
Abstract
Acute ischaemic stroke care has long been guided by the maxim “time is brain,” yet outcome variability suggests that clock time alone is insufficient. We propose the Time, Tissue, and Systems (TTS) framework, a quantitative model integrating temporal progression, tissue vulnerability, and health-system performance. Biological injury is conceptualized as accelerated neuronal loss scaled by tissue phenotype and systems friction, and clinical decision-making is reframed as net utility optimization. Illustrative modeling across four archetypal stroke profiles demonstrates how identical clock times yield divergent biological and functional trajectories. The TTS framework provides a coherent structure for precision stroke care, aligning biological time with system time.
Reframing the Urgency of Stroke
Stroke has long been described as a “brain attack,” a term deliberately chosen to convey urgency and elevate acute ischaemic stroke (AIS) to the same emergency status as myocardial infarction. 1 Quantitative analyses lent this message biological precision: without reperfusion, an estimated 4 million neurons, 12 million brain cells, and 15 billion synapses are lost each minute. 2 The doctrine “time is brain” reshaped practice, driving thrombolysis, mechanical thrombectomy, stroke units, and regionalised systems of care.2-5 Yet three decades into the reperfusion era, clinical trajectories remain stubbornly heterogeneous. Patients treated within recommended windows may deteriorate unexpectedly.6-10 Others presenting beyond conventional thresholds recover when imaging demonstrates viable tissue.11-14 Posterior circulation strokes show heterogeneous trajectories.15-19 Transfer delays alter prognosis even when tissue phenotype appears similar.17,20-24 Mild strokes subjected to reperfusion reveal nuanced risk–benefit balances, incurring substantial haemorrhagic risk without measurable functional benefit. 25 These realities suggest that clock time alone does not determine outcome. Stroke unfolds within a dynamic interaction of temporal evolution, tissue vulnerability, and systems performance.2,14,26 Understanding and quantifying this interaction is essential for the next phase of precision stroke care.
Why Time Alone Is Insufficient
Early thrombolysis and thrombectomy trials established that earlier reperfusion improves outcomes, but subsequent work revealed that therapeutic windows are biologically modulated probabilities rather than fixed constants.2,4,5,14,27 Collateral circulation, infarct core size, occlusion site, metabolic state, and inflammatory response influence the rate at which irreversible injury accrues.28-35 Simultaneously, stroke-unit organization, coordinated stroke teams, imaging workflows, and interhospital transfer times independently shape prognosis.24,36
The expansion of thrombectomy up to 24 hours in selected patients further demonstrated that tissue phenotype can override rigid clock boundaries.11,14,27 Conversely, systems friction - particularly in transfer pathways - may negate biological advantage despite theoretically favorable imaging.37-40 These observations underscore a fundamental limitation of single-axis thinking: neither time, tissue, nor systems alone explains outcome heterogeneity. Rather, their interaction determines biological and clinical trajectories. A more complete expression of acute stroke biology may therefore be written simply:

This formulation reframes acute stroke not as a race against the clock alone, but as a dynamic interaction between temporal progression, biological substrate, and systemic response.
The Time, Tissue, and Systems Framework
We therefore propose a unifying construct: the Time, Tissue, and Systems (TTS) framework. The probability of favorable functional outcome may be represented as:

Rather than asking whether a patient falls within a time window, this framework asks whether intervention maximizes expected biological and functional benefit.
From Clock Time to Biological Time
The heuristic estimate of 4 million neurons lost per minute without reperfusion provides a biological starting point.
2
Cumulative neuronal loss may be approximated as:

However, neuronal loss is not uniform across patients. Collateral collapse, proximal occlusion, metabolic dysregulation, and delayed systems response accelerate injury.24,28-32,37,38 We therefore introduce a biological acceleration factor:

Clock time thus becomes biological time, scaled by tissue vulnerability and systems friction. Identical elapsed minutes may correspond to profoundly different biological injury burdens. This conceptual shift is illustrated in Figure 1, where divergent neuronal loss trajectories translate into differential clinical utility across representative stroke archetypes (see Figure 1). Time remains critical, but its biological cost is context-dependent. The time, tissue, and systems framework: Biological time and clinical utility in acute stroke.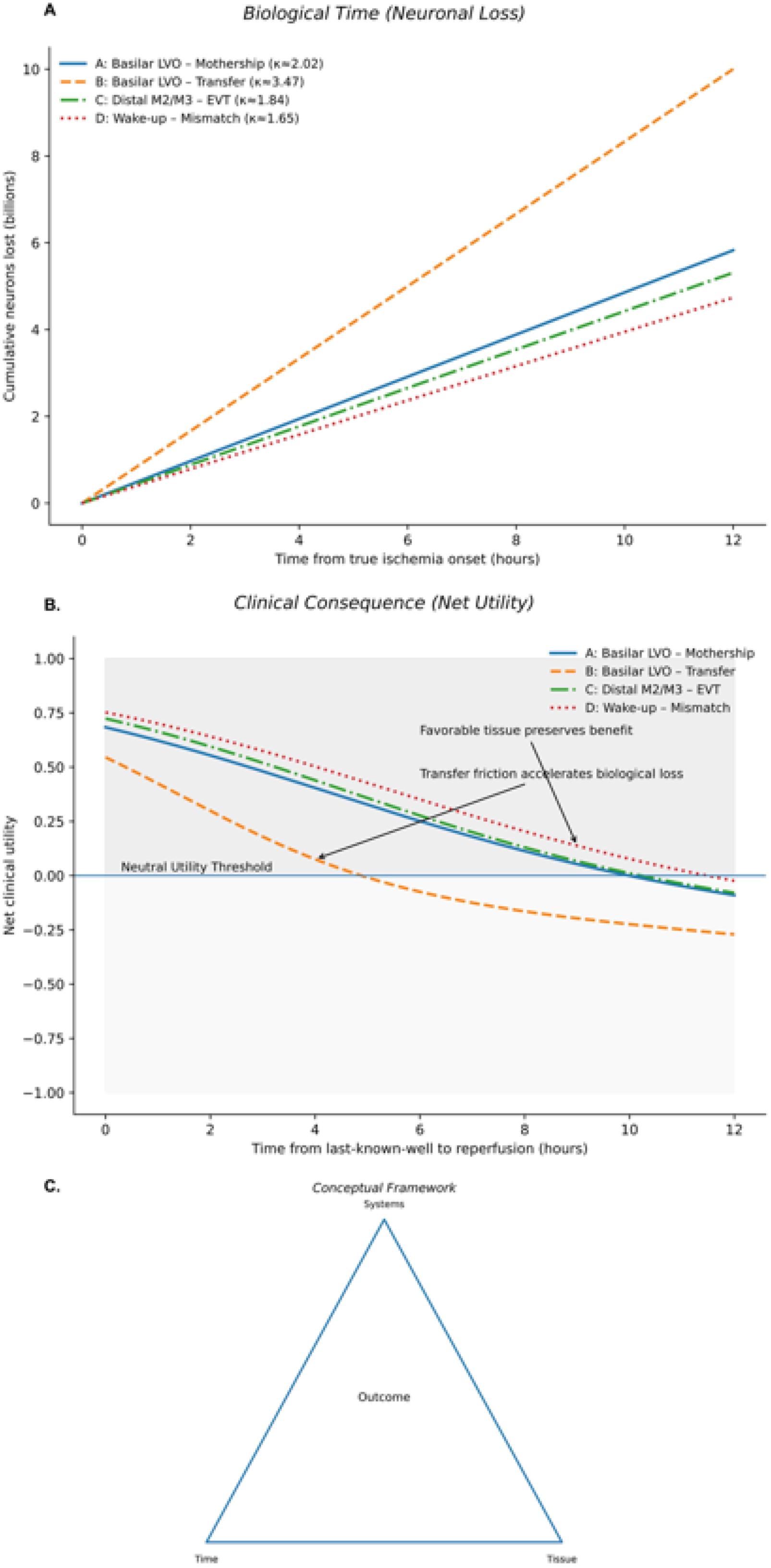
The contributions in this Special Issue exemplify each axis of the TTS model. Korol and colleagues demonstrate that stroke-related changes in tonic and phasic muscle recruitment during reaching reveal pathway-specific motor deficits, underscoring that tissue injury manifests as network-level reorganization rather than simple lesion volume. 41 Wei and colleagues integrate the triglyceride–glucose index into nomogram models predicting early neurological deterioration and 90-day outcomes in AIS patients undergoing intravenous thrombolysis, providing evidence that systemic metabolic vulnerability modifies tissue resilience. 42 Rajeswaran and colleagues, in a meta-analysis of mild stroke patients undergoing reperfusion therapy, show heterogeneous outcomes and propose SAFE recommendations, highlighting the narrow decision boundary in distal occlusions. 25 Lou’s editorial called for decoding the complexity of stroke treatment and care beyond procedural speed, emphasizing the need for conceptual integration. 43 These studies reinforce that outcome variability reflects multidimensional interaction rather than isolated factors.
Archetypes of Interaction
Illustrative Parameters Used in the Time, Tissue, and Systems (TTS) Model
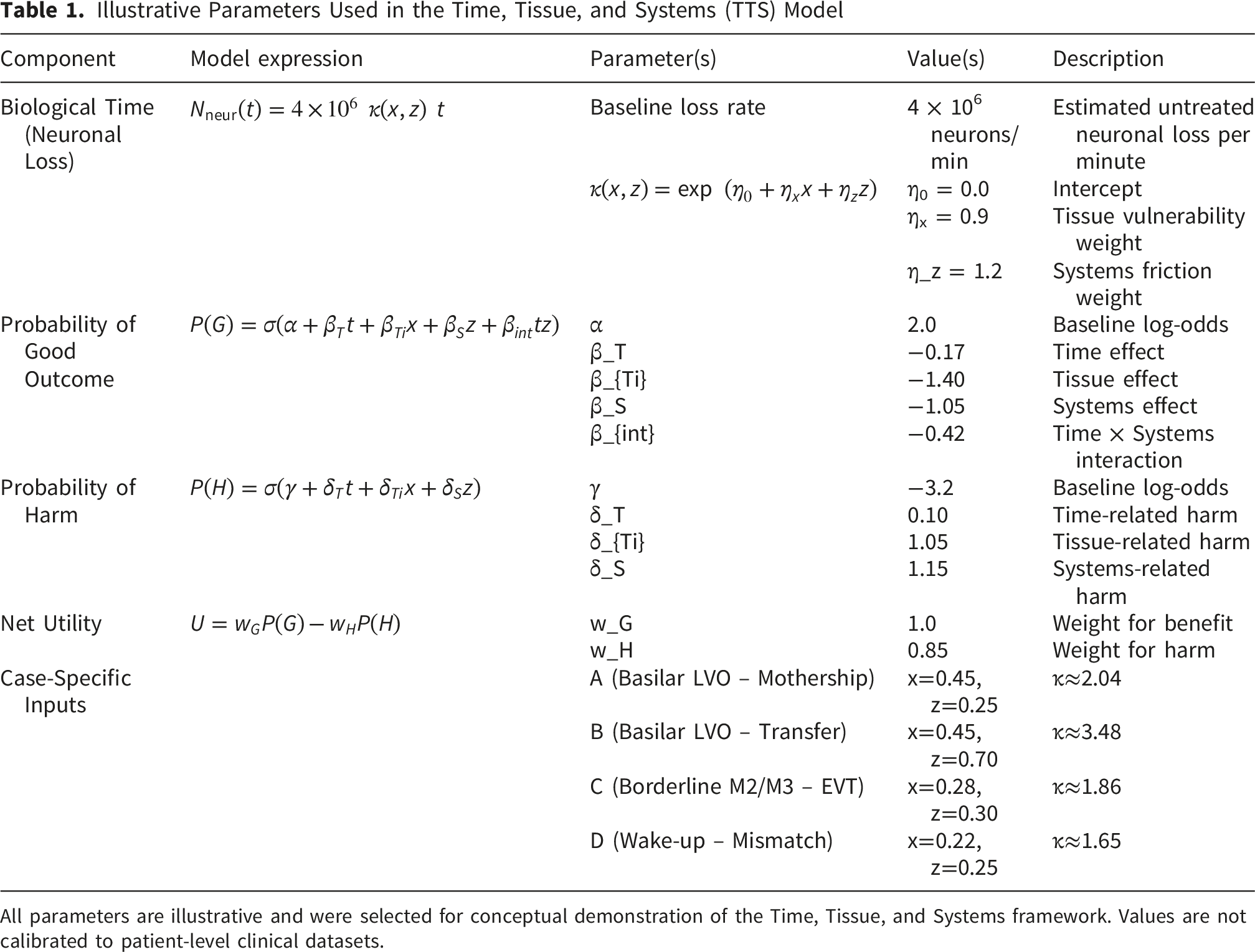
All parameters are illustrative and were selected for conceptual demonstration of the Time, Tissue, and Systems framework. Values are not calibrated to patient-level clinical datasets.
Conclusion
Stroke is not merely a race against the clock. It is a dynamic interaction between temporal progression, tissue vulnerability, and systemic response. While the maxim “time is brain” remains foundational, it is no longer sufficient to explain clinical variability.2,14,27 Biological time progresses at different rates across patients and pathways, and systems performance determines whether that progression is mitigated or amplified.20,38,44,45 The TTS framework offers a coherent, quantitative model for integrating these dimensions. By formalizing the principle that Outcome = f(Time × Tissue × Systems), it transforms urgency into measurable strategy.23,40,46 The next era of acute stroke care will not be defined solely by faster treatment, but by deeper alignment of biological time with system time.24,47
Footnotes
Acknowledgments
SB gratefully acknowledges financial support from the Japan Society for the Promotion of Science (JSPS) International Fellowship (Grant ID: P23712) and the Grant-in-Aid for Scientific Research (KAKENHI) (Grant ID: 23KF0126).
Ethical Considerations
Institutional review board approval was not required, as this article is an editorial and does not involve human participants, patient data, or identifiable information.
Consent to Participate
Written informed consent was therefore not required.
Author Contributions
SB conceived the Time, Tissue, and Systems (TTS) framework, developed the methodology and formal modeling, performed the analyses, curated and validated the data inputs, generated visualizations and outputs, secured funding and resources, administered and supervised the project, and drafted and critically revised the manuscript.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: financial support for a separate project was received through the Grant-in-Aid for Scientific Research (KAKENHI) (PI: S.B.), funded by the Japan Society for the Promotion of Science (JSPS), Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan (Grant ID: 23KF0126). S.B. was awarded the JSPS International Fellowship, supported by MEXT and the Australian Academy of Science, for the period 2023–2025 (Grant ID: P23712).
Declaration of Conflicting Interests
The author declared the following potential conficts of interest with respect to the research, authorship, and/or publication of this article: SB reports leadership or fiduciary role in other board, society, committee, or advocacy group, paid or unpaid, with the National Cerebral and Cardiovascular Center (Osaka, Japan) as Visiting Director (2023–2025); Rotary District 9675 (Sydney, Australia) as District Chair for Diversity, Equity, and Inclusion; the Global Health and Migration Hub Community, Global Health Hub Germany (Berlin, Germany) as Chair, Founding Member, and Manager; and editorial board memberships at PLOS One, BMC Neurology, Frontiers in Neurology, Frontiers in Stroke, Frontiers in Public Health, Journal of Aging Research, Neurology International, Vas-Cog Japan, TouchNeurology, Diagnostics, and BMC Medical Research Methodology. Additionally, SB serves as a Member of the College of Reviewers for the Canadian Institutes of Health Research (CIHR), Government of Canada; Director of Research for the World Headache Society (Bengaluru, India); a member of the Scientific Review Committee at Cardiff University Biobank (Cardiff, UK); Chair of the Rotary Reconciliation Action Plan (RAP), Rotary District 9675 (NSW, Australia), Scientific Adviser of Japan Connect (Osaka, Japan), and as an Expert Adviser/Reviewer for the Cariplo Foundation (Milan, Italy). These roles are unrelated to the submitted work. The funding body has no role in the study design, data collection, analysis, interpretation of findings, and manuscript preparation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the affiliated/funding organisation/s.
Data Availability Statement
All information supporting this article is contained within the main text. No additional datasets were generated or analyzed. Further inquiries may be directed to the corresponding author.