
Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) is a widely used therapeutic procedure for pancreatobiliary disorders but is associated with a range of complications, most commonly post-ERCP pancreatitis (PEP). Post-ERCP air leak syndromes—including pneumothorax, pneumomediastinum, pneumoperitoneum, and subcutaneous emphysema—are exceptionally rare, particularly in the absence of an identifiable gastrointestinal perforation. We report the case of a 72-year-old woman who developed severe abdominal pain, acute respiratory distress, and hypoxemia 6 hours after ERCP performed for common bile duct stenting and biopsy of a suspected biliary tumor. Laboratory investigations revealed markedly elevated serum amylase and lipase, consistent with acute pancreatitis. Imaging demonstrated a moderate right-sided pneumothorax, diffuse pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum, extensive subcutaneous emphysema, and radiological features of acute pancreatitis, without evidence of duodenal or esophageal perforation. The patient was managed conservatively in the intensive care unit with bowel rest, intravenous fluids, antibiotics, supplemental oxygen, and close monitoring. Clinical and biochemical parameters improved progressively, with repeat imaging showing regression of air collections. This case highlights a rare constellation of post-ERCP complications occurring simultaneously without demonstrable perforation and underscores the importance of prompt recognition, multidisciplinary assessment, and individualized conservative management in selected stable patients.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a well-established invasive procedure widely used for the diagnosis and management of distal biliary and pancreatic duct disorders.1,2 Despite its substantial clinical utility, ERCP is associated with a spectrum of adverse events ranging from mild self-limited complications to rare but potentially life-threatening conditions. Post-ERCP pancreatitis (PEP) remains the most common complication. 1 In contrast, ERCP-related perforation is an uncommon complication, with reported incidence rates ranging from 0.3% to 2%, yet it carries significant morbidity and mortality when it occurs.1,3 Rarely, perforation or transmural air leakage may lead to extra-abdominal air leak syndromes, including pneumomediastinum, pneumothorax, pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema—collectively referred to as post-ERCP air leak (PEAL) syndromes—even in the absence of radiologically evident gastrointestinal perforation.2,4,5 Most reported cases of post-ERCP air leak syndromes describe isolated thoracic or abdominal air collections, often occurring independently of pancreatitis and frequently resolving with conservative management.6-8 However, the simultaneous occurrence of post-ERCP pancreatitis with extensive air leak manifestations, including pneumothorax, pneumomediastinum, and pneumoperitoneum, in the absence of an identifiable perforation is exceptionally rare and has been described only sporadically in the literature. We herein report a rare case of post-ERCP pancreatitis complicated by pneumothorax, pneumomediastinum, and pneumoperitoneum without radiological evidence of gastrointestinal perforation, and discuss the possible mechanisms, diagnostic considerations, and management strategies in light of previously reported cases.
Case Presentation
A 72-year-old female with a past medical history of dyslipidemia and a past surgical history of lumbar laminectomy was admitted for elective ERCP for biopsy of a suspected liver tumor and stenting of the common bile duct. She had no known drug allergies and was an active smoker. ERCP was technically difficult due to an enlarged, downward-oriented and severely fibrotic major papilla. Initial biliary cannulation attempts using a sphincterotome over a guidewire were unsuccessful for approximately 8 minutes. A freehand needle-knife biliary sphincterotomy was subsequently performed and required extension. Two false tracts occurred before successful selective biliary cannulation was achieved. Cholangiography demonstrated a long (~2 cm), malignant-appearing stricture at the common hepatic duct extending into the right and left hepatic ducts, consistent with a suspected Klatskin tumor, with marked upstream dilation of the right intrahepatic ducts. The guidewire could not be advanced into the left system. Balloon dilation of the stricture was performed (8 mm × 4 cm), followed by placement of a 10 Fr × 15 cm plastic biliary stent into the right biliary system, with satisfactory bile drainage. Brush cytology was obtained, and the sphincterotomy site was closed with a hemostatic clip. The pancreatic duct was not cannulated. The procedure was prolonged and technically complex. CO2 insufflation was used, and no prophylactic rectal NSAIDs or pancreatic stenting were administered. Approximately 6 hours after the procedure, the patient developed sudden-onset severe epigastric abdominal pain associated with acute dyspnea and oxygen desaturation. On examination, she was tachypneic with decreased air entry on chest auscultation and diffuse abdominal tenderness without guarding or rigidity. Laboratory investigations revealed marked pancreatic enzyme elevation, with a serum lipase of
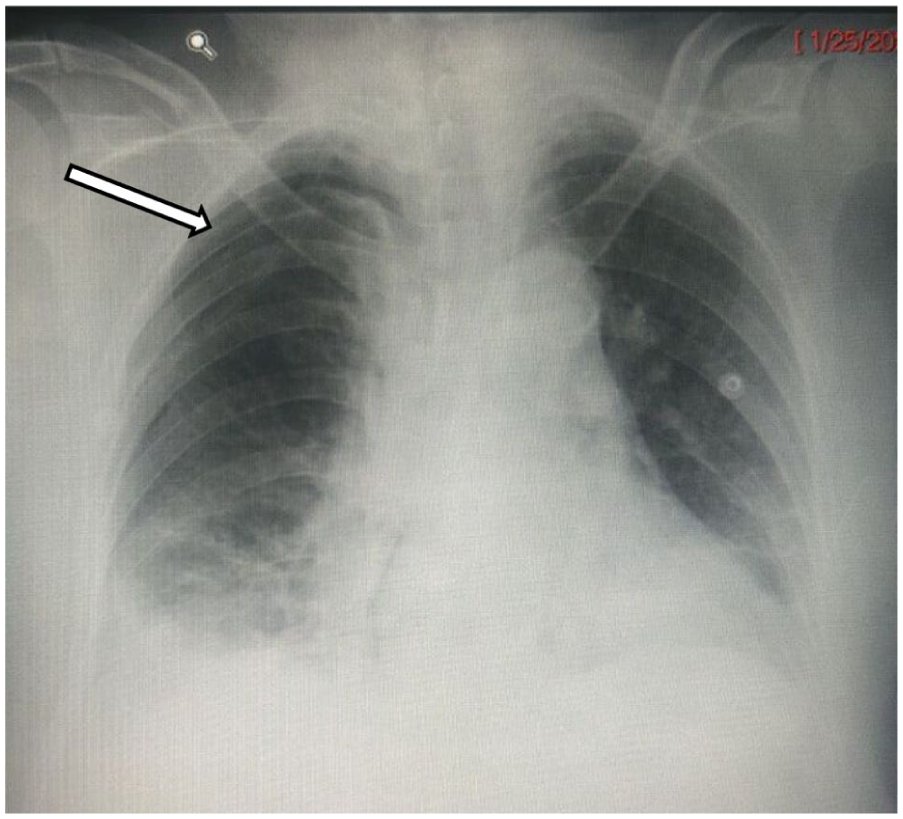
Chest X-Ray demonstrating a right-sided pneumothorax (arrow). No significant mediastinal shift is observed.
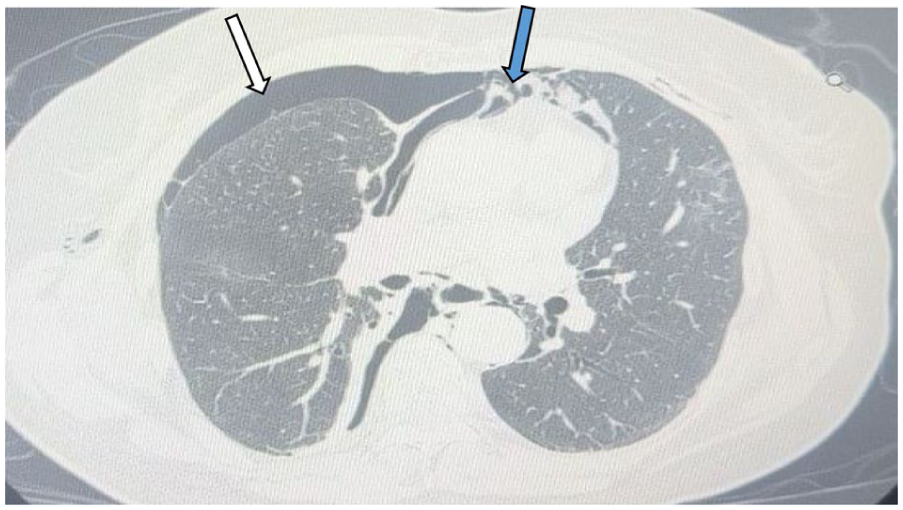
Axial CT scan image of the chest showing a moderate right-sided pneumothorax (white arrow) causing a mild deviation of the mediastinal structures toward the left with associated diffuse pneumomediastinum (blue arrow).
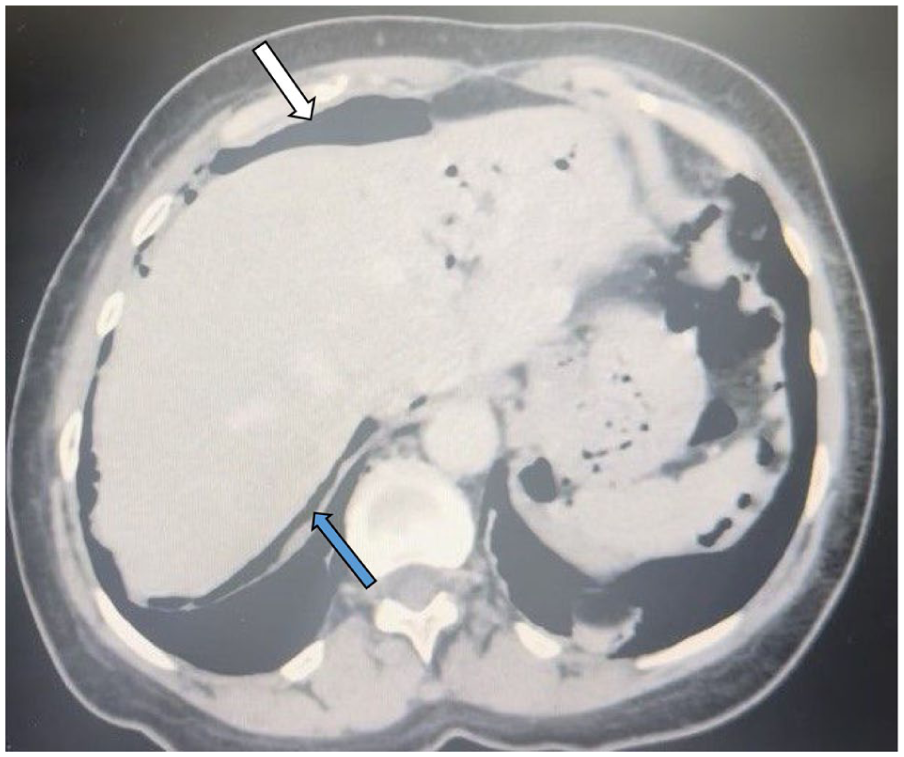
Axial CT scan image of the abdomen showing pneumoperitoneum (white arrow) and pneumoretroperitoneum (blue arrow) distributed in the subdiaphragmatic, hepatogastric, and gastrosplenic spaces, extending around the duodenum to the ligament of Treitz, the right perirenal space, and along the right paracolic gutter.
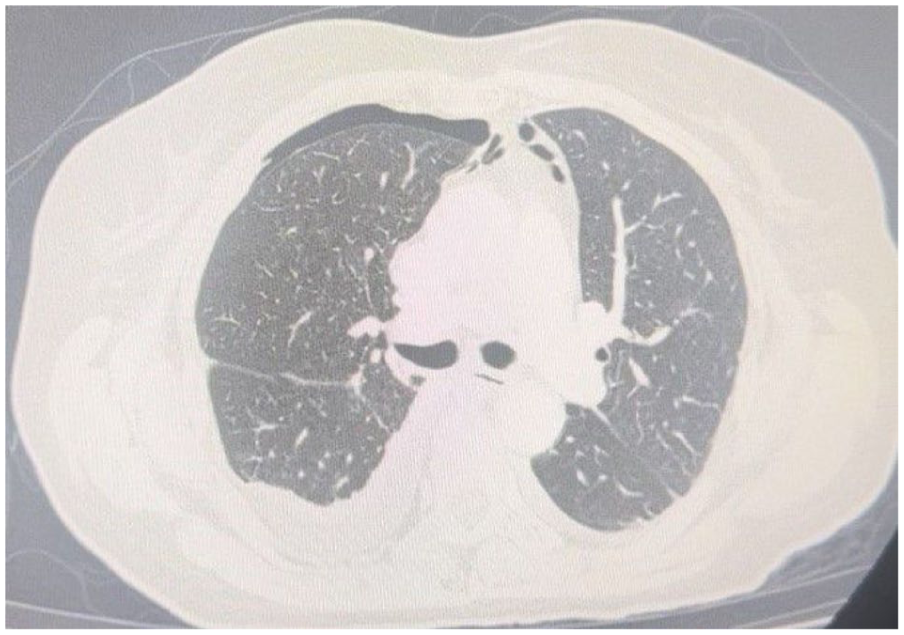
Repeat CT scan showing significant regression of pneumothorax, pneumomediastinum, pneumoperitoneum, and subcutaneous emphysema.
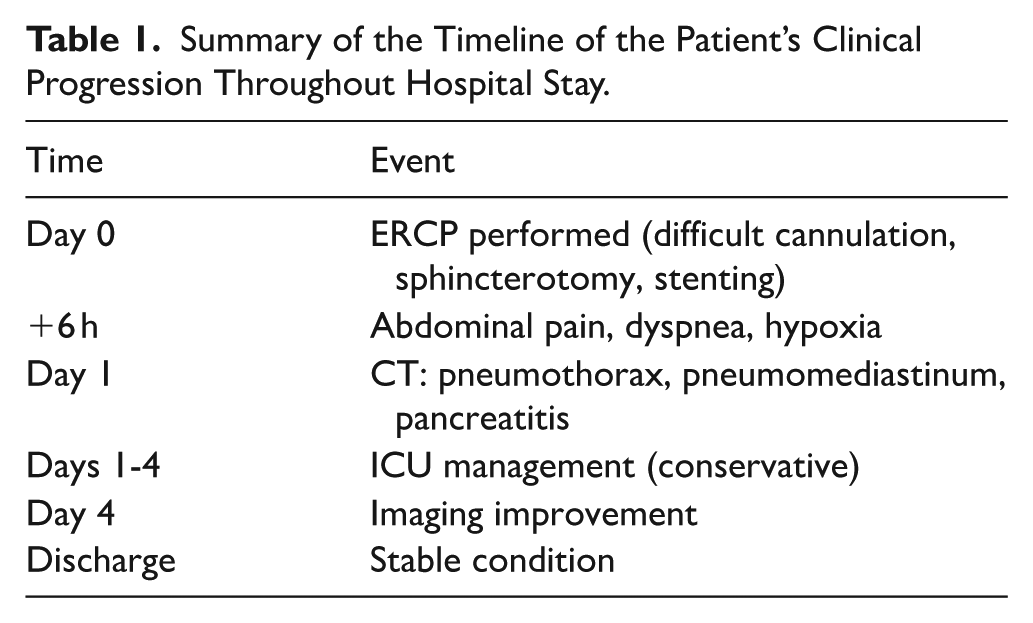
Summary of the Timeline of the Patient’s Clinical Progression Throughout Hospital Stay.
Discussion
ERCP is a standard invasive technique for revealing and management of a wide spectrum of distal bile duct disorders. 2 Since the advent of successful biliary cannulation in 1968, ERCP has evolved into a predominantly therapeutic modality, with non-invasive techniques such as magnetic resonance cholangiopancreatography and endoscopic ultrasound largely replacing its diagnostic role. 1 Despite its clinical utility, ERCP is associated with a spectrum of adverse events ranging from mild to potentially life-threatening complications.
PEP remains the most common complication and is defined by the presence of new or worsened abdominal pain accompanied by a serum amylase or lipase elevation exceeding 3 times the upper limit of normal within 24 hours of the procedure, with imaging findings consistent with acute pancreatitis when obtained. Severity is classified according to established ASGE and revised Atlanta criteria, ranging from mild disease without organ failure to severe forms characterized by persistent organ dysfunction or local complications. 1 PEP is multifactorial and arise from the interplay of patient-, disease-, and procedure-related factors. Patient-related risk factors include female sex, younger age, non-dilated common bile duct, normal bilirubin levels, obesity, congestive heart failure, CKD, suspected sphincter of Oddi dysfunction, and prior PEP. Procedure-related determinants include particularly difficult or prolonged cannulation, multiple unintended pancreatic duct cannulations, pancreatic duct contrast injection, precut sphincterotomy, pancreatic sphincterotomy, and operator inexperience, Basket use, while successful and timely biliary cannulation appears protective effect.1,9
ERCP-related perforation is an uncommon (0.3%-2%) 3 but serious adverse event, with a reported incidence of 0.08% to 0.6% and low overall mortality. 1 Clinically, perforation may present with epigastric or generalized abdominal pain associated with nonspecific symptoms such as nausea, vomiting, and dyspepsia. In rare cases, perforation or transmural air leakage may lead to pneumomediastinum, pneumothorax, and subcutaneous emphysema—collectively referred to as post-ERCP air leak (PEAL) syndrome—even in the absence of overt gastrointestinal perforation.5,10 When pneumothorax develops, patients may present with tachypnea, hypoxia, respiratory distress, or tracheal deviation, necessitating prompt recognition and management. 10 Large series and ESGE data identify sphincterotomy as the leading cause of perforation, followed by guidewire manipulation, stricture dilation, and stent-related injury. Established risk factors include advanced age, prolonged procedure duration, difficult cannulation, precut or extended sphincterotomy, periampullary diverticula, abnormal anatomy such as Billroth II reconstruction, biliary strictures, papillary stenosis, sphincter of Oddi dysfunction, and intraductal balloon dilation1,3,10,11
Infectious complications following ERCP include cholangitis, cholecystitis, and sepsis, typically related to incomplete biliary drainage or instrumentation. 1 Other rare but recognized adverse events include duodenal obstruction or restenosis, splenic injury, basket impaction, air embolism, and hepatic hematoma. 12
Post-ERCP air leak syndromes, including pneumothorax, pneumomediastinum, pneumoperitoneum, pneumoretroperitoneum, and subcutaneous emphysema, have been described only sporadically in the literature, largely in isolated case reports. Several reports document extensive multi-compartment air dissemination following ERCP or sphincterotomy without clear radiological evidence of gastrointestinal perforation, suggesting transmural air leakage or retroperitoneal tracking rather than frank rupture.2,4,5 Case series and individual reports describe predominantly right-sided or bilateral pneumothoraces frequently accompanied by pneumomediastinum, pneumoretroperitoneum, and subcutaneous emphysema, with most patients responding well to conservative management.6-8 In contrast, a minority of cases identified a definite perforation, including duodenal and esophageal injuries, often associated with more extensive air collections and occasionally requiring invasive intervention.12-14 Collectively, these reports highlight the heterogeneity of mechanisms, clinical presentations, and outcomes of post-ERCP air leak syndromes, underscoring the need for individualized assessment and management.
While reports show that pneumothorax, pneumoperitoneurm, pneumomediastium, subcutaneous emphysema and other signs of perforation, along with pancreatitis can occur post ERCP, a simultaneous occurrence of the events without visible perforation is very rare in the literature with only a few cases reported.
Several pathophysiological mechanisms have been proposed to explain the development of pneumothorax and air leak syndromes following ERCP. The most widely accepted mechanism involves disruption of the duodenal wall—most commonly related to endoscopic sphincterotomy, particularly precut or excessively deep incisions—allowing insufflated air to enter the retroperitoneal space. From there, air may dissect along contiguous fascial planes connecting the retroperitoneum to the mediastinum, peritoneal cavity, and cervical subcutaneous tissues via diaphragmatic hiatuses and perivascular sheaths. Accumulation of mediastinal air may subsequently lead to pleural rupture and pneumothorax, with severity depending on the volume and rate of air dissemination.5,8,10
Alternative routes include free intraperitoneal perforation, in which air communicates directly between the abdominal and thoracic cavities through diaphragmatic orifices, as well as transmural air entry in the absence of overt perforation through structurally weak areas such as diverticula, anastomotic sites, or areas of altered anatomy. A less common but recognized mechanism involves alveolar rupture related to increased intrathoracic pressure during hyperventilation or Valsalva maneuvers, with air tracking along perivascular sheaths to produce pneumomediastinum and secondary pneumothorax. Altered or variant anatomy such as periampullary diverticula, tumors, or surgically reconstructed anatomy may further predispose patients to these complications by facilitating aberrant air tracking.5,8,10
ERCP-related perforations are commonly categorized using the Stapfer classification, 10 with type II (periampullary) and type I (duodenal wall, distant from the papilla) perforations accounting for the majority of reported pneumothorax cases. Less frequently, air may accumulate in the retroperitoneum without a demonstrable perforation (type IV), while type III perforations typically result from guidewire-related injuries or balloon dilation within strictures. 15 Rare mechanisms include air tracking through pre-existing biliary drainage catheters or surgically altered anatomy, emphasizing the diverse pathways through which air may disseminate following ERCP.
Management of ERCP-related perforation depends on the type, size, clinical severity, and patient stability, and includes conservative, endoscopic, and surgical approaches. Conservative management is appropriate for selected patients and consists of close monitoring, bowel rest, nasogastric or nasoduodenal decompression, intravenous antibiotics, analgesia, and parenteral nutrition when oral intake cannot be resumed within several days. 10 Supportive management of ERCP-related air leak syndromes focuses on airway, breathing, and circulatory stabilization with continuous monitoring, as they usually resolve spontaneously with gradual air resorption. However, in cases of respiratory compromise or tension pneumothorax, prompt decompression with intercostal drainage is mandatory. 10 Prevention of post-ERCP pancreatitis relies on a combination of pharmacological and technical strategies. Current guidelines support the routine use of rectal nonsteroidal anti-inflammatory drugs, aggressive periprocedural hydration with lactated Ringer’s solution, and guidewire-assisted cannulation to minimize inadvertent pancreatic duct opacification. Prophylactic pancreatic duct stent placement is recommended in high-risk patients. 1
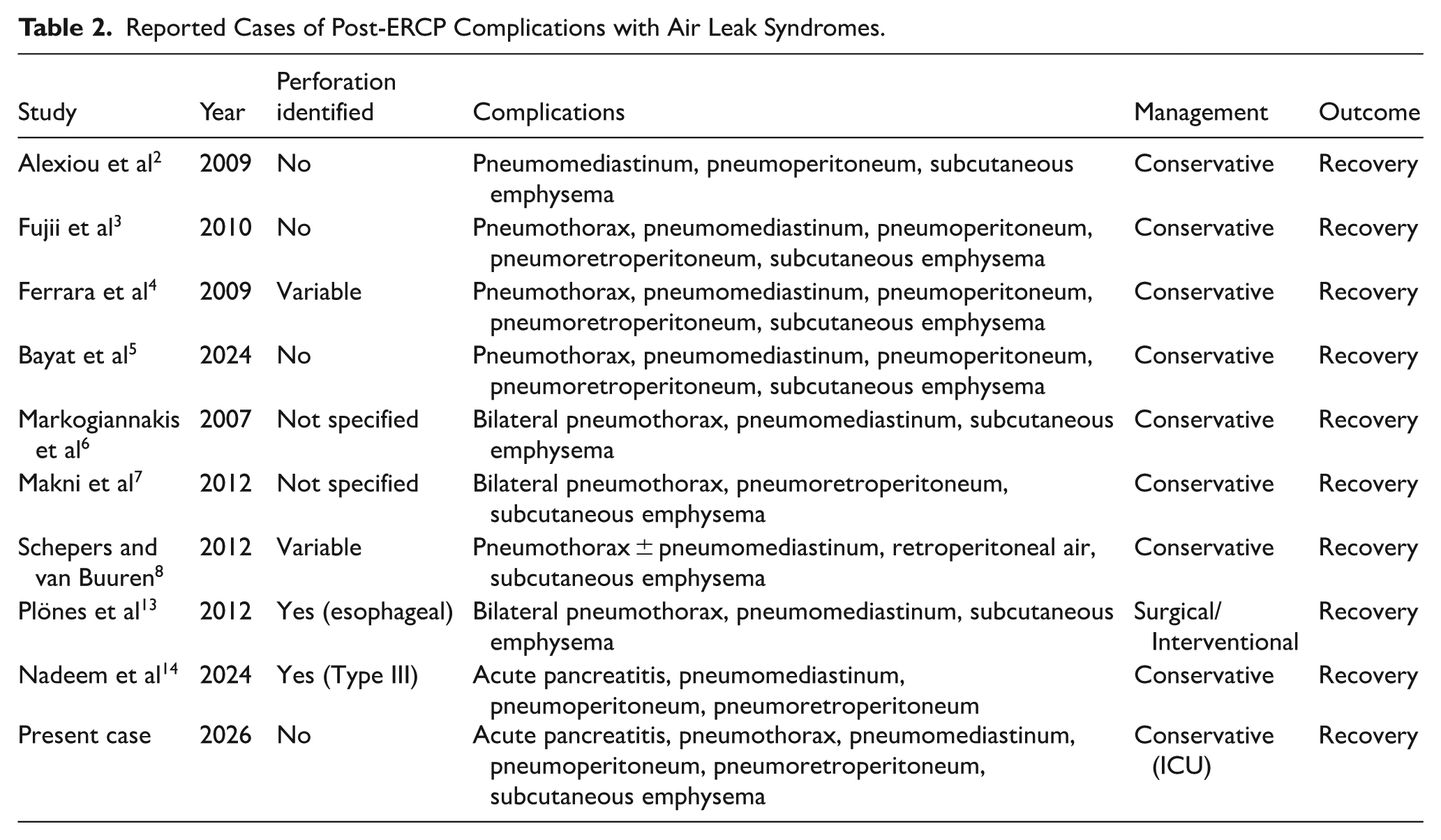
In the present case, the ERCP was prolonged and technically challenging, characterized by difficult biliary cannulation, freehand needle-knife sphincterotomy, sphincterotomy extension, and balloon dilation prior to stent placement. Prolonged procedure duration and increased technical complexity are well-established risk factors for post-ERCP pancreatitis and perforation-related air leak syndromes, likely due to cumulative papillary trauma, repeated instrumentation, and increased intraluminal insufflation. These factors may have contributed to the simultaneous development of acute pancreatitis and diffuse air leak in the absence of an identifiable duodenal perforation. Unlike previously reported cases, the present case uniquely combines acute pancreatitis with extensive multi-compartment air leak in the absence of radiological perforation, occurring after a technically difficult ERCP involving precut sphincterotomy and repeated cannulation attempts. As summarized in Table 2, most previously reported cases of post-ERCP air leak syndromes describe isolated or multi-compartment air dissemination without associated pancreatitis and frequently without identifiable gastrointestinal perforation. In contrast, cases combining acute pancreatitis with extensive air leak are exceedingly rare and are typically associated with a demonstrable perforation. Our case is unique in demonstrating the simultaneous occurrence of acute pancreatitis and diffuse thoracoabdominal air leak in the absence of radiological evidence of perforation, further supporting the hypothesis of transmural air leakage or retroperitoneal air dissection rather than frank luminal rupture. This has been rarely reported in the literature (Table 2).
Reported Cases of Post-ERCP Complications with Air Leak Syndromes.
This report has several limitations. First, as a single case report, generalizability is inherently limited and causal relationships between ERCP-related factors and the observed complications cannot be definitively established. Second, although no perforation was identified on contrast-enhanced CT imaging, a small or transient microperforation cannot be completely excluded, as such defects may seal spontaneously or remain below the resolution of imaging modalities. Third, procedural details such as insufflation type and exact intraprocedural pressures were not fully documented, which may have contributed to the development of the air leak syndrome. Finally, while our patient had a favorable outcome with conservative management, this approach may not be applicable to all patients, particularly those with hemodynamic instability or signs of peritonitis.
Conclusion
This case illustrates a rare but important constellation of post-ERCP complications, combining acute pancreatitis with extensive air leak manifestations involving the thoracic and abdominal compartments. Although alarming on imaging, such findings do not invariably indicate overt gastrointestinal perforation and may result from retroperitoneal air dissection or transmural air leakage along fascial planes. Careful clinical assessment, correlation with imaging, and close monitoring are essential to guide management and avoid unnecessary surgical intervention. Most patients, including ours, can be successfully managed with a conservative, multidisciplinary approach when hemodynamically stable and without signs of uncontrolled sepsis or peritonitis. Increased awareness of this rare presentation may facilitate early recognition, appropriate risk stratification, and optimal outcomes following ERCP.
Footnotes
Ethical Considerations
Case reports are exempted from ethical approval at our institution.
Consent to Participate
A signed written informed consent was obtained from the patient prior to manuscript submission
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon request from authors.