
Abstract

The prevalence of multiple sclerosis (MS) has increased in all regions of the world 1 (Figure 1). Earlier diagnosis and treatment with appropriate disease-modifying therapies (DMTs) equate to better outcomes and less disability, yet most countries report significant barriers to accessing DMTs2–4 This is especially so in low/lower-middle income countries (LLMICs); for instance, in some regions, almost all LLMICs reported not having access to a single high-efficacy DMT.1–4
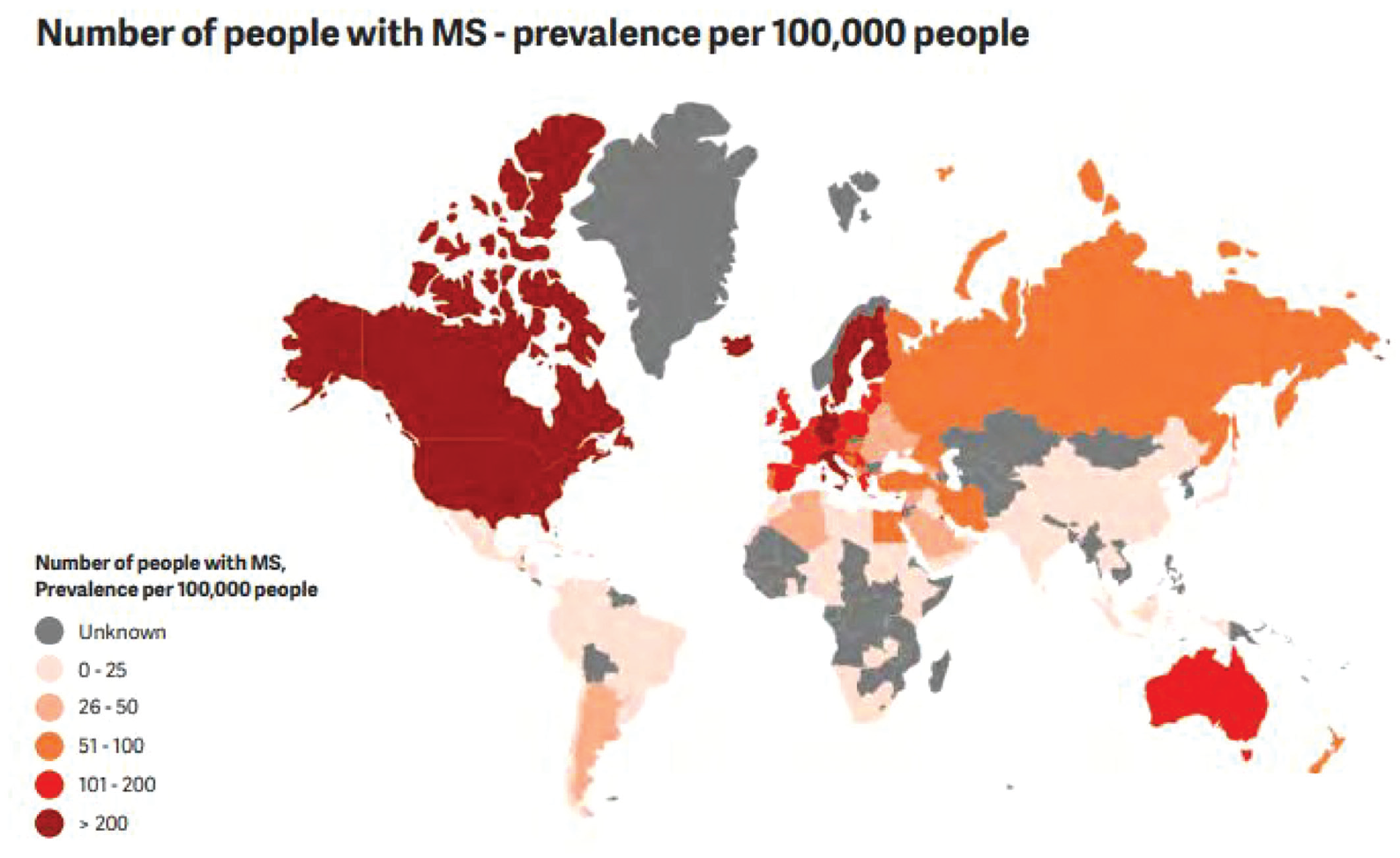
Reproduced with permission from the Multiple Sclerosis International Federation, Atlas of MS, 3rd Edition (September 2020).
The World Health Organization (WHO) Essential Medicines List (EML) comprises evidence-based, high-priority, cost-effective treatments applicable to any healthcare system with the premise that the drugs are made available by local governments by endorsing them in their respective national formularies. 5 The recent endorsement by the WHO of including three MS DMTs – glatiramer acetate, oral cladribine and intravenous rituximab – on the EML is therefore a significant milestone for people with MS (pwMS) across the world, and addresses the urgent need to improve disease control and quality of life for pwMS globally. 6 Rituximab has been extensively used for treating MS patients especially in LLMIC due to its cost-effectiveness, 7 but its off-label status has curtailed reimbursement by governmental and private insurance systems. 7 Its inclusion on the WHO EML should help circumvent this problem.
However, despite countries endorsing the concept of the EML over the years, implementing the list into local practice is variable and fraught with challenges especially in LLMICs.8,9 Taking epilepsy as an illustrative example: the Intersectoral Global Action Plan (IGAP) report from 2022 describes how the epilepsy treatment gap had not narrowed significantly in the preceding decade despite concerted efforts by members states, the WHO secretariat, international and national organisations.9,10
Anti-epileptic drug (AED) availability continues to be challenging particularly in developing countries, which have the highest burden of epilepsy, even in the face of simplified formularies, standardised treatment guidelines and mechanisms to reduce cost. 9 In some cases, inclusion of a third-generation AED from the 1990s took as long as a decade to appear on a certain national medicine list for 2022. 10
The IGAP attends to the above challenges in epilepsy by providing a robust roadmap enshrined in five main pillars: relation with policy makers, therapy, prophylaxis, research and public health. This roadmap is applicable to other neurological disorders including MS and is an ideal structure to effect the new EML iteration. 10
There are already some real-world examples of such work occurring globally:
Certain world regions have developed standardised MS-specific guidelines with local policy makers. 11
Lobbying from patient advocacy groups to have rituximab covered by their national health budgets. 12 Indeed, success stories such as the provision of AEDs and drugs for hepatitis C through global collaborations 13 provide a template on how to improve the sustainable availability and accessibility of DMTs on the EML. 14
Launching of more region-specific TRIMS committees, for example, Pakistan CTRIMS (PAKTRIMS) and African CTRIM (AFRICTRIMS).15,16
Therefore, in the current situation with this momentous result, implementation of the WHO EML through the IGAP, or similar, frameworks will require coordinated leadership at national levels, changes in clinical governance and more cross-pollination between frontline clinicians, researchers, policy makers and patient groups.
All of this may come with their own challenges particularly in LLMICs, 17 but thankfully there are opportunities to leverage from cross-cutting non-governmental organisations, for example, the MS International Federations toolkit on engaging efficiently with national health. 18
Conclusion
The successful WHO EML result came about through rigorous collaborative efforts coordinated by Multiple Sclerosis International Federation (MSIF) over many years between key stakeholders and was a process that embraced diversity and inclusivity so as to be representative of all the regions of the world. Endorsement of the three DMTs by the WHO is testament to its acknowledgement on the urgent action needed to tackle the global burden of MS, given it is the most common disabling neurological condition of young adults, and its impact ripples into families, societies, communities and economies.
We recommend the following actions:
Prioritisation: Advocate for policy changes in the national health systems to recognise and prioritise MS by mobilising attention and resources. This effort needs to be co-led by key opinion leaders from regional and national TRIMS or neurological associations, together with patient organisations, to create direct dialogue with decision-makers. 19
Standard of MS care: Ensure current and appropriate national consensus statements, treatment guidelines/algorithms and formularies are in place, and where possible, officially recognised. Adopting and adapting regional guidelines or those from a similar health setting to the local setting improves utility and efficiency. This activity should be led by national MS experts in collaboration with patients, their representatives and officials in the health system for smoother implementation. 19
Access, funding and reimbursement: Medicines will not be accessible to pwMS unless they are registered, quality-assured, procured, made available and are affordable at the point of care. Health systems need to align prioritisation with resource allocation and procurement decisions. Round-table discussions between industry, health system representatives and payers, supported by healthcare professionals and patient groups, allow for practical steps to improve access and affordability. International and regional organisations can play a critical role by engaging and supporting a systematic approach across countries improving efficiency. The strategies may include negotiating fair prices, organising markets through larger orders and more reliable forecasting, pooled procurement, local repacking or manufacturing of medicines.14,19
All of these actions require collaborative advocacy between clinicians, patient groups and others, such as government and health systems officials, and industry. There needs to be agreement on what the priority needs are and how to tackle them. 19
International and regional organisations such as MSIF, World Federation of Neurology (WFN) and the TRIMS networks can enable convening and learning between countries, and catalyse practical steps empowering global advocacy efforts and regional/national EML effectuation.
Patients with MS cannot wait for decades to have this EML implemented: the time for action is now, through the growing international momentum to improve care and access to treatment for neurological diseases.
Footnotes
Acknowledgements
Multiple Sclerosis International Federation (MSIF), MSIF Essential Medicines Panel (MEMP), MSIF Off-Label Treatments (MOLT) Panel, WHO Collaborating Centre in Evidence-Based Research Synthesis and Guideline Development Bologna, Cochrane Multiple Sclerosis and Rare Diseases of the Central Nervous System (CNS), McMaster University’s MacGRADE Centre.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: B.Y. and S.V. were Co-Chairs of the MSIF Off-Label Treatments (MOLT) panel. S.V. and D.S. were panel members on MSIF Essential Medicines Panel (MEMP). J.L.D. works as a consultant for Multiple Sclerosis International Federation (MSIF) and has coordinated both MOLT and MEMP panels. MEMP members used recommendations from both MOLT and MEMP guidelines to develop the WHO EML application.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
This is a non-interventional editorial piece. Institutional approval was obtained for permission to publish.