
Abstract
Objective
To identify factors affecting variation in avoidable emergency admissions that are not usually identified in statistical regression.
Methods
As part of an ethnographic residual analysis, we compared six emergency and urgent care systems in England, interviewing 82 commissioners and providers of key emergency and urgent care services.
Results
There was variation between the six cases in how interviewees described three parts of their emergency and urgent care systems. First, interviewees’ descriptions revealed variation in the availability of services before patients decided to attend emergency departments. Poor availability of general practice out of hours services in some of the cases reportedly made attendance at emergency departments the easier option for patients. Second, there was variation in how interviewees described patients being dealt with during their emergency department visit in terms of availability of senior review by specialists and in coding practices when patients were at risk of breaching the NHS’s 4-hour waiting time target. Third, there was variability in services described as facilitating discharge home from emergency departments. In some cases, emergency department staff described dealing with multiple agencies in multiple localities outside the hospital, making admission the easier option. In other cases, proactive multidisciplinary rapid assessment teams were described as available to avoid admissions. Perceptions of resources available out of hours and the extent of integration between different health services, and between health and social services, also differed by case.
Conclusions
This comparative case study approach identified further factors that may affect avoidable emergency admissions. Initiatives to improve GP out of hours services, make coding more accurately reflect patient experience, increase senior review in emergency departments, offer proactive multidisciplinary admission avoidance teams, improve the availability of out of hours care in the wider emergency and urgent care system, and increase service integration may reduce avoidable admissions. Evaluation of such initiatives would be necessary before wide-scale adoption.
Introduction
Provision for emergency hospital admissions is a necessary part of any health care system but some patients may be admitted when they do not need hospital care. These unnecessary admissions may cause harm through hospital-acquired infections, distress to patients and their families, difficulties for service providers trying to balance elective and emergency care and cost pressures within resource-limited health care systems. Therefore, reducing unnecessary admission rates is important to policy makers, commissioners, service providers and patients globally.
Avoidable admissions
Identifying unnecessary emergency admissions is challenging. Researchers have focused on ‘ambulatory and primary care sensitive conditions’, where emergency admissions can be prevented through intervention in primary care. 1 Another approach identifies conditions that can be dealt with by services in the wider emergency and urgent care system to avoid hospital admission. 2 In England, services in emergency and urgent care systems include general practice services in and out of hours, emergency departments, ambulance services, community nursing and social services. For example, for some conditions, an emergency ambulance service may treat patients safely at home instead of conveying them to an emergency department where they might be admitted. An expert panel identified 14 conditions where exacerbations could be treated in the wider emergency and urgent care system without resort to a hospital bed. 2 These 14 conditions, which are rich in avoidable admissions, include non-specific chest pains, non-specific abdominal pains, chronic obstructive pulmonary disease and urinary tract infections.
Variation in emergency admissions
Considerable variation in emergency admission rates exists internationally between general practices, populations served by health care commissioners and hospitals.3–12 Exploring reasons for this variation may help to identify ways of reducing admissions and improving efficiency. 13 Variation is usually explored using statistical regression. Factors found to explain variation in age and sex-adjusted emergency admission rates include population characteristics such as deprivation and morbidity 14 and geographical characteristics such as urban/rural status 11 and distance to hospital. 9 When testing the effect of service characteristics on emergency admission rates, researchers have tended to focus on the availability, accessibility and quality of general practice and the characteristics of hospitals. General practice characteristics have explained only small amounts of variation in emergency admission rates; evidence is consistent that continuity of care by a general practitioner reduces emergency admission rates. 14
Our recent research moved beyond this focus on general practice and hospitals by testing the effect of characteristics of services in the wider emergency and urgent care system on emergency admission rates. We considered avoidable emergency admissions rather than all emergency admissions, defined as admissions from the 14 conditions identified by an expert panel as described earlier. We identified four-fold variation in avoidable admission rates between different emergency and urgent care systems in England and found that as well as factors usually identified as explaining variation, characteristics of ambulance services and emergency departments also explained small amounts of variation.11,12
Quantitative approaches to exploring variation in emergency admission rates can only test factors where there are data available and may miss other important factors. The aim of this study was to use qualitative research to identify further factors that might explain variation in avoidable admission rates.
Methods
Wider mixed methods study
We report the findings from the qualitative component of a wider mixed methods study. We briefly describe the wider study here to put the qualitative study in context. We used a mixed methods design known as ethnographic residual analysis. 15 The first phase involved undertaking a regression to identify factors affecting variation in age and sex-adjusted avoidable emergency admission rates in 150 systems in England. Systems were defined by the emergency and urgent care services used by geographic populations served by the NHS health care commissioning bodies known as primary care trusts at the time of the data collection (2011–2013). The results of this regression are reported elsewhere. 11 In summary, systems with high avoidable admission rates were associated with high levels of deprivation, urban areas, high percentages of short-stay patients, high rates of emergency department attendances, high conversion rates from emergency department attendance to admission, low non-conveyance rates by the ambulance service and high levels of perceived access to a GP within 48 hours. 11 A further analysis of acute hospitals identified that high-avoidable admission rates were associated with high numbers of beds. 12
The second phase of the wider mixed methods study involved identifying emergency and urgent care systems that the regression did not fit and undertaking case studies of a sample of these to identify further factors that might affect avoidable emergency admission rates. Twenty-seven of the 150 systems had large residuals in the regression and were candidate systems for our case studies. We selected six systems and used a multiple case study design, 16 undertaking qualitative interviews with stakeholders within each system. We obtained ethics approval for the study from the National Research Ethics Service Committee Yorkshire and the Humber 11/YH/0400.
Sampling the six emergency and urgent care systems
We sought diversity when sampling our six cases in terms of size of avoidable admission rate and direction of lack of prediction in the regression. We ordered the 27 cases with large residuals into six groups of high, medium and low-avoidable admission rates, which were either over- or under-predicted in the regression. Our intention was to select one case from each of these six categories, but some categories had no cases. We selected cases from all categories with cases in them. Some of the 27 cases were geographically clustered, so we selected only one from each cluster because we assumed that similar issues might affect cases within the same geographical area.
Qualitative interviews within each case
We undertook semi-structured, face-to-face and telephone interviews with commissioners of health services, providers of the range of health and social services in each emergency and urgent care system and local representatives of a national patient advocacy group. Each stakeholder was contacted by email and formally invited to participate in the study. Our intention was to undertake around 15 interviews per case, totalling 90 interviews. EK began the interviews by clearly explaining the geographic population we were interested in and the health conditions we had used to calculate the avoidable admission rates. The interviews covered perceptions of key drivers of potentially avoidable admissions within both the interviewees’ organization and the emergency and urgent care system used by the relevant population. A topic guide was developed based on our research objectives and piloted in the first few interviews (see additional file). Written informed consent was gained. Interviews were digitally recorded with permission and lasted around 60 minutes. We offered remuneration to the organization (not the individual) for the time given for the interview.
Analysis
Interviews were transcribed verbatim. Analysis was undertaken in three stages. First, AOC wrote a summary of each case based on reading 6–10 transcripts within a case. The aim was to describe the case and consider why it had been over- or under-predicted in the regression. Each summary was discussed by the research team and compared and contrasted with subsequent case summaries. Second, we analysed all the interviews using framework analysis. 17 AOC and EK developed a thematic framework based on the issues identified in our case summaries. EK coded transcripts to these themes using NVivo 10. EK and AOC read data extractions related to a theme and identified within-case perceptions of that issue in preparation for the multiple-case analysis. Third, AOC and EK summarized findings for each case for each theme to facilitate multiple case study analysis. 16 We used pattern-matching logic 16 to look for cross-case patterns, particularly issues that appeared distinctly in one type of case (e.g. under-predicted rate) and not another (e.g. over-predicted rate). Rather than attempting to categorize each case for each variable, we only identified cases where we were confident of a distinct difference in the ways in which interviewees described aspects of their system.
Results
Description of cases and interviewees
Variation between six emergency and urgent care systems.

Rank is 1 = lowest and 150 = highest.
Standardized for age, sex and deprivation.
Types of interviewees in each case.

Not applicable.
Overview of findings
There was variation between the six case studies in how interviewees described factors affecting avoidable emergency admissions. These factors operated in three parts of the emergency and urgent care system: first, before patients made the decision to attend an emergency department, where the availability or actions of alternative services in the system affected rates of attendance at emergency departments; second, during the visit to an emergency department, where availability or actions of hospital staff affected admission rates; and third, after emergency department investigations when emergency department staff wanted to discharge patients from the department, but the availability and actions of services in the wider system affected admission rates (Figure 1).
Admission avoidance in three parts of the emergency and urgent care system.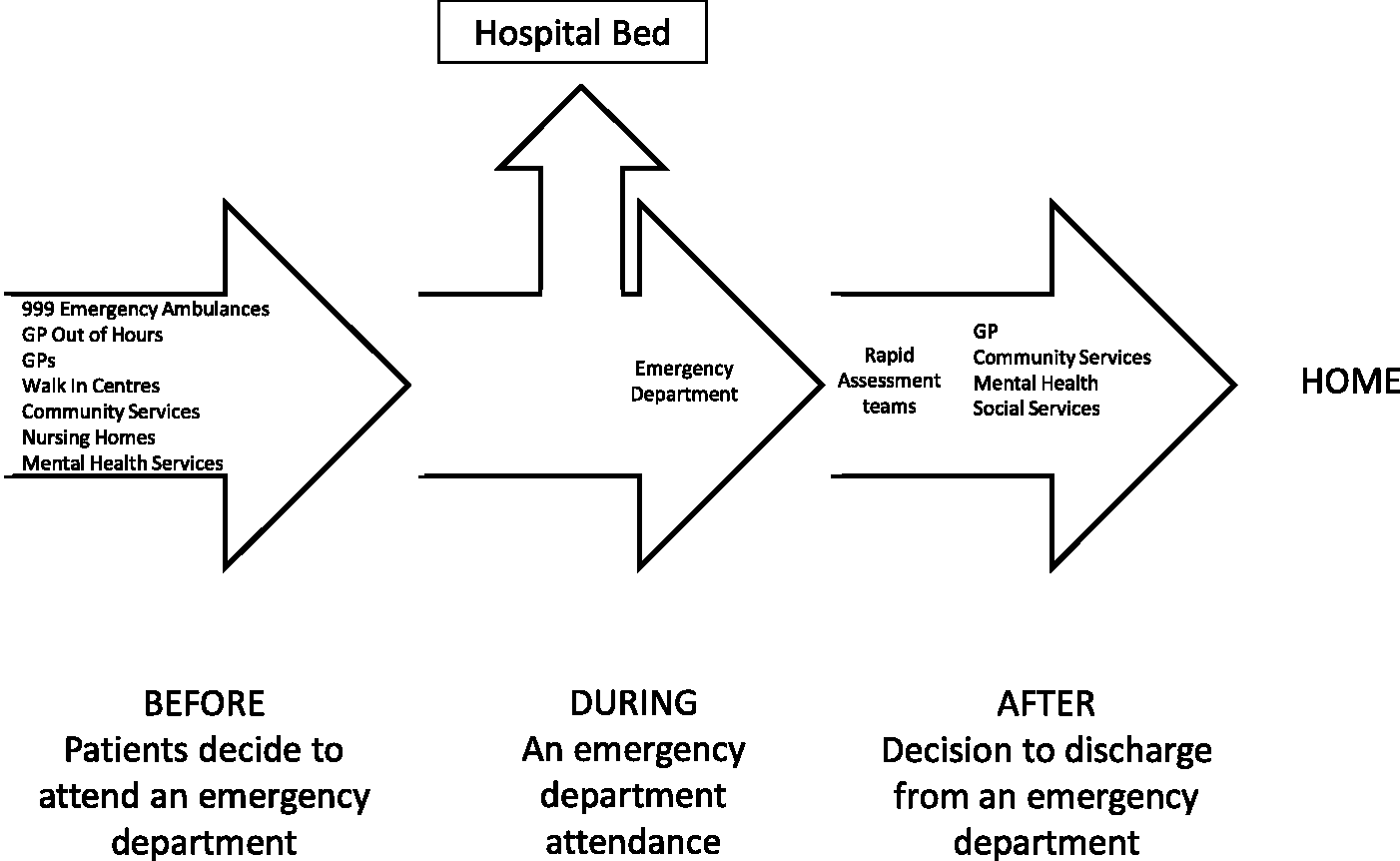
Factors affecting avoidable admissions before attendance at an emergency department
The evidence shows that higher emergency admission rates are associated with patient perceptions of poor accessibility to general practice. In the regression, we added to this evidence by identifying that systems where ambulance services treated patients without taking them to an emergency department had lower avoidable admission rates. 11 Our case studies added further to the evidence base because there was variation in how interviewees described the availability and actions of GP out of hours services (Table 1). GP out of hours services were criticized in all six systems for relying on locums from outside the area who did not know local services enough to access alternative services or have the commitment to invest their time in avoiding unnecessary admissions. Interviewees from rural systems discussed the challenges of offering this service across a wide geographical area (LO2, MU4). However, in one of our cases (MU4), interviewees expressed much more concern about this service than in the other cases. This was one of the two cases with higher admission rates than could be explained in the regression.
Factors affecting avoidable admissions during attendance at an emergency department
Previous research has generally not addressed factors operating within the hospital that affect admission avoidance. In the regression in the wider mixed methods study, we found that high-avoidable admission rates were associated with high conversion rates from emergency department attendance to admission and high rates of short stay patients. 11 In the case studies, interviewees described how management within emergency departments varied by case in terms of availability of senior review and the consequences of attempts to avoid breaching NHS waiting time targets (Table 1). These characteristics of services were important because interviewees described how, once people attended an emergency department, the chance of being admitted unnecessarily was dependent on systems within the hospital and its emergency department. Interviewees described busy emergency departments relying on decision making by junior doctors. Inexperienced doctors ordered multiple diagnostic tests that took time to deliver results. While patients waited for diagnostics, there was a risk of breaching the ‘4-hour target’ for waiting in an emergency department. Hospital admission was sometimes used by doctors to avoid such breaches. That is, hospital admission was seen as a better option than contributing to the hospital being in breach of a target. It was also considered likely that multiple diagnostic tests – which interviewees suggested that a senior doctor might not order – could identify something that required further investigation, increasing the length of time a patient stayed within the department. Additionally, requests for advice from doctors in medical and surgical specialities in the wider hospital could be met by junior doctors who admitted rather than discharged patients because this was the safer option for them in the light of their lack of experience. In contrast, senior doctors were described as being more confident about discharging patients from emergency departments, starting the discharge process earlier than junior colleagues or identifying those needing diagnostic tests earlier.
Availability of senior review
There was variation between cases in how hospital-based interviewees described availability of senior review within emergency departments and the wider hospital. In the two cases with higher admission rates than predicted (HU1, MU4), interviewees discussed a severe shortage of emergency department specialists. In contrast, in other cases, there was an emphasis on senior review from emergency department consultants (LO5) or appreciation of timely senior review from colleagues in the wider hospital environment in medicine and surgery (MO6).
Coding of admissions
We found extreme differences in reported coding practices within hospitals in two of our cases (Table 1). In HU1, our interviewees described how emergency department attendances, which risked breaching 4-hour targets in the emergency department, were moved to another unit to await the outcome of their diagnostic tests. These were coded as admissions even if they stayed on a chair in the unit for 1 hour. In MO6, interviewees also described patients at risk of breaching the 4-hour target being moved to another unit. However, interviewees reported that these were not coded as admissions even if they stayed overnight in a bed in that unit. The incentive for both cases to move patients out of the emergency department was similar: to avoid penalties for their hospital if an emergency department target was not met. The incentive for coding practices in HU1 was reported to be a need to keep admissions high to fund the hospital’s private finance initiative debt repayments. That is, hospital admission on paper was seen as the better option financially for the hospital. ‘all our patients that stay in the [emergency] department beyond 4 hours are called admissions […] but they would still count on a Trust basis as an admission, although they would zbe a less than 24 hours stay. […] [pause], you’ve avoided admission into the main hospital but you haven’t avoided a nominal admission’. (HU1) ‘And they specifically set up [the unit] for admission avoidance. Now they are admitted in the traditional sense, they are on a ward, but […] not on the main-stream hospital, not in the investigation part, they’re there purely for the purpose of getting them back where they came from’. (MO6)
Factors affecting avoidable admissions after attendance at an emergency department
The evidence does not include factors in the wider emergency and urgent care system that affect whether patients can leave emergency departments when they are considered to be medically fit for discharge. In the regression, we could not locate quantitative data on characteristics of this part of the system. 11 In the case studies, interviewees described how discharge from emergency departments could be facilitated by timely access to services such as community beds, community nursing, mental health services and social services, especially out of hours. However, interviewees’ descriptions of the availability and actions of these services differed by case in terms of the complexity of the emergency and urgent care system, the schemes focused on facilitating discharge from emergency departments, the availability of resources and the level of integration between services (Table 1).
Complexity of systems
Interviewees’ descriptions of some emergency and urgent care systems were that they were so complex that emergency admission was easier than discharge from the emergency department. By contrast, MO6 was a relatively simple system. The population mainly attended a single hospital for emergencies and was the primary source of emergency admissions for that hospital. Therefore, there was an incentive for staff at that hospital to undertake admission avoidance work with services for that population. It was relatively easy to do this because there was a single community health services provider and local authority with which to develop relationships. It was very different in HU1 and LO5 where the populations of these systems attended two hospitals that took patients from a number of emergency and urgent care systems, so that staff had to develop schemes and relationships with a large number of community, mental and social care services in different systems in order to avoid admissions. This was particularly complex for HU1 where both hospitals were based outside the geographical boundaries of the system population. The HU1 population was not the primary population for either of the two hospitals it used, and hence there was no incentive for staff in any hospital to develop schemes with community services to make discharge from emergency departments an easier option than admission.
Proactive multidisciplinary teams
There was variation in the reported availability of proactive admission avoidance schemes using multidisciplinary teams (LO2, MO3, LO5, MO6; see Table 1). These teams – sometimes called rapid assessment teams – included community nursing, physiotherapy, occupational therapy and sometimes social services. They actively sought out patients attending the hospital (particularly emergency departments) and organized all the facilities and visits required for safe discharge home in a time scale that suited the hospital staff. These multidisciplinary teams offered an integrated approach to service delivery, especially if they included social services. Interviewees identified a key characteristic of these teams as being proactive to avoid admissions, thus making it easier for staff to use them than admit to a hospital bed. In one system, where the population used two hospitals, which ran the same type of scheme (LO5), one scheme was described as successful at admission avoidance and the other not because the latter scheme required staff to make the effort to use it: ‘[name of acute trust] as an organisation were not as proactive’ (Community service). In contrast, in HU1, a similar type of team was described, which focused on discharge from a hospital bed rather than discharge from the emergency department to avoid admissions in the first place.
Resources within a system
There was variation in how interviewees described the resources available in the different systems for avoiding admission after attendance at an emergency department (Table 1). Lack of availability of a range of alternative services that might be available during normal working hours (weekdays 9 am to 5 pm) made hospital admission the easier option during evenings and weekends. Interviewees were more likely to express concerns in HU1, MU4 and LO5.
Level of integration between services
Admission avoidance often depended on collaboration between different health services (primary, secondary, community and emergency care) and between these health services and social services. There was variation in how the interviewees described integration of services in their systems (Table 1). Interviewees described historical integration embedded in their work practices in LO2, whereas HU1 interviewees described their system as fragmented. In other systems, integration was described as working well between some partners only (e.g. between health and social care, but not between the acute hospital and community care).
Discussion
Summary of findings
Interviewees in different emergency and urgent care systems described how services operated to avoid emergency admissions in three parts of their systems: before patients attended emergency departments; within the hospital when patients attended emergency departments; and in the wider emergency and urgent care system when patients were deemed medically fit for discharge from an emergency department. Two cases had avoidable admission rates that were higher than predicted in the regression in our wider mixed methods study, and, in both of these, interviewees described considerable problems with a range of factors not tested in the regression. The case with a very high-avoidable admission rate, much higher than could be predicted in the regression, was described by commissioners and providers as having multiple problems, which interviewees associated with avoidable admissions: lack of senior review in the emergency department, coding practices which increased the numbers of emergency department attendances coded as admissions, a focus on early discharge from a bed rather than admission avoidance, a complex system where its population was not the primary population for any acute hospital, a lack of services out of hours and fragmentation rather than integration between services within the system. The other case with a higher rate than predicted in the regression was described as having a poor GP out of hours service, a lack of senior review from emergency department specialists, poor availability of out of hours services and weak integration between services. Some of these problems were described in the other four cases where admission rates were lower than could be predicted in the regression, but not were not described as severe and were always accompanied by compensatory factors in that they were perceived to perform well in terms of senior review or coding practices, etc. These factors tend not to be included in statistical regressions due to a lack of data.
Findings in the context of other research
Two initiatives were well-regarded in our study – senior review and proactive rapid assessment teams. These have not been evaluated with randomized controlled trials, 18 but some evidence from a non-randomized study shows that rapid assessment teams appear to offer a very small reduction in emergency admissions. 19 A type of senior review scheme has identified a lower conversion rate to admission, again using a non-randomized design. 20 Also, a scheme to integrate systems within a hospital, including early decision making by senior clinicians, has been shown to reduce emergency admissions. 21 It is important to evaluate these types of schemes using randomized controlled designs if possible, because, in practice, they may have little impact on emergency admission rates. 22 Finally, it has been found that some emergency and urgent care systems receive less money than their target allocation based on population and need. 23 That is, resource shortages affect different emergency and urgent care systems to different extents.
Strengths, limitations and reflexivity
The strength of this qualitative study was that it provided a rigorous and systematic approach to identifying further potential explanatory factors for avoidable emergency admissions. In addition, it moved beyond quantitative exploration of variation in emergency admissions to understand how factors affected avoidable emergency admissions. A limitation was that the case studies focused largely on the views of managers and health professionals rather than patients. We attempted to include a patient advocacy group in each case study to offer a patient perspective but because this organization was being set up during our study, we only managed to undertake two interviews out of the six planned. Therefore, the study offers the health and social care professional voice, with little understanding of how patients and their families viewed factors affecting avoidable admissions in the different cases. A further limitation was that the case studies drew on interviews when it is usual to combine data sources such as interviews, observation and documentary analysis. 16 We undertook documentary analysis 24 but it added little to the case studies. We took the views of interviewees as valid individual perceptions of a system, but interviewees may have given accounts to show themselves or their service in a good light, while finding fault with others. This is unlikely to have affected variation between cases. However, variation was judged subjectively. We did not send a summary of each case to interviewees for respondent validation. Additionally, our aim was to engage with the breadth of stakeholders within each system, at the cost of some depth that could have been achieved through non-participant observation. Finally, the data were collected in England in 2012–2013. National health and social care systems differ, so the findings may only be transferable to other countries with similar health care systems.
We have undertaken a large amount of research about emergency and urgent care as ‘systems’. It is a concept we support but it may not be one that is supported by others. Therefore, we allowed our interviewees the opportunity to offer different perspectives of factors affecting avoidable admissions and indeed disagree with our definition of avoidable admissions. Interviewees engaged and agreed with the concept of a system and our definition of avoidable admissions. On reflection, although we interviewed some staff from GP admission units and the majority of admissions occur through emergency departments. The interviews were weighted towards emergency department views in terms of the numbers of interviews. This might have resulted in too much emphasis given to emergency departments in the analysis.
We found the ethnographic residual analysis approach helpful because it identified cases where it was most likely that further factors would emerge. The final step in this approach is to look for further quantitative data to measure the newly identified factors in a regression. Our attempts to do that were rarely successful, and indeed, some of these factors were already included in the regression in some way. 24 For example, the conversion rate from emergency department attendance to admission was already in the regression and is likely to be correlated with the availability of senior review.
Implications
There is a need to evaluate robustly schemes that health care staff perceive make alternatives to a hospital admission the easier option, such as senior review and proactive admission avoidance schemes. Quantitative data are not accessible for some key services in the emergency and urgent care system, such as GP out of hours services, and these should be made available to allow understanding of the impact of the availability and quality of this service on emergency admission rates. In addition, some systems may have more structural barriers to admission avoidance than others because their system populations are not the primary source of emergency admissions for any acute hospital. These systems may need extra support to establish admission avoidance schemes.
Conclusions
This multiple case study approach identified further factors that may affect avoidable emergency admissions. Initiatives to improve GP out of hours services, make coding more accurately reflect patient experience, increase senior review in emergency departments, offer proactive multidisciplinary admission avoidance teams, improve the availability of out of hours care in the wider emergency and urgent care system and increase integration between services may reduce avoidable admissions. However, evaluation of such initiatives would be necessary before wide-scale adoption.
Footnotes
Acknowledgements
We would like to thank Colin O’Keefe for help with the data coding, all the interviewees for giving their valuable time for the study and the reviewers for offering extremely insightful advice.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was funded by the National Institute for Health Research Health Services and Delivery Research Programme (project number 10/1010/08). The views and opinions expressed in this article are those of the authors and do not necessarily reflect those of the HS&DR Programme, NIHR, NHS or the Department of Health.