
Abstract
Following the global economic recession, health care systems have experienced intense political pressure to contain costs without compromising quality. One response is to focus on improving the continuity and coordination of care, which is seen as beneficial for both patients and providers. However, cultural and structural barriers have proved difficult to overcome in the quest to provide integrated care for entire populations. By holding groups of providers responsible for the health outcomes of a designated population, in the United States, Accountable Care Organizations are regarded as having the potential to foster collaboration across the continuum of care. They could have a similar role in England’s National Health Service. However, it is important to consider the difference in context before implementing a similar model, adapted to suit the system’s strengths. Working together, general practice federations and the Academic Health Science Networks could form the basis of accountable care in England.
The need for rapid evolutionary change
With a projected funding deficit for the NHS in England of over £30 billion by 2020 and £2 billion next year alone, policymakers are faced with the challenge of an ageing population with multiple conditions and the rising costs of paying for that care, but little or no additional resources. 1 Patients with complex multi-morbidities often require treatment that traverses traditional service boundaries. As a result, they typically receive disjointed care, inappropriate for their needs. The conflicting interests of different providers entrench organizational siloes providing episodic and hence fragmented care. Miscommunication during care transitions and duplication of services due to the lack of coordination lead to poorer clinical outcomes and wasted resources. 2 Consequently, patients receive care in expensive and overburdened hospitals when they could be better served in the community.
In order to make better use of resources, all political parties in the UK have committed to greater integration within the English National Health Service. The Labour Party established an independent commission led by Sir John Oldham, which emphasized the ‘needs of one person to be addressed by people acting as one team, from organizations behaving as one system.’ 3 Furthermore, the new Conservative government has supported integrated care initiatives with the £3.8 billion Better Care Fund operative since April 2015. 4
The appointment of Simon Stevens as chief executive of NHS England and the Five Year Forward View also throws weight behind new care delivery options to enable the English NHS to continue to provide a reasonable standard of care.
5
The majority of the models proposed are forms of integrated care organization, in particular:
Multispecialty Community Providers (MCP) – large group practices that could employ or partner with specialists alongside a wide range of nursing and therapy staff to provide outpatient, out of hours, diagnostic and other services; Primary and Acute Care Systems (PACS) – single, vertically integrated organizations permitted to provide NHS list-based GP and hospital services, together with mental health and community care services, led either by the acute hospital or multi-specialty community provider
The Five year forward review deliberately avoids providing a universal blueprint for the future, and instead acknowledges the importance of local leadership and innovation. Unlike so many similar high-profile policy reports, it has been widely praised yet it risks not being able to transform its vision to reality. This paper outlines the potential role of Accountable Care Organizations (ACOs) in the future NHS landscape and what must be considered to successfully achieve integration.
What are ACOs?
Borne out of the US 2010 Affordable Care Act, ACOs are ‘a group of providers (e.g. hospital, community health service, primary care practice) that work together to coordinate care for an assigned population of patients to deliver seamless care whilst improving quality and lowering costs.’ 6 The defining feature is that providers are collectively held accountable for achieving pre-defined outcomes within a given budget for their patient population over a period of time. 7 By fundamentally altering the payment model, it is expected that participating providers have incentives aligned to improving outcomes whilst reducing unnecessary expenditure. The adaptable nature of the scheme offers different approaches to rewarding or penalizing providers depending on the level of risk they are accountable for.
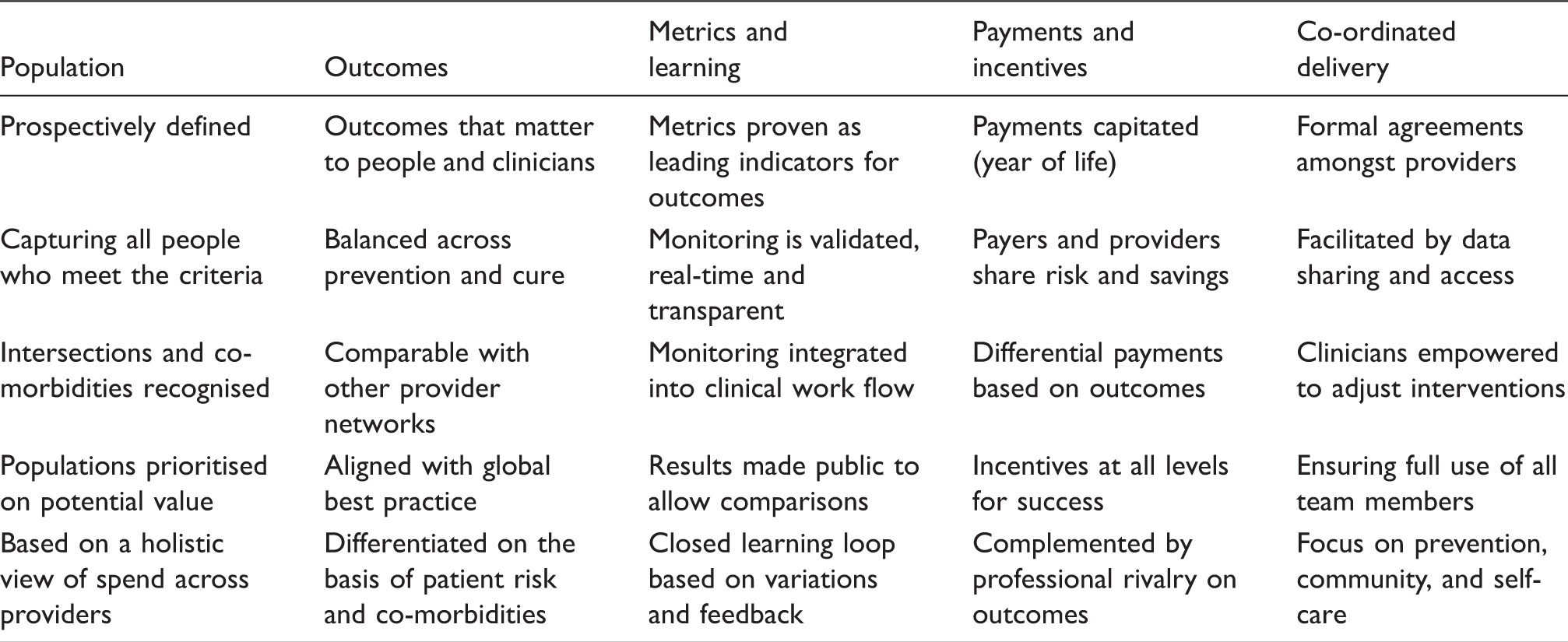
Characteristics of successful population-based accountable care systems.8
The level of success in containing costs is reliant on a range of capabilities and experience. Larger integrated delivery systems, such as Kaiser Permanente, have been more successful owing to their scale with lower start-up costs and ability to pool resources more effectively. They are well established with a long existing shared culture. NHS providers will require time and leadership if this experience is to be replicated. However, the first public performance report of the original 32 pioneer ACOs in the US produced mixed results with nearly half generating losses and two being forced to withdraw from the programme altogether. 7 Recent results have shown more promise with almost $400 million of savings across the 750 ACOs that are now estimated to cover over 20 million people. 7
ACOs have shown significant improvements in effectiveness and patients’ experiences of care particularly in relation to the management of chronic conditions. Led by the insurer Blue Cross Blue Shield, the Alternative Quality Contract in Massachusetts comprises a global budget with pay-for-performance incentives combining quality and cost targets. 8 Providers have shown annual incremental quality and cost improvements, demonstrating their long-term sustainability. Careful selection of the number and type of metrics matched with suitable incentives can be a powerful tool for promoting collaboration between different providers. By introducing downside risk, providers must make necessary arrangements between themselves to ensure resources are adequately distributed. Risk management is a differentiating factor for ACO success in the US, highlighting the need to take this into consideration when proposing any similar model in England.
What is required for an ACO to be effective in England?
Three requirements for effective ACOs, English-style, already exist, but have not been brought together in a concerted fashion. First, the need to align the incentives of multiple providers to achieve cost-effective outcomes for populations using a single, capitated outcomes-based contract. In order to develop the long-term capabilities for providers to manage risk and coordinate care, payment mechanisms must shift from incentivizing activity to capitation with an emphasis on better outcomes. Pooled budgets would facilitate greater integration between health and social care, which could potentially be governed by Health and Well-being Boards. Although capitated ACOs assume more risk, they are able to improve population health by reducing supplier-induced demand, increasing the standardization of care and encouraging greater flexibility between providers. Focusing on outcomes allows the development of new standards, sharing best practice and reduced variation, leading to lower overall costs and increased productivity.
Second, there is a need for predictive modelling to identify high-risk patients in the population and coordinate their care more effectively using case managers. Early identification and active case management of high-risk patients have the potential to improve care whilst reducing costs in the long run. This is particularly pertinent in the management of elderly people with long-term conditions who disproportionately contribute to the number of avoidable hospital admissions. 9 Information from GP registries can be collated for entire populations rather than those who have been previously admitted to hospital. NHS England’s current initiative to link primary and secondary care data can serve as a possible means of scaling up this tool to the national level. Once these high-risk populations have been identified, case managers can be used to improve the continuity of care. By adopting a population-based approach, the NHS can empower the newly formed Health and Well-being Boards to analyse the needs of entire communities through patient-centred joint strategic needs assessments to co-produce a comprehensive care plan managed by clinicians.
Finally, there is a need to develop inter-operable local electronic health records (EHRs) and encourage data sharing to be able to compare provider performance. To facilitate integration across different sectors, it is essential that data systems enable multiple providers to report and share patient information. Successful system-wide EHRs, such as Kaiser Permanente’s, can be accessed and updated by all providers enabling greater transparency and ability to coordinate care more effectively. 7 However, implementing large-scale technological changes is expensive and fraught with difficulties, causing significant disruption during the transition period. Plans for a national EHR in England were halted as the NHS ‘Connecting for Health’ programme was disbanded after more than £12 billion of expenditure over eight years. 10 Consequently, the focus has shifted towards regional EHRs to make the NHS paperless by 2018. 10 Electronic data sharing can also be used as a powerful tool for analysing and comparing provider performance. Sharing information can facilitate the development of standardized quality metrics that allow providers to compare their performance against one another. It can also help produce a range of measures to monitor progress within an ACO more accurately. 11
Who should lead the way?
The Five Year Forward View suggests accelerating the development of new ways of delivering care through a small number of test bed sites. 5 Academic Health Science Networks could serve as a potential starting point. Using the three AHSNs in London as an example, regional ACOs could develop new forms of integrated care organization closest to the PACS model in the Five year forward view. Bound by a capitated outcomes-based contractual agreement, all of the local primary and social care providers in each of the three areas could join an AHSN-ACO. Virtual, as opposed to real, integration would also avoid the complex cultural and logistical issues associated with mergers, which has led to the failure of several ACOs in the US.
While the Five Year Forward View says relatively little about local commissioners (Clinical Commissioning Groups), in areas where there are well performing PACS-style ACOs with responsibility for a wide range of services, CCGs might gradually lose their commissioning function, replaced by the AHSNs which could assume the role of commissioner and provider. However, this would require close regulation to avoid monopolies from emerging. Similar to the Alzira model in Spain, if a patient opts to seek care from a different provider outside the area, the local ACO would remain accountable for that individual’s care and bear all the costs. In addition, the ACO or other provider that receives this out-of-network patient would be remunerated depending on the level of success.
The reduced role of CCGs as commissioners could free groups of general practices to combine and achieve the necessary scale required to operate MCPs. Led by primary care providers, this alternative ACO-style model would form federations of community, social care and specialist services for a specified population. 12 Greater collaboration between primary and social care can improve the coverage and quality of out-of-hours services to reduce the need for patients to seek care from hospitals and instead receive treatment in the community. Furthermore, existing GP patient registers provides MCPs with a unique opportunity to understand the health of local populations and stratify patients by their level of risk using predictive modelling techniques. MCPs would be able to procure a variety of services best suited to their community’s needs by commissioning from other providers and delivering their own services directly.
Promise not panacea
Achieving low-cost, high-quality care remains a pressing challenge for health systems worldwide, offering the opportunity for international collaboration. The existing divide between purchasers and providers, and conflicting interests of GPs and hospital providers must be addressed in order to achieve more integrated care in England. Structural reforms under successive governments have proved a major distraction. ACOs mitigate the need for this as distinct provider organizations can still remain, bound together through risk-sharing contracts. Nevertheless, any effort to transform the diverse structures and embedded cultures that currently exist in the NHS will require the collective willpower and commitment of all relevant parties. There is neither a ‘one-size-fits-all’ approach to ACOs nor are ACOs the only solution, yet they provide a potentially viable means to realizing the principal aims of the Five Year Forward View.