
Abstract
Qualitative research is recognized as an important method for including patients' voices and experiences in health services research and policy-making, yet the considerable potential to analyse existing qualitative data to inform health policy and practice has been little realized. This failure may partly be explained by: a lack of awareness amongst health policy makers of the increasing wealth of qualitative data available; and around 15 years of internal debates among qualitative researchers on the strengths, limitations and validity of re-use of qualitative data. Whilst acknowledging the challenges of qualitative secondary data analysis, we argue that there is a growing imperative to be pragmatic and to undertake analysis of existing qualitative data collections where they have the potential to contribute to health policy formulation. Time pressures are inherent in the policy-making process and in many circumstances it is not possible to seek funding, conduct and analyse new qualitative studies of patients' experiences in time to inform a specific policy. The danger then is that the patient voice, and the experiences of relatives and carers, is either excluded or included in a way that is easily dismissed as ‘unrepresentative’. We argue that secondary analysis of qualitative data collections may sometimes be an effective means to enable patient experiences to inform policy decision-making.
Introduction
Qualitative research is recognized as increasingly important in health services research, yet the potential for secondary analysis of qualitative data has been little realized. Conducting relatively unstructured, in-depth interviews with diverse samples is an established method for generating understanding of patients' experiences and perspectives, 1 but can be time-consuming to conduct, particularly when care is taken to sample the widest feasible range of perspectives. In contrast, a focussed secondary analysis of existing high quality qualitative data can be highly efficient, allowing effective use of researchers' time for analysis and rigorous testing of findings. 2
Two developments in prevailing research cultures particularly favor reuse of existing data. First, synthesizing published and unpublished research before (or instead of) conducting new research is now mainstream practice.3–5 Secondly, following the decision in 2000 by the Economic and Social Research Council (ESRC), a major funder of social science research in the UK, to require ‘award holders to offer for archiving and sharing copies of both digital and non-digital data to the Economic and Social Data Service’ and to seek the correct permission to do so when collecting data (p. 256), 6 several funding bodies nationally7,8 and internationally 9 have followed suit. Many now have explicit expectations that publicly-funded research should be shared to maximize the value of data for the public good and ‘to expedite the translation of research results into knowledge, products, and procedures to improve human health’. 10 A representative of one funder stated, ‘we need to ensure that research outputs are used to maximized knowledge and potential health benefits. In turn, the populations who participate in research, and the taxpayers who foot the bill, have the right to expect that every last ounce of knowledge will be wrung from the research’. 11
These directives, implicitly or explicitly, cover qualitative and quantitative data. It is often assumed that the case for quantitative data sharing is unproblematic and compelling, since these data are usually expensive to collect and can be reduced to variables which, theoretically, are equally useful to all analysts. Whilst this view sometimes does a disservice to the importance of circumstantial and contextual knowledge that primary data collectors have, a number of inherent features of qualitative data collection and analysis have been highlighted as particularly problematic in sharing and re-using qualitative data. Over the last 15 years12–16 there has been a lively, and sometimes ‘moralistic and polarised’ 17 debate among qualitative researchers. We rehearse the main features of this debate, and present two case studies using data from one archive to illustrate the potential for judicious re-use of qualitative data.
The debate about the re-use of qualitative data
Mason summarized the polarization of the debate into ‘on the one hand a position that says that qualitative data are special and cannot be re-used by others on epistemological or ethical grounds, and on the other a pragmatic or instrumental position that says that data should be open for use by others, not least because they are expensive to produce’. The former position has been well-articulated by Parry et al.14,15 who raise issues around ownership and copyright, the co-construction of data between respondent and researcher, confidentiality, preserving anonymity, and the problematic nature of gaining respondent consent for broader use of the data (particularly as all future potential uses cannot be exhaustively listed). Bishop, by contrast, has argued that there are good suggestive, but not prescriptive guidelines 18 on how to deal with several of the legal and ethical issues raised (e.g. copyright, ownership, acquiring appropriate consent, protecting confidentiality).
An issue that has generated much heat in the debate has been the extent to which the ‘context’, the insights that a researcher has through ‘being there’ in the research setting where the data were gathered, can be adequately summarized and captured for use by analysts other than the primary researcher. An interviewer may absorb aspects of the respondent's life circumstances and biography and become aware of limitations on their willingness and ability to discuss particular issues. Such details may be captured in fieldnotes, but these are often highly individual and difficult for others to make sense of, even if they are shared. Fielding 19 emphasizes the need to include as much contextual information as possible when archiving qualitative data, yet there are tensions between this need for detail and requirements to preserve anonymity. Mason argues that ‘the idea that only those involved in initial data generation can understand the context enough to interpret the data is not only anti-historical but it puts enormous epistemological weight onto the notion of “successful reflexivity” 17 but Parry et al. suggest that the ‘recovery of context can only ever be partial’ (p. 340). 15
Attempting to move the debate forwards, Mason has urged qualitative social scientists to be ‘leaders rather than laggards’ in thinking through the challenges of using and ‘re-using’ qualitative data.
17
Others question the clarity of the distinction between ‘reusing’ and ‘using’ qualitative data, emphasising instead: that all data are constituted and reconstituted within the research process;
20
that qualitative data are ‘re-contextualised and co-constructed whether reading transcripts or doing an interview in real time’;
21
continuities between ‘primary’ or ‘secondary’ data and the view that ‘secondary analysis’ can be conceptualized as ‘primary analysis of a different order of data’.
20
Irwin and Winterton suggest that a more productively drawn distinction is between data and evidence ¨ both primary and secondary analysts will construct data as evidence in the service of some empirically grounded set of arguments and knowledge claims … Presence at the point of data generation is not a final arbiter [of social scientific adequacy]. (p. 8)
22
Collections from different eras might illuminate changed orientations to health care or initiatives over time, or in different cultures. Interviews that were collected 10 or 15 years ago may be highly relevant in some respects and very dated in others – for example the people we interviewed 10 years ago talked about using the internet for health information as a marker of their unusual and particular engagement with their health decisions, whereas in recent years people describe looking for online information in an almost off hand, unremarked manner ‘we all looked it up’ ‘as anyone would’. We would not therefore recommend using decade old interviews on views of the internet to inform current digital health policy.
We believe that with due consideration of the issues addressed by Bishop 18 amongst others, problems are likely to be surmountable in all but a minority of cases.
In mixed methods studies, secondary analysis or qualitative data can offer the opportunity to help develop hypotheses quickly and efficiently, or to compare important dimensions of health care experiences (e.g. access, waiting-times, communication, information, dignity and respect) in people with different health conditions, social characteristics and biographies.
Case studies
The Health Experiences Research Group (HERG) Archive, University of Oxford: an example of a qualitative data resource for secondary analysis.
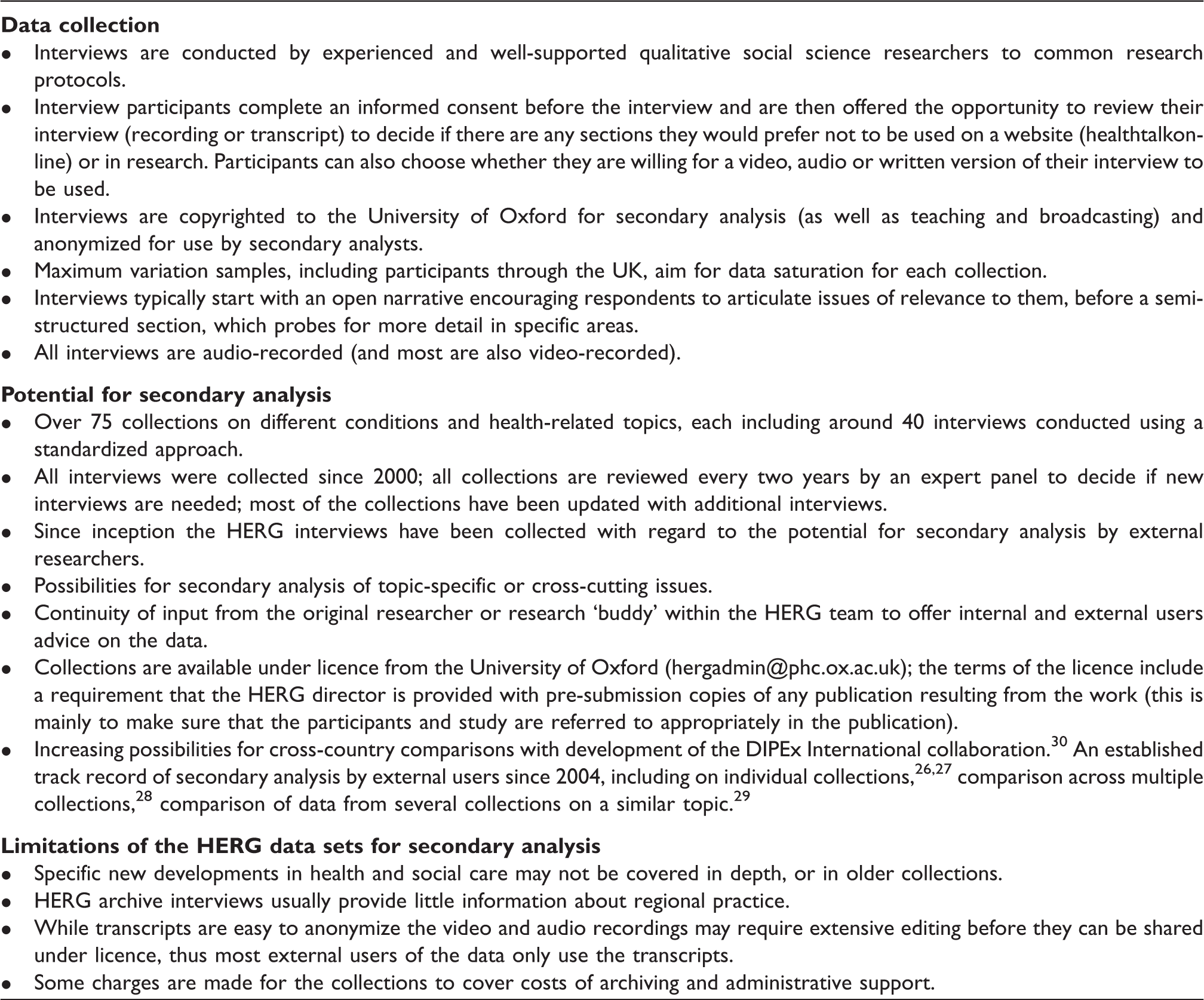
The first example was commissioned by the General Medical Council (GMC) when preparing the 2010 guidelines on end of life care. The GMC recognized the importance of including the perspectives of patients but were concerned that it could be unacceptably burdensome for patients close to the end of life to contribute and that those who could contribute might, for a variety of reasons, not represent a sufficiently wide range of the health and social care issues that are faced at the end of life. The GMC therefore commissioned HERG to undertake a secondary analysis of interviews with people at the end of life. The HERG data archive included 95 interviews, which were pertinent to end of life experiences, from patients with a range of conditions including advanced cancers, Motor Neurone Disease and COPD, and people's experiences of bereavement. The interview transcripts were analysed drawing on anticipated issues that were of interest to the GMC and additional, emergent themes. The final GMC report noted that the qualitative secondary analysis research produced a rich source of first-hand views and comments from patients and carers about the care provided towards the end of life. The findings of the research report provided greater context to many of the issues in the draft guidance, and contributed to ideas about where our implementation work should focus. (General Medical Council
23
)
Our second example is a collaboration to explore whether secondary analysis of HERG interviews could accelerate the process of experience based co-design (EBCD). EBCD uses a Participatory Action Research design which involves the ‘coupling of participation and research to action and change’. Integral to the approach, which has demonstrated positive effect 24 is that patient, carer and staff experiences are first collected by video-recorded qualitative interviews and then presented as ‘trigger films’ to groups of patients and staff who work together to co-design and improve local services. With funding from the NIHR HSD&R programme, a researcher from the Oxford group re-analysed two collections, one for which she had been the primary researcher and one in which she had had no previous involvement. Informed by this analysis, two ‘trigger films’ were compiled with excerpts from the interview video recordings. The aim of the study was to find out whether trigger films based on the existing collection of HERG interviews, as an accelerated form of EBCD, could achieve comparable results to EBCD, even though the data were not ‘local’. The accelerated approach proved readily acceptable to staff and patients; using films of nationally-gathered rather than local narratives did not adversely affect local NHS staff engagement, and may in some cases have made the process less threatening or challenging. The films served their purpose as a ‘trigger’ to discussion, and the resulting 48 co-design activities across the 4 pathways were similar in nature to those in EBCD but achieved at reduced cost. 25 Qualitative research is often thought to be highly context specific, yet in this approach to service improvement, trigger films based on existing interviews from other services and contexts were effective in stimulating change.
Discussion and Conclusions
Qualitative secondary analysis for health services research and policy.

Other selected resources with potential for qualitative secondary analysis for UK health policy research.
Increasingly, as with studies which contribute to the HERG data archive, the potential for secondary analysis needs to be carefully considered from the outset, to ensure respondents can give appropriate consent for re-use of the data.
The perspectives of researchers whose interviews may be used for secondary analysis have received little consideration in the literature. 21 Researchers in HERG are aware from the outset that the data they collect will be available, under licence, to other researchers. The original researcher has an opportunity to publish key findings first, is often involved as a consultant to a secondary analysis project and may contribute to the resulting papers. While the secondary analysis process can feel somewhat exposing, those in HERG whose data has been used by other researchers emphasize the benefits of approaching the interviews through a new analytical lens, the helpful challenge of a perspective that is more distant from the context of the original data collection and the opportunity to maximize the utility of data (especially if re-use may lead to improvements in services for the patient group).
In conclusion, it is important for policy to be evidence based and patients' experiences form a vital part of the evidence about healtaposrsquo;s experiences is not always achievable within financial or time constraints yet its exclusion can silence or marginalize the patient voice. We argue for a pragmatic approach that develops appropriate archiving practices and analytic skills among qualitative researchers so that rigorously collected qualitative data sets can be used to establish patients' perspectives at the center of health policy.
Footnotes
Acknowledgement
We are very grateful to colleagues who contributed to the November 2012 workshop on qualitative secondary analysis, especially Libby Bishop, Janet Heaton, Clive Seale, Sarah Irwin, Mandy Winterton, Emma France and Ulla Raisanen.
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the HS&DR Programme, NIHR, NHS or the Department of Health.
Funding
This project was funded by the National Institute for Health Research Health Services and Delivery Research Programme (project number 10/1011/19).