
Abstract
The measures, restrictions, and death-related rituals in the COVID-19 pandemic have affected the mourning-related routines of individuals. Moreover, mourning processes have been affected by the restriction of death-related cultural rituals, funeral ceremonies performed only by the officials, and the prohibition of visiting graves. This study aims to investigate the experiences of individuals who lost their loved ones in Turkey during the COVID-19 pandemic. For that purpose, the phenomenological method is employed in the design of the study. Individual interviews were conducted with nine participants who lost their relatives during the COVID-19 pandemic. Data were collected through semi-structured interview forms prepared by the researchers. The study participants described the various factors contributing to the grief and mourning process in the COVID-19 pandemic. These factors were categorized into three following main categories: grief and mourning responses of the individuals lost loved ones, including cognitive, emotional, and behavioral responses; risk factors including the expectation of harm, unfinished business, and restriction of death-related religious-cultural rituals; and protective factors including relative support (i.e., family, spouse, friend, partner), tele-support (i.e., mobile phone, internet, social media), positive coping strategies (cognitive, behavioral, and religious-spiritual), and delayed business. The “delayed business” concept was also addressed within protective factors and explained in general terms. Finally, the findings were discussed considering the literature and presented some theoretical and practical implications.
Introduction
Since 2019, the world has struggled with a global pandemic: COVID-19. Millions of people died due to the pandemic. Turkey is one of the countries with the highest number of cases globally (WHO, 2021). Due to the rapid spread of the virus and the emerging mutants, the measures taken have been tightened, including the curfew, mandatory use of masks, social distance, and hygiene rules. Keeping people away from public areas minimizes the spread of the virus. Similarly, restrictions have been imposed on communal areas in Turkey, and partial closure has begun to be implemented. Various measures were taken, including curfew at certain hours/days; limiting the activities of cafes and restaurants to takeaway; reducing the number of people using public transport by 50% of the vehicle capacity; and flexible working hours (Government of Turkey, 2021). The pandemic affected all individuals physically, economically, psychologically, and socially with these measures.
Many studies reported that the COVID-19 pandemic and restrictions negatively affected mental health (Erbiçer et al., 2021; Metin et al., 2021, 2022; Pfefferbaum & North, 2020; Rajkumar, 2020; Vindegaard & Benros, 2020; Yalçın et al., 2022). In addition, safety measures such as restricting family visits, not allowing to accompany patients hospitalized in health institutions, and complete prohibition of intubated patient visits have been widely implemented to reduce the effects of COVID-19 (Çelik & Gündüz, 2020; Wallace et al., 2020). In this process, patients (infected or uninfected) hospitalized in health institutions were isolated entirely to reduce the risk of transmission, regardless of the effects of isolation on patients and their families (Ingravallo, 2020; Wallace et al., 2020). Some of these patients died alone, without their relatives. Those who lost their relatives could not find the opportunity to say goodbye to their loved ones (Ingravallo, 2020). Religious-cultural rituals such as funerals, burials, and condolences after the loss were either partially or entirely prohibited in many countries to prevent the spread of the virus. Considering social distancing rules, only close family members were allowed to attend funerals. In some cases, the relatives of the deceased were not allowed to attend the burial, and the officers carried out the burial ceremony by wearing protective clothing (Hamid & Jahangir, 2020; Lazzerini & Putoto, 2020; Government of Canada, 2021; Government of Turkey, 2021; O’Mahony, 2020; Omonisi, 2020; Public Health England, 2021).
People react in a variety of ways to loss. When emotions such as sadness, anger, guilt, loneliness, and hopelessness are experienced intensely, it is called grief (Stroebe et al., 2001). The feeling of sadness is experienced intensely during the grieving process (James & Friedman, 2009). As a biological emotion, one of the functions of sadness is to help people regain their strength (Matsumoto & Hwang, 2013). Sometimes, when sadness is experienced intensely, behaviors like depression periods can be observed. For example, introversion, negative influence on routine behaviors, and desire to sleep more (Bui, 2018; Doka & Martin, 2011). However, mourning is not a psychopathological condition, it is a normal process that exists in the flow of life and shows that the living thing is not immortal. The experience of grief and mourning show cultural differences. Although different behaviors are observed in societies with different beliefs, emotions such as sadness experienced by people are similar (Ekman, 2007). We thought that experiencing grief and mourning may have been changed during the COVID-19 pandemic due to restrictions on rituals and traditions related to mourning and grief.
Although the restriction or prohibition of religious-cultural rituals such as funerals, burials, condolences, and other rituals (i.e., grave visit, Mawlid) prevents the spread of the virus, it makes mourning difficult. In this process, individuals might not have the opportunity to say goodbye to the person they lost, as any loss experienced by the individual was fast and sudden. Not being with them at the last moment, not being able to touch them for the last time, and not saying goodbye have made the mourning process, which is already difficult to cope with, more destructive for individuals (Aguiar et al., 2020; Hamid & Jahangir, 2020; Omonisi, 2020; Wallace et al., 2020). Besides, after the loss, individuals need the moral support of their loved ones and be together with them. However, it has become almost impossible to provide face-to-face social support during the pandemic (eCondolence, 2021; Farahmandnia et al., 2020; Kokou-Kpolou et al., 2020). In the non-COVID-19 process, individuals hug the people they love, cry, and closely share their pain. They have been deprived of this support due to physical distance rules and avoidance of contact (Farahmandnia et al., 2020).
Mourning is the individual’s response to loss (Archer, 2003). Many factors can affect these responses, from the event’s meaning for the individual to cultural elements (Marrone, 1999). Almost every society has its rituals and traditions regarding death and mourning. Although these rituals and traditions differ from society to society or culture to culture, they have been going on for thousands of years (Hoy, 2013). For example, in Muslim societies, the funeral prayer of the deceased is performed in mosques. The deceased is buried by his/her relatives and loved ones, with religious officials' participation. Following the ceremony, prayers are said at the grave, and the Qur’an is read. After the burial, people visit the deceased’s relatives to offer consolation and condolences (Rubin & Yasien-Esmael, 2004; Sheikh, 1998). In Christian societies, the body of the deceased is specially prepared for burial. A ceremony is held before the burial with the coffin closed or open, relatives of the deceased share their memories and feelings with other participants (Ramshaw, 2010). Similarly, there are death-related rituals and traditions in other religious beliefs (Hoy, 2013). The main function of these rituals and traditions is to help individuals who experienced the loss overcome their mourning. Besides, it helps individuals accept the reality of death, provide an environment where they can express their feelings and thoughts comfortably, and give meaning to the loss they experience (Castle & Phillips, 2003; Reeves, 2011). However, ceremonies in mosques, churches, temples, and synagogues or other rituals that bring people together have been restricted or entirely prohibited during the pandemic (Hamid & Jahangir, 2020; Lazzerini & Putoto, 2020; O’Mahony, 2020; Omonisi, 2020). In other words, rituals, ceremonies, and traditions related to mourning and grief have changed with the pandemic in the countries affected by the virus. This change negatively could also affect the individual’s experiencing loss in Turkey during the COVID-19 outbreak. For this reason, individuals who have lost their loved ones may be at risk of complicated/prolonged grief (Mayland et al., 2020; Walsh, 2012). Based on all these, this study aims to examine the experiences of individuals who lost their loved ones due to COVID-19 during the COVID-19 pandemic in the Muslims of Turkey and reveal theoretical and practical implications.
Methodology
Study design
A qualitative research method, the phenomenology approach, was employed in this study. Phenomenology is a method that focuses on evaluating the experiences of individuals (Jasper, 1994). The concept was proposed by the German philosopher Husserl and detailed by Heidegger (Rodriguez & Smith, 2018). According to this approach, the meaning that individual responses to the same event may differ. This study investigated the participants' experiences regarding the grief and mourning process during the pandemic. The responses and perceptions of each participant to their loss may differ. The restrictions and lockdowns applied during the pandemic and other factors, such as getting infected, may have affected the mourning experiences of individuals. Therefore, the phenomenological approach was preferred in the design of this study. The recordings were transcribed and analyzed by Miles and Huberman’s phenomenological analysis method.
Participants
Demographic information on participants and their deceased relatives.

aHow long ago he/she lost her relative at the time of the interviews.
Data collection tools
The demographic information form includes information about the participants' age, gender when they lost their relative, the cause of death, relative’s age, and degree of relative deceased.
The semi-structured interview form prepared by the researchers consists of nine questions prepared to evaluate the participants' experiences regarding the mourning process during the pandemic. The first two questions are related to the way of experiencing mourning. The third question is about coping with mourning; questions four to eight are related to rituals, whereas the last question is “Is there anything else you would like to add?” The questions of the semi-structured interview form are given in Appendix A.
Data collection
The semi-structured interview form developed by the researchers was used to collect data. First, the questions of the interview were prepared based on the literature on the grief and mourning process in the COVID-19 pandemic and non-COVID period (e.g., Aguiar et al., 2020; Castle & Phillips, 2003; Hamid & Jahangir, 2020; Hoy, 2013; Lazzerini & Putoto, 2020; Ramshaw, 2010; Reeves, 2011; Rubin & Yasien-Esmael, 2004; Sheikh, 1998; Wallace et al., 2020). Then, the researchers requested the opinions of two experts who have studies on grief and mourning regarding the interview questions. The interview form was finalized by the researchers based on expert opinions.
Ethics committee approval was obtained before data collection (Erciyes University Social and Humanities Ethics Committee – 29.12.2020; Application number: 210). The researchers prepared an interview protocol about how to conduct the interviews and what will be considered during the interview. Afterwards, the researcher contacted psychiatrists/counselors/psychologists/social workers in some cities of Turkey (e.g., Ankara, İzmir, Kayseri, İstanbul) to reach potential participants. In addition, the announcements were posted on some social media platforms (e.g., WhatsApp, Twitter). Then, two researchers (ESE, and AM) contacted voluntary participants by phone, informed the participants on the purpose of the study, and scheduled an appointment.
Firstly, a preinterview was conducted with two participants who lost their loved ones before the main interviews, and the conditions that could negatively affect the validity and reliability were adjusted. The voluntary participation form was shared with the participants in the data collection phase, and they were informed about the study. Demographic information form and the semi-structured interview form were used to collect data. The interviews were conducted between January and March 2021. Due to the risk of infection, restrictions, and lockdown in the pandemic, the interviews were held online (Zoom Meetings) and recorded. The average duration of the interview was 25 minutes.
Validity and Reliability
Trustworthiness is used as an equivalent for internal/external validation and internal/external reliability in qualitative research (Guba & Lincoln, 1985). Trustworthiness, used by Guba and Lincoln (1985), was achieved by credibility, transferability, dependability, and confirmability in the present study. For credibility (internal validity), preparation of the questions of the interview based on the grief and mourning literature, requesting opinions of experts on the interview questions, participant confirmation on the transcribed data, and warm-up conversation with participants to make the participants more comfortable and create an atmosphere of trust at the beginning of the interview were ensured (Creswell, 2014; Guba & Lincoln, 1985; Miles & Huberman, 1994; Patton, 2014). For transferability (external validity), a purposive sampling method was used to recruit the participants, and study design, preparation of interview questions, data collection stage, and data analysis (creating codes, subcategories, and categories) were described in detail. In addition, direct quotations obtained from the participants' statements were presented (Creswell, 2014; Guba & Lincoln, 1985; Miles & Huberman, 1994; Patton, 2014). For dependability (internal reliability), and confirmability (external reliability), the interview questions were formed based on the theoretical baseline as well as expert and participant confirmation during the data collection process. In addition, the study findings were discussed based on existing relevant literature (Guba & Lincoln, 1985; Miles & Huberman, 1994; Patton, 2014).
Data analysis
In qualitative studies, the data analysis process consists of the following three stages: (a) encoding the data, (b) visualization of the dataset with graphs, tables, or figures, and (c) comparing, interpreting, and confirmation of concepts, themes, and relationships (Miles & Huberman, 1994). The transcripted recordings in this study were analyzed by the content analysis method, following the steps suggested by Miles and Huberman (1994). Firstly, the recordings were transcribed for content analysis, and the transcripts were sent to the participants to confirm the texts and give them an opportunity to include if they had additional perceptions or experiences they would like to add. In the first stage of the content analysis, codes were created separately by the two researchers (ESE and AM) in the team based on the transcripted recordings. A coding percentage was obtained by comparing the differences and similarities of the codings. It is recommended that the percentage of reliability should be at least 70% in qualitative studies (Miles & Huberman, 1994; Yıldırım & Şimşek, 2016). Percent agreement was calculated as .87 in this study. Afterwards, codes were inductively grouped into subcategories, and categories were named based on their contents. The main purpose at this stage is to find the similarities between the codes. The first two stages provide researchers to create a system in which they can organize the data (Miles & Huberman, 1994). Conflicting on the contents of categories and subcategories was discussed and resolved by arbitration (third author). Finally, the results were reported and interpreted in the data reporting stage.
Results
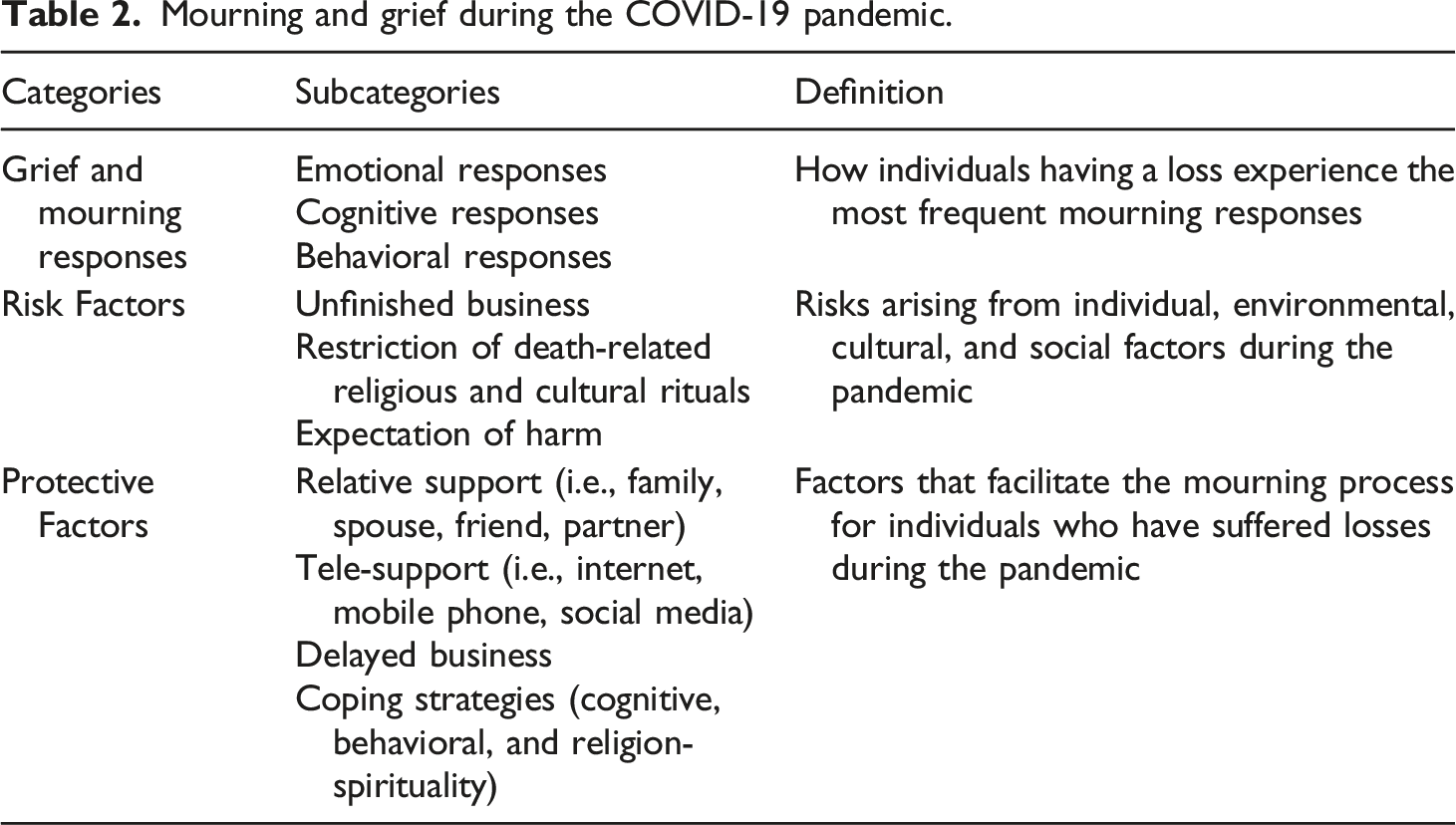
Mourning and grief during the COVID-19 pandemic.
Grief and mourning responses
This main category consisted of three subcategories, namely, cognitive responses, emotional, responses, and behavioral responses of individuals who lost their loved ones in the COVID-19 pandemic.
Emotional responses
Emotional reactions such as sadness, hopelessness, loneliness, helplessness are normal and natural reactions in grief and mourning process (James & Friedman, 2009). However, due to the COVID-19 pandemic, death-related religious-cultural rituals that people enable to share their grief were restricted, and people who have lost loved ones have been deprived of the support of their neighbors, relatives, and friends (Hamid & Jahangir, 2020; Kokou-Kpolou et al., 2020). Therefore, the individuals who experienced a loss during the pandemic were observed to experience emotional responses such as regret, sadness, helplessness, and loneliness. “Nothing could be done, neither during the treatment nor after it. You feel helpless” (
Cognitive responses
Cognitive reactions such as difficulty concentrating, and thoughts about the deceased are frequently seen in individuals who lost loved ones (Stroebe et al., 2001; Worden, 2018). Cognitive reactions seen in the non-COVID-19 period were also observed during the pandemic. The most common cognitive response among participants was thoughts about the deceased (reminiscence): “Because we used to drink tea and coffee together. Well, I was buying a cake and go to her, she was pouring the tea. I was going there with my friends.” (
Behavioral responses
Some behavioral reactions of individuals who lost loved ones are crying, excessive physical activities, obsessive behaviors, visiting the places reminding the deceased, and alcohol and substance use (Gross, 2018). Regarding behavioral responses, one participant stated that she sometimes cried: “Some nights I still cry when I think of grandpa.” (
Risk Factors
The three subcategories of this main category were expectation of harm, unfinished business, and restriction of death-related religious-cultural rituals.
Expectation of harm
One of the circumstances accompanying mourning in the COVID-19 pandemic was the expectation of harm
Unfinished business
One of the most important factors that enable individuals to overcome the grieving process is to overcome the unfinished business in their relationship with the deceased and to be able to say ‘goodbye’ to the deceased (Worden, 2001). Unfinished business, a concept in gestalt therapy, is addressed as feelings that are not expressed during relationships (Perls et al., 1951; Tobin, 1971). Due to the restrictions during the outbreak, the participants could not find the opportunity to say goodbye to their deceased relatives and be with them before they passed away, which causes more unfinished businesses to be experienced in this process. “If there was no pandemic, it was possible to visit the intensive care unit during the visiting hours. However, there were no visits due to the pandemic, so we could only call his doctor once a day and get information about my father” (
In addition, the lack of death-related rituals such as funerals, burials, and offering condolences causes unfinished business related to religious-cultural rituals. “…it should not have been like this. An imam should read the Qur’an at her funeral. I don’t know, they should have prayed. They should water the grave” (
Some participants stated that they could not express their feelings during this process, or they suppressed their feelings after the loss to avoid making other relatives upset: “But we couldn’t perform those. Everyone lived something, but all endured in silence. To prevent others from being upset. The things we can’t face will blow up in us after a while, spiritually and psychologically” (
Restriction of death-related religious and cultural rituals
One of the most important determinants of individuals’ mourning responses after the loss is the culture they live in (Reeves, 2011; Castle & Phillips, 2003). Although rituals differ from culture to culture, it can be said that these rituals have the functions of commemorating the deceased and socially supporting the individuals who experience the loss (Hoy, 2013; Marrone, 1999). However, religious-cultural rituals such as funerals, burials, condolences, and other rituals (i.e., grave visit, prayers of seventh, 40th, fifty-second day, Mawlid) could not be performed in the pandemic. Some participants stated that they could not perform the funeral and burial ritual: “…In my culture, when there is a funeral, the funeral house is always full. In other words, meals are prepared, neighbors bring food, the funeral house is supported. The loss-owners live their sadness. So that would be the case. However, in this process, no one could go anywhere.” “Nobody went to the burials anyway, neither relatives nor the others. Only their sons have participated in the burial. City officials have done the burial with protective clothing. There was no particular ceremony.” (
Some participants said that only close relatives were allowed to participate in these rituals: “They did the funeral prayer in the courtyard of the mosque without even taking him out of the hearse and took it to bury. And there was only us a few relatives, no one else” (
Some participants stated that they could not accept condolences because it was forbidden and because of the fear of getting infected: “Funeral houses are prohibited due to Covid. Even relatives and neighbors don’t want to come for condolences.” (
Participant views revealed the necessity of religious-cultural rituals which have a social support function: “Rituals are sometimes misunderstood. Sometimes that condolence house turns into a gossip house. It’s something I’ve always been against. However, it is needed somehow. It should be as it should have been. It’s like I can’t say goodbye. However, funeral ceremonies were necessary to live that process somehow. We don’t accept it at first because it’s painful, but when the ceremony is missed, we’re left unfinished; I think it’s troublesome.” (
In addition, some participants stated the following about the negative impact of the lack of rituals on the mourning process: “Before the pandemic, condolences are made when someone dies. Everyone comes to the funeral house; it gets very crowded. Everybody tries to console you. However, in this process, no one comes, and you are on your own. There are too many thoughts and regrets because we are left alone. In the normal process, we would mourn for a week or ten days, but in this process, we have been mourning for months.” (
Protective factors
The four subcategories of this main category were relative support (i.e., family, spouse, friend, partner), tele-support (i.e., mobile phone, internet, social media), positive coping strategies (cognitive, behavioral, and religious-spiritual), and delayed business.
Relative support (i.e., family, spouse, friend, partner)
In the non-COVID period, individuals who experience loss have a wide social support network through religious-cultural rituals such as funerals and condolences in Turkey
Tele-support (i.e., mobile phone, internet, social media)
Information and communication technology tools became one of the most important social support sources during the pandemic (Bar-Tur et al., 2021; Honey et al., 2021). Those failing to provide face-to-face support to the individuals who experience a loss started to support them via mobile phone, internet, and social media tools. Some participants stated that those who failed to provide face-to-face support provided support on the phone: “They called on the phone. So thank god, everyone, supported” (
Some participants stated that they received support via both phone and social media. “In general, the calls were done on the phone. Yasin recitation, juz recitation took place online and broadcasted through the online environment” (
Positive coping strategies (cognitive, behavioral, and religious-spiritual)
Coping skills contribute positively to the grief processes of individuals (Parkes & Prigerson, 2010). For example, individuals with an optimistic mindset tend to find a positive direction in their lives after lost loved ones (Kosminsky, 2016; Worden, 2018). The cognitive coping strategies of some participants who lost loved ones during the pandemic were as follows: “I realized that this is the normal flow of life. I realized that my negative emotions, succumbing to my sadness, my fears, and acting against the flow of life are the things that only hurt me” (
Reading and studying were prominent as positive behavioral coping strategies. For instance, one participant said: “I felt strong by keeping her alive, for example, by reading her books.” (
In addition, some participants’ states indicated that religious belief and spirituality are important coping strategy: “It is a very difficult process for us. This is a very serious illness. However, I have faith in Allah and the afterlife. Sometimes I think about it; if I don’t have faith, I don’t know what to do, I guess I’ll get mad.” (
Delayed business
Some participants’ experiences showed that they wanted to perform religious-cultural rituals that they could not do due to the pandemic-related restrictions after the pandemic. “We could not perform the prayers of seventh, fortieth, fifty-second days, recite mawlids, or host a meal, none of these. I did it myself at home, both the mawlid and Quran reading. I hope we will host a big meal for my father when the pandemic is over” (
Discussion
The current study explored the grief and mourning experience of the individuals who lost their loved ones due to coronavirus during the COVID-19 pandemic in Turkey. The findings of the study revealed that the pointed factors contributing to the grief and mourning process during the COVID-19 pandemic like cognitive, emotional, and behavioral responses of the individuals (i.e., grief and mourning responses); the expectation of harm, unfinished business, and restriction of death-related religious-cultural rituals (i.e., risk factors); and relative support, tele-support, positive coping strategies, and delayed business (i.e., protective factors) rise from sociological, psychological, environmental, cultural, and individual factors.
Regarding the grief and mourning responses of the participants after the loss, the most frequently observed emotional responses are sadness, helplessness, loneliness, and longing; cognitive responses include thoughts about the deceased (reminiscence), and behavioral responses. These are normal and natural responses that can be seen after a significant loss (James & Friedman, 2009). In general, we think that evaluating the reactions in the grieving process independently from each other will cause problems in making sense of what individuals experience. For example, although the behaviors experienced by PF6 are evaluated in a separate category as reactions, we cannot ignore the existence of emotional and cognitive responses that lead to the behavior. According to the cognitive model, our thoughts determine our behaviors (Beck, 1979); according to the emotion model, our feelings direct our behavior (Greenberg, 2015). For this reason, emotional, cognitive, and behavioral responses to loss interact with each other. Mourning responses are expected to decrease by expressing them through social support and religious rituals (Walsh, 2012). In the non-COVID-19 period, people who have lost their loved ones could share their pain (Walsh, 2012). When the participants’ answers are examined, we saw that the grief reactions were similar before the pandemic (Freeman, 2005; Gross, 2018; Worden, 2018). However, the rituals that allow people to share their pain after a loss are restricted, and people who have lost loved ones may even be deprived of the support of their neighbors, relatives, and friends (Hamid & Jahangir, 2020; Kokou-Kpolou et al., 2020; Wallace et al., 2020). In Turkey as a Muslim society, after someone’s death, neighborhoods, people who know the deceased or their relatives, and other members of the community attend the funeral and perform the burial together with İmam, the person who leads prayers in a mosque (Albayrak & Arıcı, 2007; Biçer, 2009; Ministry of Culture and Tourism, 2022). In addition, during the condolence phase that lasts for days, members of the society support people (i.e., wife, husband, father, mother, aunt, uncle) who lost a loved one (Bahar et al., 2012; Çelik & Sayıl, 2003; Ministry of Culture and Tourism, 2022). In other words, individuals who have lost their relatives share their burden of grief and mourning with the society. However, religious-cultural rituals such as funerals, burials, and condolences have been partially or entirely prohibited due to the risk of contamination in the COVID-19 pandemic in Turkey (Government of Turkey, 2021). The restriction of religious and cultural rituals related to death, an important source of social support, leads to feelings of loneliness and helplessness to be experienced. Therefore, the experience of these mourning-related emotions may increase the burden of mourning.
In addition, the findings revealed that restriction of death-related religious-cultural rituals, unfinished business, and expectation of harm were risk factors contributing to the grief and mourning process in the COVID-19 pandemic. The measures taken during the pandemic, such as social isolation and quarantine, cause individuals to perform their funeral ceremonies differently. Due to these measures, the participants who were not permitted to attend funeral ceremonies could not say goodbye to the loss and perform the religious rituals in the cemetery. Restricting funeral ceremonies, cemetery visits, and condolences due to the pandemic lead to the individuals experiencing the grieving process alone, preventing the mourners to accept their loss, and limiting face-to-face social support (Aguiar et al., 2020; eCondolence; 2020; Farahmandnia et al., 2020; Hamid & Jahangir, 2020; Omonisi, 2020). The lack of the religious-cultural rituals that mediate the sharing of the emotions with the member of the community leads to a more intense experience of the mourning process for the individuals who lost a loved one in Turkey, characterized as a collectivist culture. Unfinished business (Perls et al., 1951), another risk factor, is unresolved, unexpressed, or incomplete relationship issues with the deceased (Holland et al., 2014). One of the most important factors that enable individuals to overcome the grieving process is to complete the unfinished business in their relationship with the deceased and to be able to say ‘goodbye’ to the deceased (Worden, 2001). The restriction or prohibition of hospital visits due to the risk of contamination caused the participants not to have the opportunity to say goodbye to the deceased and not be with them. The individual who has a conflicted or unresolved relationship with the deceased in the past may experience feelings of guilt due to the unfinished business (Field & Horowitz, 1998; Holland et al., 2014, 2020; Klingspon et al., 2015) and accordingly, the mourning process may be prolonged. Another dimension of unfinished business is cultural factors. For example, at the funeral in Turkey, the relatives of the deceased see or hug the deceased to bid his/her farewell for the last time (Bahar et al., 2012; Ministry of Culture and Tourism, 2022; Tapucu & Aksoy, 2004). The relatives of the deceased wash their deceased relatives together with Gassal who washes the deceased in Gasilhane where the deceased is bathed (Başçetinçelik, 2001; Keskin, 2003). After the burial, İmam reads the Qur’an and prays at the graveside (Bahar et al., 2012; Biçer, 2009; Ministry of Culture and Tourism, 2022). In addition, the deceased is remembered on the 7th, 40th, and 52nd days of his death with a religious ceremony, known as Mawlid (Biçer, 2020; Bolçay, 2014). However, the prohibition of funeral, burial, and post-mortem rituals in Turkey (Government of Turkey, 2021) may lead to unfinished business related to religious-cultural rituals. Another factor that negatively affects the grieving process is the expectation of harm. The participants' statements revealed that the risk of contamination is an important risk factor in the grief and mourning process. Individuals in a collectivist culture interact more with family members and other members of society than with individualistic ones (Germani et al., 2020). The individuals may experience more fear and anxiety of contagion due to close relationships with family members, friends, or other community members. They may also experience fear and anxiety of infecting others (Van Bavel et al., 2020). Especially, in Turkey characterized by higher interaction and interdependence such as close relationships with family members, and other members of the community (Kağıtçıbaşı & Üskül, 2006; Kağıtçıbaşı et al., 2007) the individuals who lost their loved ones fear that they will be infected or will be infected their relatives by the virus. Also, they are worried about dying due to the virus or losing their loved ones again. These fears and worries which result from uncertainty about the spread of the virus may negatively affect the grief and mourning process. Based on all these, unfinished business, restricted death-related religious-cultural rituals, and expectation of harm which negatively affected individuals’ grief and mourning experiences, were considered as risk factors. Unresolved or unexpressed grief is more likely to develop complications and maladaptive reactions (Jordan & Litz, 2014; Prigerson et al., 2009; Zisook & Shear, 2009). Maladaptive grief has been named ‘complex and prolonged grief’ by researchers in recent years (Prigerson et al., 2009; Parkes & Prigerson, 2010; Shear, 2012). Personal characteristics of the survivor such as age and gender (Burke & Neimeyer, 2013; Parkes & Prigerson, 2010), the cause of death (Kübler-Ross & Kessler, 2005; Lobb et al., 2010), and cultural factors such as death-related rituals (Parkes et al., 1997) affect grief and mourning process. Psychological (e.g., unfinished business and expectation of harm) and cultural (e.g., restriction of death-related cultural rituals) risk factors during the pandemic period cause the individuals to experience the grieving process more intensely and may negatively impact the individuals' mental well-being. As a result of these risk factors, people who lost loved ones in the COVID-19 pandemic are at a higher risk of prolonged grief (Hamid & Jahangir, 2020; Zhai & Du, 2020).
Finally, the results indicated protective factors such as relative support (i.e., family, spouse, friend, partner), tele-support (i.e., mobile phone, internet, social media), positive coping strategies (cognitive, behavioral, and religious-spiritual), and delayed business. These findings were similar to the previous studies. The studies showed that factors that protect the complexity of grief are family support and social support (Feigelman et al., 2009; Hibberd et al., 2010; Kalantari et al., 1993; Nader & Salloum, 2011), use of pleasant activities, spiritual, problem-focused coping strategies, and palliative care (Mason et al., 2020; Parro-Jiménez et al., 2021). In addition, we found the importance of tele-support as a source of social support in the COVID-19 outbreak. One of the issues affecting participants’ mourning processes during the pandemic was the limitation in social support. Limited social support negatively affects individuals' well-being and mourning processes (Rando, 1993). In this context, it can be said that the lack of face-to-face social support affects individuals negatively. The literature has similar views (Aguiar et al., 2020; Farahmandnia et al., 2020; Hamid & Jahangir, 2020; Omonisi 2020). For example, Farahmandnia et al. (2020) mentioned the negative impact of the lack of family and friend support on mourners’ ability to cope with intense mourning and emotional exhaustion. As a result, they state that there will be a deep sense of sadness in society. However, the current study showed that individuals who lost their relatives received face-to-face support from their nuclear family, close friends, spouses, or partners. Moreover, as death-related religious-cultural rituals, an important source of social support, were not performed, individuals outside the immediate surroundings could not provide face-to-face support. However, they provided social support through tele-support (i.e., mobile phone, internet, social media). Therefore, although social support is limited, it cannot be said that this support does not exist at all. It can be said that these factors contributed positively to individuals’ mourning process. Apart from social support, the coping skills of the individual who has experienced the loss is another factor that contributed positively to the mourning processes (Parkes & Prigerson, 2010). Positive cognitive coping strategies are one of the factors that affect responses to the loss. Individuals with an optimistic mindset tend to find a positive direction in their lives after the loss, and this tendency is a facilitating factor in coping with loss (Kosminsky, 2016; Worden, 2018). In addition, in this study, reading books and studying were mentioned as positive behavioral coping strategies. Religious belief and spirituality, another coping style, provide an opportunity to attach a meaning to the experienced negative life events by providing a close relationship with divine power. They can take the individual’s attention from thoughts about their traumatic life and direct it to a positive and protective belief.
Another factor that contributes to the experience of mourning is the “delayed business,” which is put forward as a new concept. It is understood that the participants planned to do the religious and cultural rituals, which they wanted to do but could not do, in the future. Therefore, delayed business seems to contribute to the participants' feeling good. More clearly, the concept can be explained as the desire to perform the behavior that could not be performed for any reason at an appropriate time in the future. So, it can be said that an individual with delayed business is more hopeful than an individual with unfinished business. More clearly, negative emotions prevail in unfinished business (Perls et al., 1951); positive emotions dominate delayed business. It should be noted that the task postponed to a later time should be relatively predictable and feasible. Setting an unattainable goal may cause the individuals to feel hopeless and to blame themselves. New studies may examine the operational definition of the “delayed business” concept and its relationship with other variables. Thus, it could shed light on prevention and intervention studies on the concept of delayed business, which we think is associated with positive emotions. The concept of delayed business can be confused with planning for the future, which is a method of coping with difficult situations. However, by the concept of delayed business, we do not mean just making plans. We suggest a process that involves making plans and looking to the future with hope. In addition, the delayed business suggests performing a behavior that cannot be done for any reason; In planning, a situation does not need to be done. While planning a phenomenon or behavior is not intended to be done now but, in the future, planning to be done now and planned to be done in the future expresses the concept of delayed business.
Implications and future studies
The findings of this study allow us to make some suggestions. First, the opportunity to video chat with their relatives should be offered to individuals before the loss. In this way, the meeting that cannot be done face-to-face can be done online. Another suggestion is organizing a remote attendance at the funeral for deceased relatives while the officials hold the ceremony. For example, online participation of the deceased relatives can be organized while religious officials perform final duties during the burial. Third, after the pandemic is over, a public funeral can be held throughout the country for individuals who lost their relatives. In this way, it can be ensured that the unfinished work of individuals is completed. Fourth, psychosocial support services can be provided for individuals who cannot experience a normal mourning process. Since social support is particularly prominent in these studies, various services should be planned to increase individuals’ social support sources. In this context, the use of technological tools can be effective. Finally, studies involving the concept of delayed business should be conducted, and individuals' roles under challenging processes should be investigated.
Limitations and strengths
Although this study provides important information on how COVID-19 changed the mourning process and the risk and protective factors after loss, it has limitations. First, this study was conducted with a small sample, limiting the generalizability of the results to a wider population. Second, this study was conducted on Muslim society in Turkey. Studies with people from other religious communities should be conducted to obtain different responses and experiences. Third, due to the risk of infection, the interviews were conducted online, so there are worries about missing the participants' facial expressions and difficulties in establishing relationships. Finally, the deceased’s ages were between 53 and 82. People’s mourning responses and the effects of the loss may be different when a young person dies. Comprehensive studies can be conducted with individuals who lost their relatives at a younger age. On the other hand, people of different education levels, ages, and genders, living in rural and urban areas were included in this study. This diversity makes an important contribution to the generalizability of the study findings.
Conclusion
The current study’s findings allowed us to reveal the risk and protective factors for the individuals who experienced a loss due to COVID-19 during the pandemic. In addition, it allowed us to see the most frequently observed emotional, cognitive, and behavioral responses to loss. Finally, it also plays a mediator role in making recommendations to policymakers and mental health professionals to provide psychological support services to individuals who have lost loved ones due to COVID-19.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Appendix
The semi-structured interview form
Gender
Age
Education level
SES
Region
How long ago he/she lost her relative
Cause of death
Gender deceased
Age deceased
Degree of relative deceased
1. How do you feel right now because of the loss of loved one?
2. How did your loss during the pandemic affect you?
3. From whom did you receive social support during morning process?
4. How are funerals held in your culture? How did you do the funeral during the epidemic? What did you feel?
5. How was your relative’s burial done during the epidemic? How did you feel during?
6. How did you accept condolences during the epidemic? And how did you feel?
7. Did you perform other rituals (grave visit, 7th, 40th, and 52nd day, mawlid recital etc.) during the epidemic?
a. If yes
i. How did you do it?
ii. How did you feel?
b. If no
i. How did you feel?
8. How did it affect you that you could not perform the religious-cultural rituals and spend the grief process with your nuclear family?
9. Is there anything else you would like to add?