
Abstract
Objectives
To identify the management populations of acute hospitals, and to consider how the composition of this critical but criticized group affects managerial capacity.
Methods
A multi-method study of six acute trusts, involving 1200 managers in setup interviews, focus groups and a survey. Interviews with senior managers identified the key middle management groups in their trusts. The workforce information offices at two trusts estimated the management numbers from their databases. The findings were compared with the NHS Information Centre data on the number of ‘managers and senior managers’ across the service.
Results
The management population of an acute trust includes ‘pure plays’, whose roles are mainly managerial, and ‘hybrids’, whose roles combine managerial and clinical duties. Together, pure plays and hybrids comprise around 30% of staff in an acute trust, and even this may be an underestimate. Hybrid managers typically outnumber pure plays by four to one. NHS Information Centre data indicate that only 3% of all NHS employees are ‘managers and senior managers’.
Conclusions
In a climate of cost reductions and radical change, acute trusts have challenging management agendas. Policy to ‘cut management’, if focused on pure plays, increases the managerial burden on hybrids, diluting their clinical focus, and potentially jeopardizing the change agenda along with quality and safety of patient care. To strengthen management capacity, acute trust leadership and management development programmes must target the full ‘hybrids and pure plays’ population, and particularly hybrids who comprise the majority.
Introduction
‘We want to turn this into a great organization, a great place to work. We need to engage people or lose talent, especially in general management roles. Retaining talent in management roles is going to be a problem. They could just walk away to other sectors’. (Director of Human Resources, Greenhill Hospital)
There is a widespread perception that the National Health System (NHS) in England is over-managed by ‘pen pushers’ and ‘grey suits’.1–3 Managers have thus been a popular target for politicians, especially following the general election in May 2010.4,5 Despite the negative stereotype, research in health care and other sectors emphasizes the valuable contributions of middle managers, mediating between front line and top team, implementing change, and maintaining day-to-day operations.6,7 This management agenda, for acute hospital trusts, is multifaceted and complex, especially in the context of achieving £20 billion in efficiency savings by 2015, while improving quality of care and patient safety, as demand for health care is rising.
Middle managers play key roles in implementing national policy and in achieving desired outcomes but their profile in health care is not well understood. In particular, the recent focus on management numbers has diverted attention from the question of whether or not provider organizations, such as acute hospitals, have the management capacity to implement mandated changes and improvements.
Middle managers are an elusive group, 8 defined by one leading commentator as ‘any managers two levels below the CEO and one level above line workers and professionals’. 9 An appropriate working definition thus includes anyone from ward sister to clinical director (division head) whose role includes a managerial component. It is necessary to distinguish between ‘pure plays’, whose roles are wholly managerial, and ‘hybrids’, whose roles combine clinical and managerial responsibilities. ‘Managerial responsibilities’ include planning, organizing, supervising, directing, coordinating, reporting, budgeting (‘POSDCoRB’), service improvement and human resource management (but not necessarily line responsibility for other staff). The concept of hybrids is not new, dating from developments in the late 1980s following the recommendations of the Griffiths Report on NHS management. 10 Attention has focused mainly on consultants (senior doctors) holding key service management roles as clinical directors.11,12 The management components of other hybrids have attracted less attention.
Methods
This article draws selectively from a study of middle managers in six acute hospitals (‘Burnside’, ‘Clearview’, ‘Greenhill’, ‘Netherby’, ‘South Netley’ and ‘Wattle Park’) in England between 2009 and 2012. Information was gathered from trust websites, 93 management interviews, 40 focus groups and a management survey with 600 responses. Interviews and focus groups generated qualitative information concerning the nature of managerial roles: pressures, motives, contributions to clinical and organizational outcomes, and how roles were changing. A Likert-scaled management survey with around 90 items was administered online at five trusts, with a response rate of 24%. The full details of the methodology (data collection and analysis) have been reported elsewhere. 13
At the beginning of this study, senior managers at each hospital were asked, ‘who would you include in the middle management population of your trust?’ Responses included hybrid roles (medical director, clinical director, lead nurse, midwifery manager, modern matron, ward sister, specialty lead, laboratory team leader) as well as pure plays (deputy/assistant director, general manager, department head). Using an organization’s own definition of middle management is a strategy advocated by other researchers, 14 and was deployed here to refine the working definition cited earlier.
Results
Official data on numbers of managers
NHS employment in England.
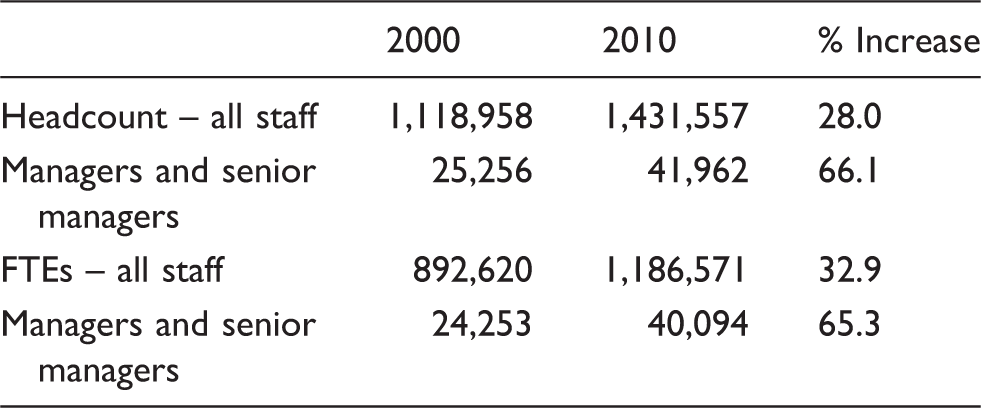
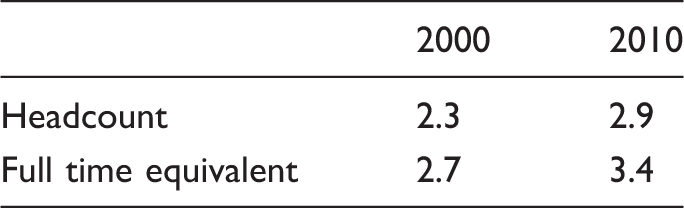
Managers and senior managers as proportion of total NHS employment.
It is, however, appropriate to explain the absolute increase in management numbers since 1999. Part of this explanation lies with the 30% increase in the number of other staff, who in turn generate a managerial workload: recruitment, selection, coaching, mentoring, training, supervision, appraisal, discipline, development. The increase was also likely to have arisen due to many other additions to the management agenda. 15
Other researchers, using Binley's Database of NHS Management, reach similar conclusions. While gathered for commercial purposes, with different inclusion criteria, Binley’s data have been compiled in a consistent manner, and reveal trends similar to those in the Information Centre figures. 16 According to Binley, the NHS management numbers in England rose by 28% between 1997 and 2010. NHS spending over this period increased by 105% in real terms, from £60 billion in 1996/1997 to around £123 billion in 2010/2011 (at 2011 prices). 16 Thus, the management workforce did not expand disproportionately, having not only more staff but also more money to manage. Management numbers in acute services (across the UK) have also been relatively stable, with 14,810 in 1997, 12,642 in 2000, and 13,985 in 2010.
How does the NHS compare with other sectors? The Office of National Statistics Labour Force Survey shows that around 15% of the total UK workforce are designated ‘managers and senior officials’. This proportion has changed little in the past decade, rising from 13.6% of all those in employment in 2001 to 15.6% in 2010 (http://www.statistics.gov.uk/statbase/product.asp?vlnk=14248). The NHS thus appears to be short of managerial expertise in comparison, with only a 3% management cohort.
The question of management numbers is linked to costs which, in a climate of global recession and domestic austerity, have also been subject to debate. Management costs were around 3% of the service budget in 2010. US charities spend between 4 and 8% of revenue on management. 17 The estimate for UK charities is between 5 and 13%. 18 These figures are evidence that the NHS is under-managed, a situation that would be exacerbated by the policy of cutting management costs by 45% by 2014/2015. 17
Management accounted for 1.5% of the NHS budget in 2009, putting the UK at number 18 in a list of 23 national health systems. 19 Management in other countries consumed much higher proportions of their health care budgets, including Mexico (11.8%), USA (7%) and France (6.8%), contrary to a claim by the Secretary of State for Health that there was no comparative international evidence to show that the NHS had low management costs.
As one of the largest employers in the world, spending over £2 billion a week, meeting the health care needs of 60 million people, the proportion of managers in the NHS is low. 20 The evidence indeed suggests that the NHS has ‘lean management’. The wisdom of policy to cut management numbers and costs is thus in doubt, as this weakens the motivation and commitment of remaining managers, and also dilutes the management capacity to implement the major changes that government policies demand. The King’s Fund 3 commission on management in the NHS concluded that it would be equally appropriate to enquire how the service could be run with only 40,000 managers.
Another estimate of management numbers
Evidence from this project suggests that official figures underestimate management numbers. This arises because the NHS Information Centre data do not count as managers those clinical and scientific staff holding hybrid roles. Employment figures compiled by the Centre are based on the Occupational Code Manual Version 7. 21 Managers are covered in the ‘G matrix for administration and estates staff’, including those with ‘overall responsibility for budgets, staff or assets, or who are held accountable for a significant area of work’; chief executives, board directors and deputies and service managers reporting to them. However, managers who must be qualified as doctors, nurses, therapists, scientists or ambulance personnel are coded in their professional area, such as clinical directors, matrons, ward sisters and laboratory supervisors. Trust chairs and non-executive directors do not appear in the management numbers either. They are coded in the ‘Z matrix for general payments’, along with Macmillan and Marie Curie nurses.
Other line managers, team leaders and supervisors are coded as ‘clerical and administrative’. They are excluded from management numbers because they ‘do not have responsibility for a significant area of work/budget’, and include ‘line managers for whom management is only a portion of their role who may also act as analysts or in some other administrative or clerical capacity’. This understates the significance of such roles – ward management, outpatient department management, the management of diagnostic units and cleaning, catering and portering supervisors. Those staff can have a major impact on hospital performance, quality of care and reputation. Staff coded in the ‘clerical and administrative’ category in the G matrix appear in the census as ‘support to clinical staff’. In 2010, those support staff accounted for 26.5% of all NHS employment in England, a proportion that has also been stable for a decade. The proportion of staff in ‘central functions’ – finance, personnel, information – has changed little, remaining at 8% of employees in 2010.
To help understand the acute hospital trust management profile in more detail, the workforce information departments (which provide the census data for the NHS Information Centre) in Clearview and Greenhill hospitals were asked to provide independent estimates of the total management populations of their trusts, including pure plays and hybrids, based on the definition of ‘managerial responsibilities’ discussed earlier. Producing these figures is not straightforward (other trusts declined to allocate staff time to this), as hospital databases do not categorize employees in this way. Occupational groups and many individual roles thus had to be inspected manually in order to arrive at an estimate.
The management populations at Clearview and Greenhill trusts.

Note: Clearview at April 2011; Greenhill at September 2011.
Are these estimates from two trusts representative? Both were long established and had foundation status. Clearview had 7000 staff, 1150 beds and a budget of £590 million. Greenhill had 8000 staff, 1100 beds and a budget of £420 million. Their management agendas were similar, including financial challenges, recent reorganizations and regulatory issues. Other trusts may display different profiles. However, given an inclusive definition of management, these estimates have face validity, supported by the consistency between the two accounts. It is thus reasonable to assume that, should estimates from other trusts differ from these, they would almost certainly support the conclusion that the hospital management function is much more widely distributed than official accounts suggest.
Management capacity
Estimates of numbers of managers say little about management capacity, which can be defined as the ability to respond effectively to the demands placed upon an organization at any given time. With only 3% of staff officially holding managerial positions, the NHS has been accused of being over-managed. Does the claim that 30% of acute trust employees have managerial roles reinforce that criticism? The management agendas of the trusts in this study were lengthy, complex and demanding. Different profiles of pure plays and hybrids may be equally effective in the context of different local conditions, past histories and current agendas. It is clearly not possible to assess capacity simply by comparing numbers. Fewer pure plays may mean lower management costs but that would increase the burden on hybrids, reducing time for patients, professional development and implementing service improvements. That may in turn lead to the appointment of more clinical staff to compensate, cancelling the cost advantage of having fewer professional managers.
At least four other factors potentially influence the management capacity of an acute trust. First, most of the 30% with managerial roles are hybrids. One senior hybrid, when asked about the mix of clinical and managerial responsibilities in nursing roles, replied: ‘Head nurses are ‘50–50’. They’re responsible for the managerial nursing aspects in their directorate. But I hold them accountable for nursing professional issues as well. For a matron, I would expect that to be very much more clinical. And probably it should be 75–25, clinical–managerial. For a ward sister, the ideal is that they should have two days a week where they can deal with the managerial elements of their role, but it’s also about making sure standards are adhered to. So probably a 60–40 split’. Interviewer: In your judgement, are some of those staff spending more time on their management responsibilities than they should? ‘No. I would say it’s the other way around. They don’t get enough management time’. (Director of Nursing, Netherby)
Interviews with matrons elsewhere suggest that this balance of responsibilities varies from trust to trust, and fluctuates over time, depending on the management agenda.
Second, some ‘pure plays’ have specialist non-managerial responsibilities, so they are not necessarily each a ‘full’ FTE. For example, one manager commented about her specialist responsibilities: ‘Question: Is my profession “manager” or “trainer/coach”? Answer: Trainer/coach. Therefore, when answering what percentage do I “manage/lead” versus what is “practical/specialist”, I’d say 70–30. I do have a practical/specialist role I fulfil that is not management. There is clear water between the two, and I suspect that many others will say the same. Few of them will see themselves as NHS managers wholly, rather a specialist first, in a management role, but their loyalties are often to the profession they trained hard in’. (Head of Leadership Development, Greenhill)
Thus, 100 pure plays do not necessarily equate to 100 FTE managers. Also, many pure plays have clinical backgrounds which they bring to their relationships with clinical staff, and use to inform decisions and judgements. Some maintain their clinical registration, asking workforce information offices not to code them in the G matrix as managers.
Third, most hybrids have limited management education, beyond short courses. A masters degree in business administration takes a year of full time study to complete; few clinical staff have the desire, time or financial resources to obtain this qualification. During this project, some trusts implemented their own leadership and management development programmes. But these still amounted to more ‘short courses’, albeit intensive and tailored. The management capabilities of many hybrids are thus dependent on limited educational input and considerable on-the-job learning: ‘We don’t have any managerial training and lots of work is left to us. I expect that in the future we will be left to make more decisions. There is more workload. You have to do appraisals, you are asked to create a new policy and deliver presentations and you are expected to do more’. (Theatre Unit Manager, Greenhill) ‘I’ve been in post for three years, and I want promotion. Are they developing me into a matron’s role? There is no ongoing development. Ward managers are just left to get on with it. You are left on your own. Find your own development. The one-to-one meetings that we have with more senior management are all about operations and finance’. (Ward Sister Medicine, Netherby)
Fourth, many hybrids do not view themselves as managers or they may use the label reluctantly. In 2010, ward managers at Netherby voted to change their job title back from ward manager to ward sister. Other examples included: ‘I’ve been a consultant nephrologist since 2003, and I’ve been involved with the emergency department project since 2005. The role of clinical lead is managerial if you want to call it that. In the emergency department project, this has involved structure change. But “management” has connotations among clinicians relating to stick not carrot. Managers are people who withhold resources rather than try to improve services. My role is more of a leadership and organization development role, much wider than management’. (Clinical Director Medicine, Greenhill) ‘I would describe my role as clinical leadership. I’m not nursing, not hands on. I am not at all managerial. My role is professional leadership. But this does influence behaviour, practice, change, service improvement, so managerial in those senses. The senior staff on the wards have managerial responsibility; ward sister, charge nurse are front line managers. Matrons and head nurses are middle management. I have a manager role, but I have professional accountability, so the emphasis of my role is with professional leadership’. (Assistant Director of Nursing, Netherby)
These participants were more comfortable describing themselves as ‘leaders’, reflecting a trend across the public sector to value leadership at the expense of mere management. 22 If the distinguishing features of leadership concern designing, inspiring and driving change, then middle management roles in the NHS are indeed a blend of management and leadership.
To illustrate how pure plays and hybrids populate a hospital management structure, Figure 1 shows the organization chart for the medicine division at Clearview. This division had 350 beds in 16 wards, employing 1200 staff (headcount). The organization chart identifies 21 ‘pure plays’ and 80 ‘hybrids’. This also confirms the typical balance of roles; the ratio of hybrids to pure plays in this division was around four to one.
Clearview Hospital Medicine Division organization chart (October 2011). *Managers with clinical backgrounds.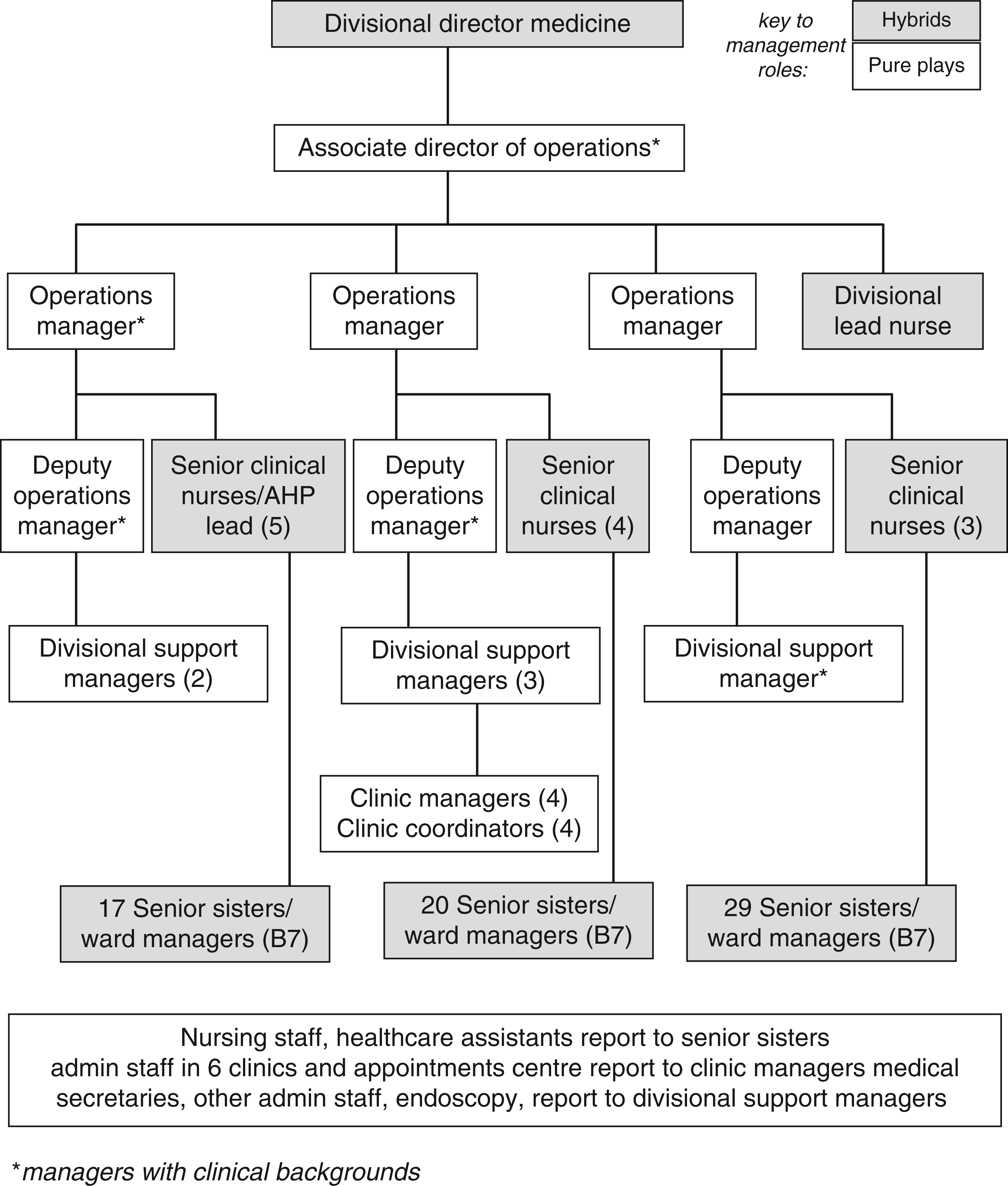
Discussion
Hospital management appears to be a widely distributed function. When middle managers and those in hybrid roles are included, the proportion of staff in an acute trust with managerial responsibilities is around 30%. The ‘over-managed NHS’ thesis does not survive this recalculation, however, for two reasons. First, most of the 30% have part time managerial roles, with limited management training, may assume that role label unwillingly, and do not consider themselves to be managers. Second, with regard to quality and safety of care, service improvement and organizational performance, the managerial capacity of an acute trust is a more important consideration than management numbers.
While derogatory comments from government ministers and the media are presumably aimed at pure plays, the resultant negative stereotype is a deterrent to clinical staff who are invited to take on managerial roles. As it is policy to encourage clinical staff to assume management responsibilities, this deterrent effect is perverse. Cuts in the numbers of pure plays also affect adversely the workloads of hybrids who have to fill the resultant gaps, jeopardizing the implementation of structural, regulatory and financial reforms, and potentially compromising patient safety by increasing the management pressures on those hybrids. Reducing pure play numbers thus has a systemic impact on management capacity by redistributing workload.
Management capacity in an acute trust can be seen as a product of: management numbers; individual capabilities; engagement and motivation; organizational resources and infrastructure; the quality of clinical–managerial collaboration and the ability to generate ‘requisite variety’.
The last two of these components of capacity are particularly important. Ashby’s 23 ‘law of requisite variety’ argues that the management function must be able to generate at least the same levels of variety and complexity as the system being managed can adopt. For example, to address health care risk and safety issues, the ‘London Protocol’ identifies the hierarchy of factors that influence clinical practice, including the institutional context, organization and management factors, work environment, team factors, individual staff factors, task factors and patient characteristics. 24 Effectively addressing problems in this domain, therefore, potentially requires knowledge, expertise and perspectives spanning that range of factors. In other words, variety and complexity are required in order to deal effectively with variety and complexity; responses to complexity are often mistakenly aimed at simplification. The absence of multiple perspectives and diversity in thinking has been shown to reduce organizational resilience and contribute to system failures. 25 A management function that draws its members from a range of different backgrounds may thus generate greater diversity than a more homogeneous group, and the quality of their collaboration is thus a key factor.
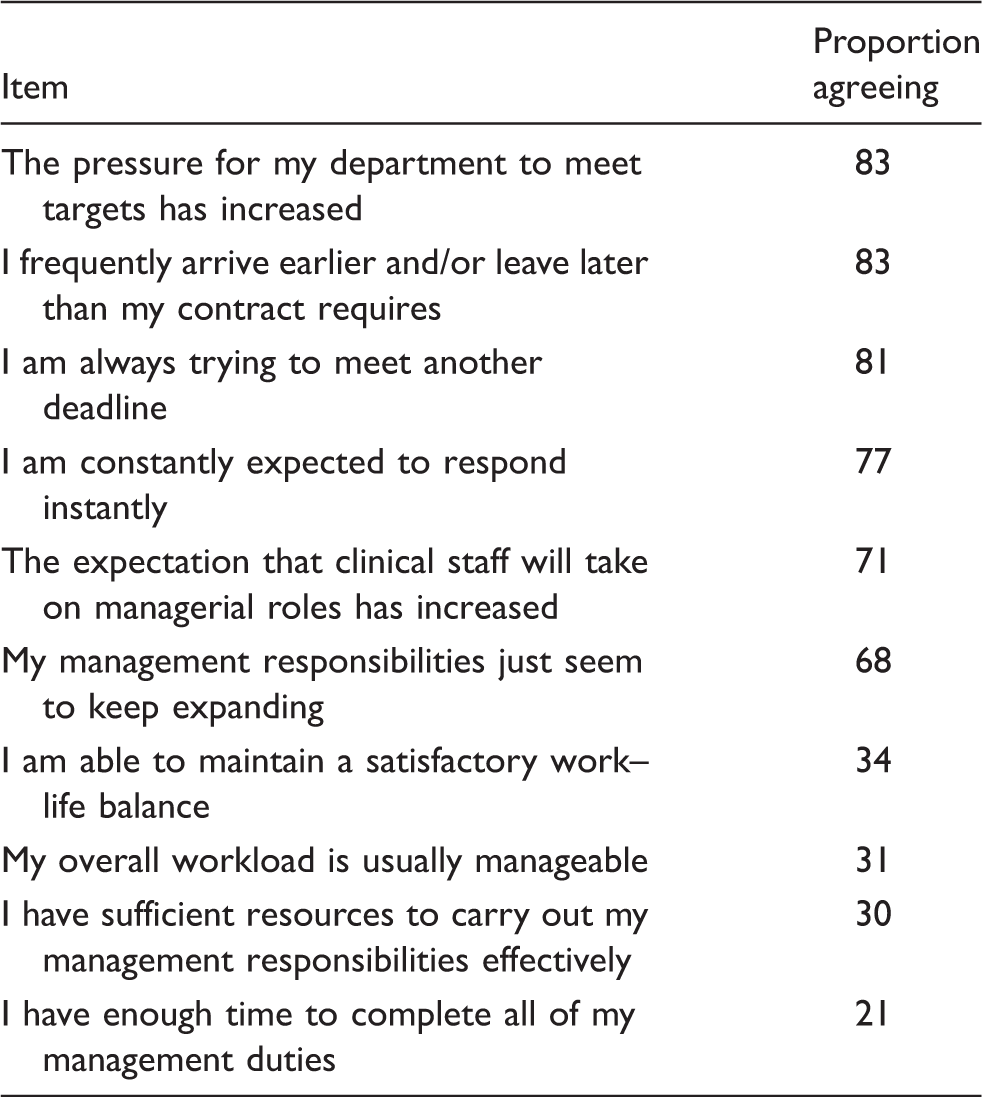
Symptoms of lack of management capacity.
This analysis suggests four main conclusions. First, policy debate over NHS management numbers could usefully be informed by a more nuanced understanding of the composition, contributions and collective capacity of the group under discussion. The debate since 2009 has relied on data which do not accurately reflect either the composition or the capacity of managers responsible for providing and developing acute services. Policy and decisions based on those figures may thus be open to question. Second, it would thus be helpful to put the preoccupation with numbers and costs aside, and to focus instead on the more significant question of management capacity. Capacity appears to be a more critical issue, for a service facing multiple demands for radical and rapid changes in the ways in which it is organized, funded, delivered and regulated. Reducing pure play management numbers, and redistributing their responsibilities to hybrids, potentially weakens capacity at a time when demands are already high and increasing. It would thus be appropriate to subject future policy initiatives to prior assessment of their impact on management capacity. It may also be helpful to consider capacity building measures, particularly where demands on the management function are being increased. With regard to the six components of the model outlined above, some capacity-building measures are cost neutral, such as initiatives to strengthen engagement, motivation and inter-professional collaboration in problem solving and service improvement.
Third, service line management structures developed by participating trusts sought to reduce general (pure play) management numbers, and to place medical staff in key managerial roles (e.g. division heads). Many of the latter struggled with the management workload, especially as they maintained their clinical duties. Trust senior management needs to consider the impact of such reorganization on overall management capacity. Fourth, leadership and management development programmes should consider extending their reach, if they have not already done so, to cover their whole ‘pure plays and hybrids’ management populations. Assessing management capacity is an area for further research, as a better understanding of how capacity can be measured, managed, maintained and strengthened, would have practical benefits for the service, for individual provider organizations, and ultimately for patients.
Footnotes
Acknowledgements
The author thanks those who gave their time to this project, particularly the workforce information managers.
Funding
This research was funded by the NIHR HS&DR programme (SDO/08/1808/238). The views expressed are those of the author, and not necessarily those of the NHS, National Institute for Health Research or Department of Health.