
Abstract
Glucagon-like peptide-1 receptor agonist liraglutide is widely used in type 2 diabetes mellitus and obesity and is generally considered non-hepatotoxic, with only rare reports of idiosyncratic liver injury. We report the case of a 58-year-old obese woman with type 2 diabetes who developed marked hepatocellular injury 12 weeks after initiating liraglutide therapy, with alanine aminotransferase (ALT) 876 U/L and aspartate aminotransferase (AST) 702 U/L after exclusion of alternative causes. Liver enzyme levels improved rapidly following drug discontinuation. A supervised rechallenge resulted in recurrence of severe transaminitis (ALT 1245 U/L, AST 980 U/L) within 10 days, with RUCAM score of 11 supporting a highly probable drug-induced liver injury. This case highlights a rare but definite idiosyncratic hepatocellular injury associated with liraglutide. Prompt recognition, discontinuation, and avoidance of rechallenge are essential. Further pharmacovigilance is warranted to better characterize incidence and mechanisms and guide safe clinical use of GLP-1 therapies in practice settings.
Keywords
Introduction
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs), such as liraglutide, are widely used in type 2 diabetes mellitus and obesity for their glucose-lowering and weight-reducing effects. Liraglutide, a once-daily injectable agent approved in 2010, mimics endogenous incretins to enhance insulin secretion and delay gastric emptying. These recombinant peptide drugs undergo minimal hepatic metabolism, and large clinical trials have not identified hepatotoxicity signals. Liraglutide has shown benefit in nonalcoholic steatohepatitis, improving liver enzymes and histology without worsening outcomes. Common adverse effects include gastrointestinal symptoms, while pancreatitis is rare.
Overall, GLP-1 receptor agonists have not been convincingly associated with clinically apparent liver injury. 1 Nonetheless, idiosyncratic drug-induced liver injury (DILI) can occur with virtually any medication. Liraglutide-induced hepatotoxicity is exceedingly rare and has been reported mainly as isolated case reports, typically presenting as hepatocellular injury that resolves after drug discontinuation; only a limited number of cases have been described in the literature.2-4 As large trials and registries have not identified GLP-1 RAs as hepatotoxic, the true incidence and mechanism of liraglutide-related liver injury remain unclear.1,4
This case adds important evidence to the existing literature by providing robust support for causality, including a typical hepatocellular DILI pattern with onset 12 weeks after initiation of liraglutide, rapid improvement after drug withdrawal, and reproducible ALT/AST elevation upon rechallenge, resulting in a RUCAM score of 11. Positive dechallenge and rechallenge findings are rarely documented in previously reported cases.2,4 Unlike earlier reports involving younger patients or individuals with hepatic steatosis, our patient was an older obese woman with type 2 diabetes but without known preexisting liver disease, suggesting that liraglutide hepatotoxicity may also occur in typical metabolic syndrome populations. Given its known benefits in fatty liver disease, this paradoxical injury is notable. 1 This report contributes an additional highly probable case to the limited literature and emphasizes the importance of clinical vigilance, even with agents generally considered hepatoprotective.
Case Presentation
A 58-year-old obese (BMI = 34.2 kg/m2) female patient presented to the clinic with fatigue, malaise, and mild right upper quadrant pain and tenderness for two weeks. The patient denied any history of fever, new-onset rash, arthralgia, pruritus, or change in stool or urine color. Her past medical history included type 2 diabetes mellitus for 5 years, controlled with metformin (2000 mg/day). She had no history of liver disease, alcohol use or toxin exposure.
Liraglutide was initiated for diabetes and weight management 12 weeks prior to presentation. The dose had been escalated per standard protocol to 1.8 mg daily, which she had been receiving for 6 weeks. She reported no use of over-the-counter medications, herbal supplements, or acetaminophen.
Vital signs were normal. She was afebrile and anicteric. Abdominal exam revealed mild tenderness in the right upper quadrant without hepatosplenomegaly or ascites. There were no stigmata of chronic liver disease.
Chronological Summary of Key Laboratory Values

Liver enzymes dropped dramatically after discontinuation of liraglutide (Figure 1). Symptoms resolved within the first week. Given the suspicion the Drug-Induced Liver Injury, a decision regarding further management was required. The patient had previously failed or demonstrated intolerance to multiple alternative glucose-lowering agents, including sulfonylureas (hypoglycemia episodes), SGLT2 inhibitors (genitourinary infections), and DPP-4 inhibitors (inadequate glycemic control). The patient’s HbA1c remained persistently above 9.5% despite maximal-dose metformin (2000 mg daily) and lifestyle modifications. Liraglutide had provided superior glycemic control (HbA1c reduction from 9.8% to 7.2%) and significant weight loss (6.5 kg over 12 weeks) compared to previously attempted agents. Alternative GLP-1 receptor agonists (exenatide, dulaglutide, semaglutide) were not available in our region at the time of management due to supply chain restrictions and formulary limitations. Given the patient’s strong preference to avoid insulin therapy (due to fear of injections, weight gain, and hypoglycemia risk), and after thorough discussion of risks and benefits, a decision of supervised rechallenge was made after 8 weeks of liver function test normalization with close monitoring. Graphical timeline of serum ALT and AST levels (A line graph showing time on the x-axis (spanning from baseline to 30 days post-2nd cessation) and enzyme levels on the y-axis (log scale may be considered). Two steep peaks corresponding to initial presentation and rechallenge are evident, with valleys during drug-free periods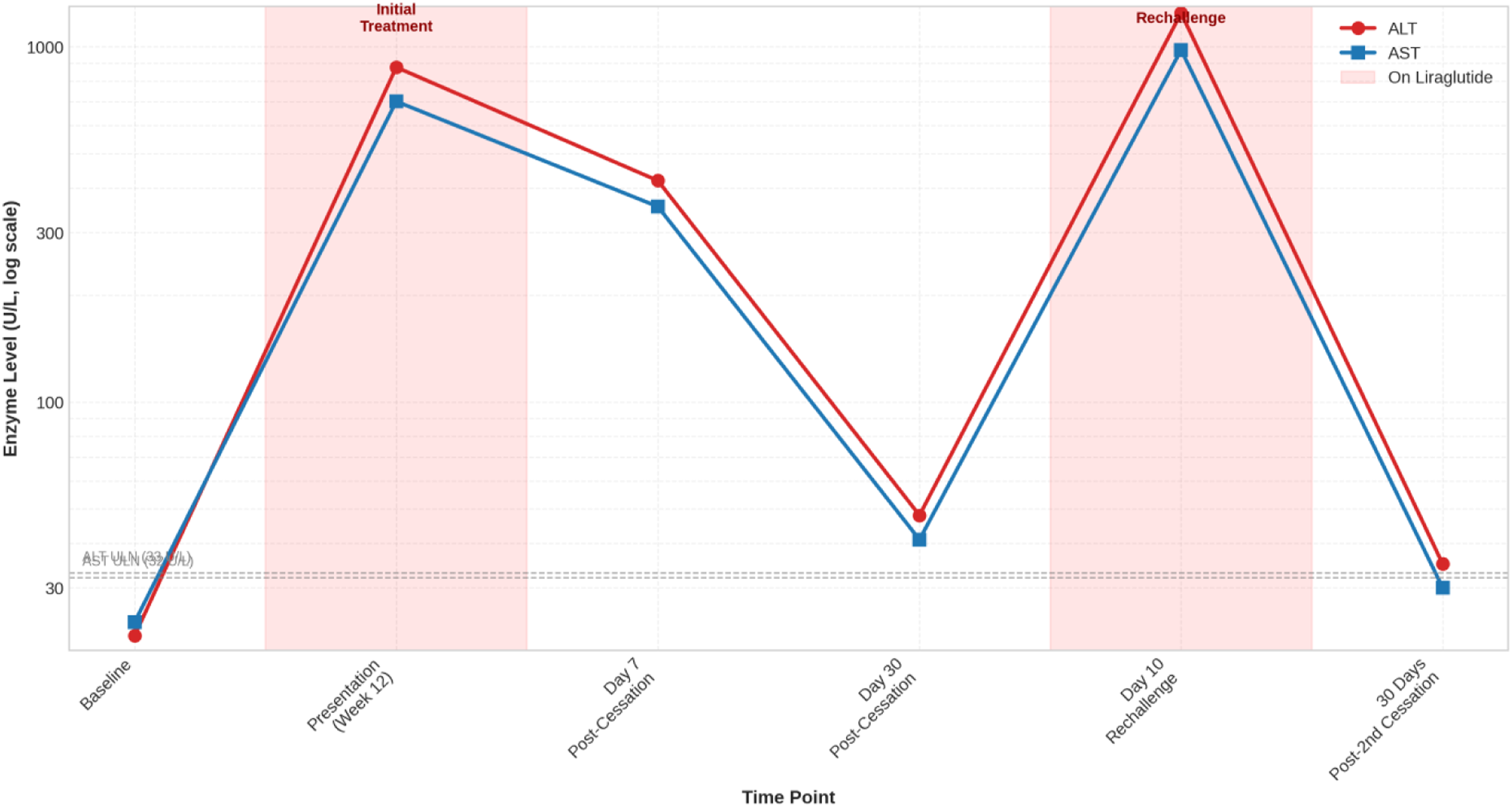
Prior to rechallenge, written informed consent was obtained specifically for the procedure, with explicit documentation that the patient understood: (a) liraglutide was the suspected cause of her prior liver injury; (b) re-administration carried a risk of recurrent, potentially more severe or fulminant liver injury, including acute liver failure; (c) there was no guarantee of recovery should severe injury recur; (d) alternative treatment options (including insulin) were available but had been declined after shared decision-making; and (e) she could withdraw consent at any time. The consent form was countersigned by an independent physician witness not involved in the patient’s care. The patient verbally affirmed her understanding of these risks on three separate occasions prior to initiation of rechallenge.
Liraglutide was restarted at 0.6 mg daily. Within 7 days, the patient reported recurrence of fatigue. Blood tests on day 10 of rechallenge demonstrated a rapid and dramatic recrudescence of transaminitis: ALT 1245 U/L, AST 980 U/L, ALP 125 U/L, R ratio 31.4, and total bilirubin 1.8 mg/dL, indicating severe hepatocellular injury (Table 1, Figure 1). The drug was permanently discontinued, with subsequent normalization of liver enzymes over the following month.
The case was evaluated using the Roussel Uclaf Causality Assessment Method (RUCAM). The chronology (score +2), dramatic improvement on discontinuation (+3), positive rechallenge (+2), exclusion of alternative causes (+2), and lack of known hepatotoxicity for the drug (-0) yielded a total score of 11, categorizing the association as “highly probable. (A completed RUCAM form is provided as Supplemental Material S1.)
Discussion
No clear class effect has been established. Liraglutide is the most frequently reported GLP-1 RA, likely reflecting longer and broader use, while only isolated cases have been described with other agents such as exenatide. Large trials of newer agents, including semaglutide and dulaglutide, have not demonstrated hepatotoxicity signals. This suggests that any risk is rare and likely agent- or patient-specific rather than a true class effect, supporting an idiosyncratic mechanism. 1
Summary of Published Cases of Liraglutide-associated Hepatocellular Injury

Including the present case, 7 case reports of liraglutide-associated liver injury have been reported in the published literature. The reported cases span multiple geographic regions, including Europe, the United States, and the Middle East, with no clear regional predilection. Ages ranged roughly 30–64 years, with female predominance. Liraglutide indications were diabetes or weight loss. Liver injury emerged after several weeks to a few months of therapy (ranging roughly 12–24 weeks). All cases exhibited a hepatocellular injury pattern: ALT and AST were markedly elevated (commonly in the hundreds to low thousands U/L) with high R ratios (often >5) and only mild to moderate bilirubin elevations. Extensive workup in each patient excluded viral hepatitis, metabolic liver diseases, and autoimmune hepatitis (serologies and imaging were normal). Liver biopsy, when performed (e.g. in Lai et al.), showed portal and lobular inflammation with eosinophils, consistent with an idiosyncratic drug reaction. All cases improved promptly after liraglutide was discontinued (with or without supportive therapy such as N-acetylcysteine); liver enzymes fell over days to months and eventually normalized in every patient. No patient required liver transplantation or died. Causality assessment (RUCAM scores, where reported) was in the “probable” range (e.g. RUCAM=8 in Lai et al.).2-7 A previous systematic review found only 4 similar cases in the literature up to 2022. Prior clinical trials of liraglutide have shown no significant hepatotoxicity signal, and several nonalcoholic steatohepatitis (NASH) studies have demonstrated improvements in liver enzymes and histology.4,8
Our case is consistent with previously reported liraglutide-associated hepatocellular injury, with metabolic comorbidities, marked ALT/AST elevation, and prompt recovery after drug discontinuation. It additionally provides supportive causal evidence through a documented positive rechallenge, with recurrence of significant transaminitis within 10 days and resolution after permanent withdrawal, supported by a RUCAM score of 11 indicating a highly probable relationship. Unlike several earlier case reports involving NAFLD or suspected steatosis, our patient had no known pre-existing liver disease, suggesting that this reaction may also occur in individuals without baseline hepatic abnormalities. We acknowledge the ethical complexity of this rechallenge, particularly in light of the more severe recurrent injury despite a lower initial dose. This observation suggests a sensitization phenomenon rather than a simple dose-dependent effect, reinforcing the idiosyncratic, immune-mediated nature of this reaction. This outcome, while diagnostically informative, also underscores why rechallenge is generally contraindicated and should only be undertaken in exceptional circumstances with rigorous safeguards. Overall, this case strengthens prior observations by adding rechallenge-based confirmation within the spectrum of rare idiosyncratic liraglutide-associated liver injury.2-8
The mechanism of injury remains speculative. Liraglutide has minimal hepatic metabolism (it is degraded by proteases) and was not thought to have inherent hepatotoxic potential. 1 Its benefits in NASH are well documented: for example, the LEAN trial (Lancet 2016) showed improved NASH histology with liraglutide, and patients generally have stable or improved liver enzymes on therapy. Paradoxical liver injury despite these hepatoprotective effects suggests an idiosyncratic reaction in susceptible individuals. Immune-mediated mechanisms are plausible. Kern’s case had prominent eosinophils and plasma cells on biopsy, 2 and Maor demonstrated that the patient’s lymphocytes had a toxic response to liraglutide in vitro. Cytokine analyses in that case showed marked elevations (e.g. TNFα 26×ULN). 3 Taken together, these findings hint at an immune-mediated or hypersensitivity reaction in rare patients. Genetic predisposition (HLA type) or prior sensitization to GLP-1 analogs might play roles, but no consistent risk factors have emerged. Metabolic stress (e.g. on a fatty liver) is another hypothesis, although several cases had minimal steatosis. Notably, cases have occurred both in patients with (Salehi) and without (Lai) known NAFLD.4,7 Liraglutide’s mechanism of action (GLP-1 receptor agonism) does not directly involve hepatic enzymes or CYP pathways. Thus, a classic dose-dependent toxicity is unlikely. Instead, immune idiosyncrasy is the leading hypothesis: the drug or its metabolites might bind to liver proteins and trigger an immune attack in rare predisposed hosts. Alternatively, off-target effects on mitochondrial or metabolic pathways have been postulated for other incretins, though evidence is lacking for liraglutide specifically. In summary, these cases do not imply a general toxic effect of liraglutide on the liver, but rather a stochastic idiosyncratic phenomenon.
Inclusion of additional reports, including the present case, brings the total number of published cases to seven, highlighting the rarity and likely underrecognition of liraglutide-associated hepatotoxicity. The absence of a signal in large clinical trials suggests these events represent sporadic idiosyncratic reactions. However, the consistent hepatocellular pattern and reproducibility on rechallenge, as observed here, support a causal relationship. Clinicians should remain vigilant and promptly discontinue liraglutide in cases of unexplained transaminitis. Rechallenge with a suspected hepatotoxin is ethically complex. Generally, rechallenge is discouraged due to risk. In this case, we performed a carefully monitored rechallenge because of the therapeutic need and high suspicion, and it provided clear diagnostic evidence. Clinicians should only consider rechallenges in exceptional circumstances (e.g. no alternatives and clear patient consent) and with intensive monitoring. Our experience shows it can be diagnostic: the rapid relapse of liver injury on a low dose confirmed liraglutide’s role beyond doubt.
The available evidence remains limited, consisting primarily of a small number of case reports, precluding any reliable estimation of incidence. Publication bias likely favors the reporting of more severe or atypical presentations, and causality assessments such as RUCAM are inconsistently applied. In addition, follow-up data are often limited to short-term biochemical resolution. Consequently, the true risk can not be quantified, although it appears exceedingly low.
Conclusion
Liraglutide should be recognized as a rare cause of acute hepatocellular injury, typically presenting with marked elevations in transaminases and minimal increase in bilirubin. A thorough evaluation to exclude viral, metabolic, and autoimmune liver disease is essential before attributing liver injury to the drug. If suspected, liraglutide should be promptly discontinued, as recovery is usually complete within weeks to months. Rechallenge is generally not recommended due to risk, although it may provide diagnostic confirmation in exceptional cases. While routine monitoring is not universally required, baseline and symptom-driven liver function testing may be reasonable in selected patients. All suspected cases should be reported to pharmacovigilance systems to improve understanding of this uncommon adverse effect.
Supplemental Material
Supplemental material - Liraglutide-Induced Acute Hepatocellular Injury With Positive Rechallenge: A Case Report and Literature Review
Supplemental material for Liraglutide-Induced Acute Hepatocellular Injury With Positive Rechallenge: A Case Report and Literature Review by Mohammad Adi, Ahmed Ashraf, Shohsanam Eshimova, Saidbek Husanov in Clinical Medicine Insights: Case Reports
Footnotes
Ethical Considerations
Ethical approval was not required for this case report, as it involves a single patient and does not meet the criteria for research requiring institutional review board (IRB) oversight. The use of authorized medications was consistent with clinical practice guidelines, and the management of this individual patient did not require IRB approval.
Consent for Publication
Written informed consent was obtained from the patient prior to publication of this case report and any accompanying images. Specifically, prior to rechallenge, additional written informed consent was obtained explicitly documenting that the patient understood: (a) liraglutide was the suspected cause of her prior liver injury; (b) re-administration carried a risk of recurrent, potentially more severe or fulminant liver injury, including acute liver failure; (c) there was no guarantee of recovery should severe injury recur; (d) alternative treatment options (including insulin) were available but had been declined after shared decision-making; and (e) she could withdraw consent at any time. The consent form was countersigned by an independent physician witness not involved in the patient’s care. The completed consent form is available to the Editor upon request and will be treated confidentially.
Author Contributions
All authors contributed to the writing and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data pertinent to this case report have been included in this article. Further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.