
Abstract
Background:
Advanced magnetic resonance imaging (MRI) of the cerebellum remains underutilized to detect early microstructural abnormalities associated with multiple sclerosis (MS) clinical disability.
Objectives:
To examine associations between cerebellar magnetization transfer ratio (MTR) and clinical measures in people with radiologically isolated syndrome (RIS), early relapsing–remitting MS (RRMS), and primary progressive MS (PPMS).
Methods:
MTR data were acquired at 3.0 T across four sites in 53 RIS, 202 RRMS, 46 PPMS, and 42 control participants, as part of the Canadian Prospective Cohort Study to Understand Progression in MS (CanProCo). Multiple linear regression analyses evaluated associations between cerebellar MTR and clinical measures.
Results:
Across MS subtypes, lower cerebellar MTR was associated with greater motor disability, most notably with impaired manual dexterity (β = −1.04 to −0.67). After the false discovery rate correction, two associations remained statistically significant (p < 0.01): lower MTR in the inferior cerebellar peduncles was associated with worse cerebellar function in RRMS, and lower MTR in the anterior lobe was associated with worse manual dexterity in PPMS.
Conclusion:
This large, multi-center, hypothesis-generating study identified two statistically significant associations between cerebellar MTR and clinical disability, alongside several exploratory findings. These results suggest that cerebellar MTR may capture clinically relevant microstructural abnormalities in early MS.
Introduction
Cerebellar damage in multiple sclerosis (MS) can cause substantial deficits in coordination, gait, cognition, and mood.1,2 Despite its clinical relevance, the cerebellum has rarely been evaluated using advanced magnetic resonance imaging (MRI) techniques, particularly in people with early MS.
Cerebellar atrophy, a conventional MRI measure capturing irreversible tissue loss, has shown inconsistent relationships with clinical measures in people with MS (pwMS).3,4 Conversely, the presence of T2 hyperintense cerebellar lesions early in the disease course portends a worse prognosis, but T2 hyperintense lesion burden has shown inconsistent relationships with clinical disability.3,4 These observations motivate evaluating the cerebellum using promising quantitative MRI measures to better understand the microstructural substrates of disability in pwMS.
Magnetization transfer imaging (MTI) is an advanced MRI technique, from which the magnetization transfer ratio (MTR) can be derived. 5 MTR reflects the magnetization exchange between freely mobile protons and restricted protons bound to macromolecules, making it sensitive to changes in tissue microstructure, particularly myelin, which cannot typically be evaluated using conventional MRI alone. 5
In this study, microstructural abnormalities were assessed in the cerebellum and cerebellar peduncles using MTR and examined in relation to a range of clinical measures across MS subtypes. It was hypothesized that (a) people with primary progressive MS (PPMS), typically characterized by more established disability, demonstrate greater microstructural abnormalities, reflected by lower cerebellar MTR, compared to those with radiologically isolated syndrome (RIS) or early relapsing–remitting MS (RRMS) and (b) lower cerebellar MTR is associated with greater clinical disability.
Methods
Participants
Participants were enrolled between 2019 and 2022 through four sites of the Canadian Prospective Cohort Study to Understand Progression in Multiple Sclerosis (CanProCo): 6 St. Michael’s Hospital (SMH), University of British Columbia (UBC), Centre Hospitalier de l’Université de Montréal (CHUM), and University of Alberta (UALB). This study included people with RIS, RRMS (including clinically isolated syndrome with MRI evidence of dissemination in space), and PPMS, and control participants (CON). RIS and MS were diagnosed according to the 2009 Okuda criteria 7 and 2017 McDonald criteria, 8 respectively. Inclusion and exclusion criteria can be found in the Supplemental Methods. All participants provided written informed consent. This study was approved by the research ethics boards (SMH: 18-325, UBC: H18-03047, CHUM: 2019-8085, 18.293—YP, UALB: Pro00086907).
Clinical data acquisition
Neurologic and cognitive function in people with RIS, RRMS, and PPMS was assessed using the multiple sclerosis performance test (MSPT), an iPad-based tool closely aligned with the traditional multiple sclerosis functional composite (MSFC).9,10 The MSPT measures included the walking speed test (WST), manual dexterity test (MDT) of the dominant hand, processing speed test (PST), and contrast sensitivity test (CST). 9 When the MSPT was unavailable or not preferred by participants, the timed 25-foot walk (T25W), 9-hole peg test (9HPT), symbol digit modalities test (SDMT), and Sloan low-contrast letter acuity test (LCLAT) were used. 10 In addition, the Kurtzke expanded disability status scale (EDSS), including the cerebellar functional system score (C-FSS), was evaluated. 11
MRI data acquisition
MRI data were acquired at each site using 3.0 T systems: Siemens Magnetom Skyra at SMH (20-channel receiver coil), Philips Ingenia Elition at UBC (16-channel coil), Philips Ingenia at CHUM (16-channel coil), and Siemens Prisma at UALB (64-channel coil). All receiver coils contained head and neck units. A three-dimensional (3D) T1-weighted sequence was acquired for tissue segmentation, image registration, and brain volume measurement. A 3D T2-weighted fluid-attenuated inversion recovery (FLAIR) sequence was acquired for lesion segmentation. To compute MTR, 3D gradient echo (GRE) sequences were acquired with (MTon) and without (MToff) an MT saturation pulse. MRI acquisition parameters are provided in Supplemental Table S1.
MRI data analysis
MRI data were analyzed using Advanced Normalization Tools (ANTs) (https://stnava.github.io/ANTs/), Functional Magnetic Resonance Imaging of the Brain Software Library (FSL) (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki), Spinal Cord Toolbox (SCT) 12 (https://spinalcordtoolbox.com/), and FreeSurfer (https://surfer.nmr.mgh.harvard.edu/).
T1-weighted images were processed with N4 bias field correction, brain extraction using the Open Access Series of Imaging Studies (OASIS) template, linear registration to MTon images, and non-linear registration to the Montreal Neurological Institute (MNI)-152-T1-1 mm template (rigid, affine, and deformable symmetric normalization transformations). Analyses were conducted in each participant’s MT space, with regions of interest (ROIs) transformed from MNI space using inverse warp.
ROIs were defined using atlases integrated in FSL: the whole cerebellum (MNI Structural Atlas), anterior and posterior cerebellar lobes (Probabilistic Cerebellar Atlas), and the superior, middle, and inferior cerebellar peduncles (SCP, MCP, ICP) (JHU-ICBM-DTI-81 White Matter Label Atlas) (Figure 1). ROIs were thresholded at a probability of 0.9 (0.8 for smaller ROIs), eroded, and binarized.
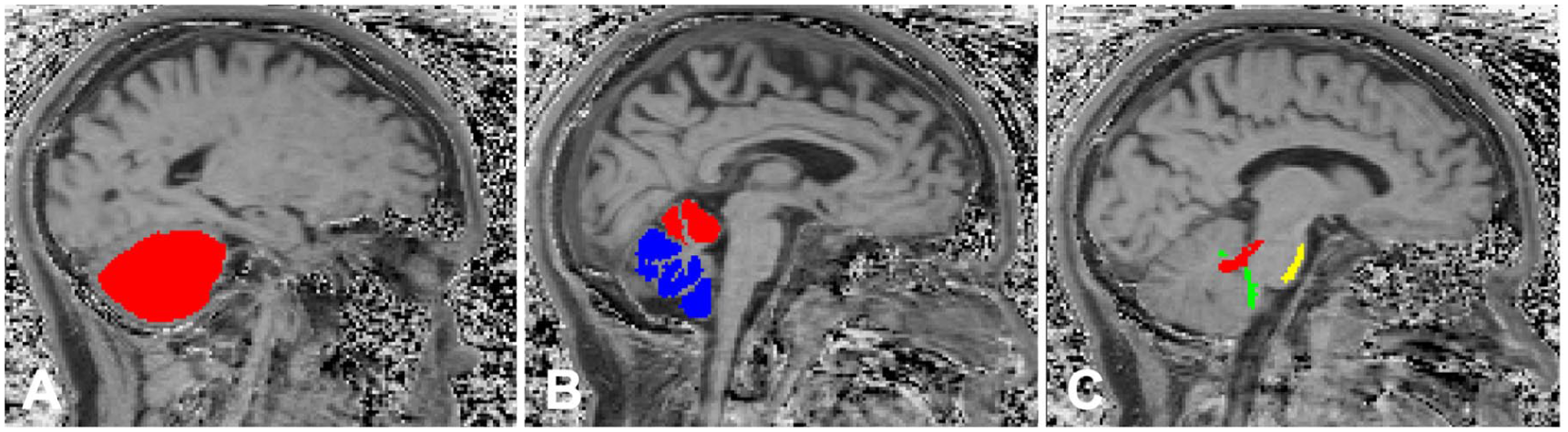
Example sagittal brain MTR map from a PPMS participant with regions of interest overlaid: (a) whole cerebellum (red), (b) anterior (red) and posterior (blue) cerebellar lobes, and (c) superior (red), middle (yellow), and inferior (green) cerebellar peduncles.
Brain lesions, including cerebellar lesions, were segmented on T2-FLAIR images using the Method for Inter-Modal Segmentation Analysis (MIMoSA). 13 Lesion masks were registered to each participant’s MT space and used to exclude lesional tissue from the ROIs, allowing analysis of normal-appearing brain tissue. MTR was calculated voxelwise as MTR = [(MToff − MTon)/MToff] × 100% using the SCT.5,12 Mean MTR was extracted from each normal-appearing ROI. FreeSurfer was run via the Canadian Brain Imaging Research Platform (CBRAIN) (https://cbrain.ca/) to compute brain volume from T1-weighted images, which was then normalized to intracranial volume to account for individual variation in head size.
Statistical analysis
Statistical analyses were performed using R software (https://www.r-project.org/). Analysis of covariance (ANCOVA) was used to assess the group differences in MTR, controlling for age, sex, MRI system vendor type, and normalized brain volume, with Tukey’s post hoc test for each ROI. Adjusted mean MTR was computed using estimated marginal means (“emmeans” package), and relative percentage differences between groups were calculated. Multiple linear regression analyses were conducted to evaluate the associations between MTR in each ROI and clinical measures for each MS subtype, adjusting for age, sex, MRI system vendor type, and normalized brain volume. Given the exploratory nature of this cross-sectional study, associations are presented as exploratory (with 95% confidence interval (CI)) and statistical (false discovery rate (FDR)-corrected p-values). FDR-corrected p-values < 0.05 were considered statistically significant.
Results
A total of 301 pwMS (mean age (SD) = 39.0 (11.1) years, 69.1% female, mean disease duration (SD) = 1.2 (1.8) years, median EDSS score (range) = 1.5 (0.0–6.5)) and 42 CON participants (mean age (SD) = 38.0 (10.6) years, 64.3% female) were included after excluding 2 RIS, 7 RRMS, 3 PPMS, and 1 CON participants due to imaging artifact, acquisition errors, or major tissue segmentation errors. Participants included 53 RIS, 202 RRMS, and 46 PPMS. Overall, 8% of participants were receiving disease-modifying therapy (DMT): 1.9% of RIS participants received minocycline, none of the RRMS participants were on DMT at baseline (as per the study inclusion criteria), and 50% of PPMS participants were on ocrelizumab. Table 1 presents the demographic and clinical characteristics of participants included in this cross-sectional study.
Demographics, clinical, and MRI characteristics of study participants.
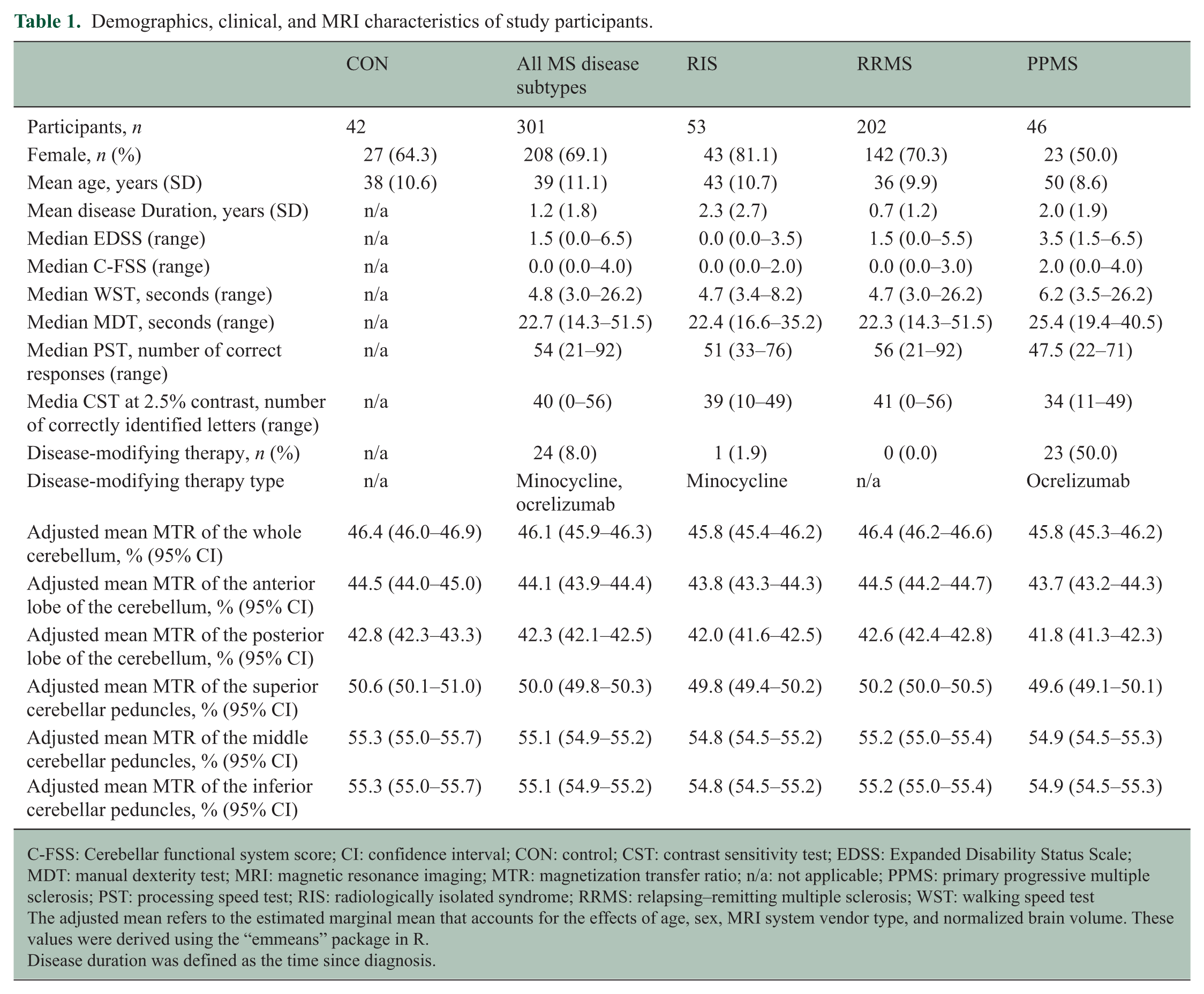
C-FSS: Cerebellar functional system score; CI: confidence interval; CON: control; CST: contrast sensitivity test; EDSS: Expanded Disability Status Scale; MDT: manual dexterity test; MRI: magnetic resonance imaging; MTR: magnetization transfer ratio; n/a: not applicable; PPMS: primary progressive multiple sclerosis; PST: processing speed test; RIS: radiologically isolated syndrome; RRMS: relapsing–remitting multiple sclerosis; WST: walking speed test
The adjusted mean refers to the estimated marginal mean that accounts for the effects of age, sex, MRI system vendor type, and normalized brain volume. These values were derived using the “emmeans” package in R.
Disease duration was defined as the time since diagnosis.
After adjusting for age, sex, MRI system vendor type, and normalized brain volume, group differences in MTR were observed across several normal-appearing cerebellar ROIs in an exploratory analysis (Figure 2). In PPMS, MTR was lower compared with CON in the posterior lobe (relative percentage difference = −2.3%, 95% CI: −1.88, −0.08) and SCP (−2.0%, 95% CI: −1.83, −0.07), and lower compared with RRMS in the posterior lobe (−1.9%, 95% CI: −1.50, −0.04), whole cerebellum (−1.3%, 95% CI: −1.26, 0.04), and anterior lobe (−1.8%, 95% CI: −1.52, 0.07). In RIS, lower MTR were observed compared with RRMS in the whole cerebellum (−1.3%, 95% CI: −0.02, 1.12) and anterior lobe (−1.6%, 95% CI: −0.03, 1.35), and compared with CON in the posterior lobe (−1.9%, 95% CI: −1.61, 0.06) and SCP (−1.6%, 95% CI: −1.58, 0.05). No differences in MTR were observed between RRMS and CON. No differences in MTR between groups remained significant after FDR correction.
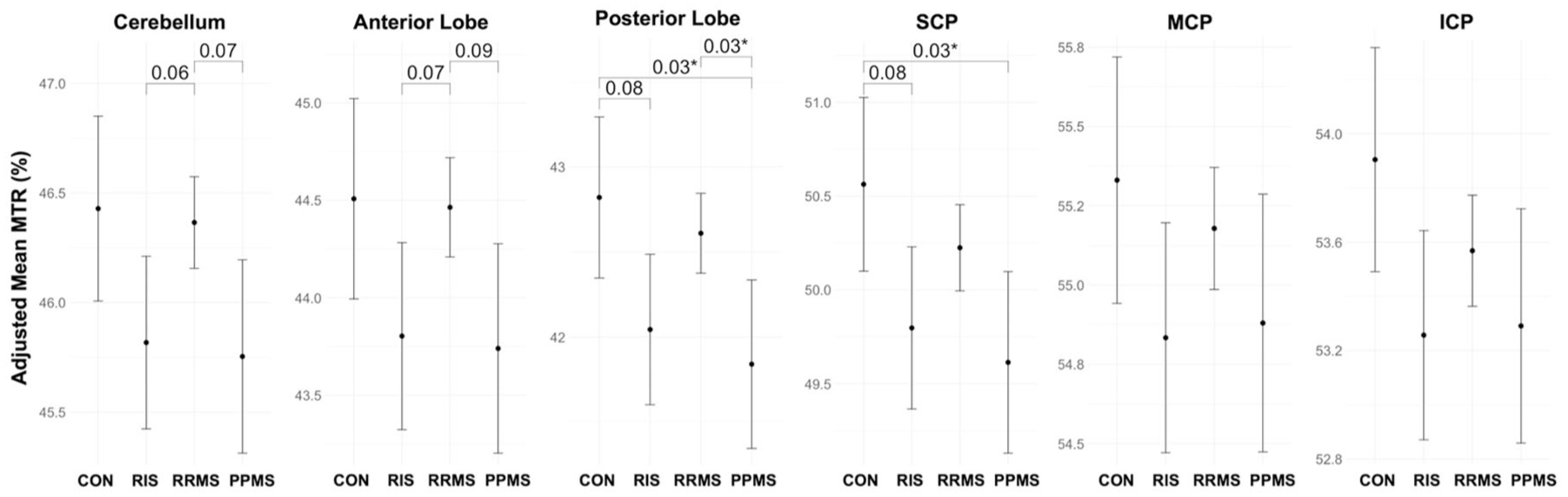
Adjusted mean MTR comparisons between CON, RIS, RRMS, and PPMS in the whole cerebellum, anterior and posterior lobes of the cerebellum, and superior, middle, and inferior cerebellar peduncles (S/M/ICP) with uncorrected p-values < 0.1. Adjusted mean MTR was derived using estimated marginal means (“emmeans” package in R) adjusted for age, sex, MRI system vendor type, and normalized brain volume. Uncorrected p-values < 0.05 are marked with an asterisk.
When evaluating the relationships between MTR in normal-appearing cerebellar ROIs and clinical measures using multiple linear regression models adjusted for age, sex, MRI system vendor type, and normalized brain volume, potential associations were observed across all MS subtypes (Table 2 and Figure 3). MTR showed the strongest associations with MDT across all MS subtypes. In RIS, higher MDT (more impaired manual dexterity) was associated with lower MTR in the posterior lobe (β = −0.87, 95% CI: −1.64, −0.10) and ICP (β = −1.04, 95% CI: −1.95, −0.13). In RRMS, higher MDT was associated with lower MTR in the ICP (β = −0.67, 95% CI: −1.15, −0.19). In PPMS, higher MDT was associated with lower MTR in the anterior lobe (β = −0.87, 95% CI: −1.44, −0.31).
Relationships between MTR and clinical measures in multiple linear regression models for RIS, RRMS, and PPMS with uncorrected p-values < 0.1.
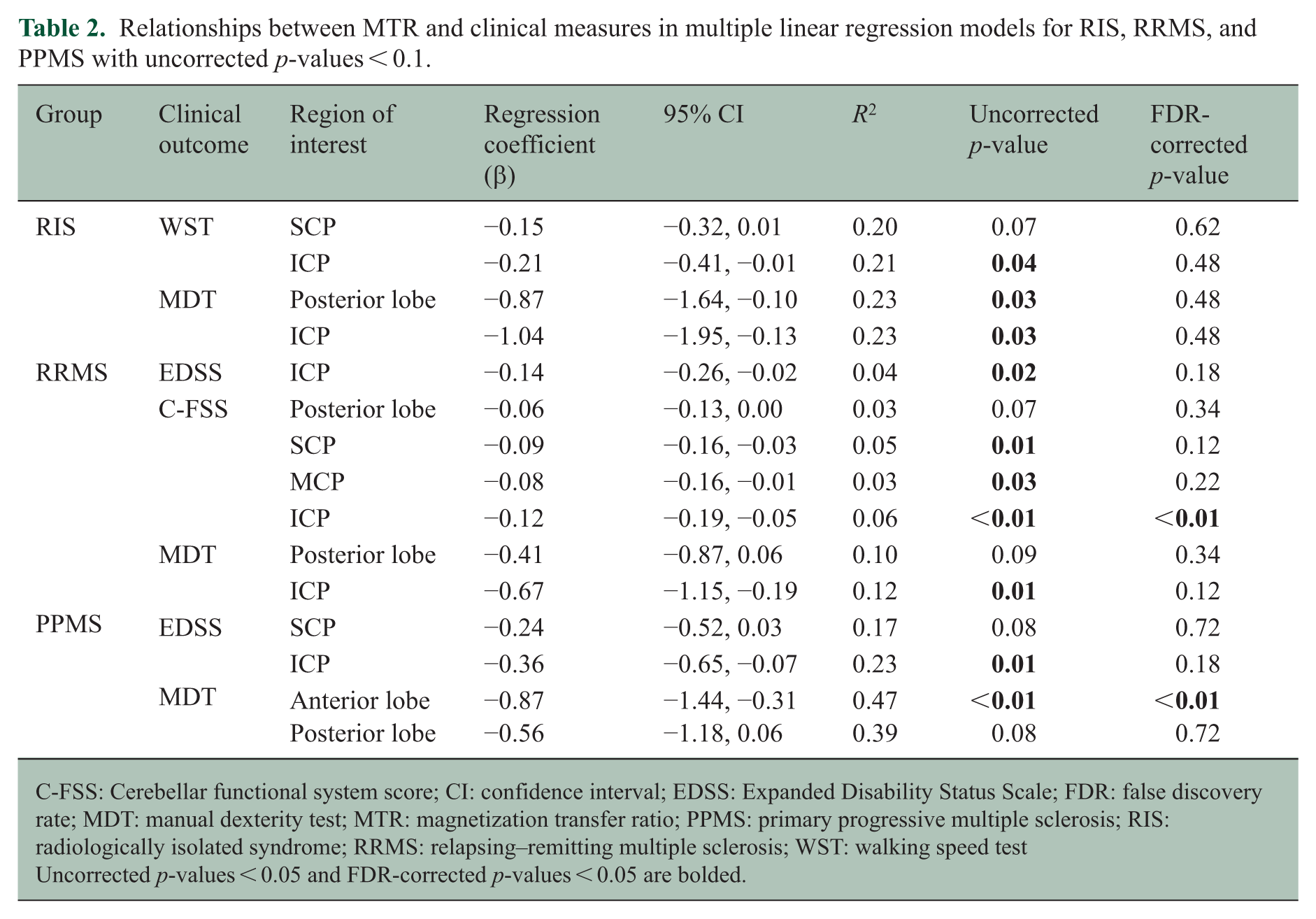
C-FSS: Cerebellar functional system score; CI: confidence interval; EDSS: Expanded Disability Status Scale; FDR: false discovery rate; MDT: manual dexterity test; MTR: magnetization transfer ratio; PPMS: primary progressive multiple sclerosis; RIS: radiologically isolated syndrome; RRMS: relapsing–remitting multiple sclerosis; WST: walking speed test
Uncorrected p-values < 0.05 and FDR-corrected p-values < 0.05 are bolded.
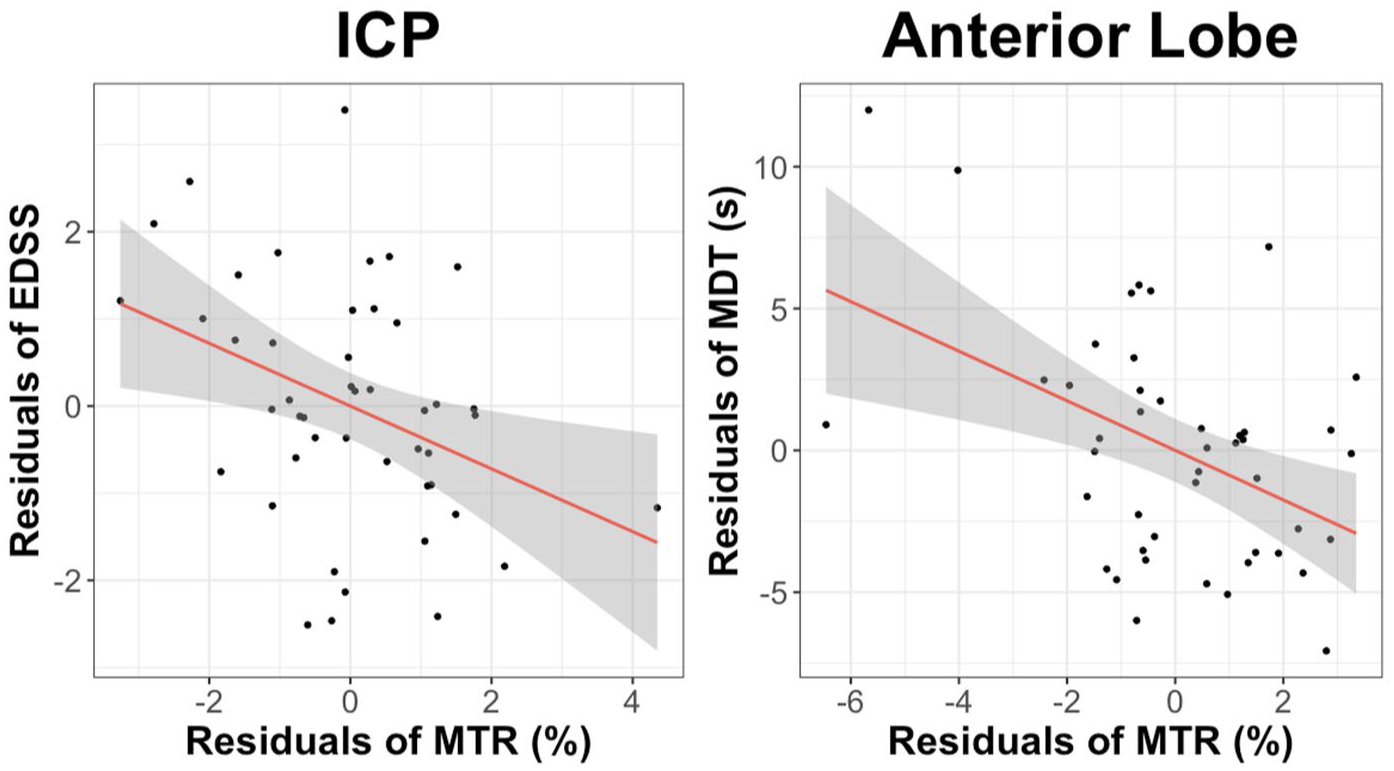
Example partial regression (added variable) plots demonstrating the adjusted relationships between inferior cerebellar peduncle MTR vs EDSS (left) and anterior lobe MTR vs MDT (right) in people with PPMS, adjusted for age, sex, MRI system vendor type, and normalized brain volume in multiple linear regression models.
In RIS, higher WST (more impaired ambulation) was associated with lower MTR in the ICP (β = −0.21, 95% CI: −0.41, −0.01). No associations between WST and MTR were observed in any cerebellar ROIs in RRMS or PPMS. In RRMS, higher EDSS was associated with lower MTR in the ICP (β = −0.14, 95% CI: −0.26, −0.02) and higher C-FSS with lower MTR across all cerebellar peduncles (SCP: β = −0.09, 95% CI: −0.16, −0.03; MCP: β = −0.08, 95% CI: −0.16, −0.01; ICP: β = −0.12, 95% CI: −0.19, −0.05). In PPMS, higher EDSS was associated with lower MTR in the ICP (β = −0.36, 95% CI: −0.65, −0.07). No associations were observed between EDSS or C-FSS and MTR in RIS, or between C-FSS and MTR in PPMS, in any cerebellar ROIs. After FDR correction, only two associations remained statistically significant: higher C-FSS was associated with lower MTR in the ICP in RRMS (FDR-corrected p < 0.01), and higher MDT was associated with lower MTR in the anterior lobe in PPMS (FDR-corrected p < 0.01).
No associations were observed between PST or CST and MTR in any cerebellar ROIs across MS subtypes. Table 2 summarizes associations between cerebellar MTR and clinical measures with uncorrected p-values < 0.1, and Supplemental Table S2 reports all regression results.
Discussion
This cross-sectional, hypothesis-generating study evaluated cerebellar microstructural abnormalities using MTR and their associations with clinical measures in a large sample of participants with early MS (mean disease duration = 1.2 years, median EDSS = 1.5). Two statistically significant associations were observed after FDR correction: lower MTR in the ICP was associated with higher C-FSS (worse cerebellar function, such as motor coordination and balance) in RRMS, and lower MTR in the anterior lobe was associated with higher MDT (worse manual dexterity) in PPMS. In addition, several potential associations were observed across cerebellar regions and clinical measures; however, these should be interpreted with caution as exploratory, hypothesis-generating findings.
Notably, among the exploratory findings, MTR was most strongly associated with MDT (β = −1.04 to −0.67) and only weakly with EDSS or C-FSS (β = −0.36 to −0.08) across MS subtypes, suggesting that MDT, which is a measure of fine motor coordination, is more sensitive to subtle deficits with coordination in early MS. In contrast, EDSS is a composite measure weighted toward ambulatory impairment, and the degree of cerebellar dysfunction required to capture substantial ambulatory impairment was likely not present in early MS. This is supported by the limited associations between WST and MTR in RRMS and PPMS.
The most consistent associations were observed in the cerebellar peduncles, particularly the ICP, across all MS subtypes. This is likely because the cerebellar peduncles, especially the ICP, are key conduits connecting the cerebellum to widespread regions of the central nervous system, including the cerebrum, brainstem, and spinal cord. 14 The ICP connects the cerebellum with the medulla and spinal cord, integrating proprioceptive sensory input and playing a crucial role in coordination and balance, 14 which likely explains the observed associations between ICP MTR and relevant clinical measures.
Furthermore, in exploratory analyses, lower MTR was observed in PPMS compared with CON in the posterior lobe and SCP, whereas no differences were found between RRMS and CON in any cerebellar ROIs. MTR was lower in RIS compared with RRMS in the whole cerebellum and anterior lobe, but the difference did not reach statistical significance. These findings are likely related to the clinical characteristics of the RRMS group, which consisted primarily of newly diagnosed individuals with a mean disease duration of less than 1 year and relatively mild disability (median EDSS = 1.5). Although these individuals likely exhibited greater cerebellar microstructural abnormalities than CON, the magnitude of cerebellar tissue damage may not have been sufficient to clearly demonstrate group differences in MTR, particularly given the small sample size of the CON group.
After FDR correction for multiple testing was applied, none of the MTR differences between groups remained statistically significant. When relationships between cerebellar MTR in specific regions and clinical measures were corrected for FDR, higher C-FSS remained associated with lower MTR in the ICP in RRMS, and higher MDT remained associated with lower MTR in the anterior lobe in PPMS, while other associations were attenuated. These findings are not surprising, given the exploratory nature of the study and the anatomical and functional heterogeneity of the cerebellum. Nonetheless, the consistent directionality of effects across specific cerebellar regions and MS subtypes suggests potentially interesting patterns of cerebellar microstructural involvement that warrant further investigation in larger, independent cohorts.
Although cerebellar impairment is common in MS, affecting a wide range of neurological functions and even cognitive tasks,1,2 pathological changes, particularly in early MS, remain poorly understood. Diffuse cerebellar pathology beyond focal lesions has been underexplored using quantitative MRI due to technical challenges. The cerebellum’s complex anatomy, including its densely folded cortical gray matter, thin white matter layers, and location in the posterior fossa near bone and vascular structures, makes it difficult to image and segment accurately. However, recent advances, including cerebellum-specific atlases 15 and improved image processing tools such as ANTs (used here), have made cerebellar MRI analysis more feasible.
MTI was chosen over other advanced MRI techniques to evaluate cerebellar microstructure because it is widely available, has a relatively rapid scan acquisition time, and requires simple post-acquisition image processing. Practically, MTI is a semi-quantitative MRI technique that can be feasibly implemented in clinical trials and clinical practice, provided there is evidence of clinical utility. Furthermore, MTI has demonstrated clinical relevance in Phase II and III clinical trials, showing measurable changes in response to DMTs and corresponding correlations with clinical disability.16,17 Compared with measures of brain atrophy (the most common quantitative MRI measure in MS clinical trials), MTI offers the potential to detect earlier microstructural changes associated with clinical disability that precede irreversible neuroaxonal loss. Despite these advantages, MTI has limitations. Although MTR is sensitive to myelin content, 18 it can also be influenced by inflammation and edema. 19 Moreover, MTR can be affected by MT pulse characteristics, MRI hardware, and sequence parameters, further complicating biological and clinical interpretation. 20
Despite prior studies highlighting the cerebellum’s role in cognition,3,4 no significant relationships were observed between PST and MTR in any cerebellar ROIs across MS subtypes. This may be because PST captures only a single cognitive domain and may not capture the broader cognitive deficits associated with cerebellar dysfunction. The “cerebellar cognitive affective syndrome” 2 involves impairments in executive function, attention, visuospatial memory, language, and affect, which are not captured by the PST. The lack of association could also be due to the characteristics of the study population, which involved people early in their disease course with relatively mild disability. In contrast, Weier et al. 21 found correlations between cerebellar volume and processing speed; however, their study included participants with longer disease duration (16.2 years) and greater disability (median EDSS = 3.0). They also found that people with cerebellar signs were older, had greater disability, and longer disease duration than those without. 21 Future studies using a comprehensive cognitive battery will be important to evaluate cerebellar MTR in MS.
MTR has been extensively used to evaluate supratentorial brain regions, with studies ranging from single-center cohorts to large Phase II and III trials consistently demonstrating that lower MTR in normal-appearing brain tissue correlates with clinical disability and has prognostic value in MS.16,17,20 In contrast, cerebellar MTR remains underexplored, with most studies limited to conventional MRI measures.3,4,20 The limited studies that have examined cerebellar MTR align with our findings and suggest potential utility in detecting diffuse pathology not visible on conventional MRI.22–25 Previous studies showed lower cerebellar MTR in pwMS compared with CON.22,23 Romascano et al. 24 found that cerebellar MTR was associated with motor function, including arm function, independent of lesion load in early MS.24,25 Similarly, our study observed potential associations between normal-appearing cerebellar MTR and motor function, particularly manual dexterity in early MS. Iannucci et al. 25 showed that cerebellar MTR correlated most strongly with cerebellar dysfunction. Similarly, in our RRMS group, higher C-FSS was potentially associated with lower MTR across all cerebellar peduncles. Cerebellar MTR abnormalities have been reported in pwMS despite appearing normal on conventional MRI, 23 highlighting the need for more sensitive MRI measures to detect diffuse cerebellar changes. Together, these findings support cerebellar MTR as a sensitive measure of early and clinically relevant cerebellar pathology, with potential utility for disease monitoring and treatment evaluation in MS.
Beyond MTI, other advanced MRI techniques, such as diffusion tensor imaging (DTI) and functional MRI (fMRI), have highlighted the cerebellum’s role in MS, with DTI measures and functional connectivity changes correlating with clinical outcomes.26–30 While DTI is sensitive to white matter microstructure, MTR provides complementary insights into myelin integrity, which may precede atrophy and is practical for use in clinical trials and clinical practice. Our findings further expand on existing DTI literature by demonstrating that region-specific MTR changes associate with clinical measures across MS subtypes, as MTR is a complementary, clinically feasible imaging measure. Together, these studies highlight the critical role of the cerebellum in MS-related functional impairment and the need for sensitive imaging markers of diffuse microstructural change.
This study has several limitations. First, only MDT data were used to assess upper limb function. Including additional clinical measures reflecting subtle incoordination may have offered a broader assessment of upper limb function. Similarly, only PST was used to assess cognitive function. Although PST is sensitive in MS, a more comprehensive neuropsychological battery may have uncovered relationships between cerebellar MTR and subtle cognitive deficits. Second, contrast-to-noise limitations precluded analysis of smaller cerebellar structures, which may have clinical relevance, and analyses primarily included gray matter and limited white matter due to cerebellar atlas constraints. Nonetheless, given that gray matter is extensively affected in MS, even in early stages, and that gray matter pathology correlates with clinical disability and cognitive dysfunction,31,32 the use of gray matter-rich cerebellar regions likely did not compromise our goal of identifying clinically relevant cerebellar microstructural changes. Third, although most participants completed iPad-based MSPT, a small subset underwent traditional clinical assessment instead. No significant differences were observed between corresponding measures (WST and T25W, or MDT and 9HPT), allowing data to be combined. Finally, future studies incorporating additional advanced MRI techniques, such as DTI, fMRI, and other myelin-sensitive MRI techniques, may provide complementary insights into cerebellar pathology and its clinical relevance. The absence of longitudinal data precludes assessment of the prognostic utility of cerebellar MTR; however, establishing cross-sectional associations with clinical measures is a necessary first step in determining whether longitudinal evaluation is warranted and in identifying clinically informative imaging measures and anatomical targets for clinical trials and clinical practice.
Notwithstanding these limitations, our study has notable strengths. Data were collected from four major Canadian MS centers using 3.0 T MRI systems from two major MRI system vendors, and the cohort included people across a wide spectrum of MS phenotypes. Despite the complexities of a multi-site, multi-vendor study, potential associations were observed between cerebellar MTR and clinical measures, particularly manual dexterity, even after adjusting for normalized brain volume and removing visible lesions. These findings highlight MTR as a potential paraclinical measure of cerebellar involvement that may have utility for monitoring MS and treatment effects in future studies. Longitudinal follow-up of this cohort will provide further insights into the evolution of cerebellar pathology and its clinical implications in MS.
Supplemental Material
sj-docx-1-msj-10.1177_13524585261450926 – Supplemental material for Cerebellar magnetization transfer ratio and its relationship to clinical outcomes in radiologically isolated syndrome and multiple sclerosis
Supplemental material, sj-docx-1-msj-10.1177_13524585261450926 for Cerebellar magnetization transfer ratio and its relationship to clinical outcomes in radiologically isolated syndrome and multiple sclerosis by Lisa Eunyoung Lee, Marc Khoury, Nathan Churchill, Irene Vavasour, Poljanka Johnson, Anthony Traboulsee, Larry D Lynd, Alexandre Prat, Yunyan Zhang, Anthony Feinstein, Simon J Graham, Mojgan Hodaie, Shannon Kolind, Tom A Schweizer and Jiwon Oh in Multiple Sclerosis Journal
Footnotes
Acknowledgements
The authors would like to sincerely thank all study participants, the CanProCo Executive Board Committee, and collaborators. This study was funded by MS Canada, Biogen Canada, Brain Canada Foundation, Hoffmann-La Roche Limited, and the Government of Alberta.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lisa Eunyoung Lee, Marc Khoury, Nathan Churchill, Irene Vavasour, Poljanka Johnson, Alexandre Prat, Yunyan Zhang, Simon J. Graham, and Tom A. Schweizer report no conflicts of interest relevant to this study. Anthony Traboulsee is the MS Canada Research Chair at the University of British Columbia. Larry Lynd has received grant funding from Pfizer Canada for research unrelated to multiple sclerosis. Mojgan Hodaie received support from NIH as co-investigator in projects that focus on neuroimaging. Anthony Feinstein received grant support from MS Canada and the MacArthur and Knight Foundations. He has book royalties from Johns Hopkins University Press, G Editions, and Cambridge University Press. He received speaking honoraria from Novartis and Merck-Serono. Shannon Kolind received consulting fees from AbbVie and has received research support from Roche, Sanofi-Genzyme, and Biogen. Jiwon Oh is supported by the Waugh Family Chair in MS Research at the University of Toronto and the Barford and Love MS Fund of the St. Michael’s Hospital Foundation, and has received research funding from Biogen-Idec, Eli-Lilly, EMD Serono, Novartis, Roche, and Sanofi-Genzyme.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by MS Canada, Biogen Canada, Brain Canada Foundation, Hoffmann-La Roche Limited, and the Government of Alberta.
ORCID iDs
Data Availability Statement
Anonymized data will be shared upon request with qualified investigators who have established data-sharing agreements in place.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.