
Abstract
The National Health Service in the United Kingdom is one of the most diverse healthcare systems globally, yet global majority women healthcare professionals from racialised and migrant backgrounds continue to experience entrenched inequalities. Their careers and well-being are shaped by the intersections of race, gender, religion, and migration status, producing compounded barriers and distinctive resilience practices. This study explores the intersectional challenges and resilience strategies of global majority women healthcare professionals in the United Kingdom, with a focus on how overlapping identities shape both disadvantage and coping. Drawing on in-depth qualitative interviews with 37 global majority women professionals across multiple healthcare roles, the study employed an intersectional feminist framework to analyse lived experiences. Thematic analysis identified patterns of marginalisation and the strategies participants used to sustain careers and well-being. Participants reported compounded professional marginalisation, cultural–religious barriers to workplace integration, motherhood penalties intensified by migration, and psychological strain. Structural exclusion within healthcare organisations further amplified inequities, often through neglect rather than overt hostility. Despite these challenges, participants demonstrated resilience through spiritual anchoring, collective resource mobilisation, strategic time management, and career restructuring. However, these strategies often displaced responsibility onto individuals and families, while institutions benefitted from their adaptability. Global majority women healthcare professionals experience intersecting structural and cultural barriers that undermine career progression and well-being. Their resilience not only highlights agency but also reveals systemic inequities that remain unaddressed. Organisational and policy interventions must move beyond individualised resilience models to dismantle structural barriers and create inclusive healthcare environments.
Keywords
Introduction
The United Kingdom’s National Health Service (NHS) is among the most diverse healthcare systems globally, with 44% of doctors and 25% of nurses identifying as having an ethnic minority background (General Medical Council, 2023). While this diversity enriches the workforce, it conceals persistent inequalities. ‘Global majority women’, a term used to describe women from racialised, and migrant backgrounds, continue to face entrenched disadvantages shaped by the intersecting axes of gender, race, religion, and migration status (Adisa et al., 2021; Ismail et al., 2025; Kline, 2014). Evidence highlights their disproportionate exposure to psychological distress, restricted career mobility, and retention concerns (British Medical Association, 2021). These challenges have been intensified by the COVID-19 pandemic, which heightened workplace discrimination and health risks for global majority women healthcare workers.
Traditional research often isolates gender, race, or migration in explaining workplace inequalities. Such single-axis analyses, however, fail to capture the lived realities of global majority women professionals, whose experiences are shaped by the simultaneous operation of multiple systems of oppression. This fragmented approach limits both theoretical understanding and the effectiveness of interventions aimed at equity and inclusion. Intersectionality theory (Crenshaw, 1989, 1991) offers a critical lens for addressing this gap. It highlights how overlapping identity markers generate unique disadvantages, and how apparently neutral practices can reproduce inequality (Bowleg, 2012; Rodriguez et al., 2016). Within healthcare, hierarchical professional cultures intersect with wider societal inequalities to marginalise global majority women, often excluding them from networks, slowing progression into leadership, and subjecting them to stereotyping (Bradley et al., 2023; Braithwaite et al., 2016). Migration further compounds these dynamics, as women frequently face the ‘triple penalty’ of gender, ethnicity, and immigration status (Hardill and Macdonald, 2000; Humphries et al., 2019). Visa dependency deepens insecurity and constrains career flexibility, especially for those balancing caregiving responsibilities (Beech et al., 2018; Warren, 2022). Religion adds another layer: Muslim women, for example, often confront Islamophobic stereotyping and conflicts between institutional routines and religious practices such as prayer or modest dress (Ghumman and Ryan, 2013; Linando, 2022).
Despite growing recognition of these issues, two gaps remain. First, the experiences of global majority women healthcare professionals are still underexplored in UK-focused feminist and organisational research, even though they are central to workforce sustainability and equity (Akanji et al., 2020; Lommel, 2024; Mordi et al., 2023). Second, resilience scholarship in healthcare has often treated resilience as an individual trait, neglecting its relational, contextual, and collective dimensions (Leodoro et al., 2018; Morse et al., 2021). This narrow framing risks obscuring the strategies global majority women develop to sustain careers and well-being in inequitable environments.
This study addresses these gaps by examining the intersectional challenges and resilience strategies of global majority women healthcare professionals in the United Kingdom. It contributes to feminist organisational scholarship in three ways. First, it adopts the term global majority women rather than deficit-based categories such as ‘Black and Asian minority ethnic’ (BAME) or ‘migrant women’. This terminology acknowledges global demographic realities while avoiding minority-centric frames. Second, it demonstrates how intersecting identities produce distinctive configurations of marginalisation within healthcare workplaces. Third, it positions resilience not merely as personal endurance but as situated, agentic, and often collective practices of adaptation and survival. From a practical perspective, this research provides insights for evidence-based interventions that support healthcare workforce diversity. As health systems face staff shortages and an urgent need for cultural competence, understanding how to build inclusive environments where all professionals can thrive is critical. By centring the lived experiences and resilience of global majority women healthcare professionals, this study not only challenges deficit narratives but also highlights critical gaps in understanding that must be addressed to enable transformative change in healthcare organisations.
The article proceeds as follows. The next section critically reviews literature on gender, race, migration, and religion in healthcare, situating these within an intersectional framework. The methodology outlines the qualitative design. The findings are presented in two parts: the intersecting challenges participants reported and the resilience strategies they employed. The discussion considers theoretical and practical implications for feminist scholarship and healthcare workforce policy.
Global majority women in healthcare
Persistent gendered inequalities
Global majority women form the backbone of healthcare systems worldwide, constituting a substantial proportion of frontline workers across nursing, midwifery, care work, and increasingly medicine (Boniol et al., 2019; NHS England, 2023). Despite their centrality, global majority women are disproportionately clustered in lower-status, lower-paid, and often more precarious positions compared to their white and male counterparts (Kingma, 2008; NIHR Leicester Biomedical Research Centre, 2025). Leadership and senior medical roles remain dominated by men and white professionals, revealing enduring patterns of vertical segregation (Carnes et al., 2015).
Beyond pay and career stratification, global majority women are systematically burdened with inflexible work structures and disproportionate domestic labour responsibilities, intensifying work–family conflict (Shanafelt et al., 2019). Institutional cultures often privilege the ‘ideal worker’ norm aligned with male, uninterrupted career trajectories, making it difficult for women especially those with caregiving responsibilities to progress (Kline, 2014). Moreover, gendered assumptions about women as ‘natural carers’ contribute to the undervaluation of their labour and the persistence of occupational stereotyping (Braithwaite et al., 2016).
Racialised, migrant, and religious precarity
The experiences of global majority women cannot be understood through gender alone; race, migration status, and religion profoundly shape their positions in healthcare. Comparative studies across North America, Europe, and Australasia show that racialised women encounter compounded discrimination, including routine questioning of competence, exclusion from professional networks, and slower progression into senior roles (Alexis et al., 2007; Pogrebna et al., 2024; Wingfield, 2019). These barriers are further exacerbated for migrant women, whose qualifications are often devalued and whose career trajectories are constrained by structural inflexibilities such as visa dependency and credential recognition barriers (Humphries et al., 2019).
Migration processes themselves are gendered. Women’s migration is frequently tied to family obligations, resulting in constrained career choices and transnational care responsibilities (Kofman and Raghuram, 2022; Parreñas, 2016). Research highlights that global majority women healthcare professionals often shoulder ‘dual care’ burdens, maintaining caregiving ties across borders while sustaining families in their host country (Baldassar and Wilding, 2020). These intersecting obligations intensify that stress and work–life conflict yet remain largely invisible in healthcare policies and workforce planning.
Religion introduces another critical dimension. Muslim women healthcare professionals, for example, often navigate institutional insensitivity to prayer breaks, fasting, or modest dress, with visible markers such as the hijab amplifying experiences of scrutiny and Islamophobia (Ghumman and Ryan, 2013; Linando, 2022). In practice, religion intersects with race and gender, creating layers of disadvantage that compound the barriers faced by global majority women within UK healthcare.
Intersectionality as a framework for healthcare workforce research
Intersectionality theory, originating from Crenshaw’s (1989, 1991) critique of legal and feminist frameworks, provides a lens for analysing how multiple social identities and structural forces interact to shape unique experiences of privilege and oppression (Weber, 2015). Collins and Bilge (2016) extend this by emphasising the role of power and institutional practices in producing compounding disadvantage. Within organisational research, intersectionality exposes how seemingly neutral practices such as mentoring, networking, or performance evaluation can reinforce structural inequities (Rodriguez et al., 2016).
In healthcare contexts, intersectionality has gained traction but remains underutilised. Akanji et al. (2020) and Adisa et al. (2019) argue that failing to account for intersecting disadvantages obscures the distinctive challenges of global majority women. For example, Bradley et al. (2023) show that global majority women healthcare workers report disproportionately higher rates of work-related mental health diagnoses and substantially lower satisfaction with organisational support compared to peers. Similarly, Reid et al. (2025) demonstrate that global majority women experience significantly higher levels of work–family conflict than white women, even when controlling for hours and family structure. Policy analyses also highlight structural dimensions of intersectional disadvantage. Warren (2022) found that migrant women professionals have 23% lower job satisfaction than UK-born colleagues, largely due to visa-linked inflexibility. Chung (2020) documents flexibility stigma, whereby Black and Asian women requesting flexible work are more likely to be penalised through racialised stereotypes of low commitment. These examples show how institutional and socio-cultural factors converge to shape inequities. Thus, this study builds on such insights by foregrounding the intersectional experiences of global majority women healthcare professionals navigating multiple margins simultaneously.
Resilience strategies
Resilience is as a central theme in healthcare professional well-being discourse, broadly defined as the capacity to adapt positively in the face of adversity (Shanafelt et al., 2019; Southwick et al., 2014). Within the NHS, resilience-building programmes have been promoted as part of well-being strategies, particularly following the COVID-19 pandemic (Warren, 2022). However, traditional approaches emphasising individual psychological traits and universal strategies have been critiqued for their limited attention to diversity and structural inequities. Feminist scholars argue that individualised resilience frameworks risk shifting responsibility onto women and minoritised professionals while leaving systemic inequalities unchallenged (Gill and Orgad, 2018; Joseph, 2013). This critique is particularly relevant for healthcare, where resilience training may help individuals manage stress but fails to address chronic understaffing, racialised hierarchies, or inflexible organisational structures that generate stress initially (Warren, 2022).
Alternative approaches emphasise resilience as relational and context-specific, shaped by collective practices and cultural resources. For global majority women in healthcare, resilience strategies extend beyond individual psychology to encompass identity affirmation, community building, and structural resistance. Extant studies show distinctive coping mechanisms including spiritual and cultural resources, with faith practices and religious community support helping buffer stress (Koenig, 2012; Padela and Curlin, 2013). Transnational family networks provide both burden and support, while ‘shifting’ strategies enable navigation of racialised and gendered expectations while maintaining authentic identities in safe spaces (Morse et al., 2021).
Global majority women also employ strategic boundary management and proactive career reconfiguration, such as work schedule negotiations or psychological detachment strategies (Adisa et al., 2021; Akanji et al., 2020). However, these adaptive strategies often reflect systemic exclusion rather than genuine empowerment, illustrating the paradox, whereby creative coping mechanisms simultaneously enable survival and normalise structural inequities (Bradley et al., 2023; Owolewa et al., 2026; Reid et al., 2025).
Research design and philosophical approach
This study employed a qualitative research design underpinned by interpretivist epistemology and intersectionality theory. An interpretivist approach recognises that social realities are produced through meaning-making and lived experience (Creswell and Poth, 2018). We used intersectionality as a theoretical lens and a methodological tool to examine how overlapping identities such as gender, race, migration status, and religion shape global majority women’s experiences in UK healthcare (Collins and Bilge, 2016; Crenshaw, 1989). The study was informed by feminist principles that prioritise participant voice, challenge hierarchical researcher–participant relations, and avoid deficit framings of minoritised groups (Hesse-Biber, 2012).
Participant recruitment and selection
We used purposive and snowball sampling to recruit participants who met the following criteria: self-identifying as women; belonging to an ethnic, religious, or cultural minority group; working in healthcare in the United Kingdom; and having at least 1 year of professional experience. For recruiting the participants, we leveraged professional networks, community organisations, and social media platforms. Snowballing was particularly useful in reaching individuals who might otherwise hesitate to participate due to professional vulnerability or precarious immigration status.
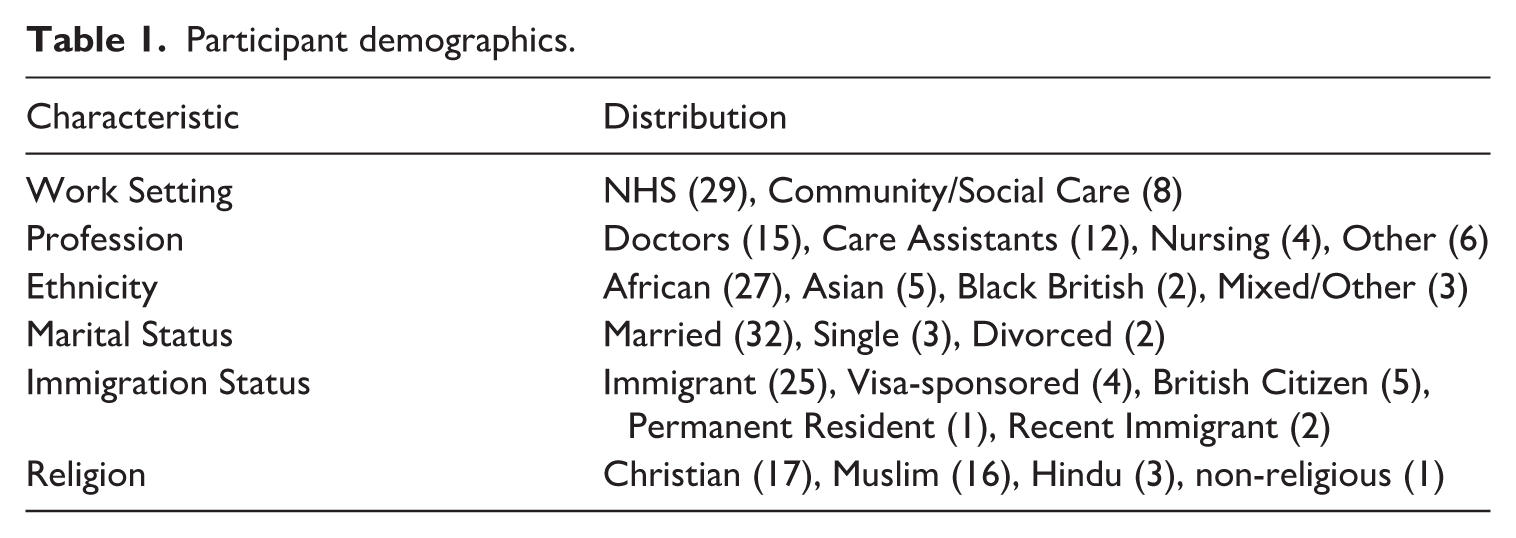
The final sample comprised 37 (n = 37) participants (see Table 1) aged between 24 and 52 years, across a range of roles (including general practitioners, medical specialists, nurses, midwives, physiotherapists, healthcare assistants, and administrators). Participants represented diverse ethnic backgrounds (African, South Asian, Middle Eastern, and mixed heritage), religious affiliations (Muslim, Christian, Hindu, Buddhist), and migration statuses (recent migrants, visa-sponsored, British citizens, permanent residents). This diversity enabled comparative insights into how multiple identity markers intersected to shape challenges and resilience strategies.
Participant demographics.
Data collection
Data were generated through semi-structured interviews conducted between October 2024 and February 2025 lasting between 60 and 90 minutes each. The interview schedule was informed by a review of relevant literature and refined through consultation with community representatives to ensure cultural sensitivity. Questions explored professional trajectories, workplace experiences, identity negotiation, work–family balance, encounters with discrimination, and coping mechanisms. Most of the interviews were conducted via secure video conferencing platforms to accommodate geographical spread, convenience, and preference of the participants. However, six interviews were conducted in person at participants’ chosen locations. All interviews were conducted in English, though participants were encouraged to draw on heritage languages where appropriate. Interviews were audio-recorded with consent and professionally transcribed.
Data analysis
Thematic analysis was employed, guided by Braun and Clarke’s (2012) six-phase approach and adapted to reflect intersectional principles. Coding combined inductive and deductive strategies: data-driven codes captured emergent meanings, while theoretical sensitivity to intersectionality informed the identification of cross-cutting dynamics. During the thematic construction, we paid particular attention to how experiences varied across intersecting identities. For example, discrimination was not treated as a single category but examined in relation to combinations of race, gender, religion, and professional role. We held regular analysis meetings with the research team, which enhanced reflexivity and rigour. In addition, we carried out member checking with selected participants to ensure cultural resonance and credibility. The lead researchers’ own identity as a global majority woman with healthcare experience shaped both access and interpretation. Shared identity markers fostered rapport and trust yet also risked assumptions of commonality. Reflexive practices, including research journaling, supervision discussions, and peer debriefing, were integral to managing positionality and minimising bias. These practices enhanced transparency and supported the production of credible, contextually grounded findings.
Ethics
Ethical approval was obtained from the University Research Ethics Committee. Informed consent emphasised voluntary participation and the right to withdraw. Given participants’ concerns about job security and immigration status, confidentiality was prioritised: pseudonyms were assigned, identifying information removed, and all data stored securely. In addition, the study followed principles of reciprocity. Findings were shared back with participants through community presentations and policy briefings, aiming to contribute knowledge of practical benefit to the wider communities represented.
Global majority women’s experiences in UK healthcare
The analysis revealed that participants’ experiences in healthcare workplaces were profoundly shaped by intersectional dynamics, producing both significant challenges and resourceful coping strategies. These experiences were not reducible to single identity categories but instead reflected the complex interplay of race, gender, religion, and migration status. Two overarching categories emerged: (1) intersectional challenges that intensified workplace marginalisation and (2) resilience strategies that enabled participants to sustain professional effectiveness and personal well-being.
Compounded professional marginalisation through multiple identity intersections
Participants described a distinct form of marginalisation that stemmed from the convergence of multiple identity positions. The intersection of race, gender, religion, and migration status generated a form of hypervisibility, subjecting individuals to heightened surveillance, diminished credibility, and disproportionate consequences for errors.
Generally, I think and that’s all over the world not only in the UK . . . as women you are at a disadvantaged position . . . as Muslims, you are also at a disadvantaged position in the UK . . . And as a Black person, you are also in the minority position. So now imagine being a Black African Muslim woman. So that puts you in . . . exactly. (P16, African Muslim General Practitioner)
Professional knowledge was frequently discredited, with Black participants reporting systematic dismissal of their contributions.
So, when you give . . . we can do this thing this way . . . but because the idea came from we Blacks, they don’t want to accept it. (P1, Healthcare Assistant)
For those on work visas, sponsorship arrangements deepened this vulnerability, making it difficult to challenge discriminatory practices without risking job and residency security.
I’m on sponsorship. I can’t say I want to stop coming to work because of that. (P1, Healthcare Assistant)
These narratives suggest that intersectionality within healthcare professions is not additive but compounding. Overlapping identities created qualitatively new forms of disadvantage that systematically eroded professional credibility and curtailed agency. Marginalisation was amplified through institutional surveillance, revealing how organisational structures position intersectional professionals as perpetually precarious.
Religious–cultural–gender nexus in professional integration
Religious identity, cultural norms, and gender roles intersected in ways that shaped participants’ capacity to integrate into professional spaces. Muslim participants, in particular, described the guilt associated with missing prayers due to inflexible schedules and the suspicion that prayer practices could arouse among colleagues.
When I work . . . I miss my prayer times because our prayers have to be in a certain time frame . . . When I can’t get a break during that time, I feel very guilty. (P17, Turkish Muslim GP Trainee) As a Muslim and a Black person . . . I am seen as like a threat . . . I was questioned about my going to pray. Why should I have to go and pray always? (P31, African/British Muslim Nursing Assistant)
Beyond religion, cultural expectations of women as caregivers clashed with career ambitions, creating further friction.
They expect that women should be stay-at-home moms . . . particularly in the Asian community, that is something from the old generation that is quite difficult. (P2, Hindu Midwife)
Visible markers of faith, such as the hijab, created barriers to social belonging, signalling difference in ways that prompted distancing from colleagues.
There’s people just by me wearing head scarf . . . they will feel the need to keep a distance. (P21, African Muslim Physiotherapist)
These accounts highlight how professional integration is mediated by wider religious and cultural discourses. Healthcare institutions, by enforcing rigid norms of practice and neglecting to accommodate cultural difference, reproduce exclusionary environments where identity and belonging must be constantly negotiated.
Motherhood penalties and gendered migration burdens
Motherhood introduced career penalties that were intensified by race, religion, and migration status. Pregnancy and maternity leave were often interpreted as incompetence or lack of commitment, rather than temporary absence.
So, because I have to be the one to carry pregnancy, I have to be on my leave . . . That has slowed me down . . . currently in GP training. (P15, African Christian Medical Doctor) I was asking for flexibility, especially when I was pregnant . . . It felt like I was being unreasonable towards my team. (P28, African Christian GP)
Cultural norms reinforced this strain, with Black African women describing expectations to manage both full domestic and professional workloads.
As a Black African woman . . . you’re meant to run the house, after the children, still do your work, go to work and look after the whole family. (P28, African Christian GP)
Migration further exacerbated these burdens, as distance from extended families deprived participants of support networks.
Culturally, we look after our families . . . but I live far away from home. I cannot even see them in a year sometimes. (P33, African Muslim Nurse)
These findings reveal that motherhood penalties in healthcare are not uniform but intersectional. They are compounded by racialised stereotypes, cultural obligations, and transnational responsibilities, creating unique career progression barriers and intensifying the double shift of domestic and professional labour.
Psychological and emotional burdens
The cumulative strain of managing multiple marginalised identities manifested in psychological challenges, including identity concealment, guilt, and mental health strain. Some participants described suppressing parts of their identity to fit professional norms, resulting in feelings of inauthenticity.
You can be intimidated . . . having like inferiority complex because you’re coming from a particular background. (P8, African Muslim Medical Practitioner)
Others spoke of maternal guilt, where professional obligations were experienced as betrayal of cultural expectations of motherhood.
The more you are away from the child, you feel that . . . like you’re cheating on the child. (P9, African/British Christian Medical Doctor)
In some cases, these pressures escalated into acute mental health struggles.
I actually had to go . . . to see my GP. ’Cause it was stressful . . . I was even thinking of leaving my training at that point. (P10, African Christian Medical Doctor)
This theme underscores that intersectionality operates not only structurally but also emotionally. The intersection of cultural, professional, and domestic expectations produced identity fragmentation and chronic psychological strain, demonstrating how organisational contexts can exacerbate mental health vulnerabilities.
Systemic and structural intersectional barriers
Institutional arrangements within healthcare frequently failed to accommodate intersectional realities. Policies around religious observance, flexible work, and training progression were applied inconsistently, often disadvantaging global majority women.
In Ramadan . . . it can be a little bit hard to cope with . . . I believe they weren’t very aware of it. (P14, African Christian GP Trainee) After I had my daughter and requested flexible working, the management declined . . . It wasn’t fair because other midwives with children had flexible contracts. (P2, African Hindu Midwife)
Rigid training requirements further compounded exclusion.
My colleagues who I started with finished their training, became consultants, and I’m still training. (P13, Turkish Muslim Doctor)
These accounts point to systemic exclusion not as deliberate hostility but as institutional neglect. Structures that assume an ‘unencumbered worker’ norm reproduce inequality by overlooking the intersectional realities of global majority women.
Resilience strategies and coping mechanisms
Despite facing significant and sustained challenges, participants demonstrated remarkable resilience. This resilience was not merely about ‘getting through’ adversity but reflected strategic, resourceful, and culturally embedded practices that enabled professional survival and, at times, personal well-being. Five interconnected strategies emerged, revealing resilience as both an act of agency and a practice constrained by organisational structures.
Internal psychological adaptation
Participants reshaped their inner experiences through spiritual anchoring, cognitive protection, and expectation recalibration. Religious practices were a recurring source of stability, grounding participants during periods of professional and personal strain.
Religion has been really good. Because obviously you have like good times and bad times, even at work . . . when you come back to the basics of your religion, trying to like reconnect with your Lord, trying to listen to some sermons on words of comforting words. They kind of also just help with your well-being in general. (P12, Medical Doctor)
Alongside spirituality, others described deliberate efforts to limit overthinking and avoid dwelling on unfair treatment, framing this as a way of protecting their mental health.
So, what I do as much as possible is not to overthink it . . . I try to enjoy every moment of my life rather than complaining . . . even though I feel it’s tiring and stressful. (P11, Healthcare Assistant)
Some participants recalibrated expectations altogether, adapting routines to avoid burnout and maintaining a sense of calm acceptance in the face of competing pressures.
If I get home and I can cook, I cook. If we can’t cook, we eat out . . . I take things really calm and whatever I can do, I do it. If I’m not capable, I leave it. (P9, Healthcare Worker)
These strategies highlight resilience as a form of cognitive and existential labour. Participants not only found ways to cope but also actively crafted internal narratives that reframed adversity, often through religious or cultural repertoires. This psychological adaptation was crucial for survival, but it also reveals how the burden of resilience was displaced onto individuals rather than addressed through systemic change.
External resource mobilisation
Resilience was also sustained through relational infrastructures. Participants highlighted spousal encouragement, extended family contributions, and collaborative arrangements with colleagues as essential supports.
My husband encourages me a lot when I’m down . . . to push me up. Yeah, it works like a protective factor for me. (P4, Medical Doctor)
For migrant professionals, extended networks were often reconstructed across borders, involving significant investments of time and money.
We invested in bringing our moms to help . . . that was very helpful. (P8, Medical Practitioner)
These interpersonal resources were not limited to the family; colleagues also provided a buffer through mutual arrangements and solidarity.
Luckily, I had a partner there who I was working closely with, so she was also in the same field like me. So, we kind of make an arrangement or so. (P9, Medical Worker)
These accounts challenge individualised notions of resilience. Instead, resilience was enacted collectively, relying on webs of relational care that extended across households and, in some cases, continents. Yet, this also underscores a paradox: while these networks sustained women, they simultaneously allowed organisations to abdicate responsibility, depending on family systems to absorb the costs of structural inflexibility.
Strategic life course reconstruction
Many participants described reshaping career trajectories and temporal arrangements to balance professional aspirations with caregiving responsibilities. This often meant slowing progression, restructuring work schedules, or creating alternative income streams.
Because I have to be the one to carry pregnancy . . . that has slowed me down . . . I’m going to reduce my hours . . . if I was a man, I would just continue. (P14, Medical Trainee)
For others, reconstructing careers involved finding creative ways to sustain income while maintaining family roles.
I decided I was going to work two days in my normal practice and then I worked out of hours for another organisation . . . I work weekends and evenings when my husband is at home with the kids. (P28, Medical Doctor)
Even interactions with extended family overseas were carefully timed and restructured to fit within professional constraints.
Sometimes I used to speak with her while on the bus going home . . . sometimes I walk so early before my work time, because back home this would be the time she would be going to school. (P34, Medical Doctor)
These narratives reveal resilience as a form of temporal and structural engineering. Women altered the rhythm of their lives to preserve both career and caregiving, often at personal cost. Such adaptations demonstrate extraordinary ingenuity, but they also highlight how organisations place the onus of adjustment on global majority women rather than addressing structural rigidity.
Strategic time management and boundary creation
Time management and firm boundaries were vital for protecting mental health and preserving family relationships. Participants described strategies ranging from daily planning to disciplined compartmentalisation.
Without cooking in the morning, I do cooking at night for the next day. (P11, Healthcare Assistant)
This kind of preparation was echoed by others who treated days off as opportunities to stay ahead.
Any day I’m off work . . . I have to have a good preparation for those days. (P22, Healthcare Worker)
Boundary creation was also enacted psychologically, with some participants training themselves to leave work behind once their shifts ended.
Once I get out of work, I don’t think about work anymore . . . I’ve trained my brain, once I step out, that’s it. (P4, Medical Doctor)
For others, refusing work technologies was a way of enforcing physical boundaries.
I refused a work laptop because I don’t want to bring work home. Anything that happens at work stays at work. (P16, GP)
These accounts demonstrate resilience as a form of boundary work. By setting limits, participants carved out protected spaces for rest, recovery, and family. In doing so, they resisted professional cultures that valorise overwork, subtly pushing back against the expectation of constant availability.
Flexibility and structural accommodation
Where organisational flexibility was available, participants reported dramatic improvements in well-being and work–life integration.
The fact that I was able to choose the number of hours I want and the days that I want has enabled me to achieve a work-family balance. (P25, Healthcare Professional)
Others emphasised how remote work provided greater autonomy over their environment.
Being able to work at home some days . . . gives me the opportunity to plan. I feel very relaxed. (P27, Medical Doctor)
Some also used shift selection to align work with childcare demands.
I try to do night shifts. I can have time for them during the day. (P31, Nursing Assistant)
However, these opportunities were not evenly distributed, and many participants described exhaustion when such flexibility was denied.
When you work close to 50 hours per week, all you can do is sleep and eat right. (P17, GP Trainee) Every time my husband is home, I’m at work . . . it’s very difficult for us to have personal time or family time. (P19, Healthcare Worker)
These accounts reveal that resilience is not purely an individual achievement, but a relational outcome shaped by organisational design. Where flexibility existed, women could exercise agency more fully; where it did not, they were left depleted. This unevenness demonstrates how organisational structures actively shape the capacity for resilience, even as resilience is discursively positioned as a personal responsibility.
These strategies reveal resilience as multi-layered, relational, and paradoxical. On the one hand, participants demonstrated adaptability, mobilising cultural, religious, relational, and temporal resources to sustain careers in the face of systemic inequities. On the other, their accounts expose how resilience is organisationally appropriated. Notably, healthcare institutions depend on global majority women’s ingenuity and sacrifice, while failing to dismantle the inequities that necessitate such adaptation. The findings here position resilience as an intersectional practice, produced at the nexus of identity, culture, and institutional constraint, simultaneously empowering and constraining.
Intersectionality as lived organisational reality within UK healthcare
This study demonstrates that intersectionality is a lived organisational reality within UK healthcare, challenging single-axis analyses of workplace inequality. Participants’ accounts highlight compounded professional marginalisation, whereby race, gender, religion, and migration status interact to create disadvantages qualitatively different from their sum. These findings affirm Crenshaw’s (1989, 1991) articulation of intersectionality while extending it to professional contexts where legitimacy, belonging, and authority are continually negotiated. A key mechanism identified was hypervisibility. Global majority women healthcare professionals described heightened scrutiny that cast them as provisional members of their professions. This echoes Collins and Bilge’s (2016) discussion of simultaneous visibility and invisibility and illustrates how intersectional positioning undermines epistemic authority (Dotson, 2012; Puwar, 2004). Here, inequality operates not only through blocked career progression but also through the dismissal of knowledge and expertise.
Visa dependency further exposed how immigration regimes interact with organisational dynamics to enforce structural silencing. Precarious legal status intensified racialised and gendered vulnerability, making resistance to discrimination professionally and personally hazardous. This extends scholarship on migrant healthcare workers (Beech et al., 2018; Humphries et al., 2019; Owolewa et al., 2026; Warren, 2022) by showing how immigration policies compound organisational marginalisation and constrain agency.
Religion emerged as a critical yet under-examined axis of inequality. While often collapsed into ethnicity or treated peripherally (Ghumman and Ryan, 2013; Modood, 2020), participants’ accounts revealed how Muslim women faced distinctive challenges: constraints on prayer time, hijab-related discrimination, and Ramadan insensitivity. These ostensibly neutral policies reproduced exclusion (Linando, 2022), resonating with debates on multicultural accommodation (Joppke, 2017; Meer and Modood, 2011). Religious visibility, when combined with gender and race, intensified scrutiny and marginalisation. Work–life integration was also shaped by intersectionality. Participants navigated professional demands alongside cultural–religious expectations of intensive mothering, illustrating how inequality extends across organisational and domestic spheres. This develops feminist work–life scholarship (Gatrell, 2013; Mordi et al., 2023) by showing how caregiving is mediated through cultural and religious frameworks rather than universal norms.
In response, women developed resilience strategies embedded in cultural, spiritual, and relational resources. Spiritual anchoring was central, demonstrating how faith practices provide support overlooked by well-being programmes. These findings align with critiques of resilience as a neoliberal discourse that masks structural inequities (Gill and Orgad, 2018; Joseph, 2013). What emerges is a resilience paradox: women’s adaptability ensures survival yet legitimises organisational inflexibility. Resilience also operated transnationally, as participants mobilised extended kin networks and spousal support across borders. This challenges individualistic and nationally bounded frameworks of resilience, situating global majority women’s professional participation within global care chains (Hochschild, 2014; Yeates, 2012). Recognition of these transnational dynamics is essential to supporting diverse healthcare workforces. The findings further reveal organisational complicity: while espousing diversity, institutions benefitted from inequities through exclusion from informal networks, inconsistent policy implementation, and tolerance of discriminatory patient behaviour. This supports critiques of diversity work as symbolic compliance (Ahmed, 2012; Zanoni et al., 2010). Policies such as flexible working arrangements often reproduced rather than disrupted inequality, particularly for global majority women.
Finally, systemic barriers to progression, limited access to training, exclusion from mentorship, and disproportionate workloads underscored how professional hierarchies intersect with wider social inequalities. These findings resonate with critical race and feminist analyses of organisations (Rodriguez et al., 2016; Wingfield, 2019)
Conclusion
This study has examined the intersectional challenges and resilience strategies of global majority women healthcare professionals in the United Kingdom, drawing on qualitative insights from 37 participants (n = 37) across diverse roles, ethnicities, religions, and migration statuses. The findings demonstrate that the experiences of global majority women are shaped by compounded inequalities at the intersections of race, gender, religion, and migration status, producing unique forms of marginalisation that extend beyond single-axis analyses. Challenges such as hypervisibility, dismissal of expertise, motherhood penalties, and institutional inflexibility were accompanied by profound psychological and emotional costs. Yet, participants also demonstrated agency through multi-layered resilience strategies, including spiritual anchoring, relational support, strategic career restructuring, boundary creation, and utilisation of organisational flexibility. These strategies highlight resilience not as an innate trait but as relational, contextual, and paradoxical—sustaining survival while simultaneously masking structural inequities.
Theoretically, the study contributes by (1) foregrounding global majority women as central to healthcare systems, (2) extending intersectionality to include emotional and psychological dimensions, and (3) conceptualising resilience as relational and politically charged. Practically, the findings call for systemic reforms, including inclusive organisational design, immigration policy changes, intersectional mental health support, and greater leadership opportunities for global majority women within UK healthcare.
As healthcare systems globally face workforce shortages and increasing diversity, addressing these challenges is both an ethical imperative and a practical necessity. Creating inclusive environments that recognise and value the intersectional realities of global majority women is essential for workforce sustainability, professional equity, and patient care quality. By centring the lived experiences and resilience of global majority women healthcare professionals, this study not only challenges deficit narratives but also provides a roadmap for transformative change in healthcare organisations.
Footnotes
Acknowledgements
The authors would like to thank all participants who generously shared their experiences and insights.
Ethical Considerations
The BLSS Ethics Review Committee at Birmingham City University approved our interviews (approval: Owolewa /#12812 /sub5 /R(A) /2024 /Oct /BLSS FAEC) in October 2024. Respondents gave written consent for review and signature before starting interviews.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive and potentially identifying nature of qualitative interview data, the full transcripts are not publicly available. De-identified excerpts supporting the findings of this study are available from the corresponding author upon reasonable request.