
Abstract
Background
Diabetes mellitus (DM) is a common comorbidity in patients undergoing neurosurgical procedures and has been associated with adverse surgical outcomes. However, the extent to which DM, particularly the presence of chronic diabetic complications, affects perioperative outcomes and healthcare utilization in patients undergoing craniotomy for brain tumors remains unclear. Clarifying this relationship is essential for perioperative risk stratification and optimization.
Methods
We conducted a retrospective cohort study using the National Inpatient Sample (NIS) database, identifying adults (≥18 years) who underwent craniotomy for brain tumors between 2016 and 2022. Patients were stratified into three groups: non-DM, DM without chronic complications, and DM with chronic complications. Outcomes included in-hospital mortality, postoperative complications, length of stay (LOS), discharge disposition, and hospitalization costs.
Results
A total of 49,100 patients were included, of whom 8,822 (18.1%) had DM. Overall, DM patients experienced higher rates of postoperative complications, longer LOS, increased non-routine discharge, and greater hospitalization costs compared with non-DM patients. Notably, patients with DM without chronic complications had outcomes comparable to those of non-DM patients. In contrast, DM patients with chronic complications demonstrated significantly higher risks of adverse outcomes across all measured endpoints.
Conclusions
DM alone does not significantly worsen outcomes after craniotomy for brain tumors. However, the presence of chronic diabetic complications is strongly associated with increased perioperative morbidity, mortality, prolonged hospitalization, and higher healthcare costs. These findings underscore the importance of incorporating diabetic complication status into preoperative evaluation and targeted perioperative management strategies.
Introduction
Diabetes mellitus (DM) is a widespread chronic metabolic disorder that continues to pose a significant burden on global health.1,2 It has well-established links to microvascular and macrovascular complications, causes wound healing challenges, raises infection risk, and adversely influences perioperative outcomes in multiple surgical fields.3-6 Given that neurosurgical procedures often involve physiological stress, extended durations of surgery, and intensive postoperative management, patients with DM may be especially at risk for postoperative complications after cranial surgeries (craniotomy). 7 However, despite the growing number of DM patients needing neurosurgical treatment, the impact of DM, particularly DM complicated by chronic complications, on outcomes following craniotomy for brain tumors has not been well defined.
Craniotomy for brain tumors is a significant neurosurgical procedure with high risks. 8 Postoperative complications can greatly affect the recovery of neurological function, daily activity ability, and the utilization of medical resources. 9 Therefore, it is important to understand how DM, and the severity of the condition, influence the risks associated with craniotomy for brain tumor. This understanding is important for optimizing preoperative stratification, planning the operation, and managing postoperative care. However, there are still few large-scale, population-level analyses capable of clearly delineating these associations.
Although the evidence remains fragmented, several studies have investigated the impact of hyperglycemia on neurosurgical outcomes. For instance, one prospective study of 224 craniotomy patients reported that severe intraoperative hyperglycemia independently increased the risk of new infections within the first postoperative week. 10 A large retrospective cohort study investigated 12,281 patients who had brain tumor craniotomy. It found that even mild elevations in preoperative glucose (≥5.6 mmol/L [≥101 mg/dL]) were linked to higher 30-day mortality. The risk of death increased as glucose levels went up. 11 Another cohort of 4564 elective intracranial surgery patients found that elevated preoperative HbA1c was associated with higher rates of early postoperative infection. 12 Using the National Inpatient Sample (NIS), an analysis of 7745 meningioma resections showed that DM was independently associated with increased postoperative complications, greater in-hospital mortality, longer hospitalization, and higher costs. 13 A small prospective observational study of elective craniotomy further showed that structured perioperative glucose monitoring combined with intravenous rapid-acting insulin could significantly reduce postoperative infections. 14 Despite these findings, most prior work has not differentiated between DM with and without chronic complications. This difference is becoming more important because the severity of DM is associated with various health issues and can affect surgical risk in different ways.
The present study investigates clinical outcomes and healthcare utilization in non-DM patients, DM patients without chronic complications, and DM patients with chronic complications who underwent craniotomy for brain tumors, using the NIS dataset. We assess in-hospital mortality, postoperative complications, discharge destination, length of stay (LOS), and hospitalization cost to determine whether DM severity is independently associated with adverse outcomes. This study aims to provide a better understanding of perioperative risk profiles and to support more personalized management strategies during neurosurgical oncology procedures.
Methods
Data Source
This investigation employed a retrospective cohort approach, using data from the NIS database. The NIS is developed by the Agency for Healthcare Research and Quality. 15 The NIS is part of the Healthcare Cost and Utilization Project (HCUP). 16 The NIS serves as a comprehensive and nationally representative resource for inpatient hospitalizations in the United States. Covering over 95 % of all inpatient admissions, the NIS consists of a 20 % stratified sample of hospitalizations from participating states. 16 This dataset includes discharge information from a diverse range of hospitals, enabling the assessment of clinical outcomes and healthcare resource utilization in various kinds of patient populations. Given the de-identified nature of the data in the NIS database, this study was exempted from review by the Institutional Review Board (IRB). The reporting of this study conforms to the STROBE guidelines. 17
Study Cohort
Our analysis included patients aged 18 years and older who underwent craniotomy for brain tumor resection between 2016 and 2022. We identified patients who received a craniotomy for brain tumors by utilizing the relevant diagnoses and procedure codes from the International Classification of Diseases, 10th Revision-Clinical Modification (ICD-10-CM) (Supplementary Table 1). Records with missing essential demographic, socioeconomic, or hospital-level information were excluded from the analysis. The cohort was stratified into three groups: non-DM patients, DM patients without chronic complications, and DM patients with chronic complications. DM status was identified using the HCUP Elixhauser Comorbidity Software Refined (CMR v2025.1), which applies standardized ICD-10-CM coding algorithms (Supplementary Table 1). The specific ICD-10-CM codes included in each category were those predefined by the HCUP CMR v2025.1 algorithm. Comorbidities were also identified using this same tool.
Outcomes
Study outcomes were defined to evaluate major clinical and economic measures. Comparisons between groups focused on in-hospital mortality, LOS, total hospitalization charges, and discharge disposition. In addition, all in-hospital complications were systematically captured and analyzed. Complications were identified using ICD-10 codes. These included cerebrovascular events such as stroke and intracranial hemorrhage, other neurological complications including meningitis and brain abscess, cardiac events such as myocardial infarction and cardiac arrest, respiratory complications including acute respiratory failure and pulmonary embolism, renal complications such as acute kidney injury, thromboembolic events including deep vein thrombosis, surgical site complications such as postoperative wound infection and wound dehiscence, extracranial infections including pneumonia and urinary tract infection, cerebrospinal fluid leak, and systemic infection such as sepsis. 18 The full list of ICD-10 codes is provided in Supplementary Table 1.
Statistical Analysis
Demographic profiles and clinical features across the three patient cohorts were summarized using descriptive statistical approaches. Continuous variables were characterized by means and corresponding standard deviations (SD), whereas categorical variables were presented as frequencies and proportional values. The normality of continuous variable distributions was verified via the Kolmogorov-Smirnov test. For continuous variables failing to meet the normality assumption, intergroup comparisons were performed with the Mann-Whitney U test. With respect to categorical variables, the chi-square test was applied for comparative analyses. When the expected frequencies in any contingency table cell were low, Fisher’s exact test was used as an alternative.
For the assessment of intergroup differences in outcome measures, multivariable logistic regression models were constructed to estimate adjusted odds ratios (aOR). The primary objective of covariate selection was to control for potential confounding by patient-, socioeconomic-, and hospital-level factors that may independently influence perioperative outcomes. Patient-level variables included age, sex, race/ethnicity, primary payer, median household income quartile by ZIP code, and comorbidities identified using the Elixhauser Comorbidity Index. These variables were included because of their established associations with surgical risk and postoperative outcomes. Socioeconomic indicators, including income quartile and insurance status, were incorporated to account for differences in access to care, baseline health status, perioperative management, and discharge planning. Hospital-level characteristics, including hospital region, location (urban vs rural), teaching status, and bed size, were also included to account for institutional and geographic variability. In nationally representative datasets such as the NIS, these structural factors may influence mortality, length of stay, and healthcare costs. Adjustment for these variables was therefore performed to account for differences in healthcare delivery and resource availability across hospitals. Additionally, the Kruskal-Wallis test and Cochran-Armitage trend test were used to conduct pairwise and trend comparisons among three subgroups: non-DM patients, DM patients without chronic complications, and DM patients with chronic complications. All statistical analyses were carried out using SAS software (Version 9.4; SAS Institute Inc., Cary, NC, USA) and R software (Version 4.5.0; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined as a two-tailed P-value of less than 0.05.
Results
Clinical Outcomes and Healthcare Utilization in DM vs. Non-DM Patients Undergoing Craniotomy for Brain Tumors
Baseline Characteristics of Patients Undergoing Craniotomy for Brain Tumor, Stratified by DM Status
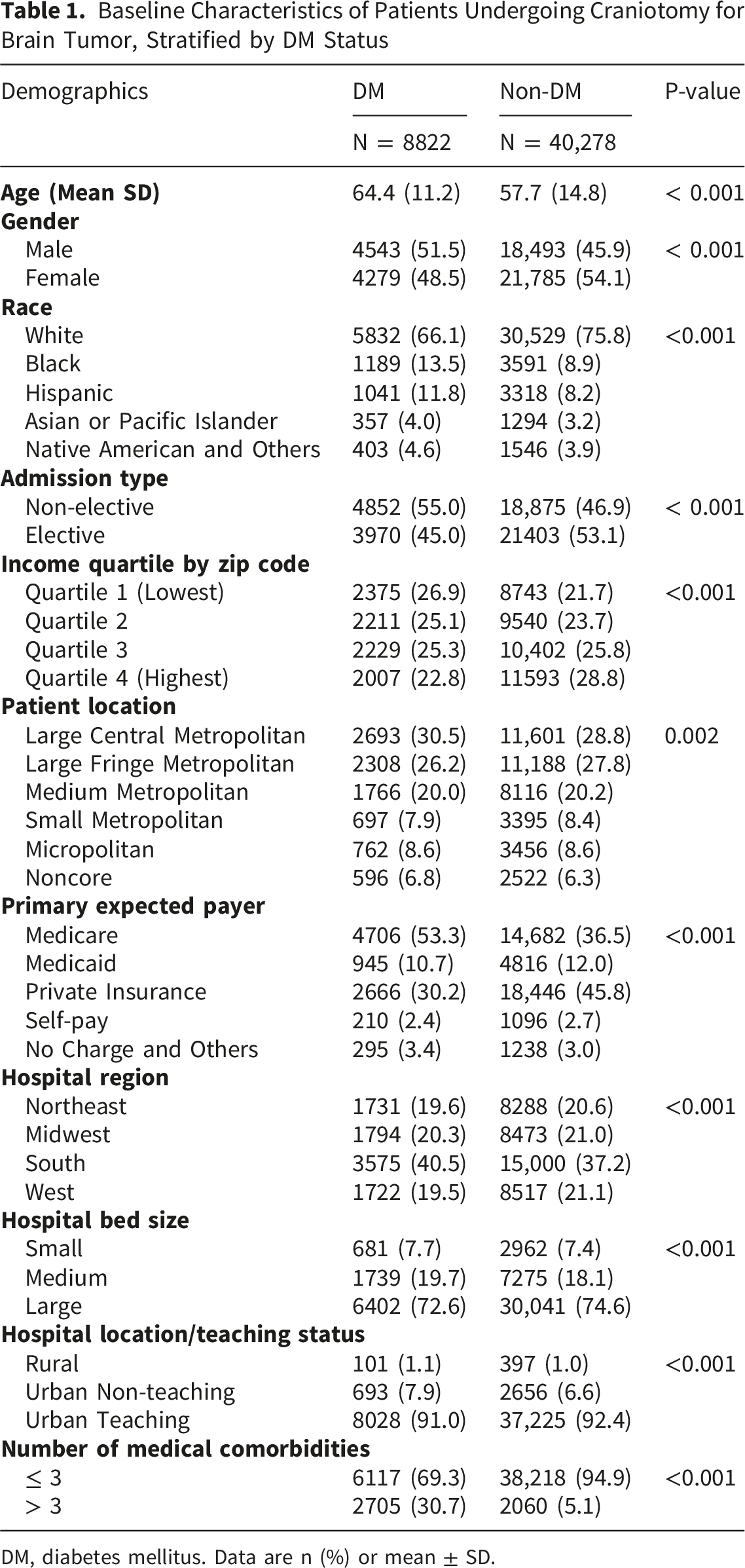
DM, diabetes mellitus. Data are n (%) or mean ± SD.
Comparison of Clinical Outcomes of Patients Undergoing Craniotomy for Brain Tumor With and Without DM
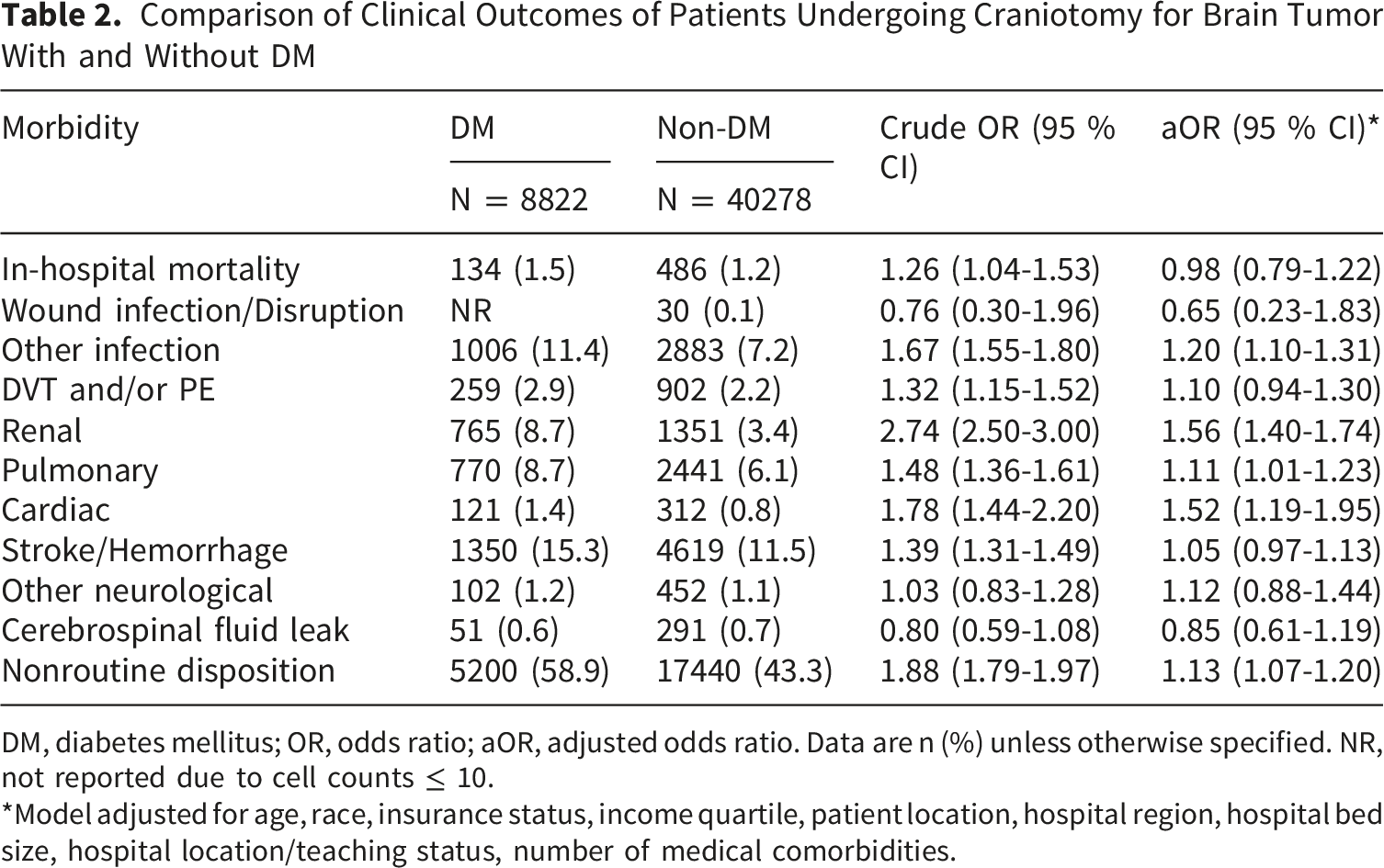
DM, diabetes mellitus; OR, odds ratio; aOR, adjusted odds ratio. Data are n (%) unless otherwise specified. NR, not reported due to cell counts ≤ 10.
*Model adjusted for age, race, insurance status, income quartile, patient location, hospital region, hospital bed size, hospital location/teaching status, number of medical comorbidities.
Comparison of Hospital Outcomes of Patients Undergoing Craniotomy for Brain Tumor With and Without DM
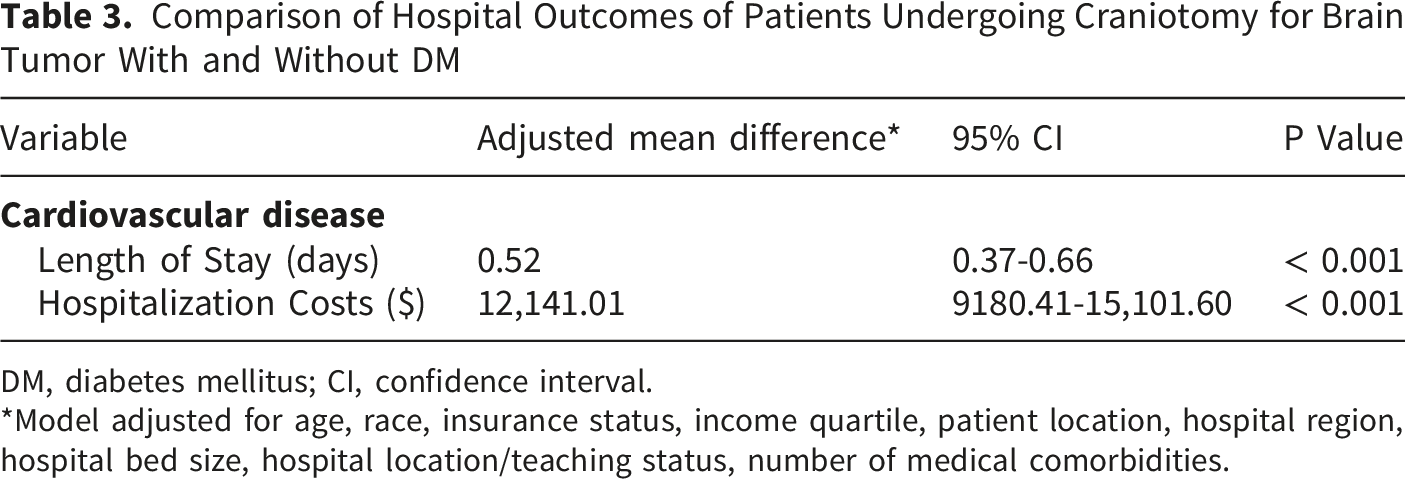
DM, diabetes mellitus; CI, confidence interval.
*Model adjusted for age, race, insurance status, income quartile, patient location, hospital region, hospital bed size, hospital location/teaching status, number of medical comorbidities.
Clinical Outcomes and Healthcare Utilization in DM Patients Without Chronic Complications Versus Non-DM Patients Undergoing Craniotomy for Brain Tumors
We next explored the clinical outcomes and healthcare utilization in DM patients without chronic complications versus non-DM patients undergoing craniotomy for brain tumors. As shown in Supplementary Table 2, patients with DM but without chronic complications were older and had a higher proportion of males compared to the non-DM group. Additionally, there were more Black and Hispanic patients among DM patients without complications. They were more likely to be from lower income backgrounds and had a higher incidence of medical comorbidities.
Comparison of Clinical Outcomes of Patients After Brain Tumor Craniotomy in Indicated Groups
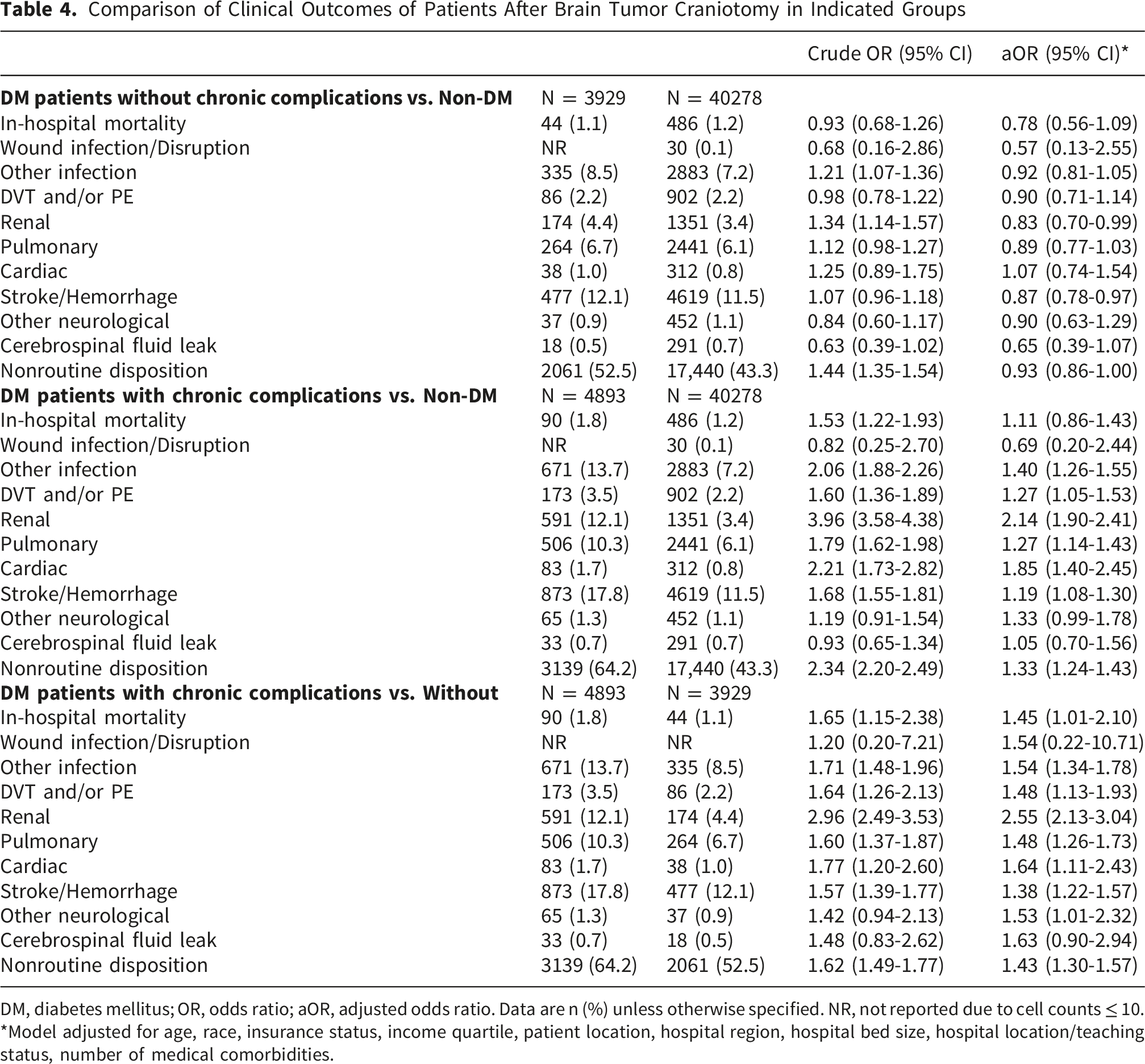
DM, diabetes mellitus; OR, odds ratio; aOR, adjusted odds ratio. Data are n (%) unless otherwise specified. NR, not reported due to cell counts ≤ 10.
*Model adjusted for age, race, insurance status, income quartile, patient location, hospital region, hospital bed size, hospital location/teaching status, number of medical comorbidities.
Comparison of Hospital Outcomes in Patients Undergoing Craniotomy for Brain Tumor (by Indicated Groups)
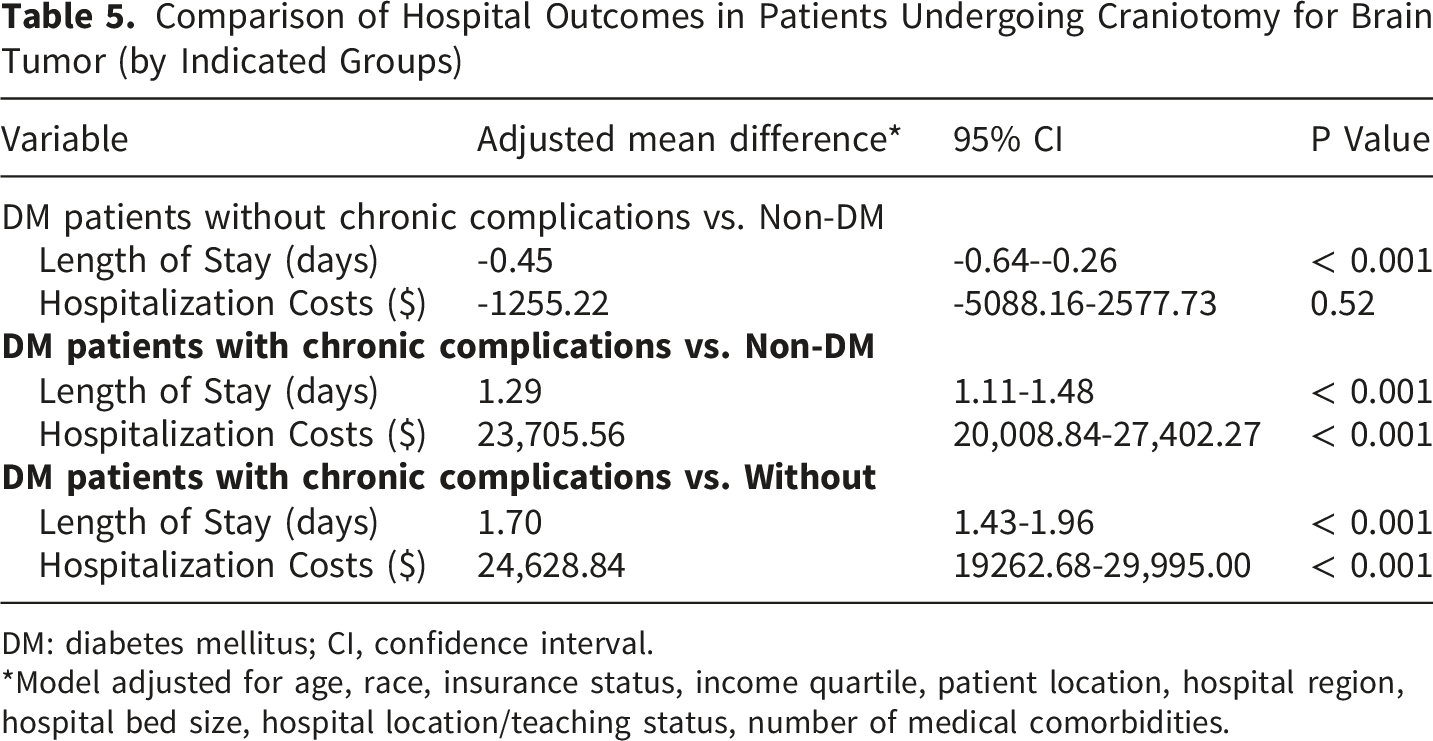
DM: diabetes mellitus; CI, confidence interval.
*Model adjusted for age, race, insurance status, income quartile, patient location, hospital region, hospital bed size, hospital location/teaching status, number of medical comorbidities.
Clinical Outcomes and Healthcare Resource Utilization in DM Patients With Chronic Complications Versus Non-DM Patients Undergoing Craniotomy for Brain Tumors
We then examined the clinical outcomes and healthcare resource utilization among DM patients with chronic complications and their non-DM counterparts who underwent craniotomy for brain tumors. The demographics and baseline characteristics of the two groups are summarized in Supplementary Table 3.
Clinical outcomes were presented in Table 4. Although no significant difference was observed, in-hospital mortality tended to be higher among the DM patients with chronic complications (aOR 1.11, 95 % CI 0.86-1.43). The results showed a notable increase in the incidence of other infections (aOR 1.40, 95 % CI 1.26-1.55), deep venous thrombosis/pulmonary embolism (DVT/PE) (aOR 1.27, 95 % Confidence Interval (CI) 1.05-1.53), renal complications (aOR 2.14, 95 % CI 1.90-2.41), pulmonary complications (aOR 1.27, 95 % CI 1.14-1.43), cardiac complications (aOR 1.85, 95 % CI 1.40-2.45), stroke/hemorrhage (aOR 1.19, 95 % CI 1.08-1.30), and non-routine disposition (aOR 1.33, 95 % CI 1.24-1.43) in the DM patients with chronic complications. No statistically significant differences were observed in the rates of wound infection/disruption or cerebrospinal fluid leak. Furthermore, DM patients with chronic complications had a longer average LOS compared to non-DM patients, with an adjusted mean difference of 1.29 days (95 % CI: 1.11-1.48, P< 0.001) and also had higher hospitalization costs, with an increase of $23,705.56 (95 % CI: $20,008.84-$27,402.27, P< 0.001) (Table 5). These findings suggest increased risks and healthcare utilization associated with DM patients with chronic complications.
Clinical Outcomes and Healthcare Resource Utilization in Patients Undergoing Craniotomy for Brain Tumors: A Comparison Between DM Patients With and Without Chronic Complications
The demographics and baseline characteristics of DM patients with and without chronic complications who underwent craniotomy for brain tumors are presented in Supplementary Table 4. As presented in Table 4, in-hospital mortality was higher in the DM patients with chronic complications compared to counterparts without complications (aOR 1.45, 95 % CI 1.01-2.10). The incidence of various complications was also elevated among DM patients with chronic complications, including other infections (aOR 1.54, 95 % CI 1.34-1.78), DVT/PE (aOR 1.48, 95 % CI 1.13-1.93), renal complications (aOR 2.55, 95 % CI 2.13-3.04), pulmonary complications (aOR 1.48, 95 % CI 1.26-1.73), cardiac complications (aOR 1.64, 95 % CI 1.11-2.43), stroke/hemorrhage (aOR 1.38, 95 % CI 1.22-1.57), and other neurological complications (aOR 1.53, 95 % CI 1.01-2.32). Notably, DM patients were more likely to experience non-routine discharge, with an aOR of 1.43 (95 % CI 1.30-1.57). Moreover, there were no significant differences in wound infection/disruption or cerebrospinal fluid leak. The results of the healthcare resource utilization analysis are shown in Table 5. DM patients with chronic complications had a longer average LOS, with an adjusted mean difference of 1.70 days (95 % CI 1.43-1.96, P< 0.001), and they also had higher hospitalization costs, amounting to an increase of $24,628.84 (95 % CI $19,262.68-$29,995.00, P< 0.001) compared to those without chronic complications. These results demonstrate the increased risks and significant healthcare burden associated with DM patients who have chronic complications in the context of brain tumor craniotomy.
Impact of Whether DM Is Accompanied by Chronic Complications on Inpatient Outcomes: Hospitalization Costs, LOS, and Complications
An evaluation of inpatient outcomes categorized by whether DM is accompanied by chronic complications was conducted. The analysis employed Kruskal-Wallis tests, which revealed significant variations in hospitalization costs and LOS across the severity subgroups. DM patients with chronic complications showed notably higher costs and longer stays (Figure 1). Additionally, the Cochran-Armitage trend test showed that in-hospital mortality rates, non-routine discharges, and postoperative complications rose significantly as diabetes severity increased. These complications included cardiac issues, DVT/PE, other infections, pulmonary complications, renal complications and strokes or hemorrhages (Figure 2). These results suggest that greater severity of diabetes is associated with increased hospitalization costs, prolonged LOS, higher in-hospital mortality, non-routine discharges, and increased postoperative complications, indicating the need for targeted interventions based on the presence of chronic complications in DM. Hospitalization costs and length of stay across non-diabetic patients and diabetic patients with and without chronic complications. Kruskal-Wallis tests revealed significant differences in total hospitalization costs and length of stay among the three subgroups. Patients with chronic-complicated diabetes demonstrated significantly higher costs and longer hospital stays compared with non-diabetic patients and those without chronic complications Trends in postoperative outcomes by diabetes severity. The Cochran-Armitage trend test demonstrates that in-hospital mortality, non-routine discharge rates, and postoperative complications increase significantly with greater diabetes severity. Rising complication rates include cardiac events, deep vein thrombosis or pulmonary embolism (DVT/PE), other infections, pulmonary complications, renal complications, and stroke or hemorrhage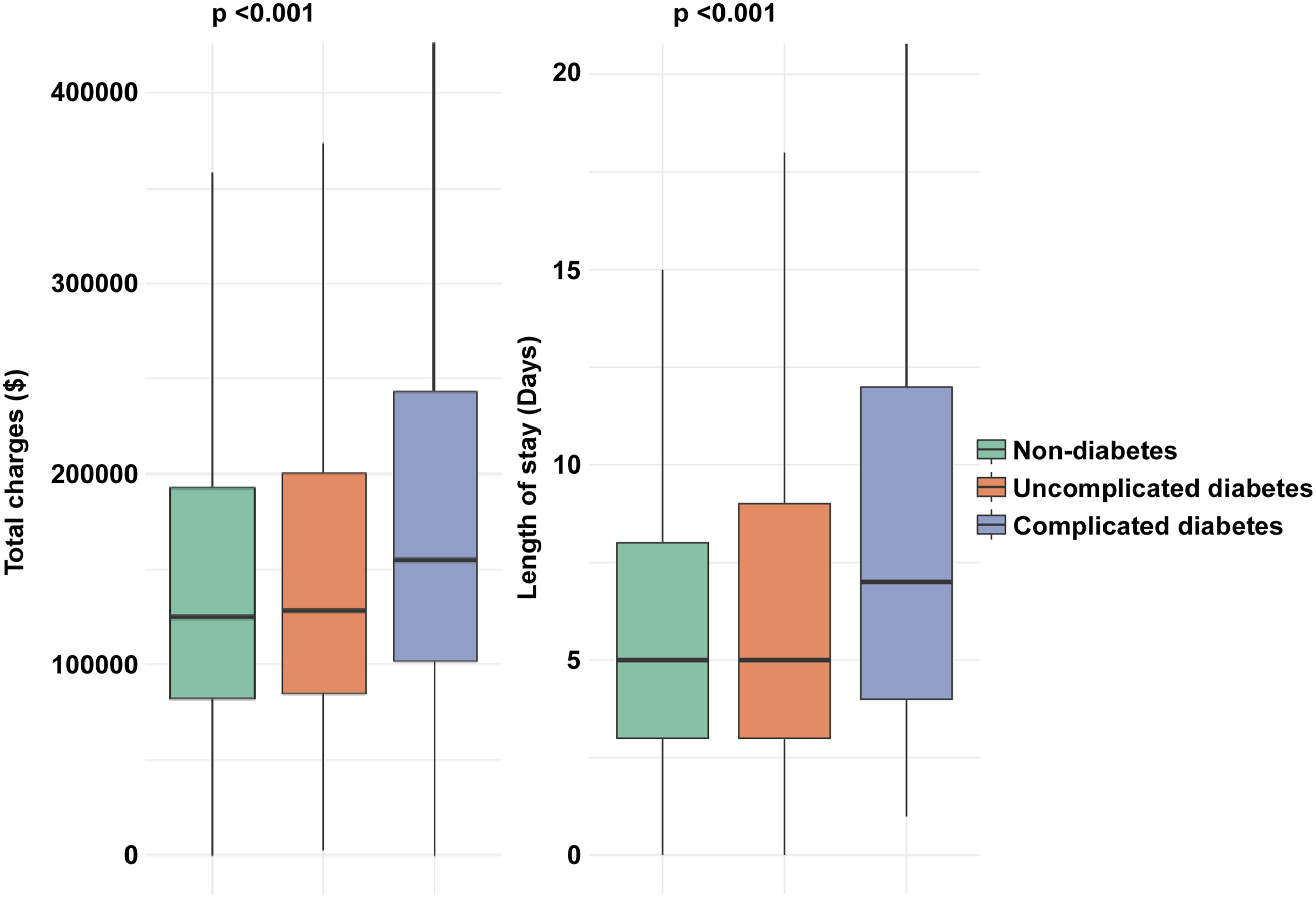

Discussion
In this large, nationally representative analysis of patients undergoing craniotomy for brain tumors, we evaluated how DM and the presence of chronic DM-related complications affect perioperative risks and healthcare utilization. The findings demonstrate that DM, especially DM with chronic complications, leads to worsening outcomes. Our results indicate that DM with chronic complications plays an important role in determining postoperative risk of craniotomy for brain tumor.
Previous studies have shown that perioperative dysglycemia increases mortality and postoperative complications in neurosurgical patients.11,19 A retrospective analysis of 1969 adult neurosurgical intensive care unit patients who underwent craniotomy found that postoperative glycemic variability, as quantified by coefficient of variation and root mean square of successive differences, serves as an independent and modifiable predictor of 28-day and 90-day all-cause mortality following cranial surgery. 20 Moreover, the hemoglobin glycation index (HGI), a marker reflecting the discrepancy between observed and predicted HbA1c, was independently associated with both short- and long-term mortality in Trauma/Surgical Intensive Care Units patients. 21 Here, our results confirm that DM remains an important clinical factor in brain tumor surgery. However, our study adds to the existing literature by distinguishing between DM without chronic complications and DM with chronic complications. Our results show that these groups have different levels of risk. DM patients without chronic complications exhibited clinical outcomes comparable to their non-DM counterparts. Notably, DM patients with chronic complications experienced significantly higher rates of adverse events, including infections, pulmonary and cardiac complications, renal injury, stroke or hemorrhage, and thromboembolic events. These complications led to longer hospital stays, greater resource use, and substantially increased financial burden.
Patients with DM and chronic complications may be particularly vulnerable in the setting of brain tumor craniotomy due to impaired physiologic reserve and end-organ dysfunction. Persistent elevation of blood glucose levels can impair vascular integrity by promoting oxidative damage and chronic low-grade inflammation, which in turn disrupts microcirculatory function. These alterations may reduce effective tissue oxygenation and weaken the body’s ability to cope with the physiological demands imposed by major surgery.22-24 Among neurosurgical patients, perioperative corticosteroids and stress-induced fluctuations in blood glucose may exacerbate these vascular and metabolic alterations, thereby weakening host defenses and increasing the risk of infection and delayed tissue repair.25,26 Additionally, diabetes-related microangiopathy can compromise cerebral perfusion, which may worsen perioperative brain edema and impair postoperative neurological recovery. 27 In patients with diabetic nephropathy, underlying renal impairment can heighten sensitivity to perioperative fluid imbalance, contrast agents, and nephrotoxic drugs, increasing the likelihood of acute kidney injury and extended hospital stays. 28 Moreover, longstanding metabolic disturbances, oxidative damage, and chronic inflammation in diabetes contribute to the progression of atherosclerosis and impairment of cardiac function. 29 In individuals undergoing major intracranial procedures, compromised cardiovascular function can impair hemodynamic regulation and weaken tolerance to surgical blood loss and postoperative stress. Overall, chronic diabetic complications may reflect a state of frailty, widespread vascular injury, and diminished physiological reserve, thereby increasing the risk of adverse postoperative outcomes after brain tumor craniotomy.
In contrast, DM patients without chronic complications generally exhibit better-preserved physiological reserves, 30 which may lead to outcomes that are more comparable to those of non-DM patients. This distinction suggests the importance of the presence of chronic complications in DM, rather than the diagnosis alone, as a more accurate predictor of outcomes of craniotomy for brain tumor.
These findings have several clinical implications. First, the routine preoperative identification of chronic complications in DM patients may be important for appropriate perioperative risk stratification. Second, enhanced perioperative monitoring, including more frequent glucose checks, optimization of glycemic control, and careful management of comorbid organ dysfunction, may be especially important in DM patients with chronic complications. Third, given the higher rates of non-routine discharge and prolonged hospital stays, early discharge planning and targeted resource allocation may improve postoperative care for this high-risk population.
This study has several important limitations. As with all analyses based on administrative datasets, diagnostic and procedural codes are subject to potential misclassification, coding inaccuracies, and inter-institutional variability in documentation and billing practices. Because these codes are primarily generated for administrative rather than research purposes, some degree of residual measurement error is inevitable, which may have influenced the identification of comorbidities and clinical outcomes in our study. In addition, the NIS does not contain detailed oncologic information such as WHO tumor grade, molecular markers including IDH status or MGMT methylation, tumor size, or radiographic characteristics, which precludes reliable stratification by tumor biology or aggressiveness. Detailed metabolic data were also unavailable, including HbA1c levels, perioperative glucose measurements, insulin regimens, and glycemic management strategies. Furthermore, granular surgical variables such as operative duration, extent of resection, intraoperative blood loss, and intraoperative complications were not available, and medication-level data including perioperative glucocorticoid exposure could not be assessed. These unmeasured factors may contribute to residual confounding. Additionally, no formal sample size or power calculation was conducted, which may limit the interpretation of statistical power for certain subgroup analyses.
An unexpected finding of this study was that, after multivariable adjustment, DM patients without chronic complications demonstrated slightly lower odds of renal complications (aOR 0.83, 95% CI 0.70-0.99) and stroke/hemorrhage (aOR 0.87, 95% CI 0.78-0.97) compared with non-DM patients. Importantly, these associations were modest in magnitude and close to unity, and the crude estimates for these outcomes were either comparable or higher in the DM group, suggesting that baseline differences between groups substantially influenced unadjusted comparisons. The reversal of effect direction after adjustment indicates that demographic factors, socioeconomic status, and comorbidity burden accounted for much of the observed risk. Several explanations may underlie these findings. First, residual confounding is possible, as administrative databases lack detailed clinical variables such as laboratory values, intraoperative hemodynamics, tumor characteristics, and perioperative physiologic severity, which may differentially affect complication risk. Second, patients with a documented diagnosis of DM, even without chronic complications, may undergo closer perioperative glucose monitoring and renal surveillance, potentially mitigating certain short-term complications. Third, misclassification bias cannot be excluded, as identification of DM severity relies on ICD-10 coding and may incompletely capture undiagnosed or subclinical metabolic disease in the non-DM cohort. Given the small effect sizes and the limitations inherent to administrative data, these findings should not be interpreted as evidence of a protective effect of uncomplicated DM. Rather, they reinforce our overall observation that the excess perioperative risk associated with DM appears to be primarily driven by the presence of chronic DM complications, which were consistently associated with substantially worse clinical outcomes and increased healthcare utilization.
Conclusion
In conclusion, while DM without chronic complications does not significantly worsen postoperative outcomes after craniotomy for brain tumors, DM with chronic complications is associated with substantially increased perioperative morbidity, mortality, LOS, and healthcare costs. These findings emphasize the need to incorporate DM and its chronic complications into preoperative assessment process. These results also indicate that implementation of customized perioperative strategies can improve outcomes in DM patients with chronic complications undergoing brain tumor surgery.
Supplemental Material
Supplemental Material - The Impacts of Diabetes Mellitus on Clinical Outcomes of Hospitalization Following Craniotomy for Brain Tumor
Supplemental material for The Impacts of Diabetes Mellitus on Clinical Outcomes of Hospitalization Following Craniotomy for Brain Tumor by Yu Hong, Pengyuan Zhang, Jiewen Jin, Weiwei Liang, Junxin Chen, Juan Liu, Hongyu Guan, Zijun Huo and Hai Li in Clinical Medicine Insights: Oncology.
Footnotes
Ethical Considerations
This study used a publicly available database that contains no identifiable personal information. Therefore, ethical approval and informed consent were not required.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by the Natural Science Foundation of Hunan Province (2026JJ50582), the Guangdong Basic and Applied Basic Research Foundation (No. 2025A1515010231, No. 2022A1515012250 and No. 2025A1515012538), the Science and Technology Projects in Guangzhou (2023A04J2190).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.