
Abstract
Objectives
Many patients with long-term conditions have multiple conditions. Current delivery of care is not designed around their needs and they may face barriers to effective self-management. This study assessed the relationships between multimorbidity, the delivery of care, and self-management.
Methods
We surveyed 2439 patients with long-term conditions concerning their experience of the delivery of care and self-management in England in 2011. We assessed multimorbidity in terms of a count of long-term conditions and the presence of ‘probable depression’. We explored the relationships between multimorbidity, patient experience of the delivery of care, and self-management
Results
Neither measure of multimorbidity was a significant predictor of patients’ experience of the delivery of care. Patients with multimorbidity reported higher levels of self-management behaviour, while the presence of depression was associated with less positive attitudes towards self-management.
Conclusions
The current data do not demonstrate a consistent impact of multimorbidity on patients’ experience of care or on self-management. Further research is required to assess those types of multimorbidity that are associated with significant deficits, or to identify other aspects of care that might be problematic in the context of multiple conditions.
Introduction
Improving quality of care in long-term conditions is a focus of health policy. The Chronic Care Model highlights the need for improvements in the delivery of care (through a ‘prepared, proactive practice team’) and in patient self-management (through an ‘informed, activated patient’). 1
What should high quality care for long-term conditions be like from a patient perspective? Important components would include effective communication 2 and shared decision-making. 3 Patients receiving care from multiple providers require effective co-ordination and many also benefit from continuity of care. 4 Other quality indicators include written care plans, 5 enhanced referral to other providers, 1 and proactive follow-up. 6 Self-management can refer to discrete behaviours (e.g. adhering to medication) as well as more general attitudes such as self-efficacy. 7
Multimorbidity
There is no consensus definition of multimorbidity, but here it is defined as ‘the coexistence of two or more chronic conditions, where one is not necessarily more central than the others’. 8
Although some care may be improved in multimorbidity, 9 patients with multiple conditions are potentially at greater risk of deficits. 10 Multiple problems and limited time may mean that needs for support and information may not be met. 11 Complex interactions with services make patients more vulnerable to failures of co-ordination 12 as well as significant burden of care. 13 In self-management, patients with multimorbidity are more likely to have to manage complex management regimes 14 and face difficult decisions about priorities. 15 They are also likely to be in poorer general health, 10 at an advanced age, 16 with cognitive impairment, 17 and low health literacy. 18 Co-morbid depression may lead to limits on patient self-management, because of links between depression, motivation, and self-efficacy. 19
Evidence on the effects of multimorbidity
Some studies based on standardized assessments of quality have reported higher quality of care in multimorbidity, 9 but the evidence from patient assessments has been more mixed. A survey of 15,709 adults found that multimorbidity was associated with lower ratings of communication. 20 In a small sample of older adults (n = 120), multimorbidity was related to lower ratings on communication and interpersonal care, knowledge of the patient, integration, and trust. 21 A recent European survey of 1745 patients with coronary heart disease (CHD) found that patients with multimorbidity reported lower ratings of care, although the effects were small. 22 A UK study including 1125 patients found lower management continuity with more long-term conditions. 23 A cross-sectional survey in the United States of 422 patients found a higher willingness to learn self-management skills among patients with multimorbidity. 24
Aims
We use data from a cohort of patients with long-term conditions in England’s National Health Service (NHS) and hypothesized that patients with multimorbidity would report a worse experience of the delivery of care and lower levels of self-management.
Methods
Data were collected as part of a wider project on written care plans in the management of people with long-term conditions as mandated in the Darzi NHS White Paper of 2008. 25 We identified practices with different levels of written care plans from the General Practice Patient Survey and recruited patients with long-term conditions from registers. To maximize variation in baseline health, we stratified the sample by age and number of conditions. Inclusion criteria were adult patients who were on the following registers: CHD; heart failure; stroke; chronic obstructive pulmonary disease (COPD); asthma; atrial fibrillation; chronic kidney disease (CKD); diabetes; and epilepsy. Patients were mailed a postal survey, with two reminders.
The study was designed and powered to function as a longitudinal quasi-experiment, creating patient groups differing in rates of receipt of care plans, but similar in all other characteristics. Here we use the data in a cross-sectional secondary analysis to explore factors (including multimorbidity) associated with patient experience of delivery of care and self-management.
Patient experience of service delivery
We used the Patient Assessment of Chronic Illness Care (PACIC), a validated measure of patient assessments of service delivery for long-term conditions.26,27 PACIC includes 20 items in five sub-scales: patient activation; delivery system design; decision support; goal setting; problem-solving; and coordination (each rated on a five-point scale, with high scores indicative of better care). We used the total score across all items as analyses do not support multiple sub-scales. 27
Self-management
We measured a number of different indices relating to self-management. Attitudes and beliefs are important mediators of the benefits of self-management 7 and we used the Health Education Impact Questionnaire (heiQ) to assess these. 28 We only used heiQ scales relating to self-monitoring and insight (seven items, such as ‘as well as seeing my doctor, I regularly monitor changes in my health’) and skill and technique acquisition (five items, such as ‘when I have symptoms, I have skills that help me to cope’). All items used a six-point scale, with high scores indicative of better self-management.
We also measured self-management behaviour via a modified version of the Summary of Diabetes Self-Care Activities (SDSCA), assessing the number of days per week respondents engaged in health behaviours (i.e. eating fruit and vegetables; undertaking exercise; and avoiding eating red meat, alcohol, and smoking). 29 Defining four to seven days as moderate adherence, 30 we counted the number of behaviours performed four to seven days per week (0–5).
Multimorbidity
We based our classification on previously published work, 31 which used a simple count of self-reported long-term conditions, combined with a separate measure of ‘probable depression’. Patients self-reported their existing conditions from a list of 17 (hypertension, chest problems, diabetes, heart problems, CKD, stroke, cancer, anxiety or depression, arthritis, stomach or bowel problems, skin conditions, vision problems, hearing problems, neurological problems, chronic fatigue, thyroid problems, or other). We based our measure on a count of reports of conditions in these categories (excluding anxiety and depression – see below). For the purposes of analysis, we recoded the ‘multimorbidity condition count’ into four equal groups (1, 2, 3, or 4+ conditions).
For depression, we used the five-item Mental Health Index (MHI-5). 32 We coded patients as having ‘probable depression’ if the MHI-5 score was ≤60 (high scores represent greater well-being). 31
Demographic characteristics
We measured age, gender, ethnicity, work and living situation, education and proxies for health literacy. Ethnicity was categorized as ‘white’ and ‘ethnic minority’ for analysis. Patients also reported their living situation, which was coded as ‘living alone’ or ‘cohabiting’. Work was coded as ‘in paid work’ (full or part time) or ‘other’. Qualifications were coded for analysis as ‘higher degree’ or ‘other’. We used an indicator of health literacy, based on a Single Item Literacy Screener (SILS) (‘How often do you need to have someone help you when you read instructions, pamphlets, or other written material from your doctor or pharmacy?’). 33
Health measures
Given the range of conditions included in the study, we measured general health using the Medical Outcomes Study instrument, which assesses self-rated health on a five-point scale (from ‘poor’ to ‘excellent’ with high scores indicative of better health). For health-related quality of life, we used the EQ5D which assesses five dimensions (personal care, mobility, anxiety/depression, usual activities, and pain/discomfort) across three levels of severity and provides a weight based on a population tariff, with high scores indicative of better quality of life. 34
We had previously identified vitality as a useful generic outcome measure across multiple long-term conditions. 35 We used five items from the Medical Outcomes Study to assess vitality, using items (e.g. ‘did you have enough energy’) rated on six-point scales, with higher scores indicative of better vitality. 36
Health care use
We used self-reported measures of general practitioner (GP) and hospital use over the previous six months. We asked patients to identify the health professional they had consulted most about their conditions (GP, practice nurse, community matron, hospital doctor or nurse, other). We used a single item measure of continuity of care (frequency of seeing a preferred doctor, on a five-point scale from ‘almost always’ to ‘almost never’). 37
Analysis
We present descriptive analyses, in terms of patient characteristics, and baseline patient experience of delivery of care and self-management.
Rates of missing data on some PACIC items tend to be higher in the UK, 27 and we restricted analysis to patients with ≤8 missing items (from 20) on PACIC and complete data on other scales. We used regression analyses to assess the relationships between variables. To identify confounding among measures of demography, health, and use, we conducted univariate regression analysis (identifying confounders as those with a p-value < 0.2). Due to associations between health status measures, we used vitality in the multivariate analyses.
We initially fitted a model including only the multimorbidity variables (‘multimorbidity condition count’ and ‘probable depression’) as independent variables. We then added the interaction between ‘multimorbidity condition count’ and ‘probable depression’. We then fitted a multivariate model including ‘multimorbidity condition count’ and ‘probable depression’, together with the relevant confounders. Finally, we added the interaction term between ‘multimorbidity condition count’ and ‘probable depression’ to this model.
All analyses used Stata (version 11.0) and accounted for within-practice clustering. Due to skewness, standard errors were calculated using a bootstrap and 10,000 samples. We generated variance inflation factors to assess multicollinearity. Single omnibus tests of significance are reported for associations between categorical variables and outcomes.
Results
Respondent characteristics.
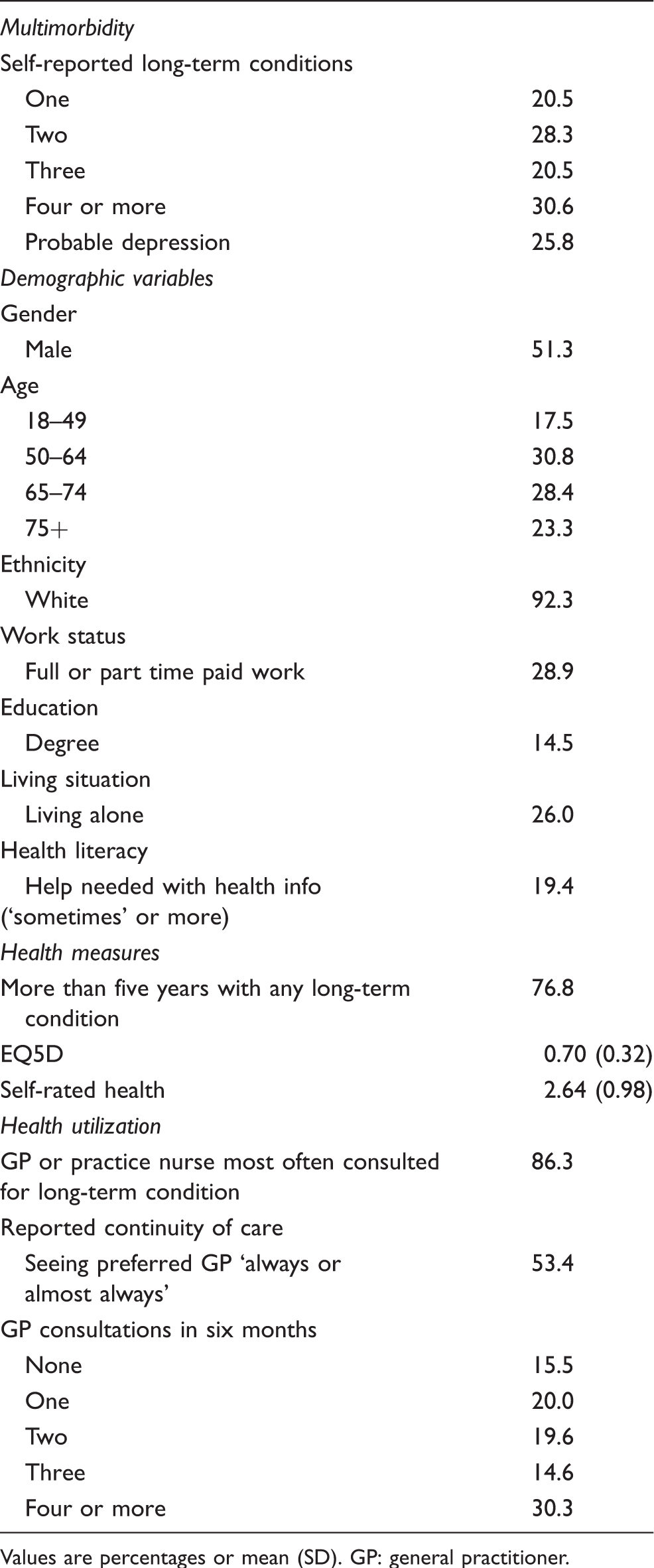
Values are percentages or mean (SD). GP: general practitioner.
Mean reports of service delivery and self-management by multimorbidity type.
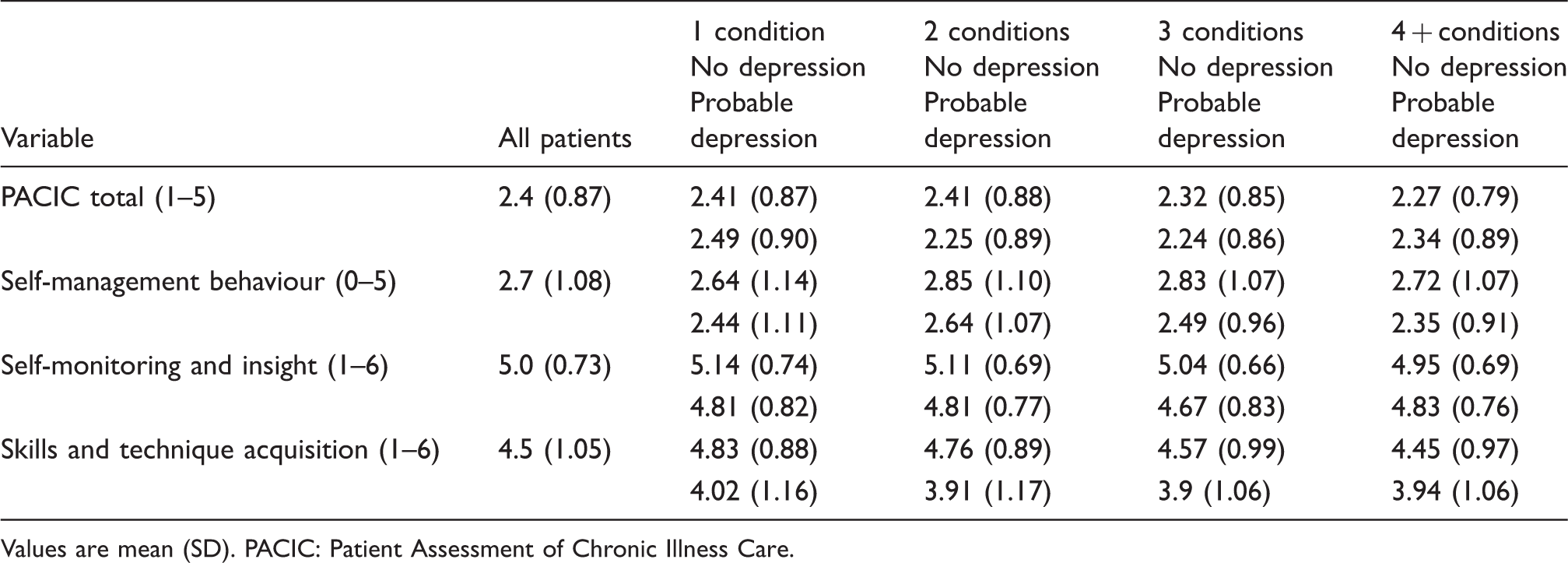
Values are mean (SD). PACIC: Patient Assessment of Chronic Illness Care.
Patient experience of delivery of care
We found no significant relationships between ‘multimorbidity condition count’ (χ2 = 5.52, df = 3, p = 0.14) or ‘probable depression’ (χ2 = 0.38, df = 1, p = 0.53) and total PACIC scores. The interaction term was also not significant (χ2 = 5.83, df = 3, p = 0.12).
Multivariate analyses of predictors of service delivery and self-management.
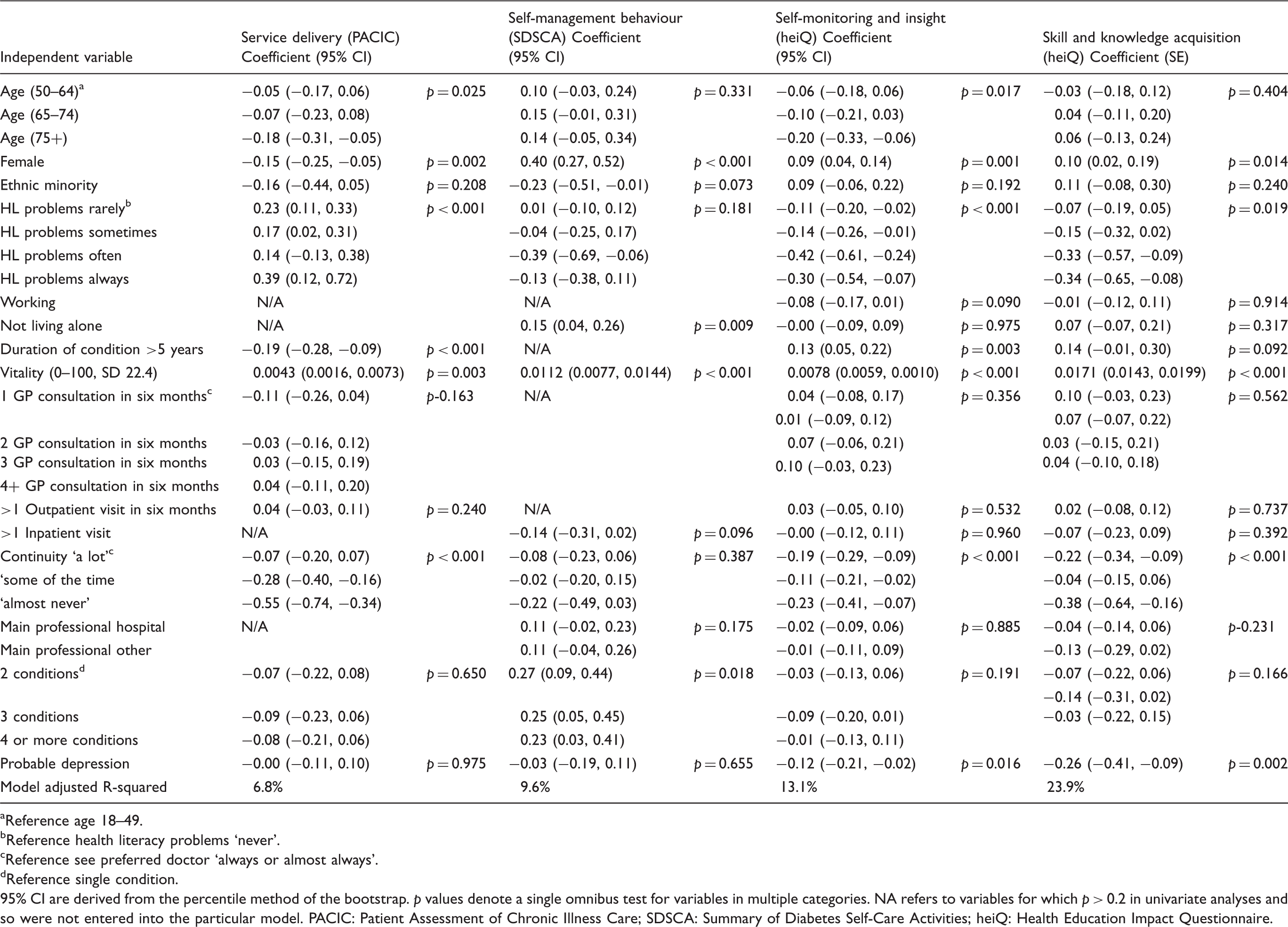
Reference age 18–49.
Reference health literacy problems ‘never’.
Reference see preferred doctor ‘always or almost always’.
Reference single condition.
95% CI are derived from the percentile method of the bootstrap. p values denote a single omnibus test for variables in multiple categories. NA refers to variables for which p > 0.2 in univariate analyses and so were not entered into the particular model. PACIC: Patient Assessment of Chronic Illness Care; SDSCA: Summary of Diabetes Self-Care Activities; heiQ: Health Education Impact Questionnaire.
Self-management
We found significant relationships between self-management and both ‘multimorbidity condition count’ and ‘coexisting probable depression’, with higher reported self-management in those with more conditions, particularly two or three (compared to just 1 – χ2 = 16.53, df = 3, p < 0.001) and lower levels in those with ‘probable depression’ (χ2 = 28.6, df = 1, p < 0.001). The interaction term was not significant (χ2, df = 3, χ2 = 2.56, p = 0.46).
‘Multimorbidity condition count’ remained significant (χ2 = 10.07, df = 3, p = 0.018), but ‘coexisting probable depression’ was not a significant predictor in the multivariate analysis (χ2 = 0.20, df = 1, p = 0.655). The results suggested that, compared to those with one condition, those with two, three or four and more conditions reported moderate levels of adherence in relation to around 0.25 more self-management behaviours (out of five, with an overall mean 2.7, SD 1.08). More self-management was reported by females, those not living alone and patients with greater vitality (Table 3).
Self-monitoring and insight
We found significant relationships between self-monitoring and insight and ‘multimorbidity condition count’ (χ2 = 11.1, df = 3, p = 0.01) and ‘probable depression’ (χ2 = 51.0, df = 1, p < 0.001), with lower self-monitoring and insight in those with more conditions and in those with ‘probable depression’. We also found a statistically significant interaction between ‘multimorbidity condition count’ and ‘probable depression’ on patient-reported self-monitoring and insight (χ2 = 9.56, df = 3, p = 0.02). The interaction showed lower reported self-monitoring and insight in patients with ‘probable depression’ at the lower end of the ‘multimorbidity condition count’, but some convergence as the number of conditions increased.
Patients with ‘probable depression’ reported lower degrees of self-monitoring and insight in the multivariate analysis (χ2 = 5.86, df = 1, p = 0.016), with a reduction in mean score in those with ‘probable depression’ equivalent to 0.12 (mean 5.0, SD 0.73). The effect of ‘multimorbidity condition count’ and the interaction between ‘multimorbidity condition count’ and ‘probable depression’ were no longer significant in the multivariate analysis. Lower self-monitoring and insight was also reported by the elderly, those reporting any health literacy issues, and patients with poorer continuity of care. Greater self-monitoring and insight was reported by females, those with higher levels of vitality, and those living with their condition for longer (Table 3).
Skills and technique acquisition
We found significant relationships between skills and technique acquisition and ‘multimorbidity condition count’ (χ2 = 24.6, df = 3, p < 0.001) and ‘probable depression’ (χ2 = 165.6, df = 1, p < 0.001), with lower levels of skills and technique acquisition in those with multiple conditions and probable depression. We also found a statistically significant interaction between ‘multimorbidity count’ and ‘probable depression’ on skills and technique acquisition (χ2 = 14.5, df = 3, p = 0.002). The interaction showed lower reported skills and technique acquisition in patients with ‘probable depression’ at the lower end of the ‘multimorbidity condition count’, but some convergence as the number of conditions increased.
‘Multimorbidity condition count’ was no longer a significant predictor of skills and technique acquisition (χ2 = 5.09, df = 3, p = 0.166), but patients with ‘probable depression’ did report significantly lower scores in the multivariate analysis (χ2 = 9.3, df = 1, p = 0.002), with a reduction in mean score in those with ‘probable depression’ equivalent to 0.26 (mean 4.5, SD 1.05). Fewer skills and less technique acquisition was reported by those with health literacy issues and poorer continuity of care. Greater skills and technique acquisition was reported in females and patients with greater vitality (Table 3).
Discussion
Our analysis indicated that patients with multimorbidity did not report a poorer experience of delivery of care, even when they reported four or more conditions, probable depression, or a combination. Depression was a more consistent negative predictor of self-management attitudes, but this effect did not extend to reports of self-management behaviour.
Limitations of the study
External validity is limited by the relatively low response rate, although the rate is conventional in studies using comparable methods.23,38,39 Although the main impact of a low response rate is on external validity, it can impact on reported associations if there are significant restrictions in range in key variables, or if people with multimorbidity are less likely to respond if they receive poor care.
The study was dependent on the validity of the measures. 40 The MHI-5 is a validated measure of depression.41,42 The validity of using self-reports of other conditions is less clear. The data on conditions were reduced to a simple count and were not dependent on highly accurate coding, but use of self-reports may have introduced error. Continuity is not rated by a significant proportion of patients, and the results will not generalize to such patients as they were excluded. PACIC has demonstrated some issues in use in UK populations, 27 although it does demonstrate a reasonable distribution of responses. More sensitive measures, such as bespoke co-ordination measures 43 may be better able to pick up relevant deficits. There is clear potential for bias in reports of self-management behaviour, but our analysis was not concerned to report mean scores, and unless the bias in reports of self-management was also confounded with other measures (such as self-reported comorbidity counts) then the impact should be more limited.
Results in context
A European study of patients with CHD did find lower PACIC scores in patients with multimorbidity, but the effect was very small. 22 The current study did not confirm published findings about lower ratings of communication in patients with multimorbidity,20,21 although the PACIC is more concerned with the content of discussions.
It is important to compare the current results with published qualitative work on patient experience of multimorbidity, which include reports of deficits in delivery of care 44 and in self-management support. 10 These differences may reflect variation in the selection of patients into different types of studies, or may highlight that the problems identified in detailed qualitative work reflect the experience of some patients, rather than a general association.
Implications of the research for policy
The current data suggest no clear relationship between numbers of conditions and patient reports of delivery of care or self-management. It may be necessary to identify particular sub-groups which are at higher risk of deficits in delivery of care or self-management, or more clearly delineate those aspects of care that might be expected to be better or worse, in people with multimorbidity. Given the prevalence of depression in multimorbidity, it is noteworthy that depression was found to be related to poor self-management attitudes (even after controlling for health status), although it is equally interesting that depression did not relate to measures of behaviour. It is still unclear which of the two are more important determinants of outcomes. 45
A striking finding is the consistent relationship between three outcomes and health literacy. The ability of a postal questionnaire to capture health literacy problems is limited, but even in the more restricted sample of respondents, health literacy was a consistent predictor. Also of note is that the effects were reversed for PACIC, where lower health literacy was associated with higher ratings of service delivery and organization. There are a variety of explanations, such as differing expectations of care in different patient groups. Given the importance of health literacy as a predictor of outcomes, these relationships deserve exploration. 46
Conclusions
Although multimorbidity raises many potential challenges to health care delivery, our data suggest that patients with multiple conditions in the English NHS do not generally perceive their care to be deficient. Patients with depression report less positive attitudes to self-management, but overall health and health literacy may be more important determinants of patient experience of delivery of care and self-management support.
Footnotes
Declaration of Conflicting Interests
None.
Funding
This paper is based on research commissioned and funded by the Policy Research Programme, the English Department of Health. The views expressed are not necessarily those of the Department of Health.