
Abstract
Objectives
Health services contribute significantly to greenhouse gas emissions. New models of delivering care closer to patients have the potential to reduce travelling and associated emissions. We aimed to compare the emissions of patients attending a teleconsultation – an outpatient appointment using video-conferencing equipment – with those of patients attending a face-to-face appointment.
Methods
We estimated the total distances travelled and the direct and indirect greenhouse gas emissions for 20,824 teleconsultations performed between 2004 and 2011 in Alentejo, a Portuguese region. These were compared to the distances and emissions that would have resulted if teleconsultations were not available and patients had to attend face-to-face outpatient appointments. Estimates were calculated using survey data on mode of transport, and national aggregate data for car engine size and fuel. A sensitivity analysis using the lower and upper quartiles for survey distances was performed.
Results
Teleconsultations led to reductions in distances and emissions of 95%. 2,313,819 km of travelling and 455 tonnes of greenhouse gas emissions were avoided (22 kg of carbon dioxide equivalent per patient). The incorporation of modes of transport and car engine size and fuel in the analysis led to emission estimates which were 12% smaller than those assuming all patients used an average car.
Conclusions
The availability of remote care services can significantly reduce road travel and associated emissions. At a time when many countries are committed to reducing their carbon footprint, it is desirable to explore how these reductions could be incorporated into technology assessments and economic evaluations.
Introduction
Health services contribute significantly to greenhouse gas (GHG) emissions. In England, the National Health Service’s (NHS) overall carbon footprint stands at 20 million tonnes of carbon dioxide equivalent (tCO2e, a universal unit of measurement that allows the global warming potential of different GHGs to be compared), or 30% of the public sector’s total. 1 In the USA, the health sector contributes 8% of total GHG emissions. 2 To help meet a national target of 80% reduction in emissions by 2050 (from 1990 levels), the English NHS has committed to a 10% reduction in its own emissions by 2015.
While the bulk of health care emissions are associated with procurement and use of energy (fossil fuels and electricity) in buildings, patient travel is the origin of significant emissions. In 2010, travelling accounted for 16% of GHG emissions attributable to the NHS, with journeys made by staff, patients and visitors representing 5% of all road transport emissions in England. 3 In the USA, the providers organized in the National Association for Home Care and Hospice alone were responsible for nearly 5 billion miles in 2008, more than those driven by the United Parcel Service in the same year. 4 Previous research has shown that reductions in travel emissions can be achieved through innovative ways of delivering health care services, in particular by bringing care closer to patients. 5 –8 This is likely not only to reduce energy requirements for travel but also building energy use. Moreover, shorter distances can be more easily covered by walking or cycling, promoting health as well as further reducing the need for health care. 9
Previous studies have explored the impact of remote care interventions on travel emissions. Masino et al. 5 estimated the reduction in GHG emissions from 840 teleconsultations completed over a period of six months in Ontario, Canada and concluded emissions were cut by approximately 185 tCO2e (220 kg CO2e per patient). Lewis et al. 6 studied the use of video-conferencing to assist multidisciplinary teams deliver cancer services in rural areas of west Wales and estimated emission reductions for 21 meetings in October 2006 (1696 kg of CO2) and 30 meetings in October 2007 (2590 kg of CO2), avoiding a total of 84 kg of CO2 per meeting. Dorrian et al. 7 investigated the use of head and neck cancer assessment teleconsultations for 42 patients from the Shetland Islands, Scotland. The authors estimated an average saving of 123 kg of CO2 per patient. Finally, Bond et al. 8 assessed the impact of mobile breast screening clinics with an estimated reduction between 233.8 and 234.6 tCO2 (3.85–3.87 kg CO2 per patient).
There are a number of limitations in previous research. All studies assume patients drive an average car with a specific fuel and engine size (or cars with an average emission). Second, patients may use other modes of transport besides cars. For example, emission coefficients for bus and coach travel are lower than for an average car. Third, there have been no studies including indirect GHG emissions. Direct emissions are those emitted at the point of use of a vehicle, while indirect emissions include those from production and distribution of fuels to their point of use (emissions from the production of vehicles or infrastructure are not considered). Finally, only Bond et al. have assessed impact over a long period of time.
In this study, we address these limitations by combining a number of data sources on modes of transport, engine size and fuel type, to estimate the impact of eight years of teleconsultations in Alentejo, a region in Portugal, on the distances travelled and associated direct and indirect GHG emissions.
Methods
Teleconsultations are real-time outpatient appointments using video-conferencing equipment to connect patients visiting their general practitioners to remotely located consultants. In Alentejo, they have been used since 1998 to help deal with a significant mismatch between the needs of a geographically dispersed population and a concentrated supply of specialized outpatient services. Local primary health care centres are free to choose whether they wish to use teleconsultations or not. The region covers a third of Portugal, yet it is home to only 5% of the population. The average alentejano is poorer, older and less educated than the average Portuguese. The region also has a poor public transportation network. All these factors create significant challenges for health care services seeking to ensure equity in access.
Sources of data
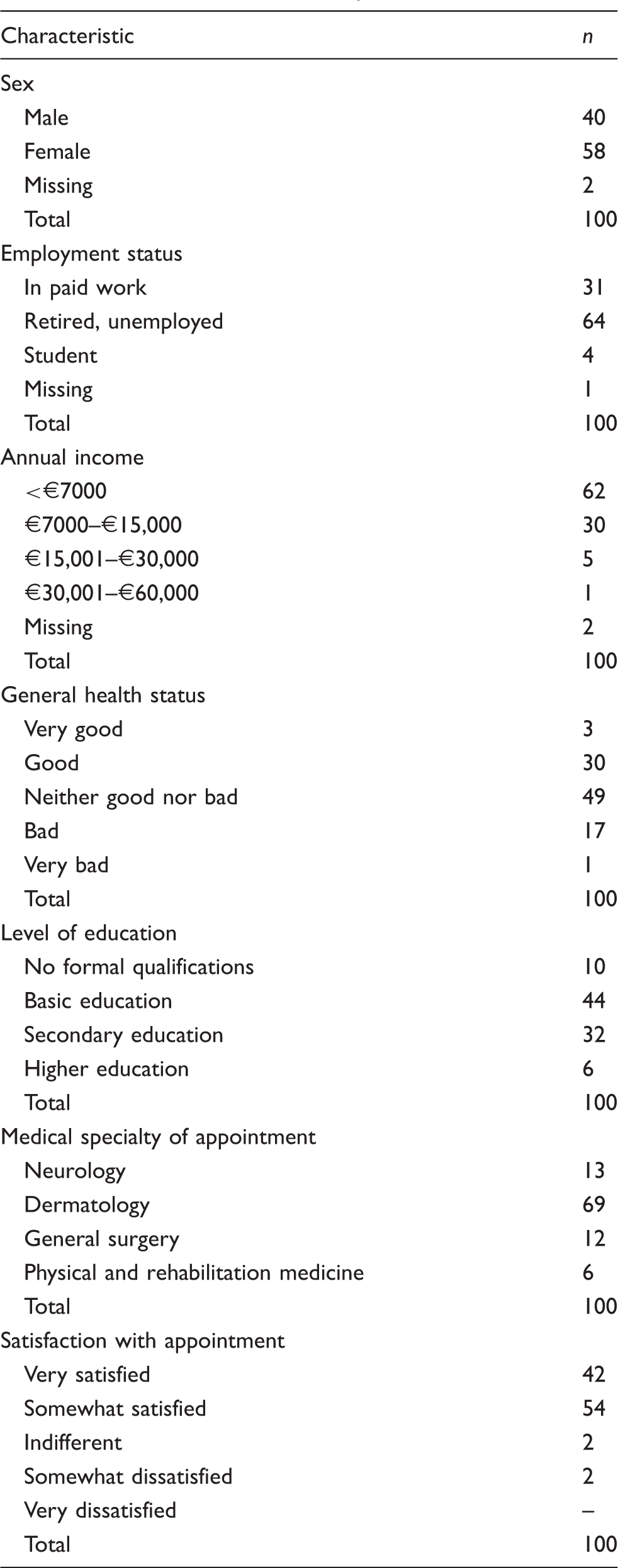
We conducted a survey of 100 teleconsultation patients and 100 face-to-face outpatients who had appointments in the second half of 2011 with consultants from the Hospital do Espírito Santo de Évora. Respondents were asked about distances travelled and modes of transport used. Patients who had had consultations in neurology, dermatology, physical and rehabilitation medicine, and general surgery were included. Lists of all patients who had an appointment were produced for each specialty and each pathway (i.e. teleconsultation or face-to-face). Each specialty/pathway combination was given a weighting factor according to the proportion of all appointments in the study population. The 100 patients were randomly selected from each pathway and within these specialties the number of patients reflected the weighting factors calculated above.
Characteristics of the sample.
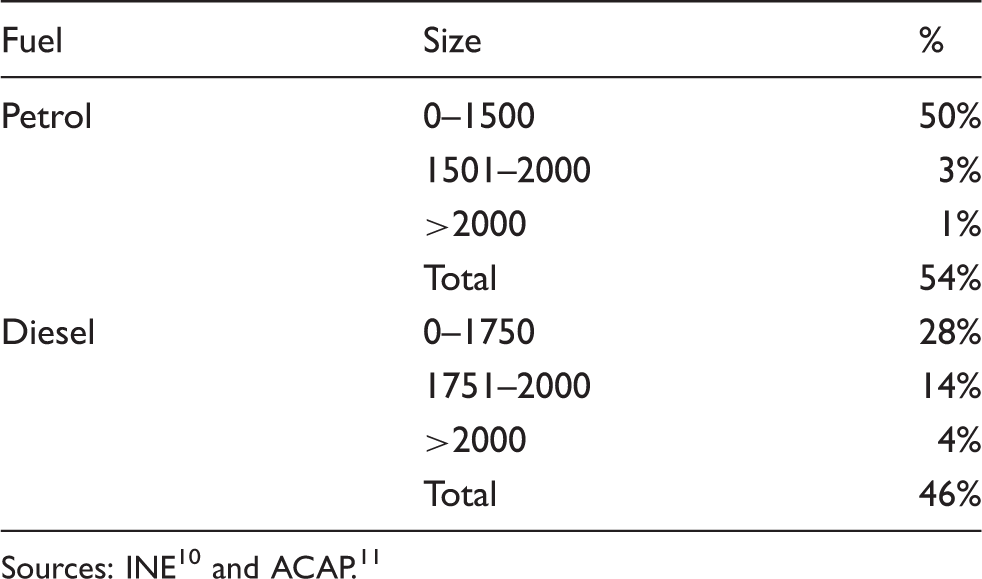
In addition to survey data, we analysed information on the referring and receiving health care units for all 20,824 teleconsultations performed in Alentejo from 2004 to 2011. Lastly, we used aggregate national data on the fuel distribution of vehicles in use and engine size for cars sold in Portugal. 10,11
Estimating emissions
We estimated the reduction in GHG emissions over eight years of teleconsultations in Alentejo. Google Maps™ was used to determine the actual travelling distances to face-to-face appointments if teleconsultations would not have been available. Because we had no information on patients’ places of residence, we assumed that patients travelled the same mean distances as those reported in the survey to get to their teleconsultation appointment in the primary care centre. We assumed that if teleconsultations had not been available, patients would have needed to travel a distance equal to the distance between the referring primary care centre and the hospital for a face-to-face appointment.
Car engine size and fuel in Portugal.
Self-reported one-way distances (km) by mode of transport: descriptive statistics.

We followed 2012 Guidelines to Defra/DECC’s GHG Conversion Factors for Company Reporting to estimate direct and indirect GHG emissions. 12 Bus emissions for teleconsultation patients were estimated using the category ‘Average local bus’ and for face-to-face patients the category ‘Coach’. All ambulance emissions were estimated using the category ‘Average van up to 3.5 tonne’. To assess the impact of the added information on modes of transport and car engine size and fuel type on the results, we estimated emissions resulting from all patients travelling in an average car using an unspecified fuel. Since the average car in Portugal is unlikely to be the same as in the UK, we adjusted the conversion factor for Defra/DECC’s category ‘Average car (unknown fuel)’, using data on average emissions of cars sold in the UK and Portugal, and taking into account that the average age of cars in use in Portugal is nine years compared to 6.9 years in the UK. 13,14
Results
Table 3 provides descriptive statistics for self-reported one-way distances, by mode of transport, from the survey. A number of face-to-face patients in our survey were from Évora (the location of the main hospital) and thus travelled very short distances to their appointments. The mean distances travelled by these face-to-face patients were actually smaller than those covered by teleconsultation patients. We thus excluded these 27 patients from the analysis, as they did not inform our understanding of what means of transport remote patients use. If we then focus on teleconsultation and face-to-face patients, excluding Évora, we notice that 39% of patients walked to the teleconsultation, avoiding costs as well as emissions and potentially improving their general health. Teleconsultation patients reported travelling an average of 5.9 km each way to their appointment, which can be compared to the average 47 km that face-to-face patients travelled. The total distance covered by teleconsultation patients was less than 20% of the distance travelled by face-to-face patients.
Return distances (km) and GHG emissions (kg CO2e) by mode of transport, car fuel and engine size.
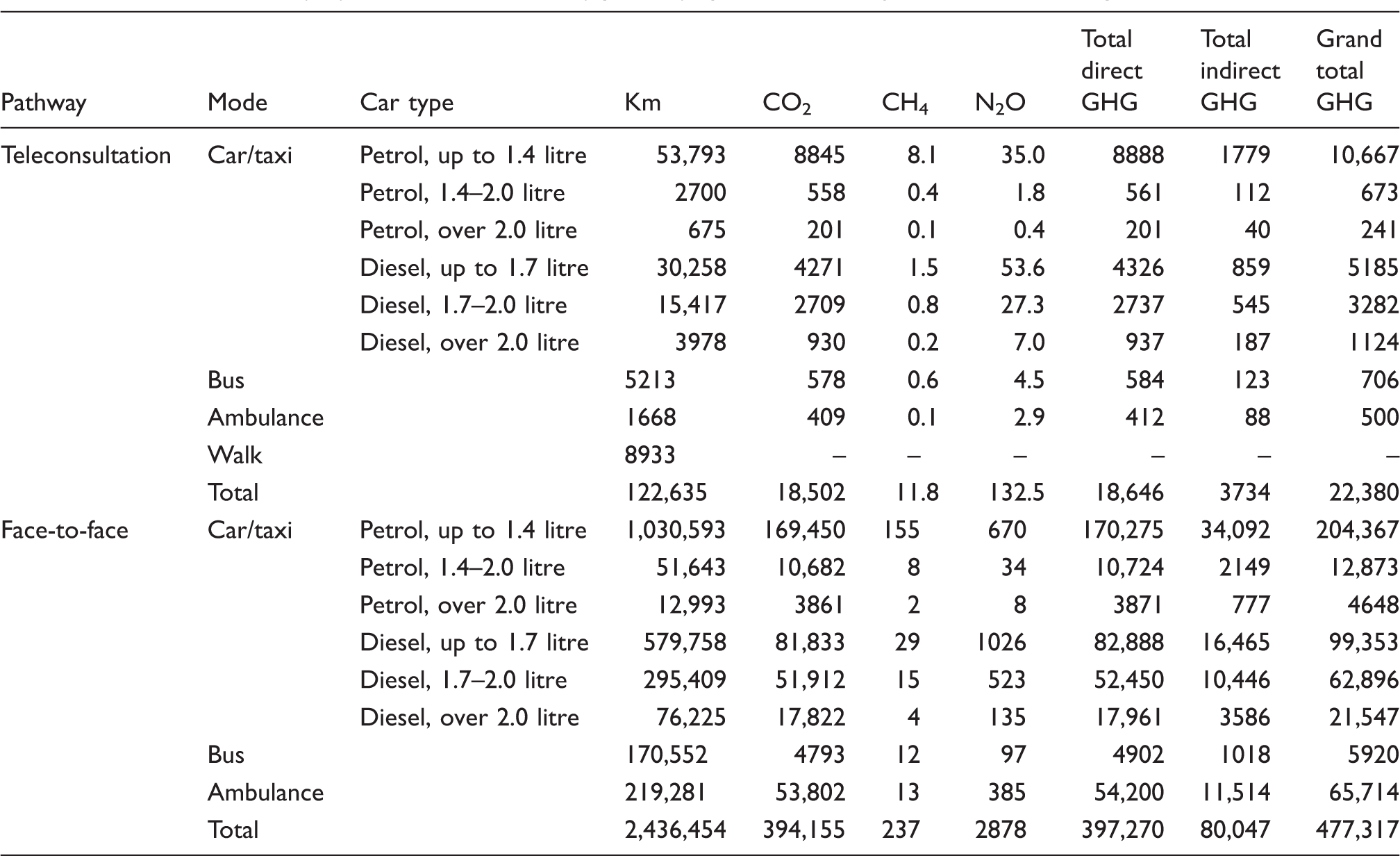
Using data on average emissions of cars sold and average age of cars in use in the UK and Portugal, we estimate that the average car in use in Portugal emits approximately 7% less CO2/km than the average UK car. Since the total direct GHG emissions for Defra/DECC’s ‘Average car (unknown fuel)’ is 0.19469 kg CO2e/km, in Portugal this would be 0.18106 kg CO2e/km (indirect emissions are not affected by this adjustment). Using this emission factor, we estimated total GHG emissions as approximately 510 tCO2e. This is 12% more than the emissions calculated using information on modes of transport and car engine size and fuel. As many patients walked to their appointments, this important feature would have been missed if the analysis had focused on a single mode of transport.
We conducted a sensitivity analysis using the lower quartile (best case scenario) and upper quartile (worst case scenario) distances reported by teleconsultation patients (Table 3). In the best-case scenario, teleconsultation patients would cover about 34,000 km, in the worst-case 159,000 km. The reduction in total direct and indirect GHG emissions from the use of teleconsultations would be 448 tCO2e in the worst-case scenario (a reduction of 94% from the 477 tCO2e emitted to attend face-to-face appointments) and 472 tCO2e in the most favourable scenario (a reduction of 99%).
Discussion
The use of teleconsultations in Alentejo is estimated to have led to reductions in distances travelled and associated emissions of approximately 95%, cutting GHG emissions by a total of 455 tCO2e between 2004 and 2011 (22 kg CO2e per patient). Even assuming upper quartile distances in the survey, teleconsultations still reduced emissions and distances by 94%.
Compared to Ontario’s reduction of 220 kg CO2e per patient over a six-month period, the impact of teleconsultations in Alentejo seems significantly smaller. 5 Yet, it is noteworthy that the average distance to a face-to-face appointment in Ontario was 473 km, and it was assumed that patients used a car to travel (even cases in which patients would travel more than 2000 km). Considering Defra/DECC’s coefficients, bus, train or even air travel would result in fewer emissions than using an average car. According to a review of patient travel assistance programmes in Canada, patients from more remote provinces/territories tend to travel by air or rail. 15 Masino et al. themselves point out that it would be desirable to include alternatives to cars. Our own estimates show that incorporating more detailed information on modes of transport, car engine size and fuel leads to estimates which are 12% smaller than assuming all patients use an average car (510 tCO2e compared to 455 tCO2e). Finally, with 39% of patients in our survey reporting they walked to teleconsultations, our findings illustrate how important it is to account for different modes of transport when estimating GHG emissions.
There are limitations to our research, mainly due to availability of detailed data (e.g. place of residence of patients in our eight year data set). It would be interesting to compare the characteristics of the sample to all those who had outpatient appointments in the second half of 2011 but, unfortunately, this is not possible. Although there are publicly available data on age, sex, income and other characteristics, they refer to the population in general in Alentejo, not to those having had outpatient appointments. While extrapolating from our survey findings to a larger data set may introduce inaccuracies, it does allow the assessment of impact over a longer period. More accurate data would be desirable. However, having health care providers collect data on modes of transport, engine sizes, fuel type, and distances on a permanent basis is not feasible.
It is important to note that teleconsultations are only one example of remote care. In Alentejo, the same equipment that is used for teleconsultations is also used for teleradiology and tele-education (which were not assessed here). The total impact of the telemedicine programme in Alentejo is expected to be greater than the figures reported here. Furthermore, there are other interventions beyond telemedicine which contribute to reductions in emissions (for example, mobile breast screening). 8
There is much potential to reduce GHG emissions by bringing care closer to patients. The challenge is how to integrate these benefits into technology assessments. One way is to monetize emission reductions in economic evaluations. Expectations are that the price of one tonne of carbon will cost $10 to $15 when California’s cap-and-trade scheme starts operating in 2013. 16 This is far below the €50 that analysts believe is needed to drive low carbon investments and achieve the reductions set out in the Kyoto protocol. 17 If the 455 tCO2e avoided by teleconsultations in Alentejo could be traded as certified emission reduction credits, they would be worth between $4500 and $6800. At €50 per tonne, they would be valued at €22,700. However, reducing GHG emissions is not the main rationale for remote care interventions and is rarely even considered in current technology assessments and economic evaluations. We suggest these reductions should be considered when assessing new ways of delivering care closer to patients, and that their impact is not negligible. 18 How we choose to monetize these reductions and include them in economic assessments needs exploration but if health care systems are to take action on climate change, the impact of remote care interventions on national carbon footprints must be considered.
Footnotes
Acknowledgements
We thank Manuela Rosado, José António Estrompa and the personnel at the Hospital do Espírito Santo de Évora’s Patient Management Department, Fernando Miranda, José Robalo, Hugo Quintino, Sónia Martins, Filomena Mendes and Jenny Nelson for their support and collaboration.
Funding
This research was partly funded by a doctoral grant from Fundação para a Ciência e a Tecnologia, Portugal (grant reference SFRH/BD/66305/2009). We also acknowledge the support of the UK Engineering and Physical Science Research Council’s Health and Care Infrastructure Research and Innovation Centre (HaCIRIC).