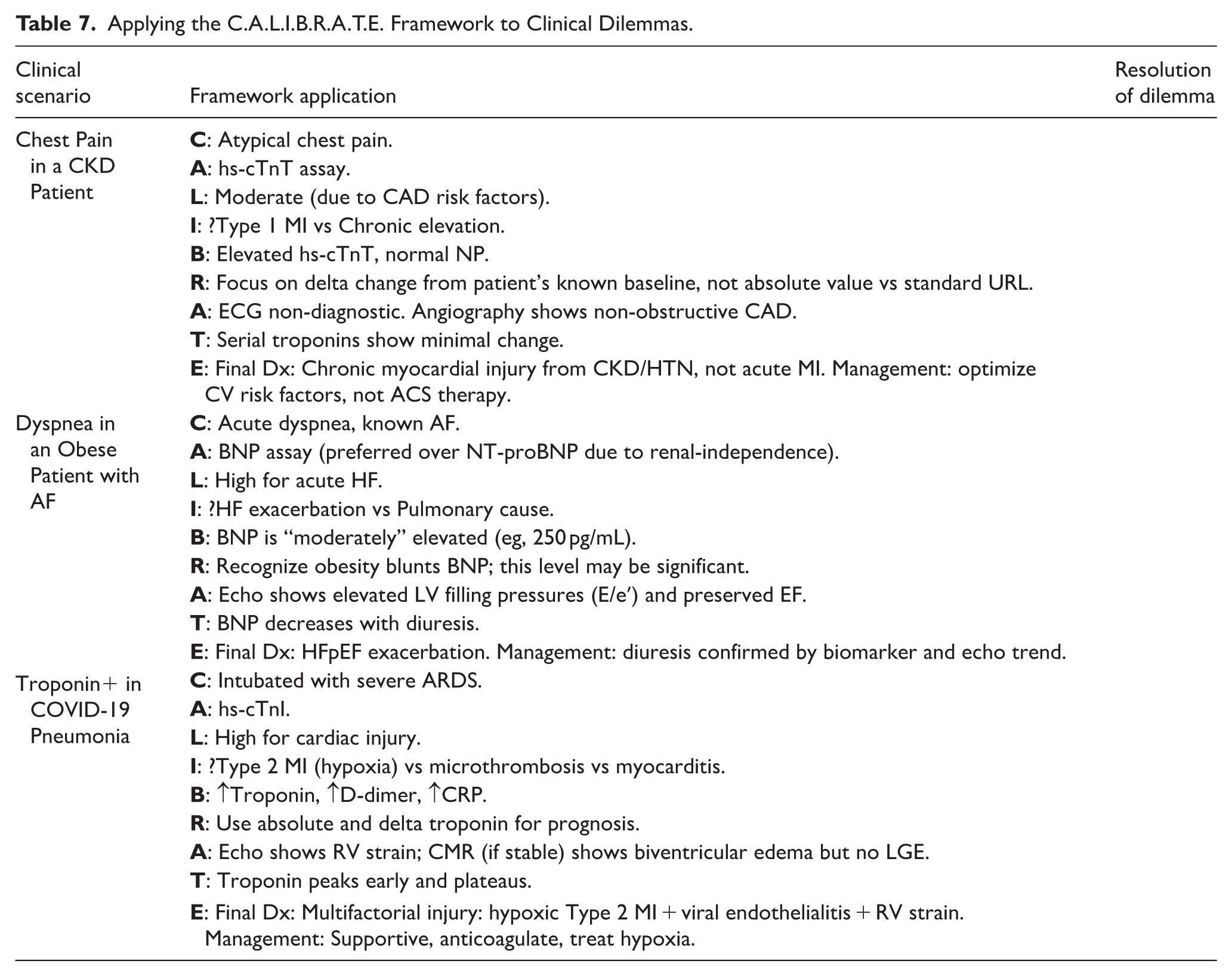
Operationalizing the Framework: Practical Applications
Table 7 illustrates how the C.A.L.I.B.R.A.T.E. framework is applied to resolve classic diagnostic dilemmas discussed earlier.
Applying the C.A.L.I.B.R.A.T.E. Framework to Clinical Dilemmas.
The C.A.L.I.B.R.A.T.E. framework represents a novel synthesis of the critical principles essential for advancing precision in the management of myocardial injury. It moves decisively beyond the outdated model of reactive, biomarker-led diagnosis to a proactive, integrative, and personalized clinical reasoning process. By providing a structured yet flexible approach to navigating biological complexity, diagnostic uncertainty, and therapeutic choice, this framework directly addresses the translational chasm. It offers clinicians a practical tool to harness the full potential of biomarker science while safeguarding against its pitfalls, thereby transforming a compendium of biomarkers into a coherent narrative of individual patient care. This integrated approach forms the essential bridge between the promising science of biomarkers and their effective, equitable, and precise application at the bedside.
Conclusions and Future Directions
This comprehensive review has undertaken a critical journey through the evolving landscape of biomarkers for myocardial injury. We have moved beyond a descriptive catalog to interrogate the foundational principles, persistent limitations, and translational challenges that define their current and future role in precision cardiology. The central, critical insight that emerges is that the path toward personalized management is not paved with increasingly sensitive individual biomarkers, but with the intelligent, contextual integration of multi-modal data.
The advent of high-sensitivity assays has irreversibly changed the diagnostic paradigm, shifting our focus from detecting overt necrosis to identifying subtle, subclinical injury. However, this enhanced sensitivity has unveiled a parallel universe of biological complexity, where elevated troponins and natriuretic peptides are as likely to signal chronic cardiorenal interplay, age-related remodeling, or systemic illness as they are to indicate an acute coronary event. The “gold standards” are thus revealed to be powerful yet imperfect tools, whose interpretation is perpetually subject to the confounder’s veto of renal function, age, sex, and multimorbidity.
Furthermore, the expanding universe of inflammatory, fibrotic, and stress biomarkers, while enriching our pathophysiological understanding, has largely failed to transition from prognostic markers to actionable therapeutic targets. Their clinical adoption is hampered by issues of specificity, a lack of evidence for therapy guidance, and the cognitive burden of interpreting complex, multi-marker panels within constrained clinical workflows. Etiology-specific puzzles—from myocarditis to COVID-19 cardiac injury—highlight that biomarkers excel at signaling the presence of injury but are often mute on its specific cause, necessitating mandatory integration with advanced imaging.
Perhaps the most formidable obstacle lies in the translational chasm between biomarker potential and real-world implementation. Economic constraints, workflow disruptions, inadequate clinical decision support, and equity of access present systemic barriers that are as consequential as any biological knowledge gap. To bridge this chasm, we have proposed the C.A.L.I.B.R.A.T.E. framework—a structured, integrative approach that places clinical context and pathophysiological phenotyping at the center of biomarker interpretation. This model provides a pragmatic pathway for clinicians to navigate complexity, personalize diagnostic thresholds, and synthesize biomarker data with imaging and clinical findings to arrive at precise, individualized diagnoses and management plans.
Future Directions: Priorities for Research and Implementation
The future of myocardial injury biomarkers will be defined not by a quest for a single novel molecule, but by advances in integration, interpretation, and implementation. Table 8 outlines key priority areas for future research and development.
Future Directions in Myocardial Biomarker Research and Clinical Translation.
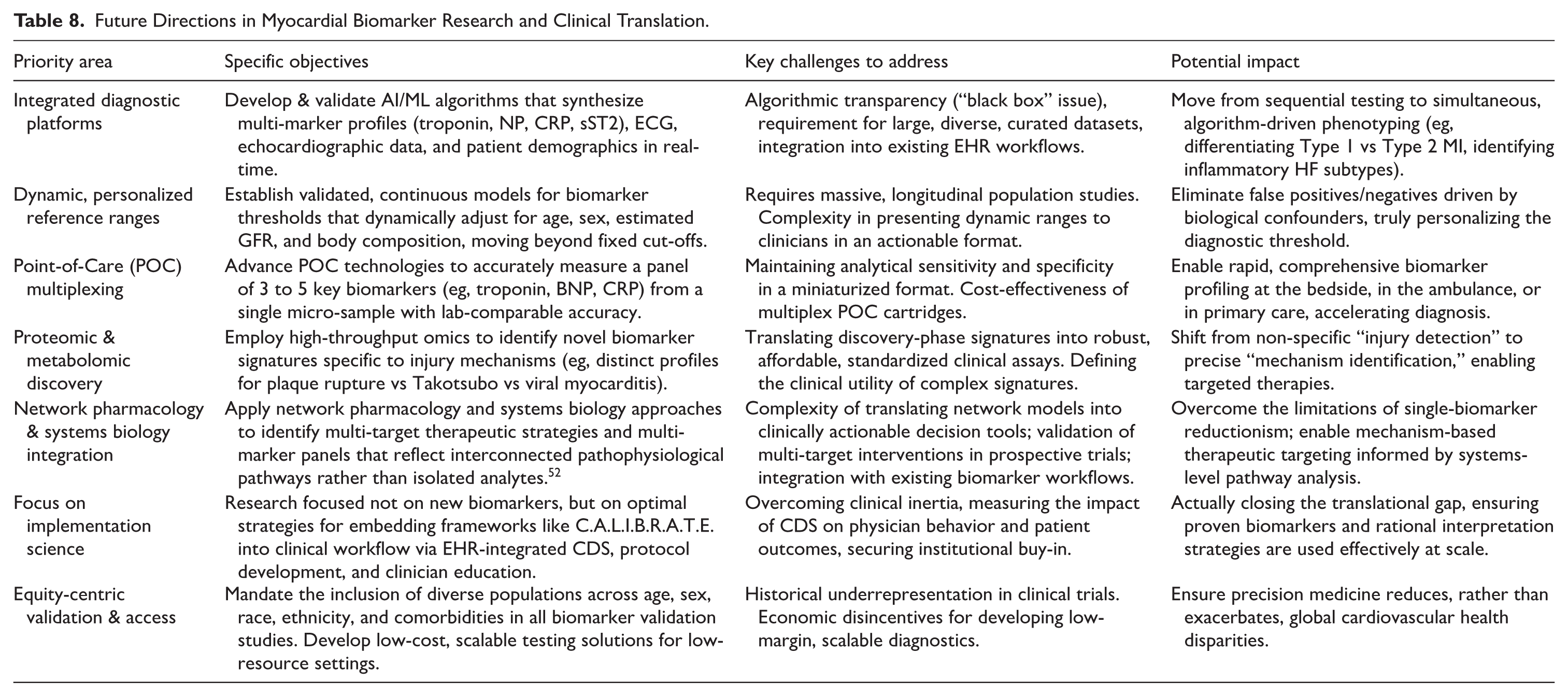
The integration of network pharmacology and systems biology approaches represents a particularly promising frontier. 52 By modeling the complex, multi-target interactions underlying myocardial injury, these methodologies can inform the rational design of multi-marker panels and identify novel therapeutic targets that address entire pathological networks rather than isolated nodes. This systems-level perspective aligns directly with the core philosophy of the C.A.L.I.B.R.A.T.E. framework: that precision is achieved through intelligent integration, not singular discovery.
The integration of wearable biosensors for continuous physiological monitoring and the exploration of circulating microRNAs (miRNAs) as early, mechanism-specific signals represent additional promising frontiers.66,67 However, their success will hinge on overcoming the very barriers outlined here: demonstrating clear clinical utility beyond novelty, establishing standardized assays, and creating a clinical pathway for acting upon their data.
In conclusion, biomarkers for myocardial injury are at a crossroads. The trajectory from here will determine whether they remain isolated, often-misinterpreted laboratory values or evolve into the core of a truly integrated, precise, and equitable diagnostic ecosystem. This future depends on a concerted shift in focus—from discovery alone to contextual integration, from analytical performance to clinical implementation, and from a one-size-fits-all model to a biologically personalized approach. By embracing this integrative paradigm, as exemplified by the C.A.L.I.B.R.A.T.E. framework, the field can fulfill the promise of precision cardiology: to deliver the right diagnosis and the right therapy to the right patient at the right time.
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data generated and associated with this research has been provided in this article.