
Abstract
Typically free, accessible on-demand and easy to use, smartphone-based applications (apps) targeting mental health have expanded in recent years. This article discusses a qualitative research study with 14 young adults aged 18 to 25 years old who use apps to understand, track, and monitor their mental health. I present four vignettes drawn from a screenshot elicitation and a qualitative interview that sought to explore what is significant, socially and materially, for young adults in their usage of apps for their mental health. In this article, I examine how apps transform, interrupt, and mediate young adults’ understandings and experiences of mental (ill) health. The analysis draws on sociomaterialism to demonstrate how, at a time when digital mental health is expanding, mental (ill) health is assembled and disassembled with and through apps, and users’ experiences are enmeshed in affective intensities and entangled with technology.
Introduction
Mental health is complex matter. Critical scholarship has framed mental health and mental ill health as enmeshments of experience, sociomateriality, and biology (Cohen, 2018). In recent decades, as part of the expansion of technology in health, applications (apps) have become popular tools for mental health tracking and management, whether through user data entry, interactive conversations with robots or ‘chatbots’ powered by artificial intelligence, or inbuilt sensors, and often as a combination of these. Most freely available apps profess to target experiences associated with anxiety and depression. Mental health and wellbeing apps claim to offer a range of support; examples include mindfulness and meditation (Calm), e-counselling with remotely located professionals (Talkspace), therapeutic chatbots (Wysa), games (SuperBetter), and mood tracking (MindDoc). Apps, then, are versatile objects buttressed by the popularity of smartphones, and people's emotional attachments to and reliance on their devices (Hjorth et al., 2012). They constitute pivotal artefacts through which to examine the amplification of digital mental health.
In this article, I discuss a qualitative mixed-methods research study with 14 young adults aged 18 to 25 years old who use apps to understand, track, and monitor their mental health. I present four ethnographic vignettes drawn from a two-step process of data collection: a screenshot elicitation and a qualitative interview. The study sought to develop an understanding of what is socially and materially significant for young adults who use mental health apps. The analysis draws on sociomaterialism to demonstrate how, at a time when digital mental health is expanding, mental (ill) health is assembled and disassembled with and through apps, and users’ experiences are enmeshed in affective intensities and entangled with technology.
Background
Digital (mental) health
Accelerated by the emergence of Web 2.0 in the early 2000s, digital health encompasses personal devices including apps and wearable devices (wearables), websites and social media, government services such as My Health Record in Australia, and the collecting, processing, and sharing of large data in hospitals, research institutes, insurance companies, and pharmaceutical corporations. Critical analyses of digital health have covered many topics, for example, surveillance, privacy, and power (Lupton, 2016), pedagogical and public dimensions of online health platforms (Van Dijck and Poell, 2016), subjectivity, agency, and the digitally engaged subject (Hohmann-Marriott, 2021), empowerment (Lupton and Maslen, 2019), healthcare and digital disruption (Levina, 2017), and the digitalisation of public health (Albury et al., 2019).
While the language of psychiatry filters into everyday vernacular, mental health and mental ill health exceed their diagnoses and therapies. Definitions of mental ill health are also contingent on social, economic, and political forces (Cohen, 2018). This article uses ‘mental (ill) health’ to highlight the entanglements of lived experiences of mental health and mental ill health, and to capture the depth of participant experiences as some lived with a diagnosis, and some did not, but experienced emotional distress. Much of the critical literature on digital mental health draws on the work outlined above, alongside critiques of medicalisation to examine how mental (ill) health is produced through neoliberalism, surveillance, political interests, marketing, and the pathologisation of gendered experiences and responses to trauma (Cohen, 2018).
‘Mental health’ has long been present in discussions of digital health, partly because apps and wearables are frequently marketed as promoting ‘wellbeing’, a term that encapsulates health, mental health, physical health, and other dimensions. This is also connected to how users actively appropriate apps to suit their personal lives, thus transforming the platform itself, and the depth of user experiences that can be generated when using apps (Carah, 2020). Nonetheless, digital mental health has become a pressing concern in recent years. To some extent, this is due to the understanding of mental health data as potentially ‘uniquely sensitive under current medico-legal frameworks’ 1 (Gooding, 2019: 2 emphasis original), and the expansion of apps available freely with little regulation (Daly, 2015).
Digital mental health has received significant attention in psychiatry. While not unproblematised, apps are frequently positioned as potential aides to detect, monitor, and treat mental ill health effectively (Insel, 2018). In contrast to concerns of effectiveness and treatment, media studies scholars have examined app design and emotional politics (Stark, 2020), and how the knowledge of developers produces an understanding of mental (ill) health (Shaw and McCosker, 2019). Other research has shed light on young people's needs and priorities. Byron, for example, argues that young people's views on mental health apps can be ambivalent and indifferent; pointing to LGBTIQ+ young people's preference for ‘peer-level engagement for mental health support [that] are rarely offered by health apps’ (2019: 61). The absence of social connectedness and collective understandings of mental health from apps is often remarked upon (Byron, 2019; Fullagar et al., 2017a, 2017b). Such mutual support and informal communities can be located on social media (Hendry, 2020) or online forums (McCosker, 2017). Instead, apps tend to encourage individualised self-management of emotional distress, through ‘play, pleasure [and] quantification’ that seldom position mental (ill) health as a ‘complex social issue’ (Fullagar et al., 2017b: 5).
Sociomaterialism
To attend to the complexities of digital mental health, researchers have drawn on sociomaterialism – a theoretical lens that stresses the inextricability and mutual dependence of the social and the material. Sociomaterialism builds on more-than-human perspectives within Indigenous and African philosophies (Jude, 2017) and is associated with feminist new materialist scholars (Barad, 2003, 2007). It is particularly useful when examining lived experiences of mental (ill) health and technology because it enables careful attention to the embodiment of distress and emotions, while tracing entanglements with technology. To that end, sociomaterialism positions matter as agential, affective, and animated. Matter, Barad (2003: 803) writes, is ‘an active participant in the world's becoming’. An object, such as an app, is not ‘over there’ dormant for eventual human interaction. The object acts, stymies, and becomes. For Barad (2007: 141), the relationship between matter and humans is one of intra-activity; one does not precede the other, rather they continually become-together and are inextricable. An object is ‘over here’ entangled with humans; so too are humans always already more-than-human. The term ‘more-than-human’ connotes not the jettisoning of the human in favour of objects, rather it troubles the bifurcation of matter and human. ‘More-than-human’ underscores materiality and human as mutually affective, entangled, and involved in processes of becoming-together. Likewise, ‘humans’ are not safely enclosed by flesh, removed from the world. A sociomaterial lens underlines that humans also become-with objects, animals, spaces, tools, technology, the climate, viruses, and so forth (Barad, 2003, 2007).
Sociomaterialism productively expands the scholarship on digital mental health by focusing not on what ‘mental illness really “is,” but rather on what it “does”’ through and with technologies (Flore, 2021: 2043). Thus, mental health apps are generative materials, rather than passive objects that collect data and respond to human interaction. Indeed, unpacking the circulation of pedagogies in digital mental health targeting young people, Fullagar et al. (2017a: 6) argue that such apps can engage young people in ways of knowing that can regulate and medicalise or open up new possibilities for understanding what embodied affects ‘do’ across the spectrum of emotions from despair to pleasure.
On this view, apps cannot be considered neutral entities; they unfurl and obstruct capacities and agencies. As Lupton (2019a: 129) observes, health apps ‘possess power, intensities and agency’. They are entangled in processes of becoming-with that assemble and disassemble mental (ill) health, however, these processes do not create a ‘settled’ experience of mental (ill) health.
To return to the opening sentence of this article, an emotional state, a set of symptoms, a diagnosis, and/or shifting sociomaterial experiences, mental (ill) health is complex matter. It is a phenomenon that not only shifts in ‘meaning’, but also moves, pushes, pulls, and orientates us. Approaching mental (ill) heath through sociomateriality troubles the ability of neuroscience, an influential scientific lens in psychiatry (Rose and Abi-Rached, 2013), to fully account for mental ill health. It does not suffice to look only to biology, the nervous system, and the ‘mind’, or to connect neuroscience to big data in the case of computational psychiatry (Huys et al., 2016). Thinking through experiences of mental (ill) health, apps, affect, and embodiment necessitates a more-than-human lens that stresses the entanglements of the social and the material.
The study
This article draws on a qualitative mixed-methods research study with 14 university students aged 18 to 25 years old, living in Melbourne and Sydney, Australia. The study was approved by RMIT University's Human Research Ethics Committee and comprised a screenshot elicitation and a qualitative interview. Recruitment was conducted through snowball sampling via posts on social media and online university pages from June to December 2021. All participants provided informed written consent prior to receiving the screenshot elicitation guide, and they were asked for consent again, before the qualitative interview.
Acknowledging the large variety of apps available for download and contested definitions of what is ‘mental health’, ‘mental ill health’, and ‘diagnosis’ (Cohen, 2018), the study did not define mental (ill) health, it did not offer descriptions of what counts as a ‘mental health app’, and it did not ask participants whether they were living with a ‘formal’ diagnosis. Hence, participants were free to assemble and disassemble their personal understanding of mental (ill) health, data, and apps. This resulted in a highly rich and complex picture of how young adults are engaging with and appropriating apps, and technology more broadly, for their mental health.
Among the 14 participants, 10 identified as female and 4 identified as male. Most were born in Australia and reported a variety of ethnic and cultural backgrounds such as Han Chinese, Middle Eastern, Jewish, Russian, Vietnamese, Indian, and Australian. Several participants identified as lesbian, gay, or bisexual, and some identified as heterosexual. In addition to being students, several worked part-time or casually. All were assigned pseudonyms and other identifying details, such as ages and significant locations (e.g. hospitals or clinics, educational institutions, and workplaces), were removed from the transcripts.
Screenshot elicitation
Screenshot or photograph elicitation enables an in-depth engagement with a smaller group of participants, thus adding layers to the data and the quotidian of app usage. Bringing together app-generated content and qualitative interviews enables a nuanced and detailed discussion of digital mental health where self-tracking, data, and mental (ill) health become-together. Media such as photos can demonstrate hidden, surprising, and ambivalent dimensions of mental (ill) health (Jaynes, 2019; Ownby, 2017). Participants were invited to email 3 to 5 screenshots of the apps they used, and they were free to send more images if they wished. This resonates with Jaynes’ (2019) description of the ‘social life of screenshots’ which captures how a seemingly innocuous practice – taking screenshots – is imbued with layered social and emotional meaning. While a brief guide was emailed to participants, the process aimed to encourage them to independently document what has value and meaning – positive, negative, ambivalent – in their usage of apps for mental health. Although the focus of the study was on apps, participants were encouraged to send images of wearables, if they used them to understand, track, and manage their mental health. A few participants availed themselves of the option. Photos evince what has presence and meaning in people's lives, while offering participants other ways to represent their mental (ill) health experiences alongside qualitative interviews.
Qualitative interview
The interviews were conducted on a digital meeting platform or over the phone, depending on internet stability and equipment, and lasted 53 to 97 min. In the interviews, participants traced their histories and futures of mental (ill) health alongside their usage of technologies (Brennen, 2021). The narrative often took the shape of ‘techno-biographies’, where apps, smartphones, laptops, and other media, were adopted, changed, and sometimes discarded as participants’ lives moved. The interviews were semi-structured and explored experiences of using apps for mental health, including a discussion of each photo or screenshot emailed, broad understandings of mental health and the role of technology, what prompted and/or altered their use of apps, how they understand and engage with their data, and views on limitations and benefits of apps. Participants were emailed $50 vouchers to thank them for sharing their experiences.
Analysis
Following professional transcription, the data were managed and coded using NVivo. I conducted a preliminary analysis through a reflexive thematic process that generated dominant themes, diverging ideas, and patterns and tensions in the data (Braun and Clarke, 2019). To add depth and nuance to the analysis, during each interview, I followed the participant's narrative by writing ethnographic fieldnotes in a notepad. After the interview and upon receiving the transcripts, I returned to the notes, recording, photographs, and transcript to develop a vignette detailing each participant's background, lived experiences of mental (ill) health, their views and expectations of apps, and notes on everyday life, family situation, hobbies. The fieldnotes, photographs, and transcripts all formed the material for my analysis, enabling a process of ‘plugging in’, where data refer not only to what is captured from participants, but also to what is made with participants, alongside fragments of my notes, and sociomaterialism (Mazzei, 2014). Thus, the analysis unfolded as moments of ‘plugging in, of reading-the-data-while-thinking-the-theory, of entering the assemblage[s], of making new connectives’ (Mazzei, 2014: 743). This type of engagement with data involved ‘dwelling’ with participants’ stories and photos and reflecting on my personal experiences of mental (ill) health and technology, ideas and comments, and position as a researcher. This layered process enabled the development of ethnographic vignettes, and the selection of four that reflect the commonalities, trends, and divergences across participants. Ethnographic vignettes can convey the ‘messy and entangled relationships between concepts as they actually occur within the field’ (Jarzabkowski et al., 2014: 280). They offer a contextualised snapshot of participants’ experiences with digital mental health artefacts. The vignettes represent key characteristics across participants – a frequent user for whom data patterns are significant, an occasional user of a single app, a chatbot user, and a wearable enthusiast.
Vignettes of Ari, Thea, Steve, and Joni
Ari
Ari is a part-time student. She referred to her ‘brain’ and her mental health as her ‘full-time job’. For Ari, her smartphone is ‘indistinguishable from myself’, using a range of apps for her mental health including Calm, Clue, Spotify (for meditation), Calm Harm, and she referred to her iPhone AirPods as a wearable that she uses for mental health, and her laptop, which is important for contact with her therapist. While she has several apps, Ari uses Calm and Clue most frequently. She shared that she has experienced anxiety, depression, and physical illnesses, and has a lived experience of attention-deficit/hyperactivity disorder (ADHD). Her app use is not directly related to her diagnosis, rather she assembles support targeted to her experiences through multiple tools. Ari explains that a psychologist first recommended a mood tracking app five years ago. From there, she began trying several apps and she views her need for variety in apps as reflecting ADHD: I can’t seem to explain it to anyone who doesn’t have ADHD […] I’ve tried many different things, and they’ve all been effective, but then no longer work for me. […] For the first three months, having a notification at the same time every morning to be like ‘take your meds’ works, and then at some point […] it just stays there. But I’ve learnt to […] accept that that's who I am, and I need that variation, rather than trying to force something when it's no longer working.
Her comments evoke the becoming-together of ADHD, apps, and their functions (notification), and the need for ‘variation’. Becoming attuned to the apps is temporary; the connection with and usefulness of the app does not last, and she feels the need to move on as her mental (ill) health intra-acts with her apps.
As a researcher of digital mental health, I have downloaded and intermittently used several mental health and wellbeing apps, however, the diversity of apps mentioned by participants led me to seek information online about each of them. This was an important step to develop an understanding of the promissory discourses at work. Clue is a popular app – most participants who menstruated used it – for tracking menstrual cycles. The app can track fertility, and predict cramps, hormonal and mood changes, and premenstrual syndrome (Clue, 2021).
Like many (Hohmann-Marriott, 2021), Ari views her mental health as connected to menstruation and hormones, in addition to mentioning the functioning of her brain several times. As shown in Figure 1, ‘emotions’ and ‘mental’ are key features of Clue. Ari explains: [Clue] has all the different things of how to do sleep and what are your emotions and your mental capacity right now, and I find [tracking] really helpful, if I’m distressed and then I notice that my period's coming, then I can be like ‘well, that might be why’. […] having that kind of data, tracking over time, helps me to locate where I am on the mental wellness scale of ‘okay, you’ve said that you’re really depressed for four weeks now; this isn’t getting better over time, maybe it's time to look at medication, or doing more therapy, or looking to an inpatient admission’ […] It's helpful because my brain can’t be relied on to know what's happening.
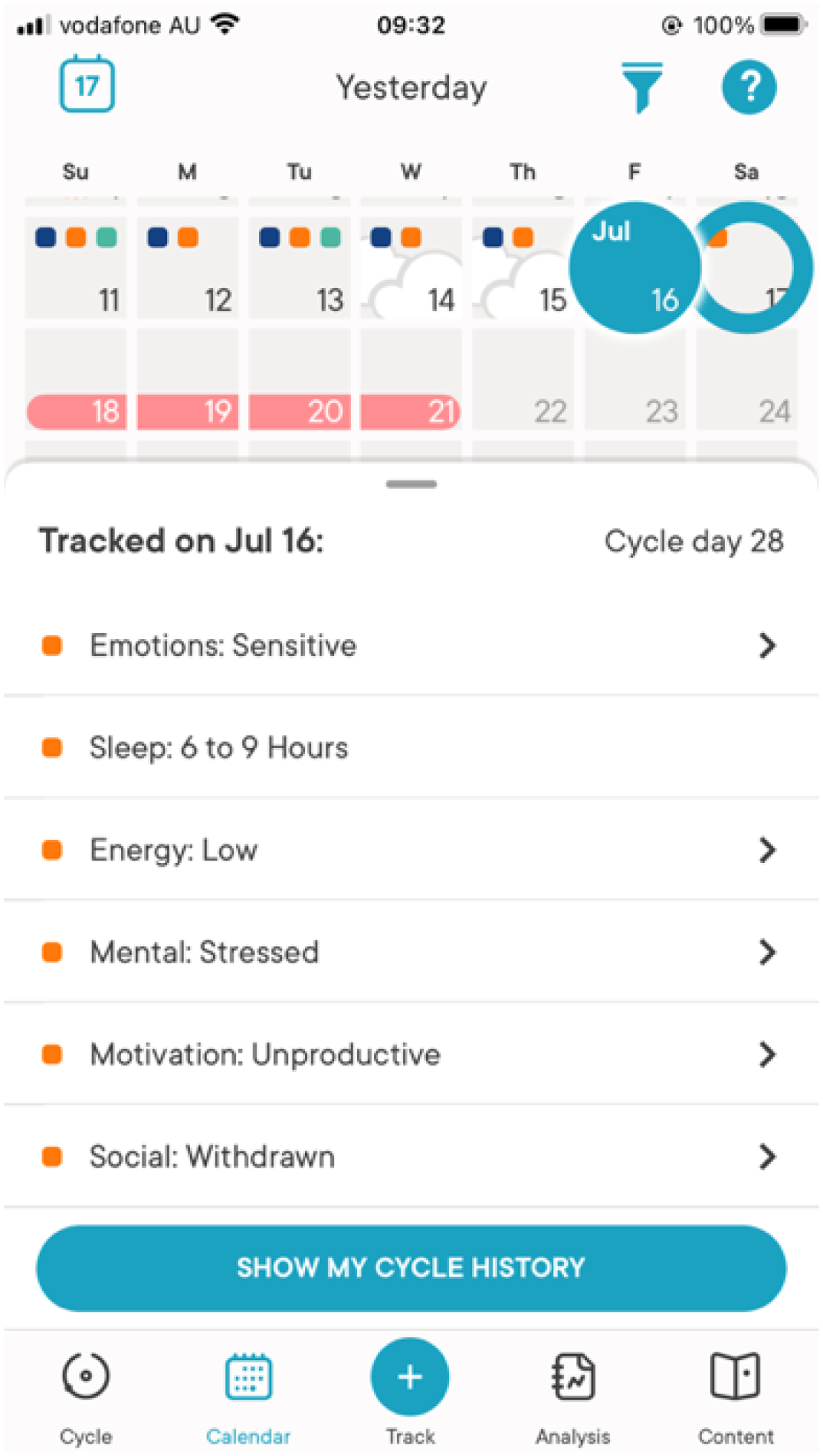
A screenshot of Ari's Clue app.
She shared that she has a paid subscription for Clue that unlocks ‘more specific analysis’. Clue uses machine learning to process user data (Mack, 2016). Automated functions powered by machine learning include ‘advanced period predictions’ and ‘recurrent symptoms analysis’ (Eckersley, 2021). Through Ari's comment above, we can see a process of assembling and disassembling experiences, practices, and data to assess her ‘emotions’ and ‘mental capacity’. Further, seeing data patterns is crucial for Ari: ‘we need to know the patterns so that when you’re okay, you can do that thing for your future self’. The ‘thing’ is the emotional labour enacted through the app. Tracking over time and visualisation are key here because, as she says, ‘my brain can’t be relied on to know what’s happening’. She added that paying for a subscription makes her feel ‘good about supporting them, as an app and as a company’, demonstrating the affective connections produced through software, technology companies, and mental health.
One of the more surprising aspects of asking participants for screenshots or photographs is the unexpectedness of meaning that participants draw from seemingly ‘simple’ photos. An example of this is another participant who sent photos of their AirPods as well as app screenshots. Figure 2, likewise, does not generate resonance with my lived experiences – having tried and abandoned several guided meditation apps (and upon receiving this screenshot, I was concerned that I had not provided sufficient guidance to participants). However, for Ari, this was her ‘favourite part of the app’, and this is intimately tied to her understanding of mental (ill) health and the embodiment of breathing. Calm is an app specialised in sleep and meditation that several participants found useful. Its website notes that the app can ‘reduce stress or anxiety’ (Calm, 2022). Ari values viewing data on how many meditations she listened to: ‘I like patterns and data and proof of things’. She shares: [I]t's my favourite part of the app […] I love the breathing with the visual cue because […]. If I’m anxious and you start hyperventilating, and then you get dizzy, or your face is all tingly and stuff. It's not easy to just breathe, so having that there and being able to watch it […] it does sound and visual, and your breathing, and that's enough things that there's not really space in your brain to also freak out.
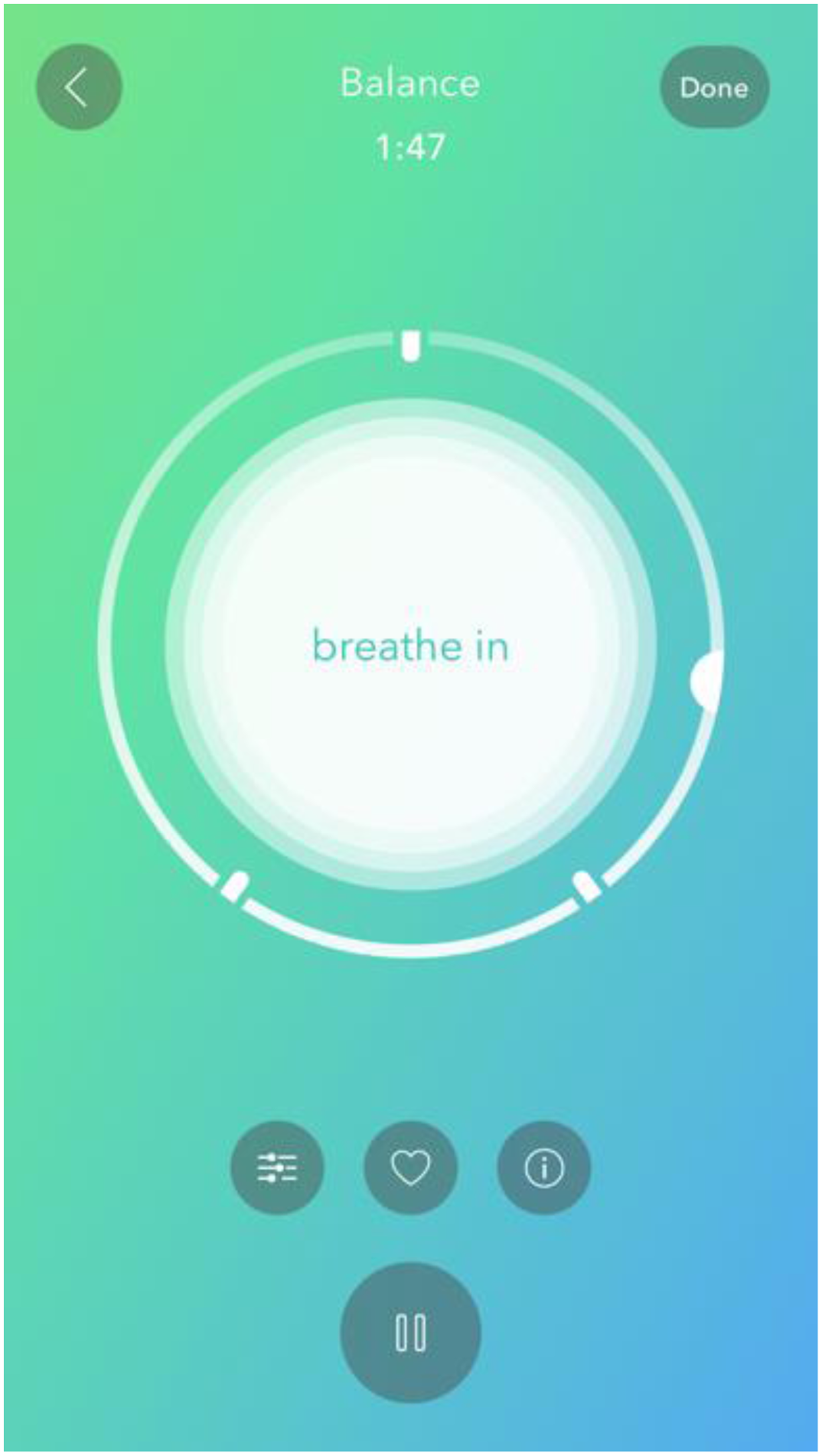
A screenshot of Ari's Calm app.
The embodiment of emotional distress is powerful here. Ari describes being ‘anxious’ as entangled in the guided breathing exercise of the app. Focusing on the app, breathing, and visuals, enables her ‘brain’ to not ‘freak out’.
Thea
Thea is a student who is employed casually. She explained that mental health became particularly important when she began experiencing chronic pain in recent years. Unlike most participants, Thea uses only one app for her mental health: MindDoc. However, the connections between physical and mental health hold several commonalities with other participants. Thea seemed reluctant to share specificities about any health diagnosis. She preferred to discuss the app, and the benefits to her mental health and physical wellbeing more generally. During our discussion, it was difficult to engage Thea in detailed discussions about what she gains from using apps for her mental health; my sense was that she preferred broad discussions and was careful not to disclose ‘too much’ to a stranger-researcher. This was compounded by an unstable internet connection during the interview.
MindDoc (2022) is a ‘modern online psychotherapy and self-help for your mental health’ – it claims to be helpful whether ‘you are suffering from depression, an eating disorder, anxiety or compulsions’. Having downloaded the app several years ago, when it was called MoodPath, but never used it due to the daily tracking required, I was curious about Thea's experiences. She encountered MindDoc through Instagram advertising. The app attracted her because it mentioned ‘managing both your emotional and physical wellbeing’, and she now records levels of pain and how she is feeling daily.
Figure 3 provides an example visualisation of Thea's tracked mood at the start of September (the interview occurred in mid-September), and Figure 4 shows the kind of mental health information provided by the app. MindDoc asks Thea questions each day and conducts analyses based on her responses. The questions vary daily, and she gives ‘Have you felt that you’ve had less energy than usual lately?’ and ‘Have you felt like you’ve had other people to rely on lately?’ as examples. She explains further: [The app will] either target specific questions for you or you can choose words to describe your emotions, or you can just write what you’re thinking about. […] I use the ‘what are you thinking about’, section to put pain levels and then answer the questions […] I choose the emotions that I’m feeling and so that allows me to match [with my] mental health.

Screenshots of Thea's MindDoc app.

Thea has devised ways to make the app work for her, so that her mental and physical health are connected to the data. It is also an example of how she appropriates the app as she responds to ‘what are you thinking about?’ by focusing on levels of pain.
Like many participants tracking mood and other health data, Thea commented on the requirement to give ‘enough’ data. MindDoc ‘prefers you do it three times a day’ and she often cannot keep up. In these cases, she describes MindDoc as ‘not happy’ because the responses are not frequent. Nonetheless, she finds that the data visualisations help her reflect on her mental health and her experience of chronic pain: it helps me notice that I’m not always feeling this way […] because sometimes you can just get into a loop of like, ‘I’ve always felt like this. This is how it always is’. If you’re having a really rough two weeks or whatever, it can be hard to get out of that headspace and realise, ‘I actually can be happier, and I have been even though not much has changed’. That is something I can do and it's the information I can use to try and change my thinking.
Mental ill health emerges as a repeated pattern that is sensed (‘I’ve always felt like this’) and challenged through the app (‘I actually can be happier’). When she realised that the app could help ‘change her thinking’ and address certain aspects of her mental health, Thea decided to use the app when she is ‘feeling good’, as she was only using it to record ‘feeling really low’. Her usage points to the agential aspects of a mental health app whose actions are not only therapeutic when one experiences distress, but also, an app that needs data and continual engagement, to generate an apparently more accurate pattern of Thea's mental (ill) health. This accuracy, of course, is far from settled as Thea explains that one of the frustrating aspects of MindDoc is the assumptions that the app sometimes makes. She recounted how she was once given the question ‘Do you feel uncomfortable doing certain actions in front of people?’. Her responses led the app to erroneously conclude that she was experiencing social anxiety. This demonstrates the app is not ‘reading’ Thea, and her rejecting the interpretation of the algorithm. Likewise, Thea's interest in MindDoc seems to be strictly about tracking, rather than self-care suggestions such as meditation, as she remarks: ‘I was more interested in recording [moods and levels of pain], than necessarily looking at the suggestions from this app’. Despite the app assembling tracking with mental health support, Thea chooses to disassemble these threads and re-assemble self-care through non-digital means such as baths and walks.
Steve
Steve is a full-time student, who also works casually, and volunteers. He has a lived experience of depression. For him, turning to technology for mental health support, which began in high school, ‘always made sense, because you always have your phone’. Steve's interview also raised the issue of stigma and family support as he shared that his parents do not know about his experiences of depression, and he seemed to want to speak softly and very close to his microphone during the interview – at the time, I thought this may be because he was living with his family.
Alongside using multiple apps, Woebot, OurHerd, Perspective, Health on iPhone, and Smiling Mind, Steve sees a therapist. Like many participants, Steve has several apps, including ones he does not use, and he does not delete them. For him, preserving the apps reflects affective intensities that emerge with app usage: ‘I want to look at it in the future, or it’s an archive of what I’ve felt, […] it’s those kinds of files. […] it is an overview of [my] progression’. The ‘progression’ refers to his mental health, and how he has understood and monitored it through technologies. Back to his present, however, during our conversation, he discussed his use of Woebot in detail. Unlike Thea and Ari, Steve uses the app only when he experiences distress. He enjoys the versatility of Woebot, noting that he has used it in bed, and discreetly at the library and on public transport as he cannot access his therapist ‘on-demand’ when he feels distressed.
A chatbot powered by artificial intelligence, Woebot's website describes the app as ‘your personal mental health ally that helps you get back to feeling like yourself’. The on-demand, 24/7 aspect of the chatbot is also underlined: ‘There's no such thing as appointments or waiting rooms here’ (Woebot Health, 2022). I was intrigued to hear his thoughts on the app as Steve was the first participant that I interviewed who uses chatbots. He describes the app as generating positivity, although, he says, he is cognisant that the algorithm is ‘not actually interested’: when you’re using it, there is an awareness that it's not a person that's saying nice things. If it says something ‘oh, it's good to see you again’. I’m aware that it's not actually interested – it doesn’t have an awareness of whether I am there or not, it's the automated prompt. But I think it's still okay, because […] you see a comment ‘I wish you the best’. […] It's still a positive thought, and if you can adapt it to be your own.
As a user of Reddit, Steve finds the stories that he encounters online as ‘looping through negative thoughts’. This resonates with research showing that while young people can obtain support online, it remains rife with tension (Hendry, 2020). He contrasts this with Woebot which provides ‘positive affirmations, or positive support’. Likewise, Steve comments on using OurHerd, an app developed by the youth mental health organisation batyr (batyr, 2022). OurHerd (2021) is ‘a storytelling app that empowers young people to share lived experience stories and use their collective voices to create a more mentally healthy world’. Steve's connections to OurHerd are affective and relational as he notes he has a sense that he is not alone in experiencing depression. One of the aspects he enjoys the most about the stories on OurHerd (unlike ‘the subreddit depression’), is that they show ‘this person has gone through this problem, but then they had that kind of change’, which he feels is more hopeful and optimistic. Hope was an important experience, necessity, and desire for all participants, though its presence, absence, and transience, were complex in their lives.
Woebot's suggested ways for Steve to practice self-care were applied in his life. He sent Figure 5 as an example of the app recommending that he does some relaxing exercises: [Woebot] tells you, ‘Why don’t you go and relax?’ And then it was like, okay, I’ll do that. […] I think it's helpful it has that remembering, and asks you how that went, and you can respond. […] And then, I’ll just go back and say what do I think of it, did I think it was good or bad, something like that.
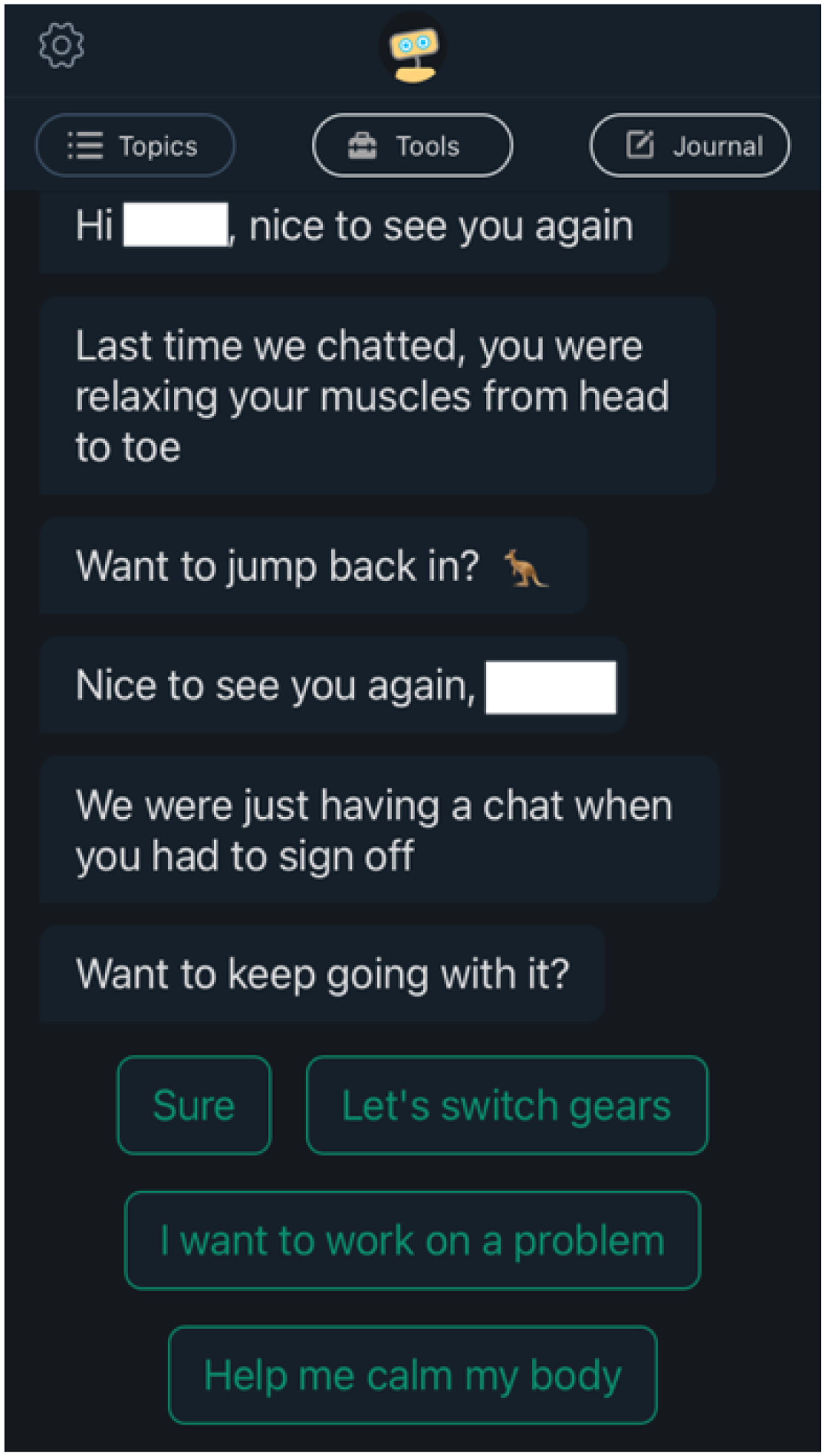
A screenshot of Steve's Woebot app.
The capacity of Woebot's algorithm to recall how he felt, what was suggested, and ‘debrief’ afterwards is positive. The app and Steve emerge together in relationality as he inputs how he feels, what he wants to work on, and Woebot responds and remembers their conversations.
Although these exercises and the app's ability to check in with Steve were appreciated, he is dissatisfied with how Woebot deals with sensitive issues: sometimes […] you notice, it's just going to loop again […] I think that's particularly a problem when it's about something that's very sensitive, like suicide. So, basically it says ‘okay, you’ve mentioned suicide’. What is the suggestion? ‘Okay, you go there, to these emergency numbers’. That's kind of it. It doesn’t have that advanced functionality to talk about suicide. It's not that helpful.
It seems that Steve has tried to have quite profound discussions with the chatbot and sought help for thoughts of suicide. The honesty and trust that one can have with an app as opposed to another person was an observation made in several interviews. One participant spoke of being able to respond to questions about alcohol and drugs more honestly on an app, because of the absence of judgement. This was also reflected in Ari's comments, who did not use chatbots, but referred to the bot as talking to herself, and felt that she would be ‘more likely to be honest and self-disclose’ her emotions and mental health to ‘myself’. For Steve, however, the chatbot's capacity to respond to disclosures of suicidal thoughts in a meaningful and supportive manner – beyond providing emergency numbers – is highly limited.
Joni
Joni studies full-time and works casually. Her parents experience complex mental ill health, and she is their carer. She spoke of becoming aware of the importance of mental health as a teenager when she felt anxiety and distress related to her parents’ mental ill health. Joni uses several apps including Headspace, Calm, and Smiling Mind. Like most participants, Joni's use of apps for her mental health started when she acquired a smartphone. She comments, ‘for [my] generation, [the smartphone is] something that they can harness already at their disposal every day. […] why not help it be something that can be really helpful when they need it?’ Her comments echo Steve's and Ari's, who both felt that the device they spent the most time with and on, and the data they generate, can be harnessed for ‘good’.
Joni's Fitbit, along with Fitbit Relax and Calm, stood out as most helpful to her experiences. She was one of five participants who mentioned wearables as a mental health technology and/or sent photos of their wearables. Three of the images Joni sent depicted her meditating. These photos are not reproduced in this article to preserve Joni's anonymity; however, she spoke at length of the Relax app on her Fitbit.
Fitbit's website notes that Relax ‘can help you find moments of calm throughout the day with personalized, deep breathing sessions’, and deep breathing ‘can help you let go of stress and maintain a quieter state of mind’ (Fitbit, 2022). Joni explains the functions in Figure 6: the line down the bottom is telling you how long you’ve been using it for, and the blank space is where you’ll end up. The circle in the middle changes throughout the course of the meditation, so it changes size. Fitbit […] reads whether you’re breathing or not in the right way, and so it will say to you slow your breathing, and then these other little stars and circles will appear.
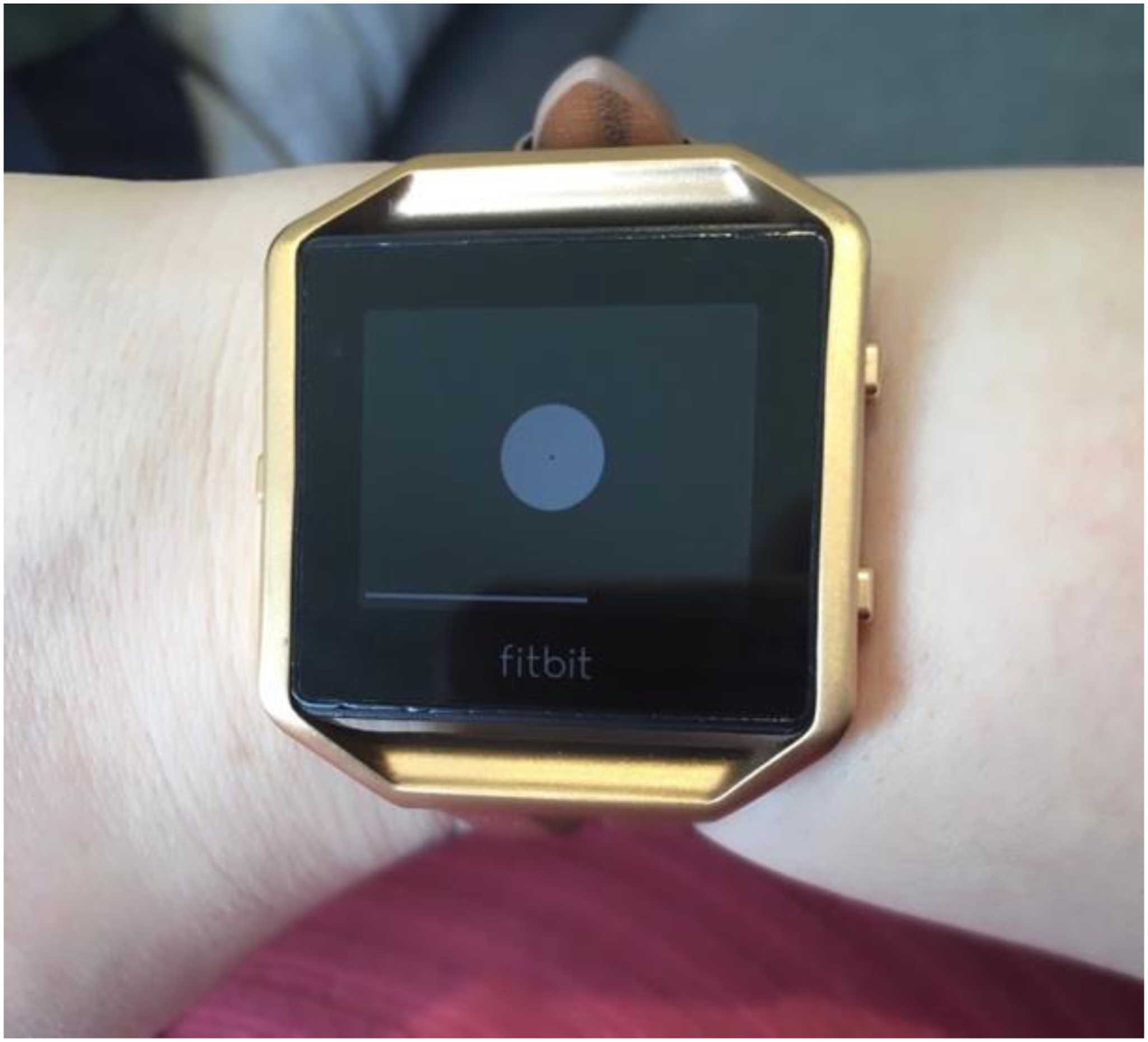
A photo of Joni using Relax on her Fitbit.
Researchers have examined Fitbit's agentialism in the production of health and illness (Lupton, 2019b). Wearables in mental health are emerging technologies and Fitbit recently filed a patent for the detection of depression and bipolar experiences (Stables, 2021). This innovation points to the expansion of sensors within wearables aiming to address ‘signs’ of mental ill health. These potential capacities are at work in Joni's experiences. While she expresses some scepticism about how data are interpreted by the algorithm, the description above shows that not only is she knowledgeable about the functions of the app-wearable, but also, she has learnt to ‘slow [her] breathing’ to manage anxiety through the technology.
The ability to address anxiety inconspicuously was highly valued (like Steve). Joni's experience demonstrates the versatility of apps and wearables in exceeding the spaces of the clinic and generating therapeutic spaces. She recounts using the app-wearable at university: Fitbit is fantastic […] if I’m feeling a bit anxious, I can go on there and subtly do a small piece of mindfulness without other people knowing about it or even realising, which can be really helpful as well when you experience generalised anxiety, which might just come up at random times. […] there was a particular subject [at university] around violence and abuse […] there were a few classes that were difficult, and I would excuse myself and […] sit outside […] and do my Fitbit [Relax] for a few minutes.
Joni also notes later in her interview that she uses the app-wearable on public transport when she experiences sensory distress due to noise and crowds. In that sense, she also describes how the flexibility of the app-wearable can provide therapeutic support in different situations. For example, using technology without headphones is useful at university when she wants to be discreet. However, to deal with noise and crowds, she prefers guided meditation because ‘you [need] to be anchored by someone describing something to you’. The intra-active relationality between the app-wearable and Joni generates mentally healthy spaces or spaces where mental (ill) health can be addressed. This kind of affective relationality is important because it highlights how mental health becomes (dis)assembled as Joni moves in her life and daily activities.
Concluding discussion
Digital mental health is on the cusp of accelerated innovation. Powered by artificial intelligence and automation, apps and wearables for understanding, tracking, and monitoring mental health continue to appear on the global market. This article sought to examine how young adults experience mental (ill) health through and with apps. The analysis showed that apps (and, for some, wearables) are not passively experienced. Apps are part of wider systems of communication in which activities are ‘digital bit trails’ in a large infrastructure (Lomborg and Frandsen, 2016: 1020). Through app usage, mental (ill) health is (re)made, (re)located, and (dis)assembled depending on the context, experience, and needs. A sociomaterial lens highlights the affective intensities and productions of mental health enacted through app usage. The ethnographic vignettes provide insights into how users and apps relationally intra-act in a complex assemblage with many other actors (other technologies, familial relations, to name a few). This assemblage challenges some of the more clinical-psychiatric discussions of apps and wearables that tend to narrowly focus on whether a technology is ‘effective’ on defined ‘symptoms’. The vignettes add nuance to this perspective not by rejecting effectiveness or symptoms, but by affirming the sociomaterialities of experiences, and of apps themselves. The vignettes revealed the versatility of apps in bringing together many aspects of participants’ lives. As a result, most participants used several apps (and/or wearables) to track their mental health and produce tailored support, demonstrating how mental (ill) health is diffused between technologies, enacting multiple embodiments, affects, and experiences. Such complex assemblages reveal the intractability of embodiment in sociomaterialities of digital mental health.
Apps are programmed and assembled within complex sociomaterialities, which are themselves unstable. Apps are, for instance, not designed to address one diagnosis, as though diagnoses were unitary, homogenous experiences; rather they are programmed for an assemblage of experiences such as loneliness, ‘low’ focus, motivation and engagement, stress, and so forth. They are also not ‘one’ technology; they combine algorithms, sensors, and some are merged with wearables. The way they are made is important as the knowledge and assumptions of programmers bear upon the experience of the user (Shaw and McCosker, 2019) – for example, the misidentification of Thea's social anxiety and the need to provide more data to the app, and Steve's frustration regarding sensitive discussions.
In the vignettes, participants’ stories and descriptions of images showed the affective relations generated through and with technologies. Several participants spoke of their apps with affection and considered them important, if not essential, for their mental health. However, Steve's vignette also indicated the inability of apps to cope with affective intensities and sensitive issues such as suicidal thoughts. This finding resonates to some extent with the literature exploring the limitations of apps for complex mental ill health and thoughts of suicide and self-harm (Sander et al., 2021). However, Steve's desire for a technology that can respond meaningfully cannot be sidelined. Through a sociomaterial lens, desire is productive and yielded by/from multiple forces, pointing to how data ‘feels’. For Ari, the feel of data and mental (ill) health is connected to her brain. Considering how the language of neuroscience and biology are part of the promissory discourses of many apps, analyses of digital mental health must consider the function that ‘science’ has in understanding, tracking, and monitoring mental (ill) health.
How mental health is embodied and digitalised through the app is vital for users. Alongside this were daily practices of tracking and labouring. This dimension of mental health apps was frustrating for some, revealing the affective labours that technology obliges. This was a nuanced experience; for Ari, data tracking meant ‘proof’ of her emotional state, while for Thea, it revealed that her mental health can improve, though she noted that apps want more data. Despite this, the vignettes showed that some users resist this request, and use it when they remember (to some extent, Thea) or as needed (Steve and Joni). For others still, this constitutes a pedagogical possibility as they spoke of apps becoming resonant in their lives over time, as they learnt to use the functions.
Aspects of pedagogy and embodiment were reflected in Joni's discussion of learning deep breathing through Fitbit – an example of the techno-pedagogy disseminated. Moreover, those techno-pedagogies were also located elsewhere in the interviews. For example, while several participants acknowledged privacy and data security as issues, for most such as Joni and others, this was framed as a pedagogical ‘problem’ (Fullagar et al., 2017a, 2017b), that is, they wanted to be more educated about how data are used and managed, rather than reject the technologies. Of interest, this imbricated the researcher as several participants asked me questions on this topic. The acknowledgement of my position as a researcher in the humanities, rather than in computer science, was important in my engagements with participants.
While this article contributes to critical studies of digital mental health, it is important to acknowledge limitations that point to directions for qualitative social research. University students are an educated cohort who tend to experience less digital inequality. It is important to consider how social and economic inequality condition experiences of mental (ill) health and access to technology, as well as how these can be addressed. So too is it crucial to capture the experiences of young adults living in developing economies. In addition, although the recruitment strategy endeavoured to include gender-diverse participants, respondents mostly identified as female. LGBTIQ+ engagement with technologically mediated forms of mental health care needs further research to develop meaningful and accessible supports that respond to lived experiences.
How digital mental health generates capacities, attunements, and embodied experiences of mental (ill) health is contingent and unsettled. This article has discussed how users assemble and disassemble mental (ill) health through apps (and wearables). This process changes over time as apps are used and discarded, however, affective resonances with past and present continue to resonate as data become records of mental health trajectories. The states of mental ill health and mental wellness are not homogeneous; they shift in meaning as users move in their lives. As such, part of my intervention in this article points to the partiality of studies of digital mental health focused on stable symptoms or diagnoses in the humanities and in the clinical sciences. If we are to develop nuanced understandings of digital mental health across the spectrum of experiences, we ought to approach mental (ill) health as complex sociomateriality.
Footnotes
Acknowledgements
Special thanks to the participants who generously shared their experiences, particularly at a time when they were facing many challenges due to the global pandemic. Thank you, also, to the anonymous reviewers for their insightful comments on my article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a RMIT University Vice-Chancellor's Postdoctoral Research Fellowship. This research was conducted by the ARC Centre of Excellence for Automated Decision-Making and Society, and funded partially by the Australian Government through the Australian Research Council.