
Abstract
Objectives
Fast tracking is one strategy that organizations use to ameliorate workforce shortfalls by attracting new recruits, and accelerating their skills development and experience. In response to the Government’s target of rapidly expanding the number of health visitors in England’s National Health Service, the fast track initiative was launched to recruit newly qualified (fast track) as well as experienced (standard entry) nurses and midwives onto health visiting programmes. This paper evaluates the fast track initiative, from the perspective of fast track and standard entry students, practice teachers and health visitor managers.
Methods
A mixed methods design was used comprising a questionnaire survey (n = 71 students), semi-structured interviews (n = 37 students), telephone interviews (n = 13 managers) and six focus groups (n = 24 practice teachers). Data were collected between April 2012 and July 2013. Descriptive statistics, t-tests and the Pearson Chi-square test were used to analyse the quantitative data. The qualitative data were analysed thematically.
Results
Motivations for health visiting as a career choice were similar for fast track and standard entry students, with career progression and interest in health promotion being key motivators. There was consensus that personal qualities and characteristics were more important than experience or qualifications. However, fast track students were significantly less confident about their public health competencies in leadership and management (p < 0.05) and communication (p < 0.02). Practice teachers and managers also reported that fast track students required more intensive supervision particularly at the beginning of the programme. Programme completion including pass rates and academic achievement showed no significant difference by route of entry (p > 0.5).
Conclusion
Fast tracking offers a useful recruitment strategy in order to expand the health visitor workforce, but longitudinal research is needed to confirm benefits such as retention and career trajectories.
Introduction
Many professions experience challenges recruiting and retaining appropriate high-calibre individuals. Fast tracking is one strategy that organizations use to ameliorate workforce shortfalls by attracting new talent, and accelerating the skills development and experience of recruits through a planned programme of enhanced opportunities. 1 Adopted initially in the private sector with a focus on increasing leadership capability, fast tracking is increasingly being used to attract entry level recruits into the health and social care professions.2–4
While fast track (FT) initiatives vary widely in design, context and duration, there are a number of common features: selection of individuals with high potential; development of individuals within a condensed timeframe; and privileged access to resources, including reward and benefit schemes.4,5 Equally important are the associated risks, for example: investment of resources may not yield desired outcomes (e.g. retention); raised expectations and an enhanced sense of entitlement among fast trackers which are not fulfilled; alienation or demotivation of non-fast tracked staff; and a mismatch between the readiness of fast trackers and the level of responsibility they are awarded.6,7
In England, the Government announced that an additional 4200 health visitors needed to be recruited between 2011 and 2015 to meet policy targets set out within the Health Visitor Implementation Plan. 8 This paper evaluates the FT initiative implemented as one approach to increase recruitment.
Health visiting in the UK
Health visitors are registered nurses or midwives with a further specialist public health nursing qualification and are central to the Government’s policy for the early years and safeguarding children agenda. 9 In particular, health visitors are recognized as key to the successful delivery of England’s Healthy Child Programme launched in 2004.8,10 This universal preventive programme aims to promote and protect children’s health and wellbeing and raise the achievement of disadvantaged children through additional services focussed on the most vulnerable families. 10
Health visiting programme
As a specialist role requiring advanced skills, experienced nurses and midwives have been the traditional recruits onto health visiting programmes. The programme comprises equal time spent in university-based education and practice (52 weeks full-time), which together prepares students to achieve the proficiencies required by the statutory regulatory body – the Nursing and Midwifery Council (NMC). Practice teachers are pivotal to the education of student health visitors. They are registered health visitors with a minimum of seven years’ experience who design the students’ practice learning and conduct assessments of their professional development in community health care settings. At the end of the students’ programme practice, teachers, who are prepared for their teaching role through a range of educational programmes, are accountable for certifying competence prior to students’ registration with the NMC. 11
The health visiting workforce
Placing health visitors in the vanguard of delivering the Healthy Child Programme has presented a number of challenges due to persistent workforce issues facing the profession when the Government’s strategy was launched, notably:
Decreasing numbers of health visitors from approximately 10,500 full-time equivalents (FTEs) in 1999 to 8000 in 2010.
12
An ageing workforce with 23% of health visitors eligible to retire.
8
A falling number of recruits resulting in commissioned places not being filled.
13
Increasing attrition rates due to, for example, lower salaries compared to other clinical specialist roles and rising levels of stress within the diminishing workforce.
14
The FT initiative
In 2011, the Government set a target to increase the health visitor workforce from approximately 8000 FTE post-holders to 12,000 FTEs by 2015. 15 To drive this growth, places for health visiting students, who are salaried during training, were increased from 500 in 2010 to 2787 in 2013: an increase of over 400%. 16 In an attempt to meet this target, the FT initiative was introduced, which suspended the requirement of post-qualification experience as a registered nurse or midwife before enrolling on a health visiting programme.
The projected growth of the profession means that by 2016 over 50% of the health visiting workforce will have been qualified for less than five years and many will have entered the profession through a FT route. Such rapid expansion has widespread implications, which are potentially compounded when recruitment strategies are deployed attracting not only a new type of recruit (newly qualified), but when such new recruits are also required to complete the same programme of preparation in terms of content, duration, support and assessment. This paper reports the evaluation of a single FT initiative which recruited both newly qualified (fast track (FT)) and experienced (standard entry (SE)) nurses and midwives onto an established health visiting programme.
Aim and objectives
The study’s aim was to evaluate the FT initiative from the perspective of students (both FT and SE), practice teachers and health visitor managers. The study objectives were to explore and compare:
FT and SE students’ motivations for choosing health visiting. FT and SE students’ experience of undertaking a health visitor programme. FT and SE students’ self-reported public health competencies. Practice teachers’ experiences of supervising student health visitors. Health visitor managers’ perspectives on the FT initiative.
Method
Design
A mixed methods design comprising a self-completed questionnaire survey, focus groups, and semi-structured face-to-face and telephone interviews was used. Participants were key stakeholders in a health visiting programme based in one higher education institution (HEI) collaborating with 12 sponsoring NHS Trusts serving communities in both inner city and urban areas. Data were collected between April 2012 and July 2013.
Sample recruitment
All students (n = 40 FT, n = 87 SE) enrolled on two intakes of the health visiting programme (commencing September 2011 and 2012) were invited to participate in the study by returning a questionnaire and taking part in a face-to-face interview. Seventy-one questionnaires were returned (21 FT (53%), 50 SE (57%)) and 37 students agreed to be interviewed (16 FT (40%), 21 SE (24%)). Twenty-four practice teachers were recruited to one of six focus groups while attending a programme meeting at the HEI. Seven had supervised FT students. Using a database maintained by the programme team, 23 health visitor managers were contacted and 13 completed telephone interviews (all but one had line managed FT students). No attempt was made to map the data from practice teachers and managers to individual students whom they had supervised/line managed due to student anonymity.
Instrumentation
The questionnaire comprised two 5-point Likert scales (5 = strongly agree, 1 = strongly disagree on: (i) reasons for a change in career pathway: 12 items 17 and (ii) self-perceived public health nursing competencies: 54 items. 18 Three researcher-developed topic guides were used to collect data during semi-structured interviews with students and managers and focus groups with practice teachers.
Analysis
The questionnaire data were analysed using SPSS version 21.0. In view of the sample size and small cell sizes for some responses, data on career change were analysed using descriptive statistics for strongly agree/agree only. The principal components analysis of the competencies scale undertaken by Poulton and McCammon 18 successfully loaded 52 items in three dimensions, each with Cronbach alpha coefficients of .85 or higher: (i) leadership and management for public health; (ii) principles and practice of public health; and (iii) communication. The t-test was used to detect significant differences (p < 0.05) by route of entry (i.e. FT, SE) for both dimension and item scores. Differences in programme completion and academic performance by route of entry were examined using the Pearson Chi-square test.
Contemporaneous note taking was used to record interviews and focus group data which were analysed thematically. Analysis was verified independently by two researchers. During analysis differences and similarities in the participants’ responses by, or about FT and SE students were noted in order to meet the study’s aim and objectives.
Ethical considerations
Ethical approval was granted by the King’s College London Research Ethics Committee. Written consent was obtained for face-to-face data collection with participants. Completion of questionnaires and participation in telephone interviews was taken as consent to participate. Student interviews were conducted by staff not involved in the delivery of the health visiting programme.
Results
Motivations for health visiting
Motivation for changing career direction by route of entry.
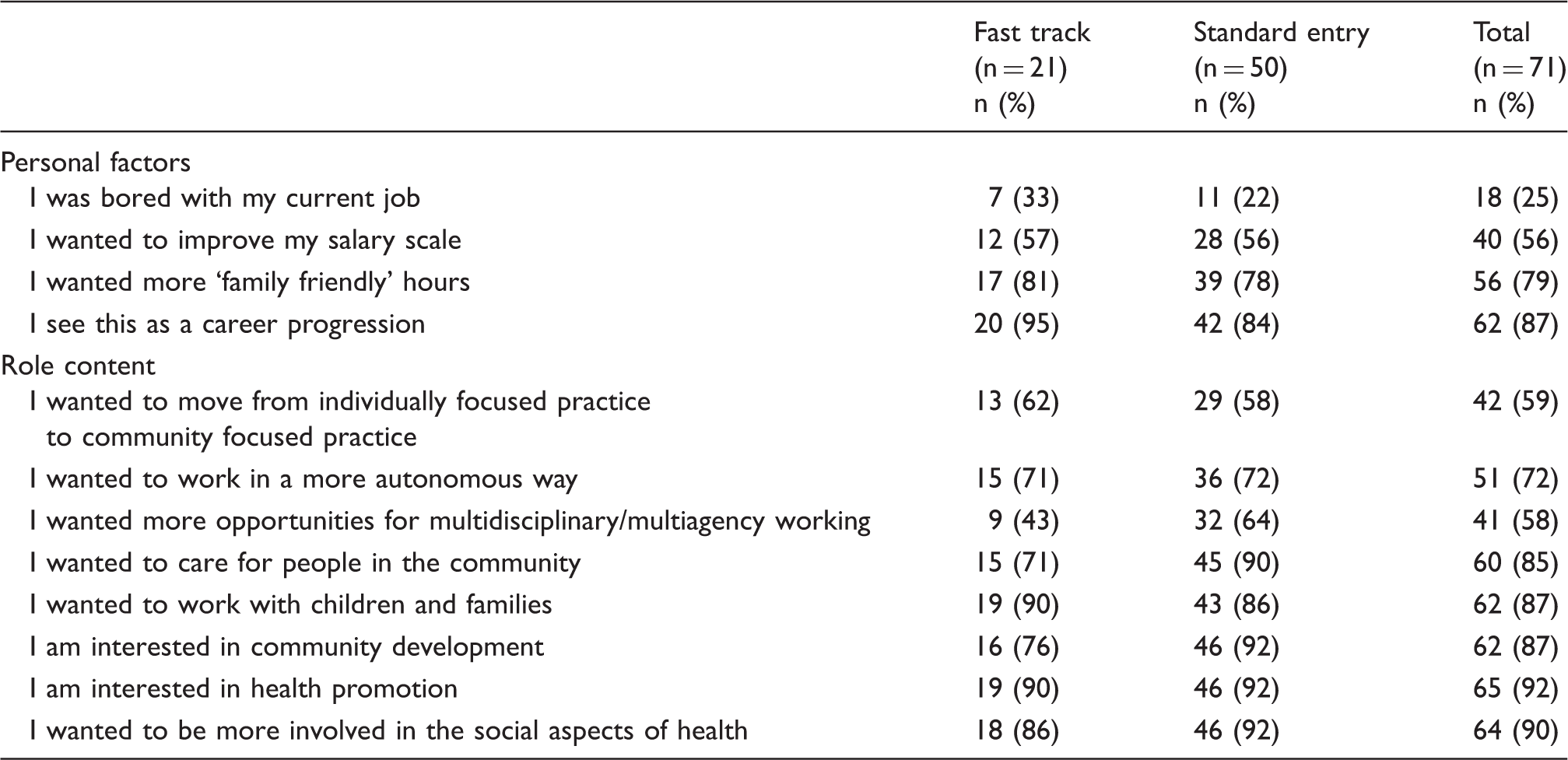
In terms of identifying health visiting as a potential career option, exposure to the role emerged as a key influence. Twenty-one of the interviewed students had either worked previously in a community setting involving contact with health visitors (n = 8) or had completed a placement in the community and/or specifically with health visitors (n = 13) as part of their initial training programme as a nurse or midwife. While for some the experience had confirmed their interest in becoming a health visitor, others stated that such exposure had sparked interest in a previously unknown career option.
The right person for the job
Selecting appropriate recruits was a theme highlighted by all participants (students, practice teachers and managers), and there was consensus that it was the attributes of the individual which marked them out as suited to the role of a health visitor and provided the foundation on which preparation for the role was built. The personal qualities and skills deemed important by both groups of students were ‘empathy’, ‘sensitivity’, ‘commitment’ and ‘resilience’, which were not always seen to correlate with professional experience. The FT students also emphasized the need to have an enquiring mind, sound academic skills, and the ability to question and challenge practice as well as apply evidence to practice.
The SE students articulated important professional attributes that perhaps reflect a more subtle appreciation of the work of health visitors. These included the need to make decisions, manage conflict and work effectively within a team, as well as the ability to ‘engage with families who find services hard to reach’, ‘decisive’ and ‘self-assured in complex situations’, and work alone and autonomously within the ‘dynamics of a team’.
The importance of recruiting the ‘right people’ rather than those with the ‘right qualifications’ resonated with both the practice teachers and managers. The importance of effective communication skills and personal attributes such as self-motivation, adaptability and empathy, rather than the issue of experience per se emerged from the focus group discussions. This was particularly illustrated by the descriptors that practice teachers with experience of supervising FT students used to describe their students: ‘highly motivated’, ‘willing to learn’, ‘adaptable’ and ‘inquisitive’ and, in this respect, ‘rewarding to supervise’.
Similarly, there was consensus among the managers that it was the individual and the attributes of applicants which were important rather than the length of professional experience. While a mixed picture emerged regarding the extent to which the FT students possessed the attributes required, some managers were explicit in their praise of the calibre of the new recruits in terms of their: enthusiasm and commitment; knowledge of research, evidence and policy underpinning practice; and ability to process information ‘to make sense of what they are hearing and seeing’.
Role preparation
Dimensions of public health competency by route of entry.
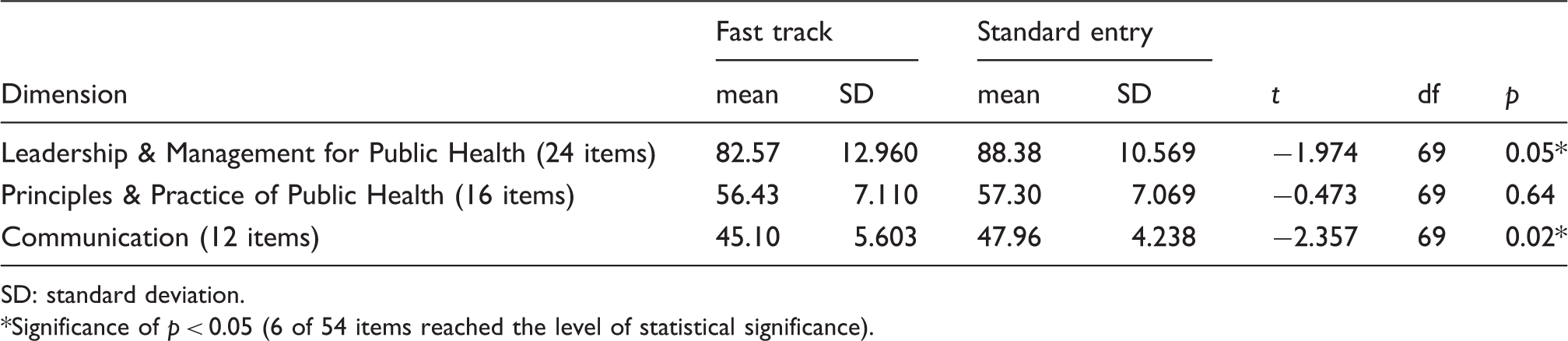
SD: standard deviation.
Significance of p < 0.05 (6 of 54 items reached the level of statistical significance).
Some SE students viewed the rapid career progression afforded FT students as having the potential to attract newly qualified nurses and midwives into health visiting for the wrong reasons such as being motivated by the salary rather than the role. However, this perspective was not confirmed by the questionnaire data (Table 1), and most SE students identified the potential benefits of a wider recruitment base. While they acknowledged that there may be additional gaps in knowledge to address in practice for FT students, SE students also reported that health visiting needs to ‘capitalise on the benefits they bring’ and frequently used the following descriptors: ‘capable’; ‘enthusiastic’; ‘bringing a fresh approach’; ‘optimistic’; and ‘less judgemental’.
Programme completion
Programme performance by route of entry.
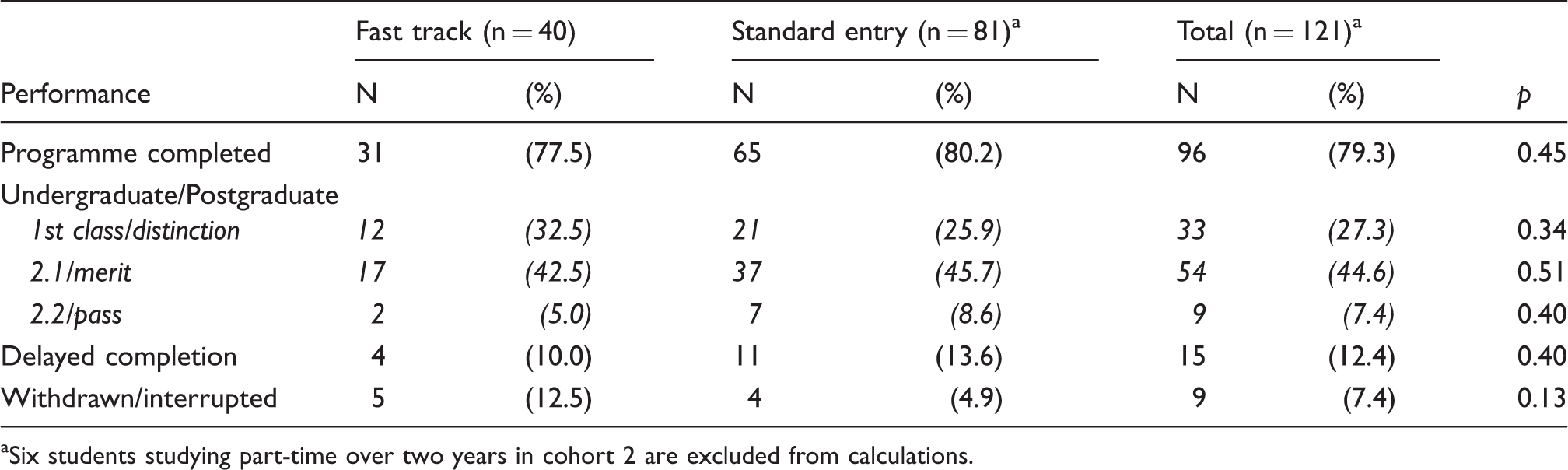
Six students studying part-time over two years in cohort 2 are excluded from calculations.
All study participants agreed that there was a need for a period of preceptorship to support the transition from student to health visitor irrespective of route of entry. There was no agreement by practice teachers or managers whether the FT graduates would need more intense or longer support but they acknowledged the possible resource implications as well as the need to manage all newly qualified health visitors equally as employees. Both the FT and SE students were optimistic about being a qualified health visitor and stated that they intended to be in a health visiting role for at least the next two years, with many setting out personal career targets of achieving promotion and/or moving to a specialized role.
Discussion
Fast tracking is increasingly being used in the professions to address shortfalls in staffing and to widen the recruitment base to attract high-calibre individuals, although published research evaluating their effectiveness is limited.6,7 The current evaluation therefore contributes to an identified gap in the literature.
FT programmes are characterized by accelerated progression through career stages often underpinned by additional opportunities and investment to support the enhanced development of participants, although practices governing duration, content and structure as well as terms and conditions are diverse.4,5 For the current FT initiative, accelerated career progression was achieved through a quicker trajectory onto a health visiting programme for newly qualified nurses and midwives, with additional investment centring on increasing the number of funded training places. Assessed in terms of expanding the health visiting workforce the FT initiative has been successful, although caution is needed in the absence of destination and medium to long term follow-up data on retention and career trajectories. Bennett 19 estimates that an additional 4000 FTE health visitors are now in post with a further 900 student health visitors nearing the completion of their programmes.
A critical challenge of the FT initiative was the added demand placed on newly qualified nurses and midwives for rapid knowledge and competency development to meet the standards for specialist practice in order to successfully complete the programme. An acknowledged risk for FT programmes is that recruits may not be developmentally ready for the enhanced learning or responsibilities expected of them. 6 This risk has been documented in relation to accelerated medical education programmes, which are considered to impede clinical skill development 7 and may fail to prepare graduates with the necessary decision making and leadership skills. 20 Thus, selecting the right recruits with the right potential is crucial. While there was a consensus that the FT students possessed the right attributes for health visiting, they required more intense support in practice for which no additional resources were provided and this attracted critical reflections from some practice teachers as well as managers. The FT students themselves reported being less confident compared with the SE students, although there was no difference in the assessed competencies reported by practice teachers or differences in programme completion rates by route of entry.
There was debate by practice teachers and managers about whether FT students would require more support than newly qualified health visitors, with the implication that if so, this would pose challenges for an already stretched service. This resonates with Dotlich et al. 21 who reported that fast trackers often faced high expectations from their organizations and managers, which could be stressful for fast tracked recruits under pressure to succeed. FT programmes are demanding but they also provide structured support and incentives often on an ongoing basis to support anticipated enhanced performance and career trajectories. In this regard, the FT initiative is distinctive as career enhancement focuses on entry into health visiting for newly qualified nurses and midwives and not on their developmental needs or career trajectories over time. While practice teachers and managers agreed that all newly qualified health visitors should be supported, there was a clear expectation that this support needs to be based on individual need rather than route of entry.
Clark 22 suggests that there is an advantage of not providing separate opportunities for fast trackers on programme completion as this can lead to resentment among co-workers. In a profession where effective team work and colleagueship is pivotal and resources limited, careful consideration of the potential (dis)benefits of providing additional opportunities to some staff and not others in similar positions (e.g. newly qualified health visitors) is particularly pertinent. Further, all graduates, regardless of route of entry, were assessed to be competent for registration as health visitors and the FT students were keen not be viewed as ‘different’. Nevertheless, the return on the investment of government finance to expand the health visiting workforce hinges on retaining new recruits and ensuring that they are able to deliver a high-quality service. Providing all newly qualified health visitors with the necessary support and opportunities to further develop is one contributing factor in attaining these objectives and, in view of this, the absence of clear plans on how to respond to the significant increase in the number of new recruits entering the service reported by both practice teachers and managers is an important gap.
While this study was not able to report on the retention of recruits following graduation, the students themselves reported a commitment to work as health visitors for at least two years after qualifying. This reflects the findings of the only lifetime careers study of an integrated nursing and health visiting programme, 23 which could be considered a prototype of the current FT initiative. Of the 45 graduates surveyed, most had remained in the same post for at least two years as newly qualified health visitors, with many remaining in health visiting as clinicians, managers or academics over the lifetime of their careers. 23 The FT Accelerated Promotion Scheme for police officers in the United Kingdom provides a similar picture. Over a 30-year period, 94% of police officers in the scheme were retained within the police force, with 29% reaching chief officer ranks. 24 Additionally, fast tracked doctors were reported to join the workforce earlier providing a longer career7,20 and graduates undertaking accelerated courses were more likely to fill posts in areas of need such as primary care, than traditionally trained doctors. 4 These studies provide important messages for programmes designed to enhance recruitment through accelerated programmes and indicate that FT graduates from the current study may be successfully retained in health visiting but longitudinal research is needed to confirm such expectations.
This evaluation has highlighted that there are inherent tensions between creating policy and its implementation in practice even if the ideology behind the policy is well supported. 25 The large increase in recruitment needed to achieve the Health Visitor Implementation Plan policy 8 was not possible without drawing upon a new pool of recruits, in this instance, inexperienced but high-calibre newly qualified nurses and midwives. The rapid expansion of funded places on health visiting programmes took place while the profession was under considerable pressure with high caseloads and staff shortages. 13 As a consequence, additional strain was placed on existing resources particularly those of the practice teachers who needed to provide intense support to FT students amidst an increase in the number of students requiring supervision. This situation reflects Van Meter and Van Horn’s 26 assertion that there are a number of variables which mediate the link between policy and practice, one of which is the availability of adequate resources to facilitate the policy’s administration without which there is a risk that policy implementation can be diluted.
Although the target to both extend and increase recruitment has been met within a tight timeframe, the significant challenge of successfully retaining the new recruits remains, and this is an area that has received less attention and investment. During interview, all students were optimistic about their new roles and expressed high expectations for their careers in health visiting. However, there is currently an absence of a strong career pathway within the profession which could lead to disillusionment. 27 Without a structured system of ongoing support, role modelling and supervision, and sufficient promotion opportunities, there is a risk that new recruits will not remain long enough to re-energize health visiting, and to allow health visitors of sufficient quality and quantity to reach the full potential of their public health role. 28 If these challenges are not met, the same problems of retaining newly qualified teachers for more than one to two years identified by McConney et al. 29 will become evident.
The evaluation is limited by being confined to one initiative albeit in partnership with multiple sponsoring NHS Trusts. While it is acknowledged that the use of different data collection methods for practice teachers and managers could have had an impact on the depth and focus of the data, analysis highlighted consistency in data quality as well as content. Of potentially greater significance was the lack of experience of working with FT students by some practice teachers and this should be borne in mind when interpreting the results. Finally, biographical data showed the FT and SE students to be similar regarding age, professional qualification and academic achievement. However, other variables which were not explored such as the experience students had before entering nursing or midwifery could have offered added insights.
Conclusion
This evaluation has demonstrated that it is possible to address policy challenges by taking risks to innovate change. The core requirements of selecting the right recruits and enabling them to achieve the standards required for successful programme completion regardless of route of entry are the key successes of this FT initiative. While not without challenges, the FT initiative offers a potential strategy to increasing the health visitor workforce but further consideration of the developmental and career needs of new recruits, and FT recruits in particular, is needed. Future research to assess the retention of FT recruits and their impact on the health of young children and their families is also required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by Health Education London (formerly NHS London). The funder played no role in the design of the study, the interpretation of the findings, the writing of the paper, or the decision to submit.