
Abstract
Objectives
To analyse the current and potential utilization of generic drugs in Japan, to examine the maximum possible cost savings from generic drug use and to develop a fairer measure to assess the level of generic drug substitution.
Methods
We conducted a cross-sectional retrospective analysis of nine million dispensing records during January to March 2010 in Kyoto Prefecture. Maximum potential quantity-based shares were defined as the quantity of generic drugs used plus the quantity of branded drugs that could have been replaced by generic drugs divided by the quantity of all drugs dispensed. We developed a ‘substitution index’, defined as the proportion of generic drugs out of the total drugs substitutable with generic drugs (based on quantity rather than cost).
Results
Generic drugs had a quantity-based share of 17.9%, a cost-based share of 8.9% and a maximum potential quantity-based share of 50.1%, which is lower than the actual generic drug shares of some other countries. The maximum possible cost savings as a result of generic drug substitution was 16.5%. We also observed wide variations in maximum potential quantity-based shares between health care sectors and health care institutions.
Conclusions
Simple comparisons based on quantity-based shares may misrepresent the actual generic drug use. A substitution index that takes into account the maximum potential quantity-based share of generic drugs as a fairer measure may promote more realistic goals and encourage generic drug usage.
Introduction
In response to a global trend of rising health care costs, the increased use of generic drugs is one mechanism to reduce financial burdens on patients, payers and health care systems.1–4 However, Japan has reported lower generic drug utilization compared to Europe and the US. 5 The total health care costs in Japan in 2009 were approximately 36 trillion yen (US$323 billion) and drug costs in 2010 made up 24% at 8.7 trillion yen (US$78 billion). 6 In 2007, the Japanese Cabinet Office's Council on Economic and Fiscal Policy set a target for the quantity-based share of generic drugs (the proportion of drugs prescribed that are generic, as regards the quantity of drugs) to double to 30% by 2012. 7
To achieve this, financial incentives were implemented. Until March 2010, community pharmacies had been awarded an additional payment if the proportion of generic drugs dispensed was over a stipulated proportion. In contrast, hospitals decide in advance what drugs to provide for inpatients. Therefore, the choice between generic and branded drugs is made at the organizational level and is beyond the influence of individual pharmacists. However, a pharmacist dispensing for outpatients may substitute generic drugs for branded drugs unless a doctor stipulated no substitution. The maximum potential generic drug use at both national and institutional levels has yet to be determined. Depending on hospital type and clinical speciality, the maximum proportion of generic drugs that could be used by a provider may be drastically different to other providers. Therefore, decisions to award or withhold financial incentives to individual institutions based on common targets are inherently unfair.
Although the approximate cost savings from generic drugs has been suggested by the government, 8 accurate estimates need to be based on unit costs and utilization. 9 Computerization of claims to medical insurance systems means that a comprehensive database is available for such estimates to be made.
Our objectives were to examine recent generic drug use in Japan, to reveal the maximum potential use of generic drugs, to simulate possible cost reduction from generic drug use within different health care sectors, and to develop a fair assessment measure of generic drug use. This study is limited to prescription drugs and does not include those bought over-the-counter.
Methods
Data source
We used a cross-sectional analysis of dispensing records from insurance claims submitted to the National Health Insurance (NHI) and Long Life Medical Care 10 systems between January and March 2010 by health care providers in Kyoto Prefecture. This database includes 9,111,618 dispensing records from 169 inpatient facilities, 1105 outpatient facilities and 747 community pharmacies. Japanese hospitals are reimbursed using either a fee-for-service or flat-sum system. The latter refers to the Diagnosis Procedure Combination/Per-Diem Payment System (DPC/PDPS), which was introduced in 2003. Providers are required to report the actual utilization of each item, which we used to calculate the amount of drug use.
Analyses were conducted for three health care sectors: outpatients in clinics and hospitals; inpatients; and community pharmacies. Institutions which dispensed fewer than 100 units per month were excluded.
Quantity and cost of drugs
We calculated the usage of all drugs, both generic and branded, and the cost according to the Japanese NHI Drug Price Standard list in use in 2010. Costs were calculated in Japanese yen and converted to US dollars using the purchasing power parity rate in 2010 (JPY111.39 = US$1).
Identification of branded and generic drugs and substitutability for generic drugs
Branded and generic drugs were priced according to the NHI Drug Price Standard list. Generic drug substitutability was determined using the drug codes provided on that list. Each drug has a unique 12-digit code, which has a categorization function: the first two digits designate each drug's therapeutic purpose, and the following seven digits indicate its chemical composition, formulation and dosage.11,12 The final three digits indicate the brand of each drug. Branded drugs and their corresponding generic alternatives were matched using the first nine digits. The list included 19,355 drugs that could be categorized as branded drugs with no generic equivalent (n = 9304), branded drugs substitutable with generic drugs (n = 1782) and generic drugs (n = 8269). Simulation analysis was conducted using the 1782 branded drugs substitutable with generic drugs. Quantity-based share was defined as the proportion of the quantity of all drugs presented that were generic and cost-based share was the same but according to the cost of drugs.
Measures of drug use
Maximum potential quantity-based share was calculated as:

We also conducted a simulation analysis of possible drug cost reduction as a result of maximum generic drug substitution. For branded drugs with multiple equivalent substitutable generic drugs at different prices, we used the mean prices of the generic drugs to reflect possible cost reduction. The lowest and highest prices were used to provide a sensitivity analysis.
To demonstrate the degree of generic drug usage, we created a substitution index, which ranged from 0 to 1 and was defined as:

This can also be expressed as:

Results
Quantity and costs of dispensed drugs and generic drugs in Kyoto Prefecture (January–March 2010).

Note: Costs were calculated in Japanese yen and converted to US dollars using the purchasing power parity rate in 2010 (US$1 = JPY111.39).
Figure 1 shows the quantities and utilization rates of branded drugs with no generic equivalent, substitutable drugs and generic drug use across all therapeutic categories as defined by the Japanese Ministry of Internal Affairs and Communications.
12
The quantities and substitutability of drugs dispensed differed widely between therapeutic categories. Cardiovascular medications, including antihypertensive and antihyperlipidemic agents, were the second largest in quantity dispensed and had the largest potential quantity for substitutability with generic drugs.
Quantities of drugs dispensed and utilization rates by therapeutic categories: branded drugs with no generic equivalent, substitutable drugs and generic drugs.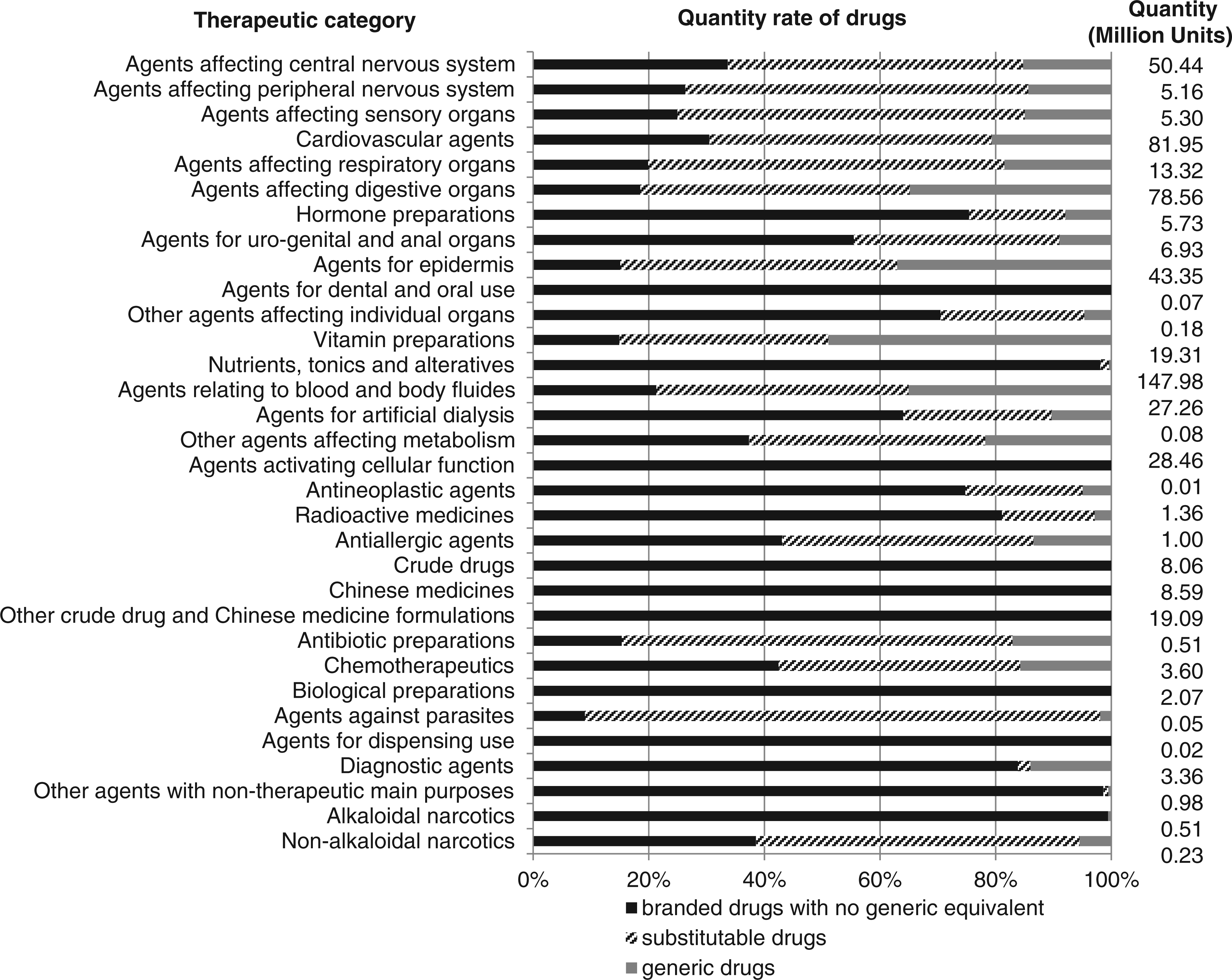
Possible cost reduction as a result of generic drug substitution for outpatients, inpatients and pharmacies was estimated to be 15.4% inter price-dependent range: 12.1%–17.5%), 9.4% (8.0%–10.2%) and 19.6% (15.3%–22.5%), respectively. Total drug cost reduction was estimated to be 16.5% (13.0%–18.8%) under maximum substitution conditions, equivalent to US$37 million.
Quantity-based share, maximum potential quantity-based share and substitution index of generic drugs for individual health care institutions.
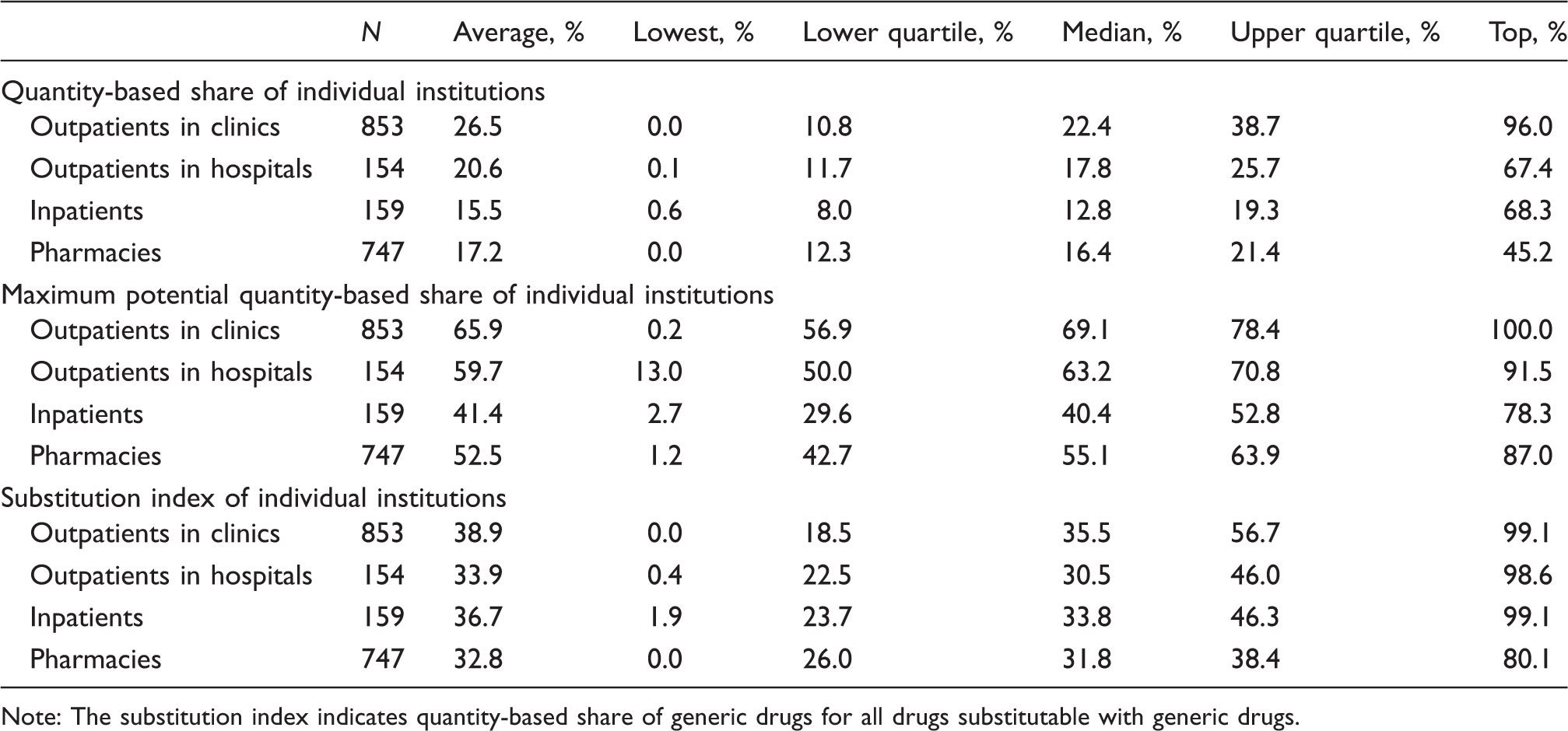
Note: The substitution index indicates quantity-based share of generic drugs for all drugs substitutable with generic drugs.
Figure 2 shows the quantity-based share of generic drug use and the substitution index of each health care institution. There were wide variations in the substitution index among institutions that scored near the quantity-based share; 40% (75 out of 187) that were in the lowest quartile according to their quantity-based share were in the top two quartiles according to their substitution index.
Quantity-based shares of generic drugs used and the substitution indices of individual health care institutions within the outpatient, inpatient and pharmacy health care sectors.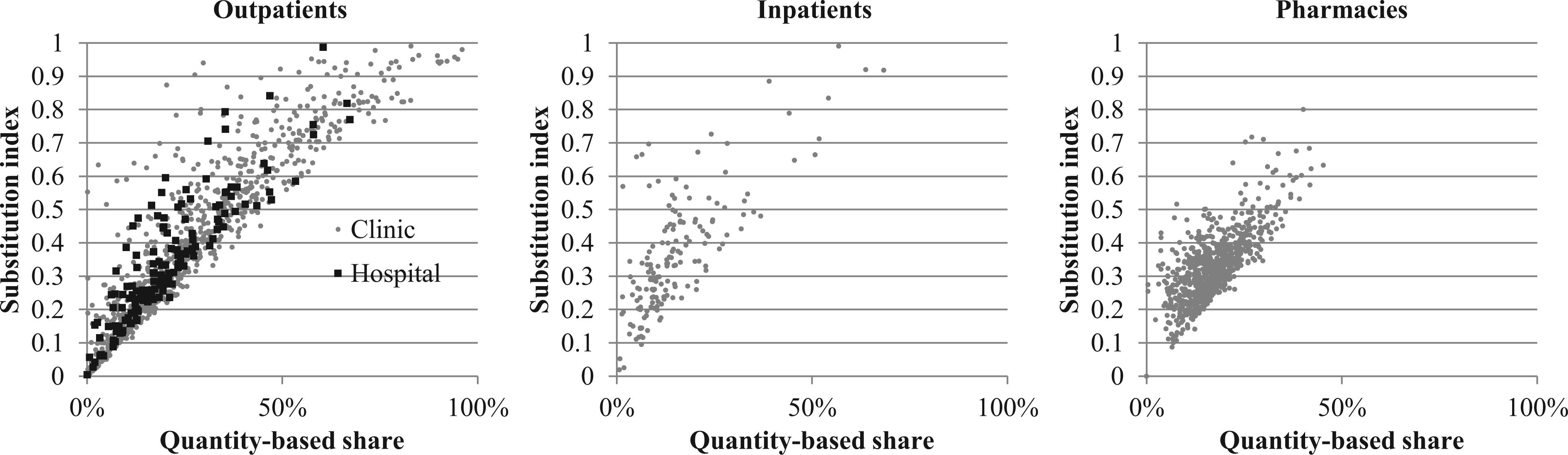
Discussion
Main findings
Generic drug quantity-based share was 17.9%, similar to that reported by the Japanese government. 13 The maximum potential quantity-based share of generic drugs was 50.1%, suggesting that generic drugs are used in only 36% (17.9% out of 50.1%) of potential opportunities. In addition, the maximum potential quantity-based share in Japan is lower than the generic drug quantity-based share in the UK (53%) and the US (55%). 5 This might be explained by the rapid diffusion of new drugs in Japan 4 which means that the number and quantity of new drugs that are not substitutable with generic drugs is high. Although the Japanese government has constructed macroeconomic policies that take these figures into account, 5 simple comparisons or target setting may be irrelevant. In other words, assessments based on quantity-based shares may misrepresent the situation.
Implications
The different maximum potential quantity-based shares across institutions are likely due to differences in the proportions of the types of drugs that are dispensed in each institution rather than on differential efforts of institutions to use generic drugs. As Japanese pharmacies currently receive financial incentives based on their quantity-based shares, these results suggest that the current incentives use an intrinsically unfair goal.
The substitution index proposed assesses the use of generic drugs in the context of substitutability, thereby reflecting their maximum potential quantity-based share. Institutions with similar quantity-based shares can score very differently when using the substitution index, and vice versa. Therefore, evaluations by the quantity-based share may undervalue individual institution efforts, as well as present a relatively weak incentive as some institutions can achieve high values without much effort if they have a high maximum potential. In contrast, institutions with low potential substitutability may not find it advantageous or even possible to increase the quantity of generic drugs dispensed in order to benefit from financial incentives. The substitution index may represent a fairer and feasible alternative to the present incentive-linked measurement to encourage generic drug use. The results of future analyses may change if doctors change prescriptions from unsubstitutable drugs to those substitutable for generic drugs, or if generic drugs become available for currently unsubstitutable ones. However, the index proposed here can still be applied, with modifications to the denominator, to reflect any drug switching.
An important contribution of this study is the analysis at the individual sector and health care institution levels. Previous reports have been mainly based on aggregated data, and arguments and incentives have therefore been geared towards aggregated data scores. However, the recent shift to electronic databases for health care claims data in Japan has allowed more detailed analyses and enables the development of better indices for monitoring drug utilization and related costs; fairer criteria can also be determined for the evaluation of future incentives aimed at encouraging generic drug use. Not only must new incentives be considered carefully before implementation but current incentives must be evaluated for potential replacement.14–16 As concerns remain about the efficacy of generic drugs,17–20 this study does not address how large the share of generic drug utilization should be. Instead, we propose a fairer indicator to monitor generic drug use at the health care institution level.
Limitations
Our results should be interpreted with some caution due to potential bias from the data source. First, the data covered only three months, and so did not take into account the seasonal variation in use. Second, the data were based on a single prefecture though generic drug use has been shown to be similar across prefectures. 13 The insurers providing the data cover more than 70% of all public insurance benefits. 21 A national database, which the Japanese government is currently developing, may allow analyses of all prefectures in the future. Another possible limitation is that drug prices are regulated by the government and cost shares may change over time even if quantity shares remain unchanged.
Footnotes
Conclusions
Generic drug usage in Japan remains low despite government efforts. Simple comparisons based on quantity-based shares may misrepresent generic drug use. Wide variations in maximum potential quantity-based shares between health care sectors and health care institutions due to differences in substitutability suggest that a substitution index, that takes into account the maximum potential quantity-based share, is a fairer assessment measure that can promote more realistic goals and more effectively encourage generic drug usage.
Funding
This work was supported in part by a Health Sciences Research Grant from the Ministry of Health, Labour and Welfare of Japan, and a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.