
Abstract
Using the concepts of medical tourism and travel medicine, this research note proposes healthcare sector development has a positive impact on inbound tourism. This hypothesis is tested with the data of ASEAN countries from 2000 to 2018. Because of the presence of cross-section dependence and heterogeneity, appropriate panel cointegration test, panel coefficient estimation method and panel Granger causality test are used. The findings indicate that (1) evidence of cointegration between inbound tourism and healthcare sector development is found when inbound tourism is the dependent variable and (2) there is a Granger causality from healthcare sector development to inbound tourism. The findings suggest that there are temporal relationships from healthcare sector development to inbound tourism in both short-run and long-run. In summary, healthcare sector development has an impact on inbound tourism.
Keywords
Introduction
Medical tourism is a subset of inbound tourism where travellers move across borders to seek medical care (Ormond and Sulianti, 2017). Adequate medical infrastructure and facilities and large stock of highly trained doctors and nurses are two of the main reasons a country becomes the choice of destination for medical travellers (Ormond and Sulianti, 2017).
Occasionally, travellers are dealing with illness or injury during and/or post travel (Page, 2009). The increasing recognition given to travellers’ health and safety issues leads to the development of travel medicine (Page, 2009). From travel medicine perspective, the risk assessment and prevention at the pre-travel phase, and the travellers’ experience in managing and handling injury or illness during travel phase are dependent on the availability of medical infrastructure and facilities, nurses and doctors at destinations. The travellers, who are risk averse, adopt risk reduction strategies, which lead to the avoidance of destinations that are lack of medical infrastructure and facilities, and highly trained doctors and nurses (Page, 2009; Wang et al., 2019).
In summary, uncompromised medical services have a positive impact on inbound tourism from the perspective of medical tourism and travel medicine. Quality medical services depend on the development of healthcare sector. Positive healthcare sector development increases the number of highly trained doctors and nurses, and the adequacy and quality of medical infrastructure and facilities. These linkages are summarised in Figure 1. Therefore, this research note hypothesises that Influence of healthcare sector development on inbound tourism.
H1. Healthcare sector development has a positive impact on inbound tourism.
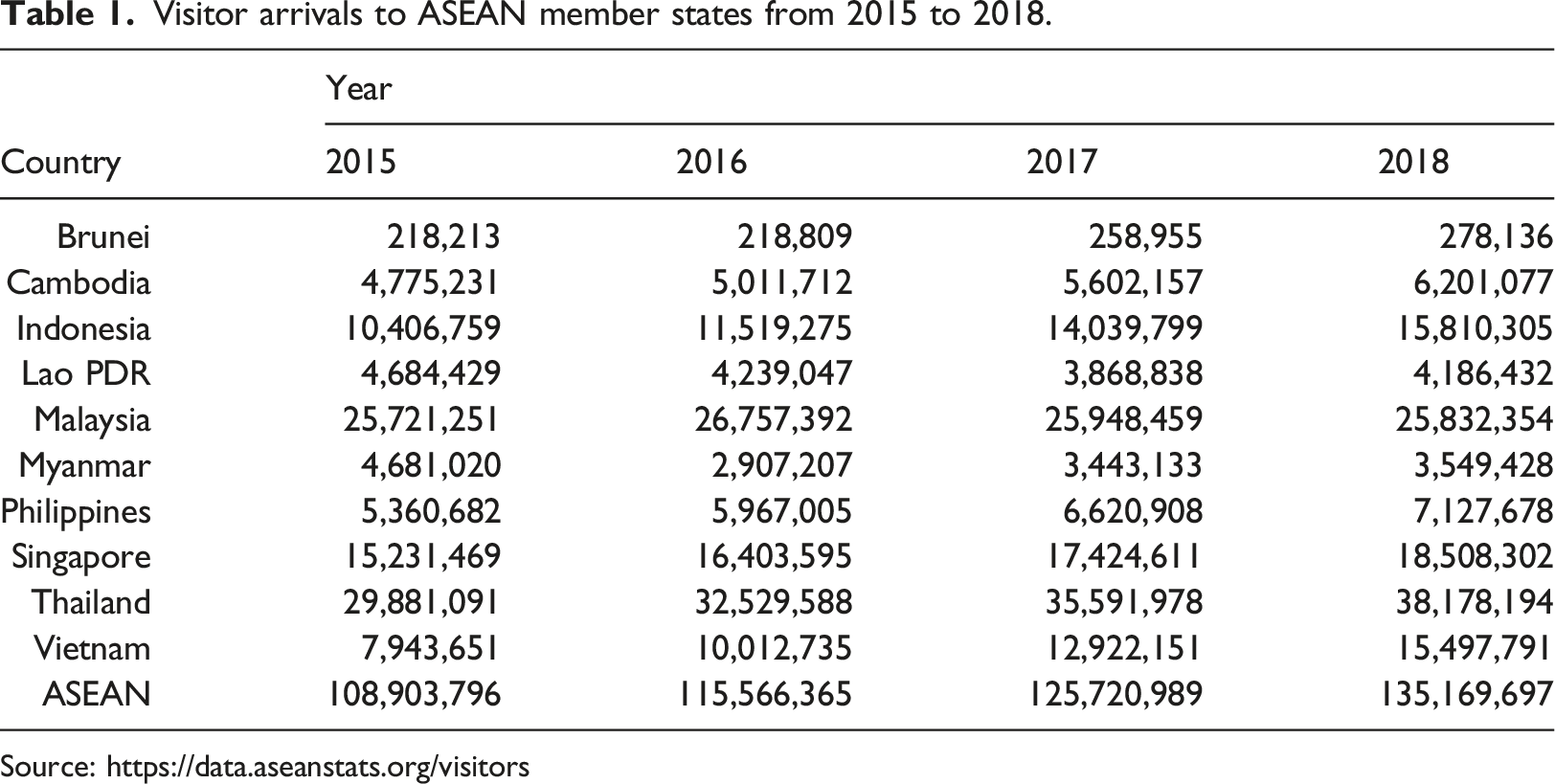
Visitor arrivals to ASEAN member states from 2015 to 2018.
Contribution of visitor arrivals of each ASEAN member state to the region from 2015 to 2018.
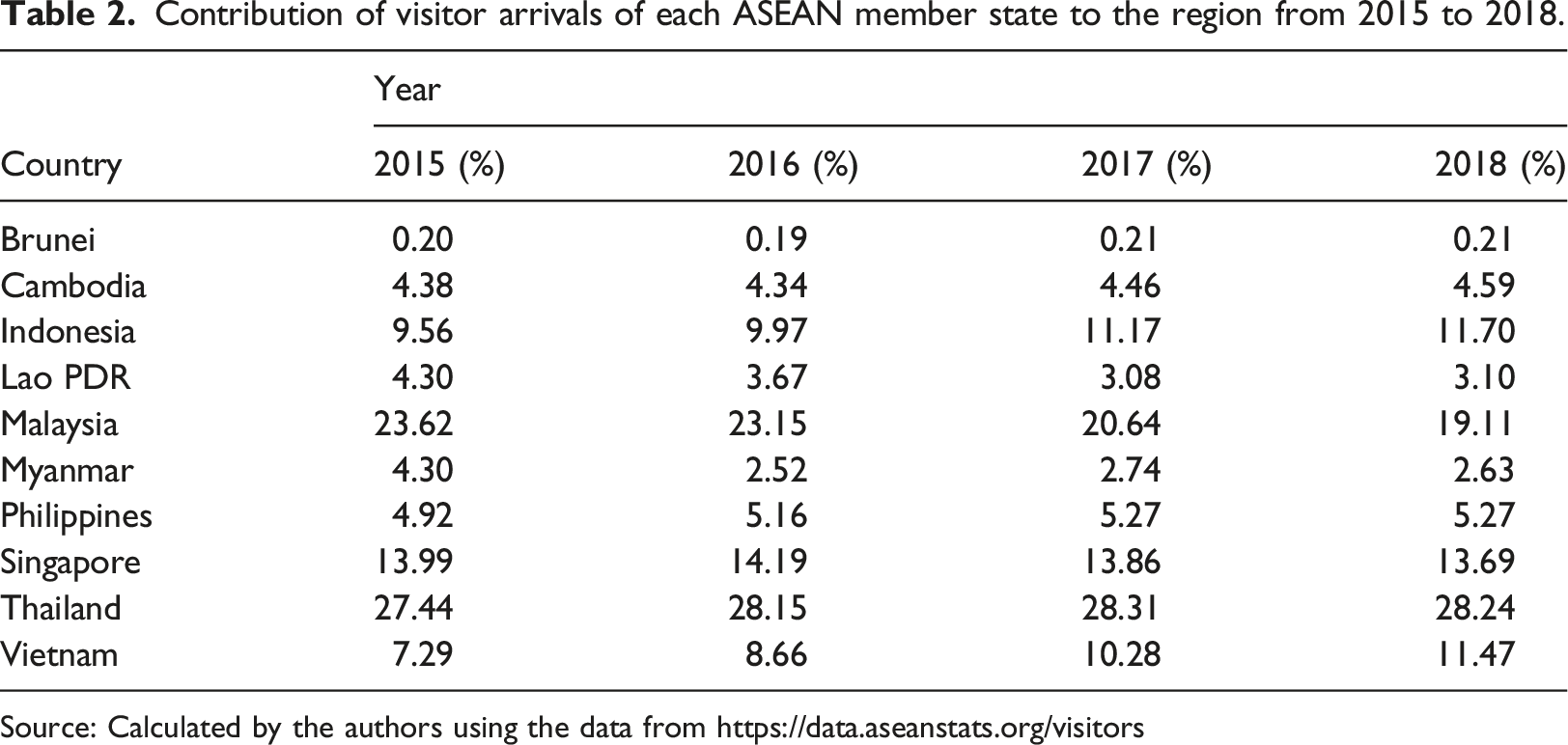
Source: Calculated by the authors using the data from https://data.aseanstats.org/visitors
Brief literature review
Many conceptual papers in medical tourism have been written. They focus mainly on identifying the factors that lead to the development of the medical tourism industry (see Enderwick and Nagar, 2011; Kamassi et al., 2020; Vovk et al., 2021; Zarei and Maleki, 2019). Li et al. (2022) indicate some of these papers are marketing-oriented. Empirical studies focussing on the impact of healthcare sector development on inbound tourism are scarce. Limited to our knowledge, there are only two studies, Lee (2010) and Lee and Hung (2010), that use time series econometric techniques to analyse the dynamic interactions between healthcare sector development and inbound tourism. However, these studies produce mixed results.
Lee (2010) and Lee and Hung (2010) study such linkages using the data of Singapore. Lee (2010) uses number of doctors per 10,000 population, whereas Lee and Hung (2010) uses government expenditure on health per capita as the proxy for healthcare sector development. Both use total tourist arrivals as the proxy for inbound tourism. Lee (2010) finds healthcare sector development and inbound tourism are cointegrated, and healthcare sector development has a positive effect on inbound tourism. Also, evidence of short-run Granger causality cannot be found between these two variables. Lee and Hung (2010) are unable to find a cointegrating relationship between healthcare sector development, inbound tourism and economic growth when inbound tourism is the dependent variable, but shows a short-run Granger causality from healthcare sector development to inbound tourism.
Data, methodology and results
Annual data on per capita tourism revenue (TR) and per capita health expenditure (HE) are collected from World Tourism Organization (Yearbook of Tourism Statistics, Compendium of Tourism Statistics and Data Files) and World Health Organization Global Health Expenditure database (http://apps.who.int/nha/database), respectively, over the period 2000–2018 for ASEAN countries.
HE is the proxy for healthcare sector development because it is prepared by the World Health Organisation under the framework of the System Health Accounts 2011, which traces all health spending of a given country that can be used for evidence-based policy making. Furthermore, the data are comparable across countries and time. Different measures of inbound tourism have been used, where the number of tourist arrivals has been used by most of existing studies (Wang and Davidson, 2010). Wang and Davidson (2010) state that economic impacts are TR driven and TR is monitored by policymakers and businesses. Therefore, this study uses per capita TR as the proxy for inbound tourism so that normalization is carried out for the comparability of the proxies for healthcare sector development and inbound tourism. Both are measured in current USD.
To examine the impact of healthcare sector development on inbound tourism in the long run, the equation below is estimated:
Results of cross-section dependence and slope homogeneity tests.
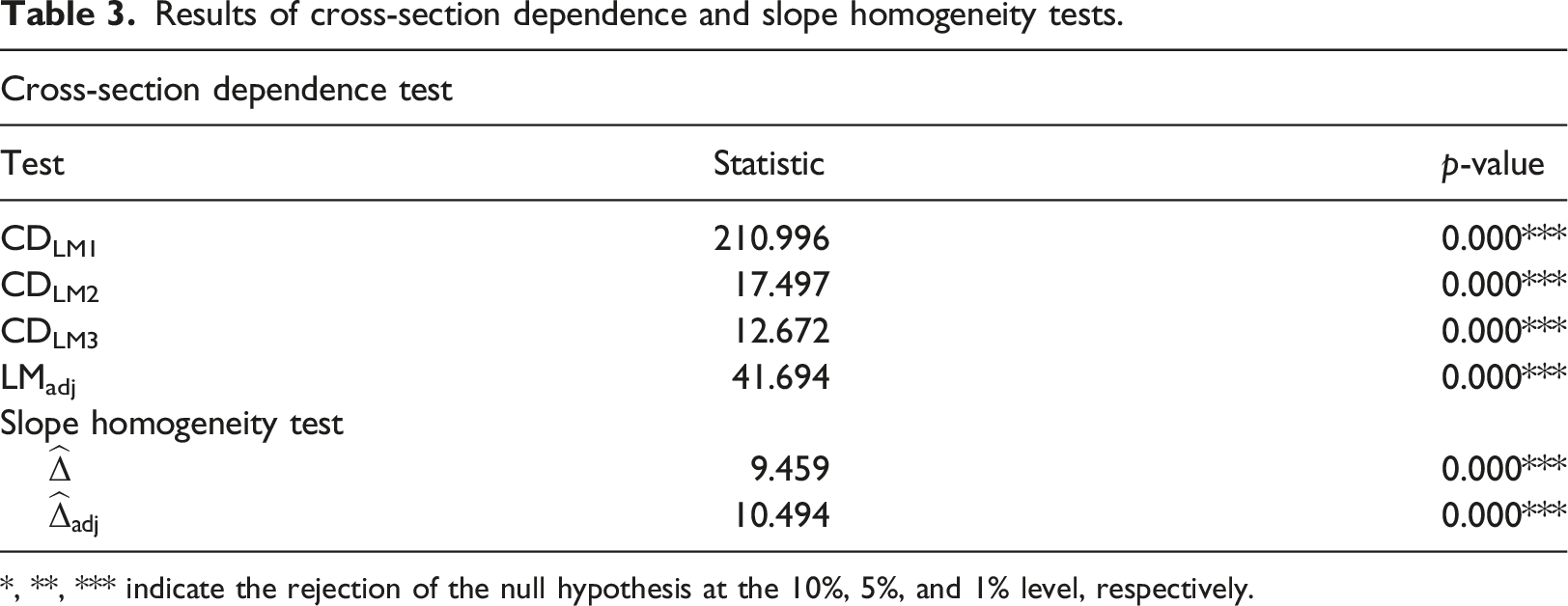
*, **, *** indicate the rejection of the null hypothesis at the 10%, 5%, and 1% level, respectively.
Results of panel cointegration tests.
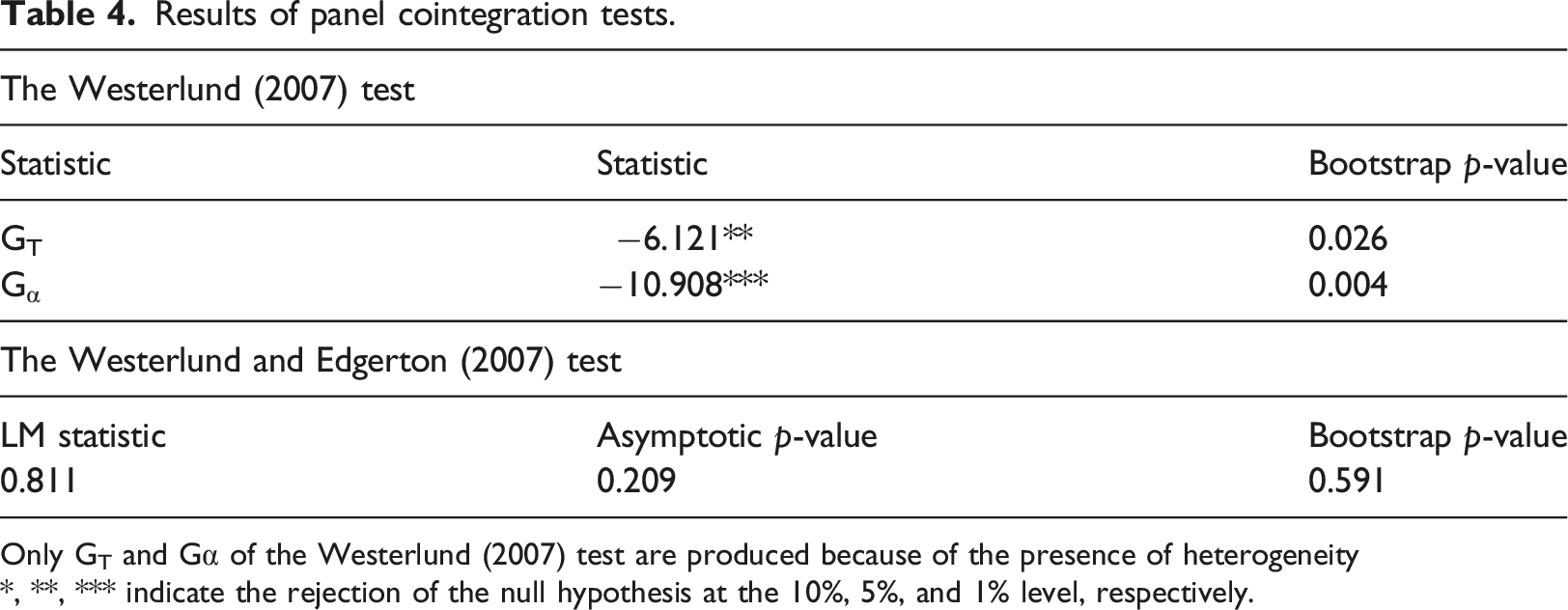
Only GT and Gα of the Westerlund (2007) test are produced because of the presence of heterogeneity
*, **, *** indicate the rejection of the null hypothesis at the 10%, 5%, and 1% level, respectively.
Results of AMG long-run cointegrating coefficients.

Values in parentheses are p-values
*, **, *** indicate the rejection of the null hypothesis at the 10%, 5%, and 1% level, respectively.
Results of Emirmahmutoglu and Kose (2011) panel Granger causality test.
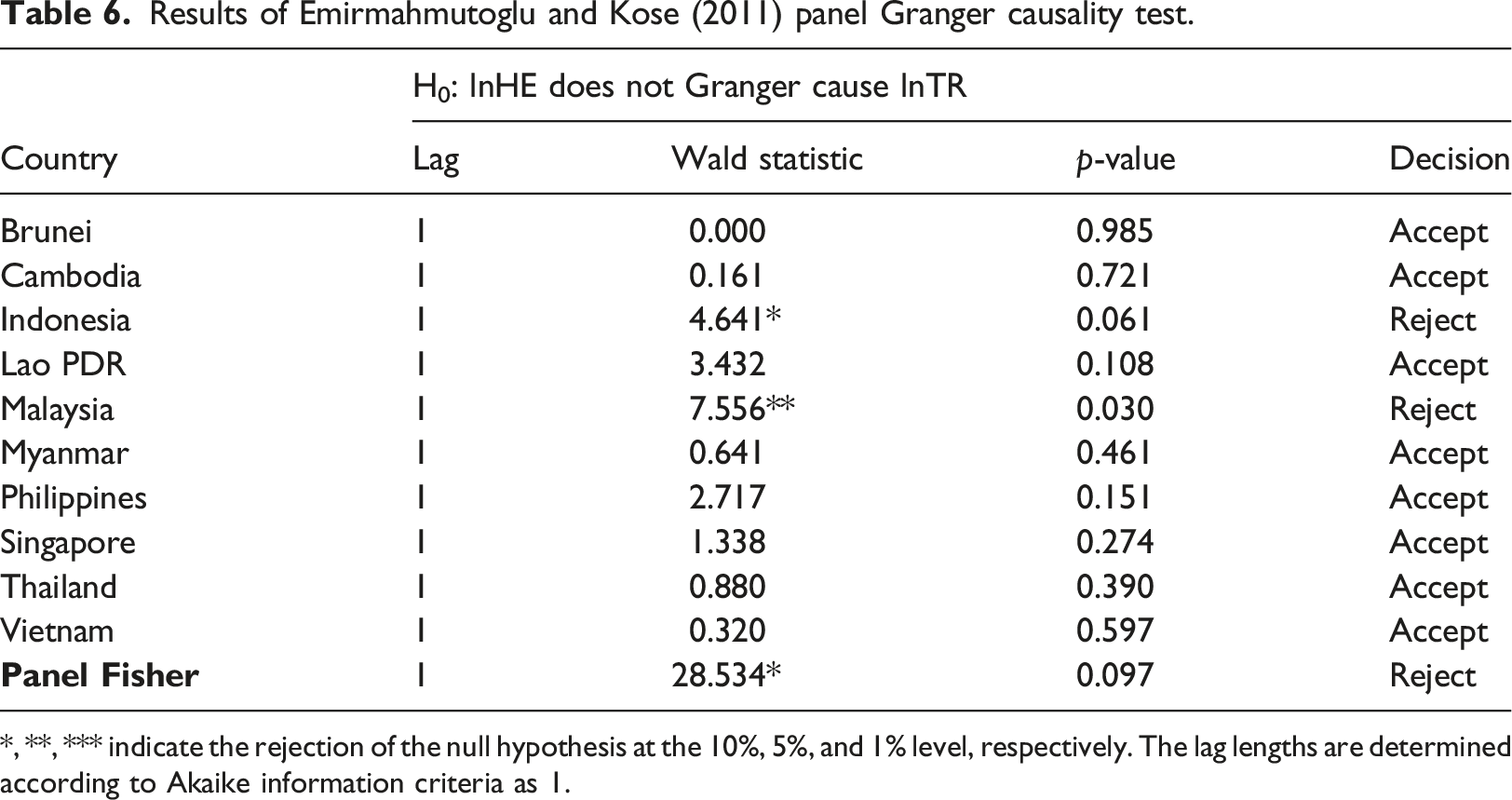
*, **, *** indicate the rejection of the null hypothesis at the 10%, 5%, and 1% level, respectively. The lag lengths are determined according to Akaike information criteria as 1.
Conclusion
This research note aims to understand whether healthcare sector development has a positive impact on inbound tourism in the context of ASEAN. From panel perspective, there exists a long-run (cointegrating) relationship between healthcare sector development and inbound tourism when inbound tourism is the dependent variable, and a Granger causality from healthcare sector development to inbound tourism. Based on the empirical findings of this research note, policymakers should allocate sufficient financial resources to enhance medical services if destinations intend to expand their tourism industry. The findings of this study will still be relevant when COVID-19 becomes an endemic because the availability of quality medical services influences the image of countries as tourism destinations.
This study is with a limitation because it uses a bivariate model to deal with small sample size constraint. Such bivariate model may lead to the omission of important variables (Brida et al., 2016). There is a risk of getting biased results. However, Lutkepohl (2007) states that a simplified model, which is justified by the theoretical foundation, is more likely to provide interesting findings than a more complex model under small sample size constraint. Furthermore, Lee (2021) emphasises that in practice it is difficult to decide which other variables to be added into the model. Therefore, the addition of new variables may affect the findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.