
Abstract
Background
Augmented reality navigation (ARN) has been increasingly applied in laparoscopic liver surgery to improve anatomical orientation and surgical precision. However, its clinical value compared with conventional anatomical liver resection (ALR) and non-anatomical liver resection (NALR) remains unclear.
Method
This retrospective single-center study included 96 patients with hepatocellular carcinoma who underwent laparoscopic hepatectomy from January 2019 to December 2021. Patients were divided into three groups: ARN-assisted laparoscopic nonanatomic hepatectomy (Group A, n=28), laparoscopic anatomical hepatectomy without navigation (Group B, n=35), and laparoscopic nonanatomic hepatectomy without navigation (Group C, n=33). Baseline demographic, clinical, tumor, and segmental distributions were comparable among groups. Postoperative outcomes, postoperative complications, and 36-month follow-up data were analyzed.
Result
Preoperative characteristics did not significantly differ among the three groups. Operative time was significantly shorter in Group A than in Group B (p=0.003) and Group C (p=0.039). Median intraoperative blood loss in Group A was 125ml, which was 175ml less than in Group B (p=0.048) and 75 ml less than in Group C (p=0.049). On postoperative day 7, median α-fetoprotein was lower (p=0.049) in group A (4.26 iu/ml) than in group C (5.82 iu/ml). 3-Year overall survival did not significantly differ among three groups. 3-Year tumor-free survival rates were 60.7% in group A, 62.9% in group B, and 36.3% in group C, with Group A and B showing significantly better tumor-free survival than group C (
Conclusion
In this cohort, ARN-assisted laparoscopic nonanatomic hepatectomy was associated with reduced operative time and blood loss and demonstrated short-term oncological outcomes similar to anatomical hepatectomy. These findings suggest that ARN may enhance the effectiveness of non-anatomical hepatectomy; however, confirmation in larger prospective studies is required.
Introduction
Hepatocellular carcinoma (HCC) remains a major global health challenge and is the fourth leading cause of cancer-related deaths worldwide. Its incidence continues to increase in many regions. 1 Surgical excision remains a key treatment option for HCC. Patients with preserved liver function, sufficient future liver remnant, and no distant metastases are considered optimal candidates for surgery. 2 Surgical approaches include open hepatectomy and laparoscopic hepatectomy, with minimally invasive laparoscopic techniques increasingly preferred due to their reduced surgical trauma and faster recovery.3,4 Intrahepatic micrometastasis through vascular dissemination is believed to a key mechanism underlying HCC recurrence. This biological behavior has provided the theoretical basis for anatomic liver resection (ALR), which removes the tumor-bearing portal territory.5-7 However, ALR is not suitable for all patients because it may increase the risk of postoperative liver insufficiency, particularly in those with compromised hepatic reserve. In contrast, non-anatomic liver resection (NALR), which removes the tumor with a margin but preserves more parenchyma, has been reported not to increase recurrence in selected patients with well- or moderately differentiated tumors. 8 In addition, tumors located at the junction of liver segments may receive blood supply from multiple vascular pedicles. In such cases, major anatomical resection may sacrifice excessive functional liver tissue without providing clear oncologic benefit. 9 Patients with small tumors or impaired liver function are therefore often less suitable for ALR. Importantly, the oncological advantage of ALR over NALR remains controversial, as several studies have reported inconsistent findings.8-10
Augmented reality (AR) technology allows real-time superimposition of computer-generated virtual information onto the physical surgical field without direct interaction between the user and virtual objects. 11 By enhancing intraoperative visualization, AR-based navigation systems have gained increasing attention in surgical practice. In augmented reality navigation (ARN)-assisted laparoscopic surgery, three-dimensional (3D) models reconstructed from preoperative computed tomography (CT) images are registered and overlaid onto the laparoscopic video. This integration enables visualization of complex anatomical structures within the operative field, thereby improving spatial orientation, facilitating precision dissection, and potentially reducing operative trauma. 12 Recent studies have reported encouraging clinical outcomes following the application of ARN in several surgical specialties, including hepatobiliary, neurosurgery, maxillofacial, and orthopedic surgery.13-15
Accurate delineation of the relationship between tumors and surrounding vascular structures, as well as complete tumor removal, is essential for safe and effective hepatectomy. 16 ARN provides real-time visualization of both vessels and tumors, assisting surgeons in performing precise resections, maintaining appropriate surgical margins, and potentially reducing residual microscopic disease. 17 In this respect, ARN shares certain conceptual similarities with ALR. However, direct comparisons between laparoscopic ALR with ARN-assisted laparoscopic hepatectomy remain limited, and the relative clinical benefits of these approaches are not well defined. To address this gap, we retrospectively analyzed patients with HCC who underwent different laparoscopic resection strategies. Patients were divided into three groups according to the use of ALR or ARN, and preoperative, intraoperative, and postoperative outcomes were compared to evaluate the clinical performance of each surgical approach.
Methods
Study Design
This retrospective, single-center, controlled study was conducted at the Second Clinical Medical College of Jinan University Hospital (Shenzhen People’s Hospital) in Shenzhen, China. The study protocol was approved by the hospital’s Ethics Committee, which waived the requirement of informed consent due to the retrospective design and use of de-identified data. The reporting of this study adheres to the STROCSS 2024 guideline for surgical observational studies, and the completed checklist is provided as Supplementary Table S1.
A total of 96 patients who underwent laparoscopic hepatectomy between January 2019 to December 2021 were included. The inclusion criteria were: (1) 18 years<age; (2) pathologically confirmed HCC; (3) absence of intrahepatic or extrahepatic metastases on contrast-enhanced CT or MRI; (4) preoperative Child-Pugh class A or B liver function; and (5) treatment by laparoscopic hepatectomy.
Patients were categorized into three groups according to surgical approach and use of ARN: group A, ARN-assisted laparoscopic non-anatomical hepatectomy (n=28); group B, laparoscopic anatomical hepatectomy without navigation (n=35); group C, laparoscopic non-anatomical hepatectomy without navigation (n=33). Perioperative data and 36-month postoperative follow-up outcomes were collected and analyzed (Figure 1). The patient selection process, including eligibility assessment, exclusions, and final group allocation, is summarized in the research route flow diagram (Figure 1). Research route flow diagram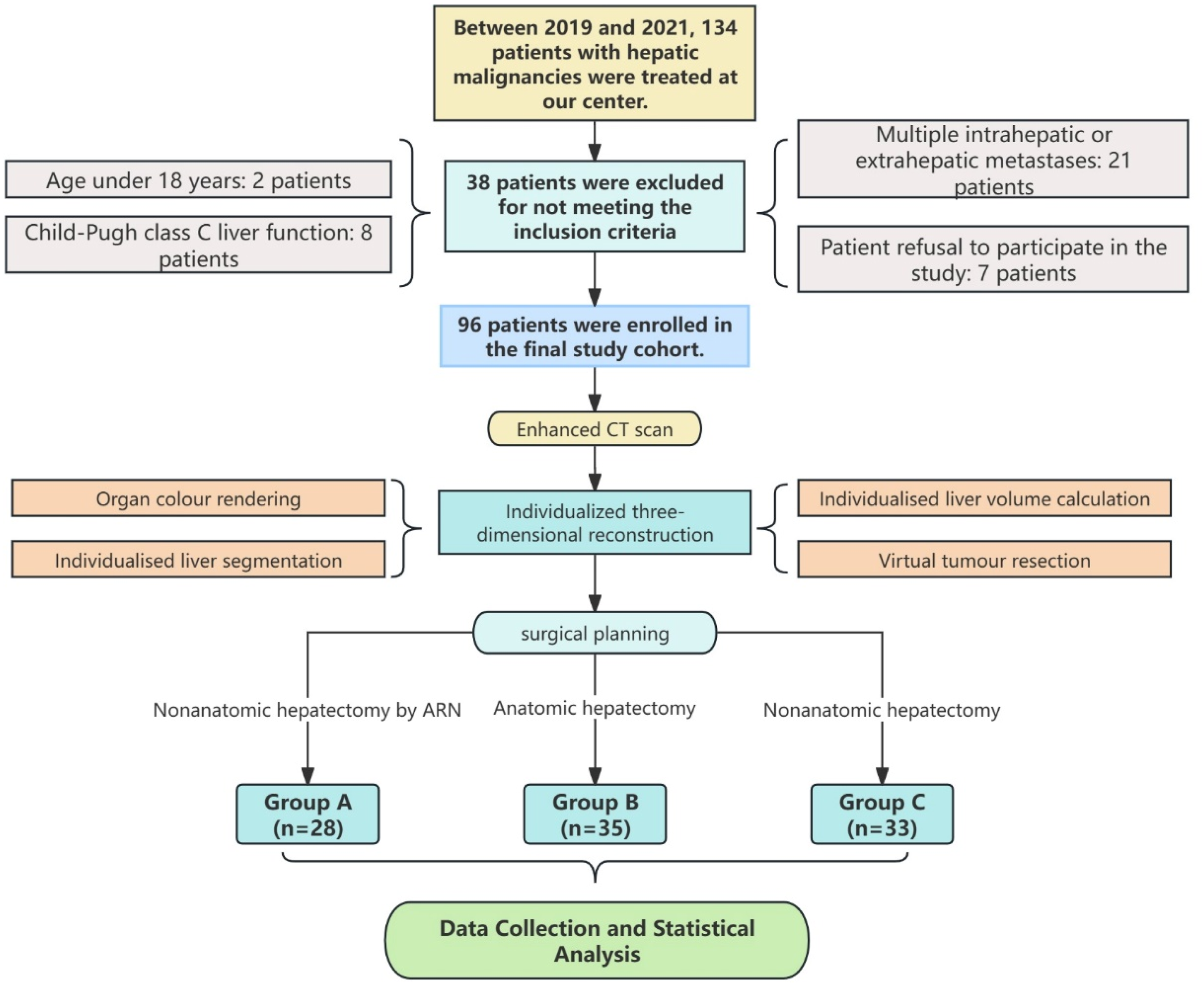
Equipment and System
A 3D Laparoscopic hepatectomy navigation system (3D-LHNS) was used in this study. The system was developed by the Shenzhen Institute of Advanced Research, Chinese Academy of Sciences team (software copyright No.2018SR840555). Intraoperative surgical videos were acquired using a 3D laparoscopy system (IMAGE1S 3D, Karl Storz, Germany) and transmitted to the 3D-LHNS, where it was integrated and calibrated with the preoperatively reconstructed 3D reconstruction model.
Preoperative Management
High-quality CT images were routinely collected before surgery, including non-contrast and multiphase contrast-enhanced liver imaging (Figure 2A). The imaging data were imported into 3D visualization software (YT-MM-3DVWorks, software copyright No. 20212211346.) for 3D reconstruction, surgical planning, and hepatic resection volume calculation (Figure 2C). Key anatomical structures, including the liver, tumor lesions, portal vein, hepatic artery, and hepatic veins, were rendered in different colors to clearly distinguish them within the reconstructed 3D model (Figure 2B). Laparoscopic hepatectomy by augmented reality navigation system. (A): Preoperative CT image and tumor location (red circle). (B): Preoperative 3D reconstruction model of the operative area and tumor. (C): Excision area design and volume calculation. (D): 3D model imported into the navigation system. (E): Import of laparoscopic surgery scenarios into the navigation system. (F): Scene of navigation-assisted hepatectomy. (G): The operating interface of the augmented reality navigation system. (H): Intraoperative virtual resection scope imaging. (I): Intraoperative real-time navigation of hepatic resection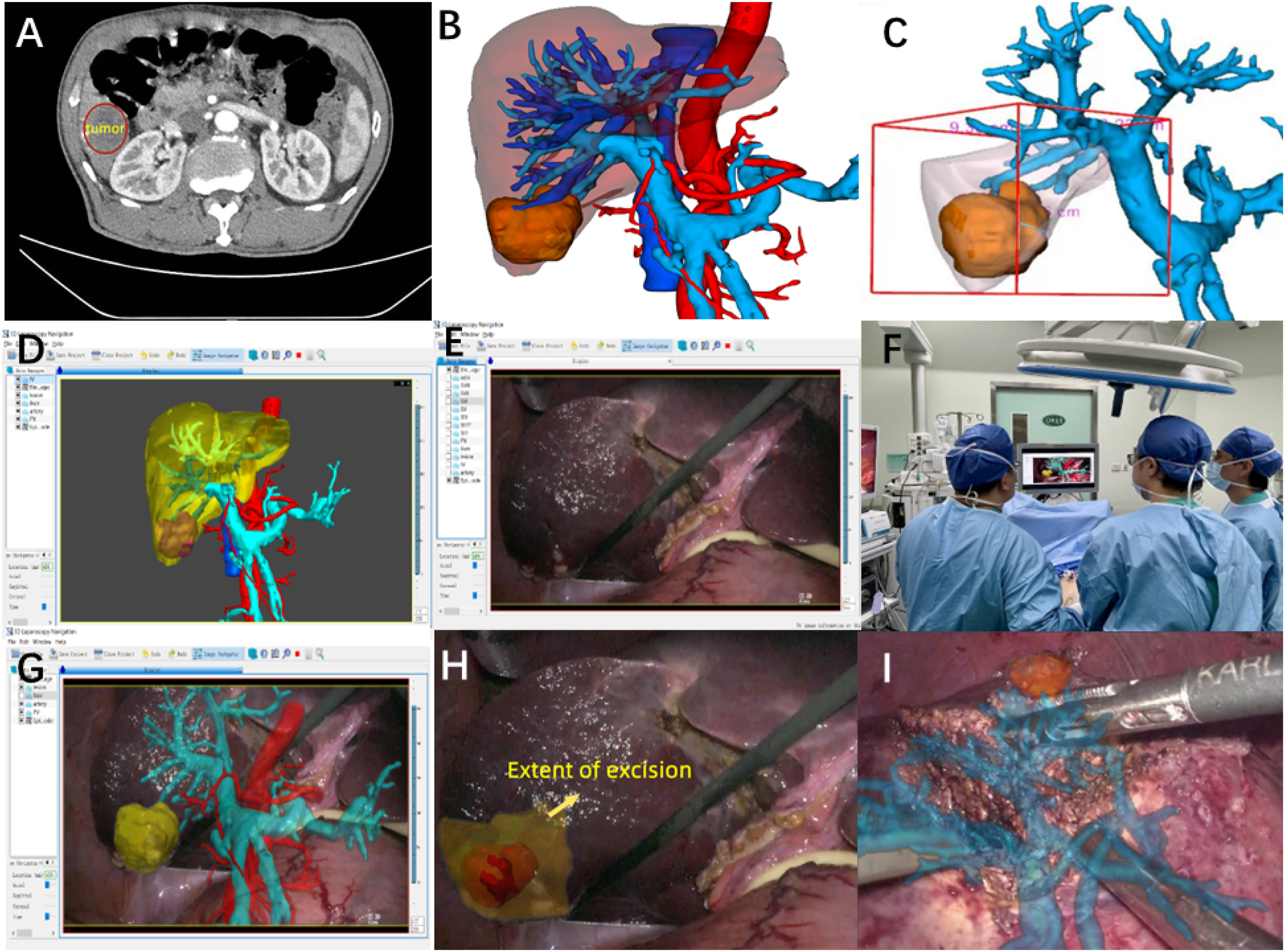
ARN-Assisted Laparoscopic Hepatectomy
The workflow of ARN-assisted laparoscopic hepatectomy is shown in Figure 2. Before surgery, the liver, tumor, and vascular structures were segmented and reconstructed into models based on preoperative CT images (Figure 2A). The laparoscope was also calibrated to obtain the intrinsic and extrinsic camera parameters. During surgery, laparoscopic images and camera parameters were used to perform dense stereo reconstruction, generating a 3D point cloud of the intraoperative surgical scene. This point cloud was registered to the preoperative liver surface,
16
resulting in a spatial transformation (Tpre-intra) that aligned the preoperative and intraoperative coordinate systems. The transformation matrix and the camera parameters were applied to the preoperative 3D model to obtain real-time AR fusion visualization (Figure 2D–G). If automated registration was not satisfactory, manual registration was performed. Under AR guidance, intrahepatic arteries, veins, bile ducts, and tumor boundaries were visualized in real time. Tumor resection was carried out according to the preoperative plan, maintaining the intended surgical margin (Figure 2H). Major vessels and bile ducts were identified, dissected, and ligated under navigation guidance until the tumor was completely removed (Figure 2I). The overall technical workflow of ARN-assisted laparoscopic hepatectomy is shown in Figure 3. The technical Route of Augmented reality-assisted laparoscopic hepatectomy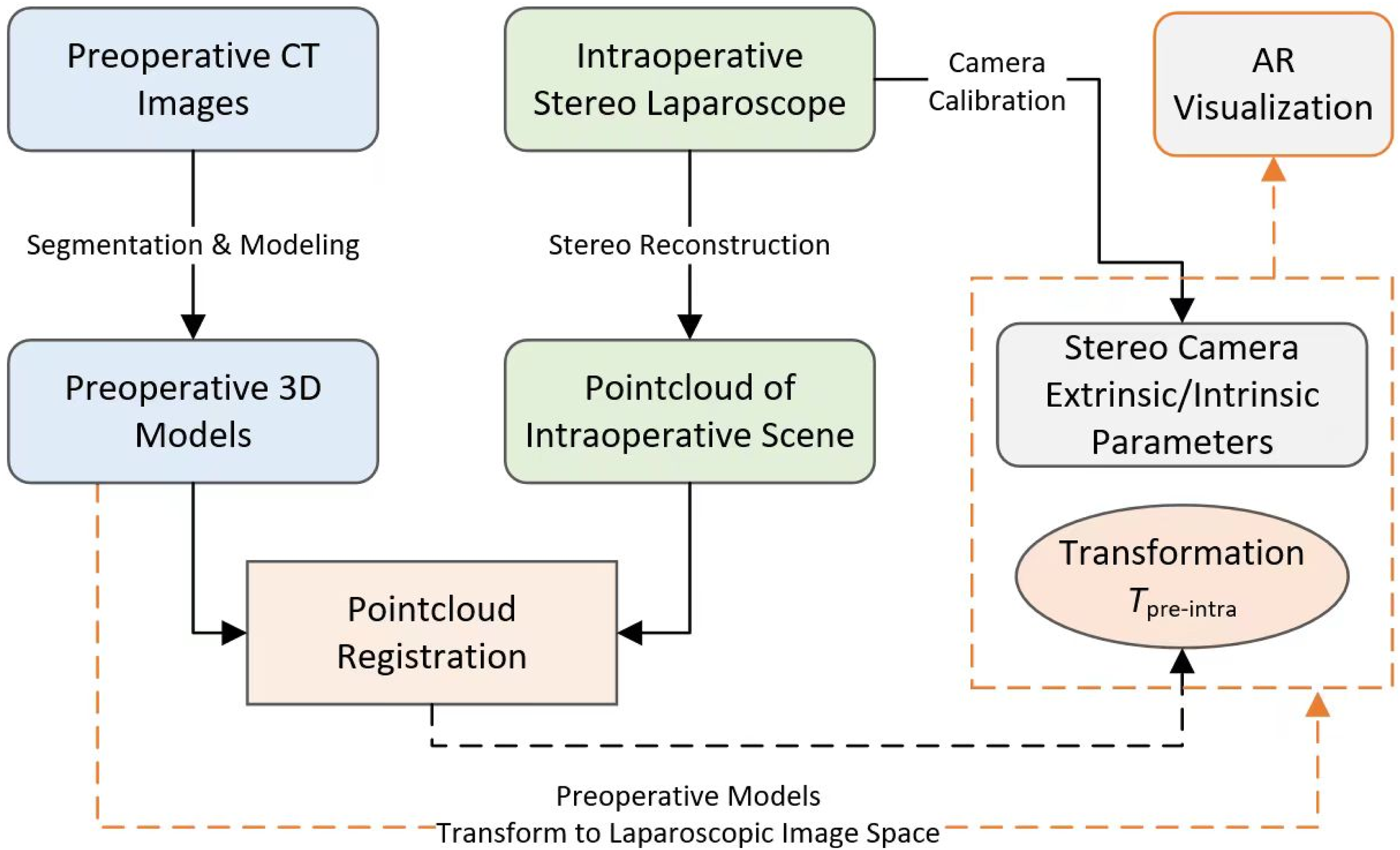
Data Collection and Processing
Demographic and Clinical Characteristics of Patients

IQR, interquartile range.
Patients underwent routine contrast-enhanced CT imaging every three months during the first postoperative year and every six months during the following two years. Patients were instructed to return to the hospital immediately if new symptoms occurred. For those who did not adhere to the schedule visit, follow-up was conducted by telephone. Follow-up data were used to generate overall survival and tumor-free curves. There were no missing data for the primary outcome variables. For secondary variables, cases with missing values were excluded from the corresponding analyses.
Statistical Analysis
Continuous data were presented as mean±standard deviation (sd) or median with interquartile range (IQR), depending on data distribution. Normality was initially assessed using the Kolmogorov-Smirnov test. Normally distributed variables were compared using the student’s t-test or Welch’s t-test when equal variances were not assumed. Non-normally distributed variables were compared using the Mann-Whitney U test. Categorical variables were analyzed using the chi-squared test or Fisher’s exact test, as appropriate. Statistical analyses were conducted using IBM SPSS Statistics version 27 software and GraphPad Prism version 10. Overall survival and tumor-free survival were estimated using the Kaplan-Meier method, and differences between groups were assessed using the log-rank test. All tests were two-sided, and a P-value<0.05 was considered statistically significant.
Results
Patients Characteristics
Tumor Distribution Across Liver Segments

P = 0.82 for inter-group comparison (chi-square test).
Laparoscopic ARN-Assisted Nonanatomic Hepatectomy
All procedures were performed by the same surgical team with extensive experience in laparoscopic liver surgery. A representative case of ARN-assisted laparoscopic non-anatomical hepatectomy for HCC located in segment VI is shown in Figure 2. The 3D visualization model showed that the lesion was located in segment VI (Figure 2B). The simulated liver resection volume was 301.95 ml, corresponding to 15.99% of the total liver volume (Figure 2C). Under intraoperative navigation guidance,, the hepatoduodenal ligament was incised, and the right portal vein branch and right hepatic artery were identified (Figure 2G). Dissection was then continued along the portal vein toward the right posterior segment, following by clamping of the right posterior portal vein branch. Hepatic parenchymal transection was performed according to the preoperative resection plan (Figure 2H). Intraoperative pathological examination confirmed HCC.
Perioperative Outcomes
Comparisons Between a and B Groups for Perioperative Outcomes, Follow-Up, and Recurrence Patterns

*Statistically significant.
Comparisons Between a and C Groups for Perioperative Outcomes, Follow-Up, and Recurrence Patterns

*Statistically significant.
Comparisons Between B and C Groups for Perioperative Outcomes, Follow-Up, and Recurrence Patterns

*Statistically significant.
The mean operative time in Group A was 256.89 ± 51.73 minutes, which was significantly shorter than in Group B (312.66 ± 84.22 min, p=0.003) and Group C (297.85 ± 90.69 min, p=0.039). The median intraoperative blood loss in Group A was 125 ml, which was significantly lower than in Group B (300 mL, p=0.048) and Group C (200 mL, p=0.049). On postoperative day 7, median α-fetoprotein levels was lower (p=0.049) in Group A (4.26 IU/ml) than in Group C (5.82 iu/ml). No significant differences were observed in other perioperative variables. There were no perioperative deaths in any groups (Tables 3-5).
Postoperative Complications and Clinical Outcomes
During postoperative hospitalization, one patient in Group A developed a lung infection, one patient in Group B developed a wound infection, and one patient in Group C developed pleural effusion. All patients recovered after appropriate treatment and were discharged in stable condition. These incidence of postoperative complications did not significantly differ among the groups.
All patients were followed for 36 months after surgery. Overall survival and tumor-free survival curves were generated based on the follow-up data. The 3-year overall survival rates were 67.9% in groups A, 65.7%, in B, and 60.6% in C were, with no significant difference among the groups (p=0.529) (Figure 4). The 3-year tumor-free rates were 60.7% in group A, 62.9% in group B, and 36.3% in group C. There was no significant difference between groups A and B (p=0.911). However, both Groups A and B demonstrated significantly higher tumor-free survival compared with group C ( Postoperative survivorship curve and Tumor-free curve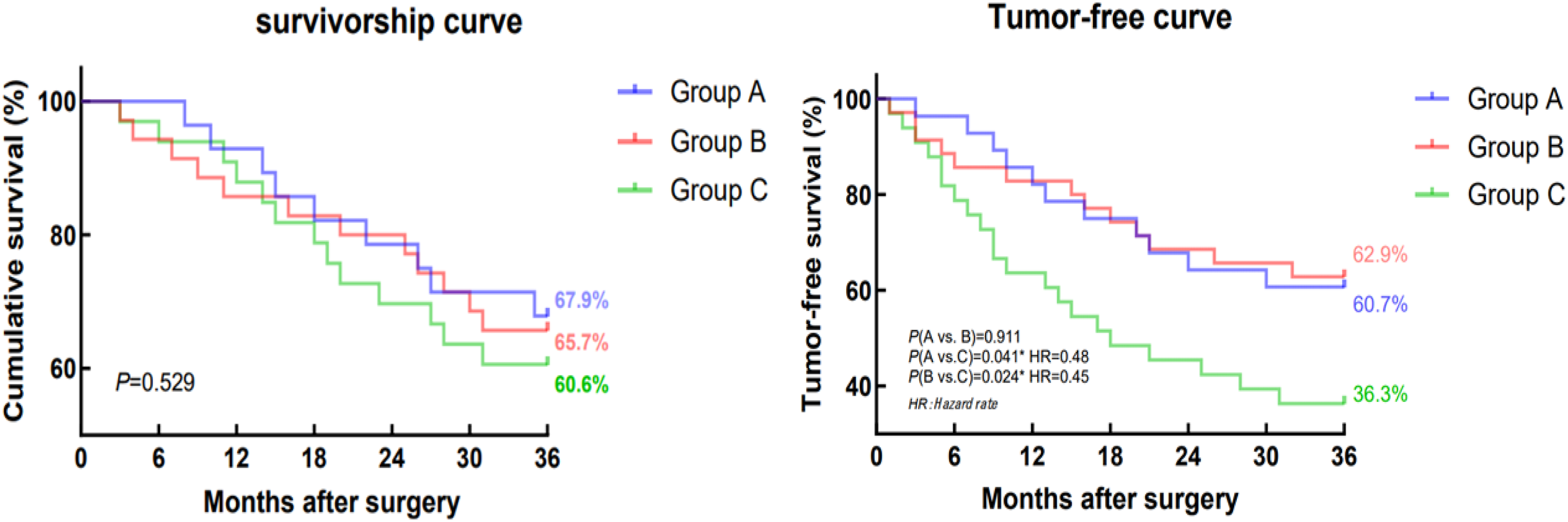
Discussion
Surgical resection remains the primary treatment for HCC in patients without vascular invasion or distant metastases in China. 8 Prognosis is closely related to tumor recurrence, and complete resection of the tumor along with its potential infiltration zone is considered the theoretical basis for cure. 18 However, surgeons must balance oncological completeness with preservation of adequate functional liver remnant. Several studies have suggested that HCC cells may spread along branches of the portal vein 10 , which provided the biological rationale for ALR. Compared with NALR, which aims to preserve as much liver tissue as possible, ALR determines the resection extent according to the portal vein drainage territory. This approach often requires removal of a larger volume of liver parenchyma and may increase the risk of postoperative liver failure. 7 In contrast, NALR determines the resection margin primarily based on tumor size and location, thereby preserving more functional liver tissue. However, this approach may carry a higher risk of local recurrence.19,20
Despite its theoretical oncological advantages, several studies have reported no significant difference in prognosis between ALR and NALR.21-23 As a result, the optimal surgical strategy for HCC remains controversial. In the present study, we compared laparoscopic anatomical hepatectomy (Group B) with laparoscopic non-anatomical hepatectomy (Group C). Although perioperative outcomes were similar between the two groups, postoperative follow-up showed significantly higher tumor-free survival in Group B than Group C. The higher recurrence observed in Group C may be attributed to several factors. While baseline demographic and tumor characteristics were comparable, patients in Group C underwent non-anatomical hepatectomy without navigation assistance, which may result in less precise margin control compared with anatomical resection or navigation-assisted procedures. In addition, unmeasured tumor-related factors such as microscopic vascular invasion, subtle multifocality, or biological aggressiveness, may have influenced recurrence pattern. These limitations are inherent to retrospective analyses and should be acknowledged when interpreting the findings. Notable, tumor-free survival in Group A was not significantly different from that in Group B. This observation indicates that ARN-assisted NALR may achieve tumor control comparable to ALR, potentially by facilitating accurate resection margins within areas at risk of microscopic tumor spread. In this cohort, the short-term therapeutic efficacy of ARN-assisted NALR appears similar to those of ALR. Although not statistically significant, a higher proportion of female patients was observed in Group A (25.0%) compared with in Group B (8.6%). In addition, the limited sample size and limited tumor burden in this cohort may have influenced these results. Therefore, these results should be interpreted with caution and considered hypothesis-generating. Confirmation in larger, prospective studies is warranted.
The liver has a complex vascular anatomy and substantial interindividual variability. 24 Therefore, surgeons must carefully evaluate preoperative imaging and mentally reconstruct 3D anatomy to understand the spatial relationships between tumors and adjacent vessels before surgery. 16 This process requires considerable experience and spatial reasoning. AR technology enables the projection of semi-transparent 3D model onto the surgical field, assisting intraoperative anatomical orientation. 12 By providing real-time visual guidance, AR navigation has the potential to reduce operative difficulty and improve surgical precision and safety. 25 ARN has been successfully applied in several surgical disciplines, including orthopedics, neurosurgery, and maxillofacial surgery,26-28 and its use in laparoscopic hepatobiliary surgery has increased in recent years. 29 Previous studies have suggested that ARN may reduce intraoperative complications, such as bleeding and biliary injury, and may contribute to improved oncological outcomes. 30 In this study, Group A (ARN-assisted nonanatomic hepatectomy) demonstrated significantly lower intraoperative blood loss (P=0.049) and a greater postoperative reduction in ɑ-fetoprotein (P=0.049) levels compared with Group C (nonanatomic hepatectomy). In terms of tumor recurrence, Group A showed a lower recurrence rate than group C (P=0.041) and a recurrence rate comparable to Group B (anatomical hepatectomy). These findings suggest that ARN-assisted resection may facilitate more accurate margin control through enhanced intraoperative visualization, potentially contributing to oncologic outcomes similar to those of anatomical resection. However, given the retrospective design and limited sample size, these results should be interpreted cautiously. Further prospective studies are required to confirm these observations.
Operative time is closely associated with postoperative complications, thrombosis, and increased anesthetic risk. 31 Therefore, minimizing operative duration remains an important objective in liver surgery. In this study, overall postoperative outcomes were comparable between Group A (ARN-assisted nonanatomic hepatectomy) and Group B (anatomical hepatectomy). However, operative time was significantly shorter in Group A than in both Group B (P=0.003) and Group C (P=0.039). This reduction may be attributed to the real-time visualization provided by ARN, which enhances intraoperative orientation and improve procedural efficiency. Although general postoperative outcomes were comparable, Group A also experienced significantly less intraoperative bleeding than Group B (P=0.048), suggesting a potential advantage of ARN-assisted techniques.
During postoperative hospitalization, one patient in Group A developed a lung infection, one patient in Group B developed a wound infection, and one case patient in Group C developed pleural effusion. All patients recovered after appropriate treatment and were discharged in stable condition. No statistically significant differences in postoperative complications were observed among the groups. Navigation-assisted surgery may allow more precise intraoperative dissection and potentially reduce the risk of surgical injuries and postoperative complications. However, this potential advantage was not clearly demonstrated in the present study, likely due to the limited sample size. Larger cohorts are needed to further evaluate this potential benefit.
This study explored the intraoperative and postoperative outcomes among patients undergoing ARN-assisted non-anatomical hepatectomy, anatomical liver resection, and non-anatomical hepatectomy without navigation, all performed laparoscopically. The results suggest that ARN-assisted nonanatomic hepatectomy may be associated with shorter operative time and reduced intraoperative blood loss. Short-term oncological outcomes over a 36-month follow-up period appeared comparable to those of anatomical liver resection and more favorable than those of nonanatomic hepatectomy without navigation.
This study has several limitations. First, as a retrospective observational study, it is subject to potential confounding factors, including baseline differences in patient characteristics, tumor features, and surgical complexity. Although efforts were made to ensure comparability between groups, unmeasured confounders may have influenced the observed outcomes. Second, despite the use of dense stereo reconstruction for real-time surface registration, intraoperative point cloud quality may be compromised by liver deformation, bleeding, smoke, surgical instruments, and partial occlusion, potentially introducing registration deviations. Continuous soft-tissue deformation during laparoscopic liver surgery further reduces the fidelity of preoperative models, and rigid registration cannot fully compensate for these changes. In this study, rigid alignment was employed primarily to enhance intraoperative anatomical visualization rather than to achieve high-precision spatial accuracy; however, deformation-aware or non-rigid registration approaches may further improve navigation accuracy in future applications. In addition, the navigation system evaluated in this study was developed and implemented within our institution. Surgical outcomes may therefore depend on factors such as system calibration, workflow integration, and team experience. As a result, these findings may not be directly generalizable to all augmented reality navigation platforms or clinical settings, and external validation is warranted. Finally, heterogeneity in tumor size and unmeasured pathological factors, such as microscopic vascular invasion, may have influenced outcomes and limited direct comparability among groups. Although baseline characteristics were similar, residual confounding cannot be fully excluded due to the retrospective design. Accordingly, the findings should be interpreted cautiously and considered exploratory, pending confirmation in larger, stratified prospective studies.
Conclusion
In this study, laparoscopic ARN-assisted nonanatomic hepatectomy demonstrated similar short-term outcomes to laparoscopic anatomical hepatectomy within this cohort. Both approaches were associated with lower intraoperative bleeding and reduced tumor recurrence compared with laparoscopic non-anatomical hepatectomy without navigation. ARN-assisted surgery was also associated with shorter operative time. However, given the retrospective design and limited sample size, these findings should be interpreted cautiously and considered hypothesis-generating, warranting validation in larger prospective studies.
Supplemental Material
Supplemental Material - Augmented Reality Navigation-Assisted Laparoscopic Hepatectomy: A Retrospective Comparison of Anatomical and Non-Anatomical Resection
Supplemental Material for Augmented Reality Navigation-Assisted Laparoscopic Hepatectomy: A Retrospective Comparison of Anatomical and Non-Anatomical Resection by Haisong Xu, Wenhao Huang, Huoling Luo, An Zhang, Yuehua Guo, Gongze Peng, Tianchong Wu and Yongzhu He in Clinical Medicine Insights: Oncology.
Footnotes
Ethics Considerations
The authors are accountable for all aspects of the work and ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The ethics committee of The Second Medical College of Jinan University, Shenzhen People’s Hospital, approved the study protocol. (Approval No. LL-ZLJS-2022083-04).
Consent to Participate
Written informed consent was waived by the Ethics Committee of the Second Clinical Medical College, Jinan University Hospital (Shenzhen People’s Hospital), Shenzhen, China, given the retrospective nature of the study and the use of anonymized patient information.
Consent for Publication
No identifiable patient data or images are included in this article.
Author Contributions
Tianchong Wu, Haisong Xu, and wenhao Huang have given substantial contributions to the conception and the design of the manuscript, An Zhang to the provision of study materials or patients, Yuehua Guo, and Gongze Peng to the collection and assembly of data, Yongzhu He and Huoling Luo to data analysis and interpretation. All authors have participated in drafting the manuscript, and author Tianchong Wu revised it critically. All authors read and approved the final version of the manuscript. Note: Tianchong Wu is the first corresponding author of this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Innovation Foundation of Shenzhen (Nos. JCYJ20220530152200001).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.